
Inaya Chowdhury1, Olabimpe Olayinka2
1 Brooks DeBartolo Collegiate High school, Florida, USA
2 University of Cambridge, UK
Abstract
This research focuses on cancer patients who struggle with mental health and biotechnological solutions that address these concerns. Cancer treatment has developed vastly over the years and saves countless lives annually. However, a commonly overlooked issue is the mental health concerns that cancer patients struggle with. The profound psychological toll of a diagnosis, including anxiety, depression, fear of recurrence, etc., is often overlooked. These can influence the possibility of poor patient outcomes, reduced quality of life, and low rates of treatment adherence. While traditional psychological approaches are effective, they tend to face gaps in accessibility, scalability, and integration with standard oncology care. To address this issue, this paper reviews recent literature (2020 – 2025) on biotechnological interventions; however, older studies are also included to highlight that the neglect of mental health concerns is a longstanding and persistent issue. This analysis focuses on digital platforms, AI-powered tools, and wearable devices, identifying scalable and personalized approaches. Findings suggest that a digital app made to help reduce depression and anxiety, and wearable technology to help monitor psychological distress, can help support mental well-being. We also address concerns regarding data privacy and ethics surrounding the use of these interventions. Overall, this paper highlights the significant impacts mental health has on cancer patients and how the strategic integration of these solutions can help bridge the gap in cancer care, providing support during a difficult cancer journey.
Introduction
Background on Cancer and Its Impact
Cancer is one of the leading causes of death worldwide and a significant health challenge of our time, affecting millions of people around the globe1. In 2022, there were around 20 million new cancer cases and 9.7 million deaths, highlighting the widespread prevalence and high mortality rates2. Regardless of the sobering statistics, over the past three decades, global cancer outcomes have improved markedly, with about a 40% overall decline in mortality and almost a 50% increase in the five-year survival rate across many cancer types2. These advances, driven by remarkable advancements in cancer prevention, vaccination, and treatment (including targeted medicine, immunotherapies, and innovative surgical techniques), are revolutionizing cancer diagnosis from a once untreatable condition to one that, for many patients, can now be therapeutically managed, and in some cases potentially cured.
However, considering that the primary goal of cancer therapy is prolonging life or survival3, the patient’s mental health, from diagnosis through to survivorship or end of life, though equally important, is often overlooked. The psychological toll of receiving a cancer diagnosis and the subsequent treatment can be profound4. For instance, Fisch et al. (2014) reported significant fatigue in ambulatory patients with common solid tumors, while studies by McManus et al. (2019) showed that approximately 25-35% of cancer patients experience clinically significant depression, and up to 45% report symptoms of anxiety during or after treatment5,6. Furthermore, nearly 1 in 3 cancer patients experience distress severe enough to impair daily functioning, yet many of these individuals remain undiagnosed and untreated7. Traditional oncology care has historically been ill-equipped to address these mental health needs holistically, leaving a critical gap in comprehensive cancer treatment.
Mental health distress has been identified as the 6th vital sign in cancer treatment. Reports from studies Chen et al. (2021) and McManus et al. (2019) have shown that 1 in 3 cancer patients experience heightened distress, which often translates to lesser treatment adherence, leading to lower survival and worsening patient outcomes.8,6Although international guidelines such as the ASCO (American Society of Clinical Oncology), NCCN (National Comprehensive Cancer Network), and the ESMO (European Society of Medical Oncology) recommend the integration of psychosocial assessment and palliative care into cancer treatment, the uptake of these guidelines remains inconsistent across different countries, creating a disparity in cancer care and subsequently poor implementation.
A study carried out by Yun-He Wang et al (2020) investigated the impact of psychological distress, particularly depression and anxiety arising from a cancer diagnosis, on patient outcomes. They found that these mental health conditions are linked to higher risks of cancer-specific mortality and overall mortality9. However, depression and anxiety did not increase the risk of cancer incidence and were more closely related to cancer-specific mortality than to general survival. Therefore, these findings suggest that effectively managing mental health conditions arising from a cancer diagnosis can help to lower cancer-specific mortality.
