
Abstract
There is significant controversy surrounding the possible link between fluoride exposure and lowered Intelligence Quotient scores (IQ) in children. Community water fluoridation (CWF) has been a widely-implemented practice for dental caries reduction, but concern has been raised around the potential for even these low levels to have a neurological impact. This narrative umbrella review aims to assess the current body of literature to provide an overview of the most recent high-level evidence and analyses on the association between fluoride exposure and children’s neurodevelopment. Google Scholar, ScienceDirect and PubMed were searched to identify relevant records. Studies included had to report on environmental fluoride exposures and children’s neurodevelopment, with lower fluoride exposures as a comparator. Only systematic reviews and meta-analyses were included. Data were extracted from each study, including effect measures from meta-analyses, and synthesis was organized in a narrative format by biomarker, analysis type and effect measure as applicable. Study quality was evaluated using the Critical Appraisal Skills Programme (CASP) Checklist and overlap analysis was conducted using the Graphical Representation of Overlap for OVErviews (GROOVE) tool. Overall, this umbrella review consistently found inverse associations between fluoride exposure at high levels and children’s IQ across the body of literature. There is limited data to support the same association for lower fluoride levels, as in those relevant to community water fluoridation. However, further investigation is required in order to fully understand the impacts of low fluoride exposures.
Keywords: Fluoride, Cognitive neurodevelopment, Urinary fluoride, Intelligence, Children’s IQ, Water fluoridation
Introduction
Background
Fluoride is the anion of fluorine, the ninth and most electronegative element on the periodic table. Water is the main source of fluoride intake1. Fluoride’s chemical properties make it an effective agent to remineralize tooth enamel as it is damaged, and thus it has long been promoted as a preventative measure for dental caries for children in particular. Fluoride salts have been widely added to municipal water supplies through CWF programs, and the intervention has been shown to be effective at reducing dental caries in these populations2.
Fluoride (F) is found most commonly in water among other foods and beverages3, and occurs naturally in groundwater in varying concentrations around the world as a result of contamination and environmental factors4. CWF has existed for decades in much of the United States, Canada, and Australia, among other countries. Moreover, the natural groundwater fluoride concentrations in parts of countries such as India, China, and western North America are significantly higher levels than are commonly approved for CWF. The limits set on fluoride levels in water most commonly cite the risk of dental and skeletal fluorosis1, side effects commonly seen in high-fluoride endemic areas. Currently, the United States Environmental Protection Agency (EPA) has an enforceable standard of a maximum of 4 mg F/L and a non-enforceable standard of 2 mg F/L4. The US Public Health Service recognizes 0.7 mg F/L as the optimal level4, which is widely regarded among others to be as well.
There has been a more recent concern, however, among scientists and members of the public surrounding the implications of fluoride from CWF as a potential neurotoxin. Meta-analyses of studies conducted primarily in China by Tang et al. (2008)5, Choi et al. (2012)6, and Duan et al. (2018)7 showed significant inverse associations between fluoride exposures and children’s IQ. Especially since the publications of these studies, there has been much debate about these possible implications within the scientific community. Recently, this concern has been exacerbated and spread amongst the general public as well. The last few years have seen a significant increase in the scientific literature on fluoride’s association with children’s IQ in addition to mainstreamed skepticism surrounding the issue and increased policy relevance in the United States in particular. In 2024, a US district judge ruled that the EPA must further regulate fluoride in drinking water, as it poses an “unreasonable risk” to children’s health8. In 2025, RFK Jr.’s appointment to secretary of the United States Health and Human Services (HHS) marked a strong exigence from the federal cabinet for agencies to reconsider fluoride guidelines9.
Problem Statement and Rationale
This paper aims to address the association between F exposure and adverse neurodevelopment impacts upon children. The PECO statement (Population, Exposure, Comparator, Outcome) for this research question is as follows: population: human children 18 years and under, exposure: higher levels of fluoride exposure (depending on assessment type), comparator: lower levels of fluoride exposure, outcome: neurological damage. This topic is currently highly relevant with escalated controversy and significant to the field of public health in shaping policy. These developments and studies have not yet been synthesized in an umbrella review.
Objectives, Significance and Purpose
This umbrella review is intended to assess the highest-level studies since 2021 on this topic, including systematic reviews and meta-analyses. This review aims to synthesize these recent high-level studies in order to provide an overview of the most relevant analyses. The last five years have seen a significant increase in the investigation into this research question along with a significantly wider range of surveyed countries in the primary research. Note, however, that there were no restrictions on the dates of the primary studies included in the reviewed analyses. Furthermore, this review aims to provide insight into the possible childhood neurocognitive implications relevant to CWF in addition to those relevant to endemic fluorosis or high fluoride areas. The objective of this article is to provide an in-depth overview of the current state of this research through a combination of narrative synthesis and quantitative reporting on the relevant systematic reviews and meta-analyses that address the research question. The synthesis and analysis are intended to be thorough and accessible with a narrative format to clearly inform on this problem. While this review does not address the entire scope of the fluoride debate, it is intended to address the controversy in part with specific respect to this problem statement.
Scope and Limitations
This review aims to assess neurodevelopment outcomes, primarily children’s IQ, but also includes memory/learning impairment and cognition. This review is not intended to provide an analysis into other fluoride side effects such as fluorosis or thyroid complications, or a risk-benefit analysis of fluoride as a public health intervention, nor does it provide an analysis of the dental benefits of fluoride. Resources for this review were limited, and the quality of the synthesis is limited by the lack of more than one author.
Methodology Overview
The general protocols of the JBI Manual for Evidence Synthesis10 were followed as a guide for this review. A search of three databases was conducted to identify records. Data was extracted and recorded in charts shown in the results section. A narrative synthesis was used to draw conclusions in addition to a protocoled quality assessment and overlap analysis.
Methods
Eligibility Criteria and Search Strategy
The search for relevant literature was conducted through the databases of PubMed, Google Scholar, and ScienceDirect. Only published peer-reviewed meta-analyses and systematic reviews were sought for inclusion, as this is an umbrella review. A date restriction was applied to only include articles since 2021. The reason for this restriction was to gain the most relevant overview of the research on fluoride. Each of the 5 years since 2021 has seen consecutive systematic review/meta-analyses and an increase in the breadth of primary research. Until these recent years, primary research had come almost exclusively from China, India and Iran. More recent articles have drawn upon new developments in primary research from Canada, New Zealand, Mexico, Pakistan, and Denmark among other countries. The more recent analyses thus have a more comprehensive body of primary studies that is less susceptible to any possible region-specific confounders. Furthermore, this restriction dramatically reduces the redundancy in primary research analysis since study overlap is pervasive between systematic reviews on this subject. Nearly every primary publication analyzed in meta-analyses prior to 2021 has been included in meta-analyses since. The exclusion of the three meta-analyses published before 2021 reduces an already redundant body of evidence while also not excluding any unique effect measures as all employed measures have been used in the articles since 2021. Therefore, this date filter allows for a more robust and relevant analysis of the body of literature without creating a biased result. Additionally, articles were limited to those written in English and to those with a specific focus on the link between environmental fluoride exposures and neurocognitive effects. Studies with a focus on dental or skeletal fluorosis or on general adverse impacts and toxicity of fluoride were excluded.
The PubMed search was conducted on June 29, 2025, using the most recent version of the interface which was updated as of June 27, 2025. Advanced search was used to include Boolean operators, generating the search string, (fluoride) AND ( (IQ) OR (Neurocognitive) ) AND (water). Articles that did not meet the date restriction were removed before screening using the date filter built into the software. Article screening was also conducted using the automation tools built into the interface to only include systematic reviews and meta-analyses in the search results. The results were then screened manually for all set criteria.