Notably, specific cancers corresponding with depression and anxiety show varying associations. For example, lung, prostate, oral cavity, and skin cancers lead to a higher incidence risk; while lung, bladder, breast, colorectal, hematopoietic, kidney, and prostate cancers are linked with higher cancer-specific mortality. In addition, lung cancer patients with depression or anxiety risk an increased all-cause mortality. Together, these findings highlight the immense impact of psychological distress on cancer development and outcomes, underscoring the clinical importance of early detection and management of depression and anxiety in cancer patients9.
The Critical Need for Mental Health Support in Oncology
A cancer diagnosis often triggers major psychological distress, including anxiety, depression, and a persistent fear of recurrence (FOR), which can impact a patient’s emotional state long after treatment ends. This distress is not only a side effect; it directly affects a patient’s quality of life, their ability to adhere to complex treatment regimens, and even their long-term survival rates10,11. While psychosocial care is available, traditional models often face significant roadblocks related to accessibility, cost, and scalability12,13. This leaves a critical gap between the mental health needs of cancer patients and the support they receive, emphasizing the urgent need for innovative and more effective solutions.
Introduction to Biotechnological Interventions
In this context, innovative biotechnological interventions offer a promising path forward. In this paper, these interventions encompass digital health platforms, wearable devices, and biomarker-based strategies. These tools leverage advancements in data science and technology to provide scalable, accessible, and personalized support via mobile apps with features ranging from mood trackers that offer real-time cognitive behavioural therapy to wearable sensors that monitor physiological markers of stress and anxiety and alert the patients in real time. Integrating these innovative biotech solutions into cancer care may foster the potential to bridge the existing gaps in psychosocial care and to enhance the management of mental health in oncology. While traditional face-to-face therapy is effective, it often places an unintended physical burden on cancer patients who may struggle to travel to therapy clinics due to treatment-related fatigue or immunosuppression. This further emphasizes the need for more accessible, biotechnical interventions, which address this issue by providing remote therapeutic support, such as mobile health platforms or digital health interventions (DHIs) 14.
Research Aim and Objectives
This research aims to identify the gaps between the mental health needs of cancer patients and the technological support currently available. To accomplish this, the study will investigate the following research question: What innovative biotechnological solutions can be explored and implemented to provide holistic mental health support for cancer patients? The objectives of this literature review are to: analyze the current landscape of mental health challenges faced by cancer patients; critically review existing literature on biotechnological interventions for mental health; and identify specific innovative biotechnological solutions with the potential to enhance mental health support in oncology.
Scope of the Literature Review
This review synthesizes evidence from peer-reviewed journals, focusing on psychosocial, digital, and biomarker-based strategies. Emphasis is placed on high-quality studies, particularly those published in Q1 journals, to ensure that conclusions are grounded in the most current and rigorous scientific evidence.
Methodology: Understanding the Evidence
To get a clear picture of how biotechnological solutions support mental health in oncology, we undertook a systematic review of recent academic literature. This involved a rigorous process of searching, selecting, and synthesizing relevant studies to ensure a comprehensive and unbiased overview.
Search Strategy and Criteria
A structured literature search was conducted across major academic databases, including PubMed, Google Scholar, and Web of Science, chosen for their comprehensive coverage of peer-reviewed scientific publications. A combination of keywords—“cancer mental health,” “biotechnological interventions,” and “digital mental health”—was used in various combinations to capture the study’s core concepts while maintaining specificity.
Inclusion criteria were defined as follows to ensure focus and rigor. The main use of studies published between 2020 and 2025 was included to capture the most recent advancements in this rapidly evolving field, with the addition of older papers to show the concern, but the lack of action to help prevent these problems. Eligible papers directly addressed biotechnological interventions designed to support the mental health of adult cancer patients. Studies limited to physical health outcomes or pediatric populations were excluded. Preference was given to articles published in Q1 journals, reflecting high standards of research quality, peer review, and scientific credibility.