The Google Scholar search was conducted from July 1-4, 2025, using the most recent non-AI interface available. Advanced search was used and the same search string as the PubMed search was obtained by searching for articles containing “all of the words”, fluoride & water; and “at least one of the words”, neurocognitive or IQ. The procedure from the PubMed search at this stage was repeated using Google Scholar’s built-in date filter, and articles were then screened with the filter that only showed results for review articles. Review articles that were not systematic reviews or meta-analyses were removed via title and abstract screening manually as were reviews that did not meet set criteria to address the research question.
The ScienceDirect search was conducted from July 1-4, 2025, using the most recent non-AI interface available and the identical search string as the PubMed search, (fluoride) AND ( (IQ) OR (Neurocognitive) ) AND (water). Years 2021 through 2025 were checked off on ScienceDirect’s built-in filter for inclusion prior to screening. All articles but reviews were excluded using another built-in automation tool and the remaining records that were not systematic reviews or containing meta-analysis were removed manually along with records that did not meet criteria via abstract and title screening.
The final search was conducted on July 4, 2025. The remaining duplicate records within and between databases were then removed, and articles were sought for retrieval and finally assessed for eligibility.
Data Extraction
Full-length articles and supplements were retrieved, and detailed notes were taken to extract information. Data points included authors, date of publication, study design, number of studies included, countries, age range, exposure assessments, the reference points for fluoride levels (including the levels considered “high” and “low” if applicable), outcomes, overall findings, limitations, future recommendations, and risk of bias in the study samples. The numerical thresholds used to classify exposure levels come from policy cutoffs of agencies like the WHO and EPA as previously described; moreover, these values were consistently applied in the reviewed articles as indicated in Table 1. For systematic reviews that included meta-analyses, the analyses were summarized individually. This also included sub-analyses addressing water and urine exposures as biomarkers individually. Data points varied to a greater degree as per the different study designs, but the results were compared according to the following: author, date of publication, type of meta-analysis, biomarkers and exposures, results and effect measure, 95% confidence interval of result, and heterogeneity expressed by p-value and I² % when applicable.
Synthesis Method
These data were organized into the charts in Tables 1 and 2 as seen in the results section. Additionally, evidence has been synthesized and discussed through a narrative approach. As applicable, findings are broken down by effect measure, analysis type, and major biomarkers, water, and urinary F. Furthermore, an overlap analysis was conducted, and data has been displayed using the tool GROOVE11 in Figure 2. The reviewed primary studies entered into the matrix of the tool were taken from the results, references, or supplements of each of the six included studies, and Corrected Covered Area (CCA) was calculated. CCA = (# of primary studies including double counting – # of index publications) / (# of index publications) (# of reviews) – # of index publications). It should be noted that due to its broader scope, results extracted from the “NTP Monograph on the State of the Science Concerning Fluoride Exposure and Neurodevelopment and Cognition” (2024)12, including the studies included in the overlap analysis, come only from its review of studies relevant to the research question. This review included the 72 studies assessing child IQ and an additional six assessing child learning and memory and cognitive development.
Quality Assessment
Overall quality of the reviews was assessed using CASP checklists for systematic reviews13 as a guideline. Estimate confidence ratings are provided in Table 1 The appropriate checklist was used depending on the study design. Questions 1 through 7 were answered with a “yes,” “no,” or “not sure.” (8 through 10 discussed risk-benefit analysis and implementation, which are not relevant to the research question). The reliability and confidence in each paper were rated based on major concerns/limitations. The rating scale used is in accordance with that given by Shaheen et al. (2023)14; these estimates are given based on the checklist outcomes and are given to illustrate the general confidence in the results. “High” indicates little to no flaws, none of which are critical to the results. “Moderate” indicates that there were several non-critical flaws and may give a reliable summary. “Low” indicates that there was one critical flaw rendering the synthesis potentially unreliable. “Critically low” indicates that the review cannot be relied upon for an accurate account of the research body. The CASP item-by-item checklist summary for each review is available in Supplement 1 and specific critical flaws and strengths that characterized these assessments are detailed in 3.3 Quality of Studies Results. Critiques of existing meta-analyses given by the NTP Monograph12, were also taken into consideration to identify any additional concerns regarding these analyses as was relevant to the checklist.
Results
Search Results
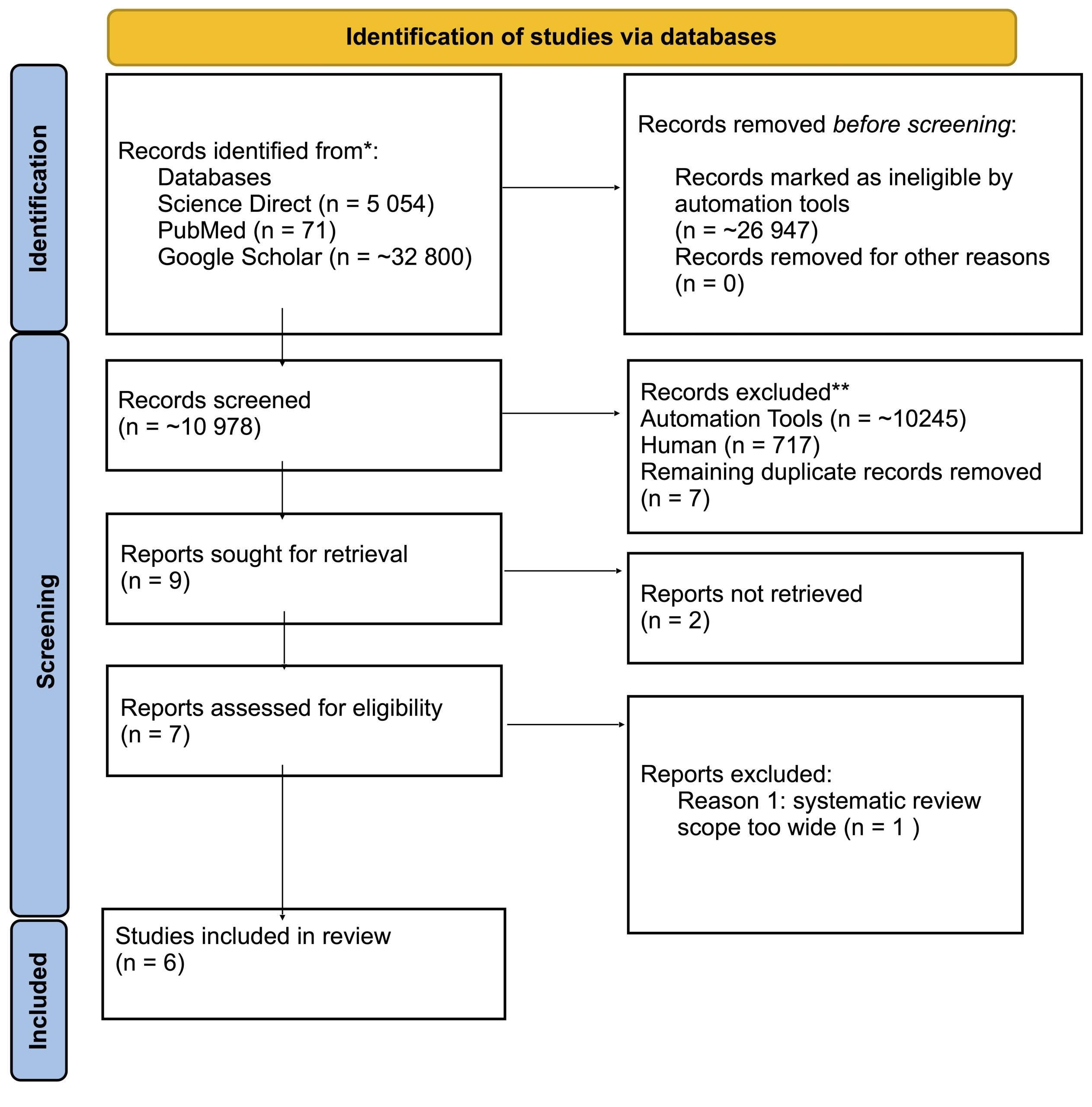
Figure 1 shows a modified PRISMA 2020 flow diagram15 showing the study selection process. Large figures for the numbers of identified and retrieved records are given as approximates, as they were given by Google Scholar search results. Approximately 10,978 records were screened; 9 in the end were sought for retrieval. The full-texts of two studies could not be retrieved, and one systematic review assessed for eligibility was excluded due to the fact that it did not provide sufficient focus on the research question being investigated. Six studies were included in the review. It should be noted that the authors of the NTP Monograph12 conducted a companion study in Taylor et al. (2025)16, which has been included separately in this review. Citations of the included studies were additionally checked, verifying that all relevant meta-analyses were included and there was no indication that any other important systematic reviews were left out of the synthesis.