Paper Selection
The selection process was conducted in two phases to maximize efficiency and accuracy. We initially reviewed the titles and abstracts of all identified papers. This first pass allowed us to filter out studies that did not meet our inclusion criteria, such as those unrelated to cancer, mental health, or biotechnological interventions. Papers deemed potentially relevant were then subjected to a detailed full-text review. This in-depth examination confirmed whether each study met all the inclusion criteria. For instance, we confirmed that the intervention was indeed biotechnological (e.g., app-based, wearable-integrated), targeted mental health, and involved adult cancer patients.
Following this selection process, ten key research papers were chosen for detailed analysis. Crucially, at least five of these selected papers were original research articles, presenting new empirical findings, rather than reviews or commentaries. This ensured that the synthesis was grounded in primary evidence.
Literature Synthesis
The synthesis of the selected literature involved a systematic approach to extract and categorize essential information from each study. For every paper, we carefully documented what specific questions did the researchers aim to answer. What were the main results and conclusions drawn from the study? What kind of biotechnological interventions were utilized? This included categorizing them as mobile applications, wearable device integrations, virtual reality, telehealth platforms, or other digital tools. Which specific mental health challenges (e.g., anxiety, depression, distress, fatigue, quality of life) were the interventions designed to address?
We critically evaluated the methodology and execution of each study, noting their strengths (e.g., large sample size, randomized controlled design) and limitations (e.g., small sample size, lack of long-term follow-up, high heterogeneity, or potential for bias). Through this detailed, systematic study, we aimed to provide a comprehensive and nuanced understanding of the current landscape of biotechnological interventions for mental health in oncology. The information synthesized from these critically reviewed reports forms the basis for our overall findings and recommendations.
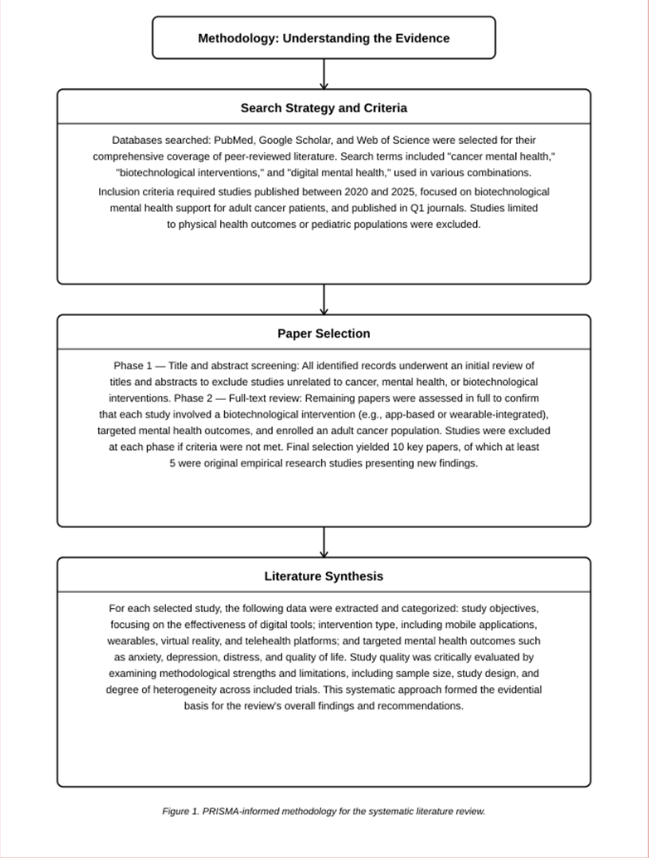
(Note: Outlines the Methodology section following 3 main steps: Search Strategy, Paper Selection, and Literature Synthesis)
Literature Review
| Author (Year) | Intervention Type | Study Design | Key Findings | Strengths & Limitations |
| Wu et al. (2025) | Digital Mental Health Interventions (DMHIs) | Meta-analysis of 22 Randomized Controlled Trials (RCTs) | Digital interventions in cancer patients had a non-significant overall impact, but are beneficial when applied to specific durations. | Large sample size, but has a high variety in study designs and outcomes. |
| Kim et al. (2025) | E-health Interventions and Mobile Applications | Systematic Review and Meta-analysis | There was a significant reduction in anxiety levels in breast cancer patients who used e-health interventions. | Provides e-health effectiveness for anxiety reduction, but focuses almost exclusively on breast cancer, limiting broader application. |
| Zhong et al. (2025) | Digital Mental Health Interventions (DMHIs) | Umbrella Review of 78 Systematic Reviews | There is a general effectiveness of digital health interventions, especially through the use of websites and smartphones, in improving the mental well-being of cancer patients. | Strongly confirms the effectiveness of digital tools in improving the mental health of cancer patients, but is limited by inconsistencies in some underlying research and a lack of data concerning older adults. |
| Pappot et al. (2025) | Wearable Technology | Clinical Analysis | Through the use of wearable technology, the heart rate variability (HRV), activity levels, and sleep patterns of cancer patients can be efficiently tracked and managed. | Provides real-world evidence of technological usage during treatment but uses a small, localized sample from Denmark, which limits generalizability. |
| Mitsis et al. (2025) | E-Health Interventions and Mobile Health Apps | Systematic Review | Confirmed mobile health apps have statistical significance in reducing anxiety levels prevalent in cancer patients. | Uses high-quality PRISMA standards and includes 2,476 patients, providing supportive evidence, but its focus is limited to breast cancer, which would not apply to other types of cancer. |
| Fortunato et al. (2025) | Wearable remote patient monitoring RPM | Observational Secondary Analysis | Confirms the high prevalence of wearable technology in remote patient monitoring (RPM) of sleep to be 79%. | Demonstrates the convenience of wearable technology, but the data is derived from cardiac patients rather than cancer patients specifically. |
| Tolboom et al. (2024) | Theranostics | Experts Reviews and Perspectives | Identifies theranostics as a therapeutic approach and integrated model using PET scans and molecular targets for combined diagnosis and therapy. | Establishes a medical roadmap for pharmacogenomics and personalized care, but is still largely conceptual. |
| Chow & Li (2024) | Telehealth Platforms and Digital Applications | Clinical Study | Emphasizes the necessity of disclosing the limitations of AI and digital applications to maintain trust and ensure user privacy and security. | Addresses the ethical requirements for AI in hospitals, though the study highlights a need for more data on long-term patient engagement. |
| Amiri et al. (2024) | Mental Health Screening | Meta-analysis | Confirmed a 23% prevalence rate for clinical anxiety and mental health issues among cancer patients. | Establishes a 23% anxiety prevalence baseline, though results are hindered by the high variety of screening tools used across different clinics. |
| Wang et al. (2020) | Psychological Distress Monitoring | Meta-analysis of Cohort Studies | Psychological distress is associated with increased cancer-specific mortality. | Shows a correlation between psychological distress and cancer-specific mortality, but can not strictly prove that distress directly causes death. |
Prevalence and Types of Psychological Distress
A cancer diagnosis is a life-altering event that often triggers a variety of psychological distress, extending beyond the physical effects of the disease and its treatment. Common mental health disorders among cancer patients include anxiety disorders, depression, fear of recurrence or progression, post-traumatic stress disorder (PTSD) related to diagnosis and treatment, and significant body image concerns.