Characteristics of Studies
Table 1 shows a summary of the characteristics and findings of the included papers. For the NTP Monograph12, the data shown only pertains to the systematic review on children as previously mentioned. It also includes overlapping sets from other reviews; the studies unique to each review and the overlap are shown in the GROOVE matrix in Supplement 2. Of the six studies included, three included meta-analysis with a systematic review, two only conducted systematic reviews, and one only conducted meta-analysis. The most recent two studies have provided the most comprehensive analyses, with wider bodies of evidence being assessed. The majority of primary research reviewed has been conducted in China, India, and Iran, with some research also coming from countries like Mexico, Canada, Pakistan, and New Zealand. Most of the studies primarily addressed fluoride exposure from drinking water concentrations and urinary fluoride levels; some also included other biomarkers and exposures like coal burning, evidence of fluorosis, and intake fluoride, but the primary research on these is much lower. Almost every review used public health agency guidelines for fluoride levels as classifications for high and low fluoride exposures, as shown in the table. Gopu et al. (2022)17 was the only study to use above or below 2 mg F/L as the reference, and Veneri et al. (2023)18 also used the median value for a reference with 0.7 mg F/L as an additional reference. Children’s IQ scores were the most assessed outcome; however, some primary research analyzed by several of the included papers assessed other neurocognitive outcomes and testing measurements.
| Reference | Study Design | Number of Studies | Countries | Age Range | Exposure Assessments | Water F Reference Levels | Outcomes | Overall Findings | Major Limitations and Future Research Recommendation | Risk of Bias (RoB)/quality of studies | Quality Assessment Confidence Estimate |
| Miranda et al. (2021) | Systematic Review and Meta-Analysis | 27 | China, India, Iran, | Children 6-18 | Drinking water; Urinary fluoride one study analyzed populations exposed to fluoride through coal burning | High > 2 mg F/L; Low 0.5-1.0 mg F/L (WHO classification) | Children’s IQ Scores; other neurocognitive testing measures | Exposure to low water F levels not associated with IQ/neurol-ogical damage; exposure to high levels is | High heterogeneity among studies compromises quantitative results; not possible to state association or lack of between F exposure and any neurological disorder | 8 high RoB; 19 low RoB | Critically Low |
| Gopu et al. (2022) | Systematic Review | 46 | China, India, Canada, Iran, Mexico, Pakistan Mongolia, New Zealand | Children < 18 | Drinking Water; Coal Burning | Low < 2 mg F/L ≤ High | Children’s IQ Scores; other neurocognitive testing measures | High levels of F exposure may result in lowered IQ/cognitive outcomes | Low quality studies and lack of comprehensive exposure estimates are a limitation to conclusions- future high quality and longitudinal studies needed | 20 poor quality; 14 fair quality; 7 good quality; 5 excellent quality | High |
| Veneri et al. (2023) | Systematic Review and Meta-Analysis | 33 | China, India, Canada, Iran, Mexico, Pakistan, New Zealand | Children < 18 | Drinking Water; Urinary Fluoride; Hair and Nail Fluoride; Fluoride Tablets; Intake Fluoride; Serum Fluoride | 1.2 mg F/L (median value); 0.7 mg F/L (US Public Health Service recomme-ndation) | Children’s IQ Scores; 1 study used IQ derived scale of intelligence | Low levels of exposure begin to show adverse effects on IQ; dose-response analysis showed substantial inverse association above 1.0 mg F/L, becoming steeper above 2.0 mg F/L | Risk of bias and confounding limits conclusions- future high quality and longitudinal studies needed | 11 high RoB; 19 moderate RoB; 3 low RoB | Low |
| Kumar et al. (2023) | Meta-Analysis | 32 | China, India, Canada, Iran, Mexico, New Zealand, Spain | Children < 18 | Drinking water; Urinary fluoride | Low < 1.5 mg/L (WHO recommendation) < High | Children’s IQ Scores | CWF exposures are not associated with lower IQ scores. | Higher level association in endemic areas requires further investigation; more scientifically robust and interventional studies required | 22 definitely high RoB; 4 probably high RoB; 2 probably low RoB | Critically Low |
| NTP Monograph (2024) | Systematic Review | 78 | China, India, Canada Iran, Mexico, Pakistan, New Zealand, | Children < 18 | Drinking water; Urinary fluoride; Coal Burning; Infant Formula; Evidence of Fluorosis; Endemic vs non-endemic residence | Low < 1.5 mg/L (WHO Recomm-endation) < High | Neurodevelopment (including Children’s IQ scores); Neurological/Neurobeha-vioral outcomes | With moderate confidence, high F exposures consistently associated with lower IQ scores; low confidence in other neurological impacts | Further research required to more comprehensively understand potential for lower exposures to have an impact | 56 high RoB; 22 low RoB | High |
| Taylor et al. (2025) | Systematic Review and Meta-Analysis | 74 | China, India, Canada, Iran, Mexico, Pakistan, New Zealand, Taiwan, Denmark, Spain | Children < 18 | Drinking Water; Urinary Fluoride; Evidence of Fluorosis; Intake Fluoride | 4.0 mg F/L (EPA enforceable standard); 2.0 mg F/L (EPA non-enforceable standard; 1.5 mg F/L (WHO recommendation); 0.7 mg F/L (US Public Health Service recommendation | Children’s IQ Scores | Inverse associations and dose-response association between F exposure and IQ scores above 1.5 mg F/L | Limited data and uncertainty regarding association when F exposure was estimated from drinking water alone with concentrations <1.5 mg F/L | 52 high RoB; 22 low RoB | High |
Quality of Studies Results
The two studies considered “critically low” were significantly lacking in their methodology. Kumar et al. (2023)19 did not appear to have followed any predefined protocol and additionally lacked criteria or trustworthy tools to assess the quality of primary evidence and RoB. Miranda et al. (2021)20 also had serious concerns with regard to their methodology. For the meta-analysis, the authors only identified studies that matched narrow concentration ranges to align with WHO classification and only included low-risk-of-bias studies. Therefore, many possibly relevant primary research studies were left out of the analysis, which only included ten studies. Additionally, each of these studies had serious problems with the reporting of results. Kumar et al.19 failed to provide adequate detail supporting how results were determined and lacked investigation into the causes for heterogeneity and its effect on the results. Additionally, the paper lacked sufficient discussion on its limitations and failed to address how the authors’ competing interests were dealt with (see 3.8 Funding Considerations and Conflict of Interests Summary).