Anxiety disorders are pervasive. A recent meta-analysis indicated that approximately 23% of cancer patients experience mental health disorders, including anxiety15. Prevalence rates of mental health disorders in cancer can vary by gender; going as high as 31% in women compared to 20% in men, and differ across cancer types, such as ovarian, breast, and lung cancers where prevalence rates range from 8% to 24%, depending on the assessment instrument, cancer type, and treatment phase16. Notably, anxiety prevalence is highest during active treatment, with reported rates of 14% identified through diagnostic interviews and 27% through self-report instruments16.
The fear of recurrence (FOR) is one of the most persistent and debilitating psychological challenges many cancer patients face. A recent analysis of published studies reported that over half (59%) of cancer survivors and patients experience at least a moderate level of FOR, and approximately one in five (19%) experience severe levels17. Younger individuals and women are particularly vulnerable17. In addition, the traumatic nature of a cancer diagnosis and subsequent intensive treatments can also lead to Post-Traumatic Stress Disorder (PTSD). The prevalence of full PTSD ranges from 3–4% in recently diagnosed patients among those evaluated after treatment18. When considering PTSD-like symptoms (those that do not meet full diagnostic criteria), prevalence rates increase dramatically in cancer patients to as high as 45%19.
Body image concerns and reduced self-esteem are common consequences of a cancer diagnosis and its treatments, particularly surgery (e.g., mastectomy). For instance, 68% of patients with head and neck cancer report body image concerns, with prevalence increasing significantly from pre- to post-treatment20. Similarly, 44% of women with breast cancer report that the disease negatively impacted their body image21. The cumulative burden of body image disturbance, alongside other psychiatric disorders, underscores the widespread psychological distress experienced across adult cancer populations22.
Impact of Mental Health on Cancer Outcomes
The psychological distress that cancer patients experience is not only an emotional burden but also has a significant impact on numerous aspects of their cancer journey and overall well-being.
Diminished mental health directly translates to a reduced quality of life, affecting simple daily activities. Such as functioning, social interactions, and overall well-being23,24. Patients who experience significant distress often report lower life satisfaction and struggle with everyday tasks25.
Psychological distress, such as anxiety and depression, can significantly hinder a patient’s adherence to a complex medical regimen, including chemotherapy, radiation therapy, and medication schedules. Non-compliance can lead to substandard treatment outcomes and uncontrolled disease progression.
Emerging research suggests potential links between mental health, treatment effectiveness, and even survival rates. People with serious mental illnesses have been shown to have lower cancer survival rates than the general population, with challenges often appearing during their treatment rather than from delayed diagnosis or screening26. For instance, individuals with serious mental illness had a 74% higher risk of death over a 4–5-year follow-up period compared to cancer patients without a history of mental illness26.
The mental health challenges faced by cancer patients also have significant spill-over effects on their family and friends. Cancer caregivers frequently experience substantial emotional, physical, and financial stress. A systematic review reported a pooled prevalence of depressive symptoms among cancer caregivers to be 25.14%27. Likewise, many caregivers report severe emotional stress (50%) and financial strain (25%), with 75.6% stating that being a cancer caregiver negatively impacted their mental health, often due to anxiety (37.29%) or depression (33.9%)28.
Gaps in Current Mental Health Support Mechanisms
Despite the clear need, current mental health support mechanisms for cancer patients remain insufficient, with several critical gaps.Geographic barriers, specifically in rural or underserved areas, limit access to specialized psychosocial care. Financial restraints, including insurance coverage and high out-of-pocket costs, also create significant challenges for many patients29. Traditional therapy models, while effective, are resource-intensive and struggle to meet the prevalent demand. The limited number of trained psycho-oncology professionals means long waiting lists and limited capacity for individualized care30. A pervasive societal stigma surrounding mental illness often discourages cancer patients from acknowledging psychological distress or attempting to seek professional help. Patients may fear being judged as weak or “not coping” if they admit to mental health struggles31. Mental health services are often siloed from medical oncology, resulting in missed opportunities for early screening, timely intervention, and integrated care. This fragmented approach can result in delay or uncoordinated care for patients who experience psychological distress. Guidelines recommend routine screening, but fragmented implementation and referral pathways remain a challenge.32. Despite the growing availability of digital tools in mental health care, there are still challenges in ensuring consistent engagement. For instance, a meta-analysis of 22 randomized controlled trials (RCTs) exploring digital interventions in cancer patients noted non-significant overall effects on depression and anxiety, but suggested potential benefits for interventions tailored to specific durations (e.g., interventions under 1 month significantly reduced anxiety)33.
NHS/NIMH Guidelines and Policies Guiding Mental Health Care in Cancer Patients
In the United Kingdom, the National Health Service (NHS) guidelines and policies emphasize the integration of mental health support and psychological well-being into comprehensive cancer care. For instance, the NHS Long-Term Plan focuses on the need for personalized care, including mental and emotional needs, as part of comprehensive cancer services. Services such as Macmillan Cancer Support, a key partner of the NHS, provide extensive resources and information on mental health support for cancer patients, advocating for access to various forms of assistance, including talking therapies, self-help groups, and referrals to specialists like counselors, clinical psychologists, and psychiatrists.
Likewise, in the United States of America, the National Institute of Mental Health (NIMH) recognizes the significant mental health challenges experienced by cancer patients. NIMH-supported research reports that a considerable number of cancer patients suffer from mental health conditions, like depression and anxiety. The research highlights how these conditions can adversely affect treatment adherence, patients’ overall well-being, and potentially cancer progression.
While the NIMH does not explicitly provide a single detailed guideline equivalent to the NHS Long-Term Plan, it offers extensive resources and information on mental health conditions, including those commonly experienced by individuals with chronic illnesses like cancer. The NIMH also supports research to better understand and address the mental health needs of cancer patients and survivors. Through consolidated efforts in research, advocacy, and community awareness, the NIMH promotes a comprehensive model of care that integrates psychological well-being into cancer management.
Limitations of Current NHS Policies/Guidelines:
Despite these frameworks, practical limitations persist. While policies exist, the actual integration of mental health screening and support into routine oncology care can vary significantly across different NHS Trusts and clinics. This leads to a “postcode lottery” in access to care. The demand for mental health services often outstrips available resources, leading to long waiting lists for talking therapies and specialist psychological support. This can delay timely interventions during critical stages of a patient’s cancer journey. While guidelines encourage routine screening for distress, systematic and standardized processes for identifying psychological distress early and ensuring timely referrals are not always consistently applied. Consequently, many patients’ psychological needs remain unrecognized until they escalate.
Even with available services, patients may not be fully aware of the mental health support options or may still face internal and external stigma that deters them from seeking help. The “warrior mentality” some patients adopt can further discourage them from admitting vulnerability and seeking mental health support34. Achieving truly integrated care, where mental health professionals are seamlessly embedded within oncology teams, remains a significant challenge. This requires systemic reforms in funding, training, and care pathways.
In summary, despite growing recognition of the need for mental health support in oncology, several critical limitations persist. Implementation of mental health screening and services is inconsistent, leading to unequal access depending on location. Resource shortages often result in long wait times for therapy and specialist support, delaying care during key phases of treatment. While guidelines promote early distress screening, they are not uniformly applied, allowing many cases to go undetected until severe. Additionally, stigma and lack of awareness prevent some patients from seeking help, particularly those who feel pressure to remain strong. Finally, full integration of mental health professionals into oncology teams remains a systemic challenge due to funding gaps and fragmented care pathways.
These limitations underscore the persistent gap between the acknowledged need for mental health support in oncology and the effective delivery of such care through traditional methods, paving the way for innovative solutions. Dealing with cancer isn’t just a physical battle; it takes a huge toll on a person’s mental health, too. People with cancer face higher risks of psychiatric disorders and even self-harm22.
Thus, this research focuses on highlighting innovative ways to leverage technology in supporting the emotional well-being of cancer patients. This research examines how innovative biotechnological interventions—such as digital health platforms, wearable devices, and biomarker-based tools—can provide more accessible, personalized, and effective mental health support throughout the cancer journey.