Miranda et al.20 had several concerns regarding its results, most importantly being its use of odds ratio (OR) as an effect measure, which is limited in its ability to measure the fluoride-IQ association. Moreover, according to Altman et al. (1998), “interpretation of the odds ratio as an approximation to the relative risk becomes unreliable when events are common, and thus its use for prospective studies, especially randomized trials and systematic reviews, has been criticized”21. Therefore, the OR is inappropriate as an effect measure for the fluoride-IQ investigation because of its inflation of relative risk due to the high prevalence of high fluoride exposures and low IQ scores. Because of the unsuitable effect measure, the pooled estimate in Miranda et al.’s20 meta-analysis of 10 studies and its usefulness for practical interpretability are unreliable and limited.
Veneri et al.18 was the only study rated “low”. This study had a well-defined protocol and appropriately extracted data and quality assessment. However, there were concerns regarding the results, including a lack of investigation into heterogeneity and no reported p-values. The effect measure, Weighted Mean Difference (WMD), does not account for test heterogeneity between studies, which is important to this research because different IQ tests and metrics are used in the primary research (Ravens Tests, WPPSI-III, etc.). The one critical flaw that characterizes this classification is inaccuracy of the results; the NTP Monograph12 details how the pooled WMD of this study is invalid. It was noted that all relevant research was likely to have been included based on the quality of the methodology; however, the NTP does note that the paper lacked justification for not including certain studies.
The remaining three papers were classified as “high” quality. Gopu et al.17 and the NTP Monograph12 were the only two studies that did not conduct meta-analyses. Each was found to have clearly defined protocols, sound methodology, and detailed quality assessment, and the main findings were consistent with the information from the primary research. The NTP Monograph12 was especially detailed and thorough in its investigation; however, much of the paper analyzed broader impacts not included in this review. Taylor et al.22 was the only meta-analysis not found to have any serious concerns with its methodology, using the appropriate Standard Mean Difference (SMD) effect measure to account for test heterogeneity and robust meta-analysis protocols and stratifications.
Overall Results
Of the six included reviews, with varying levels of confidence, two found an inverse association between IQ and fluoride exposure above 2 mg F/L, two found the association above 1.5 mg F/L, and one found a dose-response association as low as 1.0 mg/L. The one remaining paper found that fluoride exposures relevant to CWF had no influence over IQ scores and that the higher exposure association requires further evidence. Most of the studies cited low quality and lack of evidence for the lower F exposure association as a reason that further investigation is required to understand those effects. Detailed overall findings, conclusions, and RoB breakdown among primary studies are included in Table 1.
Meta-Analysis Pooled Effects Summary and Interpretation
All meta-analysis results are shown in Table 2. Miranda et al.20 was the only meta-analysis to use an OR as a measure for the pooled effect. The result of the analysis was an OR of 3.88 (95% CI 2.41, 6.23), a substantial harmful effect of high F exposure on IQ scores. This evidence was qualified by the authors as very low because of the high heterogeneity (I² = 77%, p < 0.00001) and publication bias. Significant heterogeneity was still observed after the sensitivity analysis, which excluded studies identified as having a high risk of publication bias.
Veneri et al.18 was the only included meta-analysis to use WMD as a pooled effect type. The result of the pooled WMD of IQ scores comparing highest versus lowest F categories was -4.68 (95% CI -6.45, -2.92), a strong inverse association. However, these findings were limited by the high RoB in primary studies, and heterogeneity (I² = 98.75%) was not accounted for by the effect measure of WMD.
Kumar et al.19 reported an inverse association in the pooled SMD of IQ scores of −0.33 (95% CI −0.44, −0.22) with substantial heterogeneity (I² = 83%, p < 0.0001). For endemic areas there was an effect size of -0.46 (95% CI -0.58, -0.35) with substantial heterogeneity (I² = 81%, p < 0.001). However, the result for non-endemic areas was found to be not statistically significant (p = 0.14) at SMD 0.07 (95% CI -0.02, 0.17) with no observed heterogeneity (I² = 0%, p = 0.64). Taylor et al.22 also showed statistically significant and moderately lower IQ scores with a pooled SMD of -0.45 (95% CI -0.57, -0.33) with high heterogeneity (I² = 94%, p < 0.001) and evidence of publication bias.
| Reference | Number of Studies; Number of Participants | Analysis | Biomarkers/Exposures | Result | 95% CI | Heterogeneity p value; I2 |
| Miranda et al. (2021) | 10 Studies; n= 2939 | OR Pooled Effect Type | Drinking water and urinary F | OR = 3.88 (Harmful) | (2.41, 6.32) | p < 0.00001 I2 = 77% (High) |
| Veneri et al. (2023) | 30 Studies; n= 16 154 | Random effects pooled WMD | All assessed exposures | WMD = -4.68 (Harmful) | (-6.45, -2.92) | NR I2 = 98.75% (High) |
| 25 Studies; n= 8318 | Random effects water F WMD | Drinking water F (0.13-5.55 mg F/L) | WMD = -5.60 (Harmful) | (-7.76, -3.44) | NR I2 = 91.69% (High) | |
| 15 Studies; n= 4455 | Random effects urinary F WMD | Urinary F (0.16- 7 mg F/L) | WMD = -3.84 (Harmful) | (-7.93, 0.24) | NR I2 = 96.22% (High) | |
| 25 Studies; n= 8318 | Water Fluoride Dose-Response Linear regression analysis | Drinking water F > 1 mg F/L | -3.05 IQ per 1 mg F/L (Harmful) | (-4.06, -2.04) | ||
| 15 Studies; n= 4455 | Urinary Fluoride Dose-Response Linear regression analysis | Urinary F > 0.28 mg F/L | -2.15 IQ per 1 mg F/L (Harmful) | (-4.48, 0.18) | ||
| Kumar et al. (2023) | 28 Studies; n= 11 412 | Random effects pooled SMD | Drinking water and urinary F | SMD = -0.33 (Harmful) | (0.44, -0.22) | p < 0.00001 I2 = 83% (High) |
| 23 Studies; n= 7778 | Random effects SMD; endemic areas | Drinking water and urinary F; higher F (mean 3.7 mg/L), lower F (mean 0.7 mg/L) | SMD = -0.46 (Harmful) | (-0.58, -0.35) | p < 0.00001 I2 = 81% (High) | |
| 8 Studies n= 3634 | Random effects SMD; non- endemic areas | Drinking water and urinary F; higher F (mean 0.90 mg/L), lower F (mean 0.30 mg/L) | SMD = 0.07 (Statistically insignificant) | (-0.02, 0.17) | p = 0.64 I2 = 0% (None) | |
| 3 Studies n= 3003 | Cubic spline β regression analysis for Children’s Urinary Fluoride (CUF) | + 0.5 mg F/L urine | β = 0.16 (Statistically insignificant) | (-0.40, 0.73) | p = 0.43 I2 = 0% (None) | |
| 3 Studies n= 949 | Cubic spline β regression analysis for Morther’s Urinary Fluoride (MUF) | + 0.5 mg F/L urine | β = -0.92 (Statistically insignificant) | (-3.29, 1.46) | p = 0.03 I2 = 72% (Moderate) | |
| Taylor et al. (2025) | 59 Studies; n= 20 932 | Random effects pooled SMD | All assessed exposures | SMD = -0.45 (Harmful) | (-0.57, -0.33) | p < 0.001 I2 = 94% (High) |
| 31 Studies n= 12 487 | Water Fluoride Linear Dose-Response Mean-Effects Analysis | Drinking water F | Mean SMD = -0.15 (Harmful) | (-0.20, -0.11) | ||
| 20 Studies n= 9756 | Urinary Fluoride Linear Dose-Response Mean-Effects Analysis | Urinary F | Mean SMD = -0.15 (Harmful) | (-0.23, -0.07) | ||
| 13 Studies n= 4475 | Linear β regression analysis individual-level effect | + 1.0 mg F/L urine | β = -1.63 (Harmful) | (-2.33, -0.93) | p < 0.001 I2 = 60% (Moderate) |
Meta Analysis by Biomarker Summary
Water Fluoride
Three meta-analyses measured the subgroup association of fluoridated water exposure with cognitive outcomes. Veneri et al.18 calculated a WMD for water, which was higher than the overall WMD at -5.60 (95% CI -7.76, -3.44), and heterogeneity was still high (I² = 91.69%). Their linear dose-response regression analysis showed a substantial linear decrease of 3.05 IQ points per 1 mg/L increase in water F concentration (above 1 mg F/L and up to 2 mg F/L, where the association becomes steeper). Finally, Taylor et al.22 found a linear dose-response association with water F between exposed and reference groups with an SMD of -0.15 (95% CI -0.20, -0.11).
Urinary Fluoride
According to the relation provided by Villa et al. (2010), assuming that most of F intake comes from water, 1 mg F/L in drinking water translates to a urinary concentration of ~0.38 mg F/L24. Additionally, F levels in water likely underestimate total F exposures that would be gathered from individual urinary measurements. Five meta-analyses measured the subgroup association of urinary fluoride with cognitive outcomes. Veneri et al.18 calculated a WMD for urine of -3.84 (95% CI -7.93, 0.24), lower than that of the water F measurement and still with even higher heterogeneity (I² = 96.22%). Their linear dose-response regression analysis similarly showed a lower effect with an IQ score decrease of 2.15 mg F/L per 1 mg F increase above 0.28 mg F/L. Kumar et al.19 conducted two beta-regression analyses with cubic splines for CUF and MUF. For a 0.5 mg F/L increase, the regression coefficients were 0.16 (95% CI -0.40, 0.73) and -0.92 (95% CI -3.29, 1.46), respectively. These results were found to be statistically insignificant (p = 0.43, I² = 0%) and (p = 0.03, I² = 72%), respectively. Taylor et al.22 calculated a linear dose-response mean effects SMD for urine equal to that of the calculation for water at -0.15 (-0.23, -0.07). Furthermore, a beta regression analysis of 13 studies with reported individual-level exposures found an inverse dose-response linear association with a 1.63 IQ point decrease (95% CI -2.33, -0.93; p < 0.001 I² = 60%). Associations remained inverse after stratifications by factors including RoB, age, sex, country, and exposure/outcome assessments. Threshold effects were not reported for any of the regression analyses.
Overlap Analysis Results
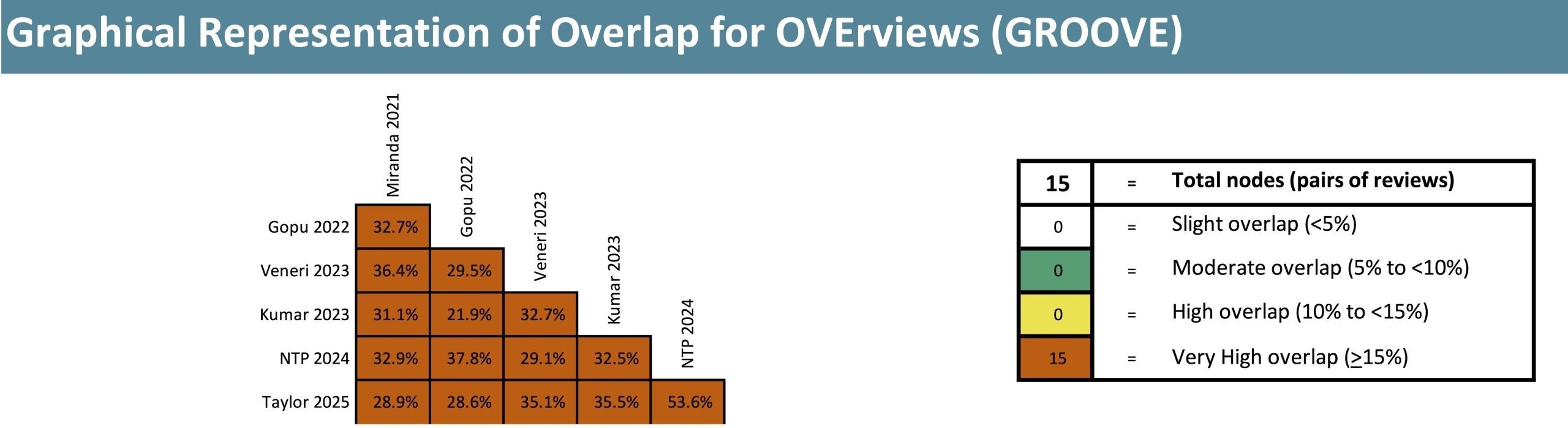
The GROOVE tool11 calculated the corrected covered area (CCA) to measure the overlap in primary research between reviews. The calculated CCA was 30.35%, interpreted by the tool as “very high overlap“. The graphical representation of the overlap between studies is shown in Figure 2. The high levels of overlap between all nodes (pairs of reviews) demonstrate a risk of redundancy when interpreting the results of these primary studies.
Risk of Publication Bias and Confounders
Assessment of risk of publication bias within included meta-analyses is inconsistent and limited in several. Miranda et al.20 and Kumar et al.19 used funnel plots for their meta-analyses. The former demonstrated potential for publication bias that was still limited after sensitivity analysis that lowered the I² from 77% to 62%. In conjunction with their quality review, the authors concluded that the evidence available was not strong enough to affirm the association for high fluoride exposure. In the latter, sensitivity analysis had no observed effect on the symmetry of the funnel plot. Similarly, Veneri et al.18 used the ROBINS-E tool to classify RoB with studies with low RoB tending towards the null hypothesis. Egger tests for sensitivity analyses suggested low RoB for water and urinary measures.
For the mean effects analysis, Taylor et al.22 found high risk of publication bias using Egger test and funnel plots. Adjustments were made to the pooled SMD using trim and fill methods which supported the statistically significant inverse association at a substantial difference of –0.63. These assessments were not present in other reviews where other quality assessments lacked criteria and rationale or where narrative analysis was used.
Management of confounding variables and covariates was consistently assessed in risk of bias and quality appraisals for individual studies in the systematic reviews. Among the primary studies reported on, the majority contained management for age and sex with several also adjusting for socioeconomic status, parental IQ, education, body mass index, and family and individual medical history. Other noted confounders adjusted for included urinary creatinine, race, parental alcohol consumption and age of pregnancy. Few studies managed neurotoxic confounders such as arsenic, lead, and iodine deficiency, which was frequently discussed as a serious limitation. Nevertheless, high quality studies such as those conducted by Green et al. (2019)25 and Bashash et al. (2017)26 continued to find inverse associations of similar magnitudes with appropriate adjustment for such confounders.
Funding Considerations and Conflict of Interests Summary
All included reviews with the exception of the meta-analysis by Kumar et al.27 declared no conflicts of interest. The latter declared several competing interests. At the time the article was published, J. Kumar was a member of the American Dental Association’s National Fluoridation advisory committee and was a reviewer of a report on the NTP Monograph in 2021. Susan Fisher-Owens was a member of American Academy of Pediatrics’ Section on Oral Health and a co-author two publications related to fluoride use in dental practice. She was also a consultant for Arcora Foundation on medical-dental integration and has research funding for said subject from Health Resources Services Administration and served on an independent Data and Safety Monitoring Board for a study funded by Colgate.
The study by Miranda et al.20 was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) of the Brazilian government. The article by Gopu et al. was funded by the Teesside University Ph.D. Studentsship. The NTP Monograph28 and its companion review by Taylor et al.22 were supported by departments of the National Institutes of Health of the US government’s HHS and performed for the National Toxicology Program and the National Institute of Environmental Health Sciences, respectively. None of these funding institutions were involved in the data collection, analysis, interpretation, or preparation of the manuscripts. The remaining articles had no grants or funding.
Discussion
In this umbrella review, an investigation was conducted into the association between both high and low fluoride exposures and children’s IQ. For high F exposures (as in those exceeding 1.5-2 mg F/L), statistically significant inverse associations between exposure and outcome have been consistently found across different study designs, quality levels, effect measures, and subgroup analyses with effect magnitudes typically ranging from moderate to substantial mean differences in IQ. However, given high heterogeneity and risk of publication bias which was pervasive throughout the body of literature, clinically meaningful results cannot be drawn from the majority of these estimates. For F exposures less than 1.5 mg F/L from fluoridated water alone, results were less clear, and most papers identified a need for further research to investigate the association at levels that are more commonplace for CWF. Notably, Taylor et al.22 conducted a high-quality individual-level exposure meta-analysis demonstrating an estimated 1.63 IQ point decrease for every 1 mg F/L increase in urinary fluoride. Because of the high quality of the study and the increased accuracy through individual-level urinary F measures, this is the most methodologically robust estimate currently available to describe the dose-response correlation. Despite the smaller estimated decrease compared to others, this estimate is significant in terms of public health relevance.
| Drinking Water F | Urinary F | Blood/Serum F | Hair/Nail F | Coal Burning | Evidence of Fluorosis | |
| Validity | Provides measurements for entire regions based on primary exposure source | Individual and precise measurements of fluoride content at specific time; lower RoB | Individual and precise measurements of fluoride content at specific time; lower RoB | Provides individual measurement of long term and chronic exposure | Provides measurements for entire regions based on one exposure source | Provides estimate based on structural changes from long term exposure |
| Limitations | Imprecise; assumptions must be made for individual estimates and does not consider other sources of fluoride | Represents recent exposure only which can vary significantly | Levels vary widely throughout the day as result of other metabolic functions | Highly susceptible to environmental confounders; imprecise especially for lower threshold investigation | Limited to certain areas where this is the primary exposure source | Restricted to chronic exposure levels; threshold effect is variable |
The results and conclusions of syntheses conducted prior to 2021 have been considerably refined by works published since. Substantial inverse associations were found in meta-analyses predating 2021, and these findings have been confirmed to more accurate effect measures and specific thresholds with higher quality evidence. Recent systematic reviews have been able to draw on primary data from many more regions outside of large Asian countries and account for confounders and effect modifiers to a greater degree. Since 2021, it has been found that high or chronic fluoride exposure levels consistently yield a notable inverse association as demonstrated by earlier syntheses. Furthermore, given the increase in the number of surveyed countries, the more recent data synthesized in this review has given greater insight into fluoride exposure in terms of CWF relevance with lower thresholds being assessed as well with several key reviews identifying this as a gap for further study. Given these reasons, the associations observed prior to 2021 have since become more meaningful as clinically relevant data.
Study Overlap
This overlap is mainly a result of the narrow scope of this research question and the relative novelty of the growth in research in this area. As a result, key primary studies from earlier years are more common across reviews. Over 50% overlap is also present between the NTP companion studies which each have their own purposefully unique scope and objectives as opposed to one being a regurgitation of the other. Given the high number of common primary studies between papers, the consistency of findings across reviews may be inflated, especially considering findings relating to IQ from high F exposure. However, the consistency in adverse effects across other neurocognitive outcomes as demonstrated by many of the non-overlapping studies such as from the NTP Monograph12, supports the generalizability of these findings with respect to adverse neurocognitive impact and therefore the redundancy from the overlap does not appear to nullify these findings or their generalizability.
Heterogeneity, Measures, and Confounders
Investigation by authors into plausible sources of heterogeneity was marginal given its prevalence in the reviewed data. It was generally noted among stratifications that differences in health outcomes evaluated, diversity of primary study designs such as IQ scales, and the wide range of ages assessed accounted for much of the heterogeneity in the results. One meta-regression29 found lowered I2 values upon subgroup restrictions with respect to geographic region, mean age and year of publication with much of the heterogeneity still unaccounted for. Taylor et al.22 noted that heterogeneity in their meta-analysis results was not found, rather, the diversity in study designs (or overall heterogeneity for the body of evidence) supports the robustness of the conclusions given the consistency in findings of the inverse association.
The primary concern regarding heterogeneity is incompatible measurement, especially pooled water and urinary effects. Several issues arise from such pooling. The conversion relationship between water and urinary F established by Villa et al.24 as previously discussed, relies on the assumption that water is the primary source of fluoride intake, which limits its usefulness as a standard for CWF-relevant levels. Table 4 provides an overview of the validity and drawbacks of measures used in this research. It is important to note that, although urinary and blood serum measures are individual, they are susceptible to significant intra-individual variability depending on unaccounted factors such as kidney function, creatinine adjustment, and hydration levels in addition to the timing of the sampling. The major implications for bias with respect to pooling water and urinary sources depend on the magnitudes of exposure. For endemic areas, the biases and imprecisions introduced by biomarkers are relatively inconsequential for interpretation of the effect measure. This is drastically different compared to CWF-relevant areas where major percentages of daily fluoride intake are likely to go unaccounted for using water concentrations alone and where the direction of bias from spot urine sampling remains unclear. The measurement error from biomarker incompatibility in addition to the individual biases make the current available data with respect to low exposure levels unreliable.
Incomplete control for key confounders such as lead, arsenic and iodine deficiency is also a limitation of the evidence base where residual confounding from these covariates could bias the results. However, given the consistency of the finding of the inverse association across the high- and low-quality studies, with and without adjustment, and with sensitivity analyses by systematic reviews, it is less likely that the inverse association can be accounted for by these confounders. The magnitude of pooled estimates, especially those without newer studies, may be moderately biased towards the inverse association. Future studies should adjust for these confounders, especially if associations are to be investigated at lower F levels.
Publication Bias
The conflicts of interest present with the authors Kumar et al.19 create a potential influence on interpretation that would bias results in favour of fluoride safety. Dental associations corporations such as those the authors were involved with have long maintained the high degree of the safety around fluoride in all its mainstream uses and benefit financially from the general acceptance of fluoride safety with usage in dental products as children’s health interventions. Therefore, if these conflicts had any influence on the results and recommendations provided by this article, the bias would be towards the null hypothesis.
The funding that studies received from government institutions also had the potential to influence interpretation as well. HHS institutions and CAPES have historically held the position that water fluoridation is a beneficial intervention, and the neurocognitive impacts had seldom been taken into consideration. Thus, if funding considerations by these institutions biased results in any way because of their policy positions, they would be more likely to underestimate the magnitude of the demonstrated effects.
Public Health Implications
Several countries around the world have high F concentrations in the water that greatly exceed standards set by health agencies. The high level of evidence supporting the fluoride-IQ correlation in children in these endemic areas could be a cause for concern in these communities. In the future, many community water systems may need to become more regulated to reduce these high exposures for neurological reasons in addition to fluorosis concern. It is important to note that no primary research concerning fluoride and children’s IQ has been conducted in the United States, where these impacts would be especially relevant in areas with elevated F levels. No primary research studies conducted in the US were detected among primary studies of reviews included in this umbrella review; furthermore there have been no such studies performed according to the knowledge of the authors Taylor et al.22. However, one 2024 study30 conducted in the US did find that fluoride exposure was associated with an increase in neurobehavioural problems.
As of 2024, over 2.9 million US residents were served by public water systems where F concentrations exceed 1.5 mg/L31. Additionally, according to the US Geological Survey, in 2015 an estimated 172,000 US residents were served by domestic wells exceeding the EPA’s enforceable limit of 4.0 mg F/L1. In addition to these implications with regard to high F areas, these results have potential impacts concerning areas with CWF and water F levels below 1.5 mg F/L. Individual-level F exposures are not known in CWF areas; additional fluoride exposures from foods, prescriptions, and dental products are not accounted for in estimates based on water alone. Water concentrations alone, especially in the US where access to fluoride in other products is high, may provide a significant underestimate of the actual exposures that can only be measured through urinary fluoride. Individual behaviours create a wide range of fluoride exposures; when these are combined with a universal intervention, it may result in higher-than-expected F exposures. A 1.63 IQ point decrease per mg F/L (95% CI -2.33, -0.93), although ostensibly minor, may have serious impacts upon populations. This metric would translate to an approximate 8-point discrepancy in IQ between those without fluoride exposure or low CWF exposure (< 0.7 mg/L) and those exposed to higher chronic fluorosis levels (~5 mg/L). According to Braun et al., a 5-point decrease in IQ in an entire population would nearly double the number of intellectually disabled people32.
Currently, no fluoride guidelines or recommendations are based on the risk of adverse neurocognitive outcomes. Those that do exist (based on fluorosis risk) do not appear to be enforced effectively to prevent against risks from either outcome, as previously demonstrated by the high number of residents in the US being exposed to high-risk F1,33 levels in water. The potential seriousness of these impacts and the ambiguity surrounding their scale for low F levels would justify further investigation. A need for more longitudinal studies investigating lower F levels, especially those in CWF areas of the US, would be especially useful to fully understand the implications of water fluoridation. Such longitudinal studies would require repeated as opposed to spot individual urinary fluoride measures from birth cohorts with consistent timing and confounder adjustment in order to more effectively and accurately gauge chronic exposure. According to a Health Canada expert panel, future studies should include detailed individual exposure profiles tracking all sources of fluoride and take into consideration potential confounders such as lead and arsenic and effect modifiers such as calcium or iodide34. Monitoring of such longitudinal data by responsible agencies should also be prioritized so that guidelines accurately reflect data in accordance with the available demonstrated evidence. For endemic areas, fluoride safety guidelines should integrate neurocognitive risks along with fluorosis risks and make similar adjustments regarding CWF areas as reliable data may become available in the future. Public health agencies can make evidence-based proposals to mitigate neurocognitive risks while advocating the appropriate dental usage. For example, policymakers may recommend topical-only fluoride treatments for young children and pregnant mothers in endemic areas.
Limitations
This umbrella review has been conducted to provide an overview of the current state of the research surrounding the association between fluoride exposure and children’s IQ. This review was limited by the presence of only one author and the resources available. This review is limited in its reproducibility and lacks a protocol registration due to being a narrative overview with quantitative synthesis as opposed to a full systematic analysis. These findings are limited by the previous research that has been conducted, which is limited in its generalizability due to an inadequate amount of research to fully understand the effects relevant to CWF and non-endemic fluorosis areas. Additionally, this synthesis is limited by the low number of high-quality systematic reviews and meta-analyses as well as potential redundancy in the findings because of high primary study overlap.
Conclusions
This umbrella review found significant evidence within the current body of literature demonstrating adverse effects of high F exposure on children’s IQ scores and cognition. Public health agencies around the world may need to more urgently address high F levels, especially in areas where guidelines are not adhered to in order to mitigate the potential impacts upon children’s health. Although this review was not intended to provide any risk-benefit analysis of water fluoridation, these findings may be useful to inform future decisions regarding the intervention for caries reduction. It should be acknowledged that there is a burden of proof on public health officials to ensure that the intervention of water fluoridation is fully safe. There is not yet conclusive evidence to support a statistically significant or clinically meaningful inverse association or a lack thereof at the commonly recommended CWF exposure levels. Therefore, public health agencies need to proceed with continued investigation to ensure that the intervention can be consistently carried out at levels with proven safety and efficacy.
Acknowledgements
I would like to express my sincere thanks to Dr. John Embil, Dr. Rae Spiwak, and Mr. Jeff Shaddock for their invaluable guidance and feedback on this research paper.
Supplementary Information
References
- US Department of Health and Human Services Federal Panel on Community Water Fluoridation. U.S. Public Health Service recommendation for fluoride concentration in drinking water for the prevention of dental caries. Public Health Rep. Vol. 130, pg. 318-331, 2015, https://doi.org/10.1177/003335491513000408. [↩] [↩] [↩] [↩]
- A.J. Rugg-Gunn, L. Do. Effectiveness of water fluoridation in caries prevention. Community Dent Oral Epidemiol. Vol. 40, pg. 55-64, 2012 https://doi.org/10.1111/j.1600-0528.2012.00721.x. [↩]
- US Environmental Protection Agency. Fluoride: exposure and relative source contribution analysis. https://www.epa.gov/sites/default/files/2019-03/documents/fluoride-exposure-relative-report.pdf, 2010. [↩]
- US Geological Survey. Fluoride in groundwater: too much or too little of a good thing? https://www.usgs.gov/news/comprehensive-assessment-fluoride-groundwater, 2020. [↩] [↩] [↩]
- Q. Q. Tang, J. Du, H. H. Ma, S. J. Jiang, X. J. Zhou. Fluoride and children’s intelligence: a meta-analysis. Biol Trace Elem Res. Vol. 126, pg. 115-120, 2008, https://doi.org/10.1007/s12011-008-8204-x. [↩]
- A. L. Choi, G. Sun, Y. Zhang, P. Grandjean. Developmental fluoride neurotoxicity: a systematic review and meta-analysis. Environ. Health Perspect. Vol. 120, pg. 1362-1368, 2012, https://doi.org/10.1289/ehp.1104912. [↩]
- Q. Duan, J. Jiao, X. Chen, X. Wang. Association between water fluoride and the level of children’s intelligence: a dose-response meta-analysis. Public Health Vol. 154, pg. 87-97, 2018, https://doi.org/10.1016/j.puhe.2017.08.013. [↩]
- Associated Press. Fluoride in drinking water poses enough risk to merit new EPA action, judge says. https://www.cnn.com/2024/09/25/health/epa-fluoride-drinking-water, 2024. [↩]
- H. Schoenbaum, M. Stobbe. RFK Jr. will tell CDC to stop recommending fluoride in drinking water. https://www.pbs.org/newshour/health/rfk-jr-will-tell-cdc-to-stop-recommending-fluoride-in-drinking-water, 2025. [↩]
- E. Aromataris, C. Lockwood, K. Porritt, B. Pilla, Z Jordan, editors. JBI Manual for Evidence Synthesis. https://synthesismanual.jbi.global, 2024. [↩]
- J. Bracchiglione, N. Meza, S Bangdiwala, E. N. de Guzmán, G. Urrutia, X. Bonfill, E. Madrid. GROOVE – Graphical Representation of Overlap for OVErviews. https://osf.io/u2ms4, 2022. [↩] [↩]
- National Toxicology Program. NTP monograph on the state of the science concerning fluoride exposure and neurodevelopment and cognition: a systematic review. NTP Monogr., 2024, https://doi.org/10.22427/NTP-MGRAPH-8. [↩] [↩] [↩] [↩] [↩] [↩] [↩] [↩]
- CASP Checklists. https://casp-uk.net/casp-tools-checklists/, 2025. [↩]
- N. Shaheen, A. Shaheen, A. Ramadan, M. T. Hefnawy, A. Ramadan, I. A. Ibrahim, M. E. Hassanein, M. E. Ashour, O. Flouty. Appraising systematic reviews: a comprehensive guide to ensuring validity and reliability. Front Res Metr Anal. Vol. 8, pg. 1268045, 2023, https://doi.org/10.3389/frma.2023.1268045. [↩]
- M. J. Page, J. E. McKenzie, P. M. Bossuyt, I. Boutron, T. C. Hoffmann, C. D. Mulrow, L. Shamseer, J. M. Tetzlaff, E.A. Akl, S. E. Brennan, R. Chou, J. Glanville, J.M. Grimshaw, A. Hróbjartsson, M. M. Lalu, T. Li, E. W. Loder, E. Mayo-Wilson, S. McDonald, L. A. McGuinness, L. A. Stewart, J. Thomas, A. C. Tricco, V. A. Welch, P. Whiting, D. Moher. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. Vol. 372, pg. 71, 2021, https://doi.org/10.1136/bmj.n71. [↩]
- K. Taylor, S. E. Eftim, C. A. Sibrizzi, R. B. Blain, K. Magnuson, P. A. Hartman, A. A. Rooney, J. R. Bucher. Fluoride Exposure and Children’s IQ Scores: A Systematic Review and Meta-Analysis. JAMA Pediatrics Vol. 179, pg. 282-292, 2025, https://doi.org/10.1001/jamapediatrics.2024.5542. [↩]
- B.P. Gopu, L.B. Azevedo, R.M. Duckworth, M.K.P Subramanian, S. John, F.V. Zohoori. The Relationship between Fluoride Exposure and Cognitive Outcomes from Gestation to Adulthood—A Systematic Review. Int. J. Environ. Res. Public Health. Vol. 20, pg. 22, 2022, https://doi.org/10.3390/ijerph20010022. [↩] [↩]
- F. Veneri, M. Vinceti, L. Generali, M. E. Giannone, E. Mazzoleni, L. S. Birnbaum, U. Consolo, T. Filippini. Fluoride exposure and neurodevelopment: Systematic review and dose-response meta-analysis. Environmental Research Vol. 221, pg. 115239, 2023, https://doi.org/10.1016/j.envres.2023.115239. [↩] [↩] [↩] [↩] [↩] [↩]
- J. V. Kumar, M. E. Moss, H. Liu, S. Fisher-Owens. Association between low fluoride exposure and children’s intelligence: a meta-analysis relevant to community water fluoridation. Public Health Vol. 219, pg. 73-84, 2023, https://doi.org/10.1016/j.puhe.2023.03.011. [↩] [↩] [↩] [↩] [↩] [↩]
- G. H. N. Miranda, M. O. P. Alvarenga, M. K. M. Ferreira, B. Puty, L. O. Bittencourt, N. C. F. Fangundes, J. P. Pessan, M. A. R. Buzalaf, R. R. Lima. A systematic review and meta-analysis of the association between fluoride exposure and neurological disorders. Scientific Reports Vol. 11, pg. 22659, 2021 https://doi.org/10.1038/s41598-021-99688-w. [↩] [↩] [↩] [↩] [↩] [↩]
- D.G. Altman, J.J. Deeks, D.L. Sackett. Odds ratios should be avoided when events are common. BMJ Vol. 317, pg. 7168, 1998 https://doi.org/10.1136/bmj.317.7168.1318. [↩]
- K. Taylor, S. E. Eftim, C. A. Sibrizzi, R. B. Blain, K. Magnuson, P. A. Hartman, A. A. Rooney, J. R. Bucher. Fluoride Exposure and Children’s IQ Scores: A Systematic Review and Meta-Analysis. JAMA Pediatrics Vol. 179, pg. 282-292, 2025, https://doi.org/10.1001/jamapediatrics.2024.5542. [↩] [↩] [↩] [↩] [↩] [↩] [↩] [↩] [↩]
- J. Cohen. Statistical Power Analysis for the Biomedical Sciences (2nd ed.). Hillsdale, NJ: Lawrence Erlbaum Associates, Publishers. 1988. [↩]
- A. Villa, M. Anabalon, V. Zohouri, A. Maguire, A. A. Franco, A. Rugg-Gunn. Relationships between fluoride intake, urinary fluoride excretion and fluoride retention in children and adults: an analysis of available data. Caries Res. Vol. 44, pg. 60-68, 2010, https://doi.org/10.1159/000279325. [↩] [↩]
- R. Green, B. Lanphear, R. Hornung, D. Flora, A. Martinez-Mier, R. Neufeld, P. Ayotte, G. Muckle, C. Till. Association Between Maternal Fluoride Exposure During Pregnancy and IQ Scores in Offspring in Canada. JAMA Pediatrics. Vol. 173, pg. 940-948, 2019, https://doi.org/10.1001/jamapediatrics.2019.1729. [↩]
- M. Bashash. D. Thomas, H. Hu, A. Martinez-Meir, B. N. Sanchez, N. Basu, K. E. Peterson, A. S. Ettinger, R. Wright, Z. Zhang, Y. Liu, L. Schnaas, A. Mercado-García, M. M. Téllez-Rojo, M. Hernández-Avila. Prenatal Fluoride Exposure and Cognitive Outcomes in Children at 4 and 6-12 Years of Age in Mexico. Environ. Health Perspect. Vol. 125, pg. 97017, 2017, https://doi.org/10.1289/EHP655. [↩]
- J. V. Kumar, M. E. Moss, H. Liu, S. Fisher-Owens. Association between low fluoride exposure and children’s intelligence: a meta-analysis relevant to community water fluoridation. Public Health Vol. 219, pg. 73-84, 2023, https://doi.org/10.1016/j.puhe.2023.03.011. [↩]
- National Toxicology Program. NTP monograph on the state of the science concerning fluoride exposure and neurodevelopment and cognition: a systematic review. NTP Monogr., 2024, https://doi.org/10.22427/NTP-MGRAPH-8. [↩]
- K. Taylor, S. E. Eftim, C. A. Sibrizzi, R. B. Blain, K. Magnuson, P. A. Hartman, A. A. Rooney, J. R. Bucher. Fluoride Exposure and Children’s IQ Scores: A Systematic Review and Meta-Analysis. JAMA Pediatrics Vol. 179, pg. 282-292, 2025, https://doi.org/10.1001/jamapediatrics.2024.5542. [↩]
- A. J. Malin, S.P. Eckel, H. Hu, E. A. Martinez-Mier, I. Hernandez-Castro, T. Yang, S.F. Farzan, R. Habre, C. V. Breton, T. M. Bastain. Maternal Urinary Fluoride and Child Neurobehavior at Age 36 Months. JAMA Pediatrics. Vol. 7, pg. e2411987, 2024, https://doi.org/10.1001/jamanetworkopen.2024.11987. [↩]
- R. Hefferon, D. E. Goin, J. A. Samat, A. E. Nigra. Regional and racial/ethnic inequalities in public drinking water fluoride concentrations across the US. J Expo Sci Environ Epidemiol. Vol. 34, pg. 68-76, 2024 https://doi.org/10.1038/s41370-023-00570-w. [↩]
- J.M. Braun. Early Life Exposure to Endocrine Disrupting Chemicals and Childhood Obesity and Neurodevelopment. Nat Rev Endocrinol. Vol. 13, pg. 161–173, 2016, https://doi.org/10.1038/nrendo.2016.186. [↩]
- R. Hefferon, D. E. Goin, J. A. Samat, A. E. Nigra. Regional and racial/ethnic inequalities in public drinking water fluoride concentrations across the US. J Expo Sci Environ Epidemiol. Vol. 34, pg. 68-76, 2024 https://doi.org/10.1038/s41370-023-00570-w. [↩]
- Health Canada. Expert panel meeting on the health effects of fluoride in drinking water: Summary report. https://www.canada.ca/en/health-canada/services/environmental-workplace-health/reports-publications/water-quality/expert-panel-meeting-effects-fluoride-drinking-summary.html, 2023. [↩]