Existing and Emerging Biotechnological Interventions for Mental Health
The landscape of mental health support for oncology patients is being transformed by a variety of existing and emerging biotechnological interventions. These innovations leverage digital platforms, wearable devices, and biological insights to offer more comprehensive and personalized care.
Digital Mental Health Interventions (DMHIs)
Digital Mental Health Interventions, or DMHIs, are becoming increasingly prominent in supporting the psychological needs of cancer patients. They offer a flexible, accessible, and sustainable way to deliver mental health care. For instance, an umbrella review of 78 systematic reviews found that digital health interventions are generally effective in improving mental health outcomes for cancer patients, with websites and smartphone apps being the most commonly used modalities. Depression was the most frequently addressed condition35.
Therapeutic apps designed for cancer patients often incorporate evidence-based techniques like Cognitive Behavioral Therapy (CBT), mindfulness exercises, and psychoeducation. These apps can feature tools for mood tracking, guided meditation sessions, and journaling, allowing patients to monitor their emotional state and engage in self-help strategies. For example, a systematic review and meta-analysis focusing on breast cancer patients showed that e-health interventions significantly reduced anxiety (Standardized Mean Difference [SMD] = -0.80, 95% CI: -1.33 to -0.27; p < 0.01) and depression (SMD = -0.74, 95% CI: -1.40 to -0.09; p = 0.026)36. The benefits of mobile applications include their widespread accessibility, providing support anytime, anywhere. They offer immense convenience for patients who may face accessibility issues or live far from specialized mental health services. Furthermore, they can be a cost-effective alternative to traditional in-person therapy37,38. Evidence supports their effectiveness: a systematic review and meta-analysis in breast cancer patients found that e-health interventions, including mobile apps, significantly reduced anxiety (Standardized Mean Difference [SMD] = -0.80; p < 0.01) and depression (SMD = -0.74; p = 0.026), while improving quality of life39. Mobile apps demonstrated statistical significance in reducing anxiety in subgroup analyses within this review.
Examples of relevant Digital Applications
Several applications show promise in this field. For instance, the Living Well App focuses on personalized CBT, while DigiBioMarC and TOGETHERCare integrate wearable data to Over a one‑month pilot, the apps achieved high adherence (patients ~86%, caregivers ~84%) for symptom and wellbeing tracking—demonstrating feasibility for real‑time emotional and health monitoring. HealthUnlocked is a moderated peer-support network where cancer patients can join communities, share experiences, access tailored educational content, and receive emotional validation from others with similar diagnoses. War on Cancer is a social app created to help cancer survivors connect, share personal stories, and support one another in a stigma-free environment. Its design aims to foster emotional resilience and community engagement for those navigating the cancer journey.
Telehealth involves delivering healthcare services remotely, including online therapy sessions and virtual support groups. This means patients can connect with mental health professionals from the comfort of their homes, reducing the burden of travel and appointments during treatment. The main advantages of telehealth platforms are their ability to overcome geographical barriers, making specialized cancer mental health support available to patients in rural or underserved areas. They also provide increased access to specialists who might otherwise be unavailable locally, ensuring that patients receive expert care regardless of their location (Telemedicine in Oncology: Benefits and Challenges). AI-powered chatbots are emerging as tools to provide immediate support, information, and even preliminary mental health assessments. They can offer instant responses to common questions, guide patients through relaxation techniques, or provide relevant educational content. However, their use comes with significant ethical considerations and limitations.
A key concern is ensuring data privacy and security, as these systems handle sensitive patient information40. There are also limitations in their ability to truly understand complex human emotions and provide nuanced, empathetic responses. Research has highlighted limitations, such as potential for algorithmic bias leading to discriminatory or inadequate advice, and the risk of therapeutic misconception, where users overestimate the chatbot’s capabilities. Therefore, these chatbots must disclose their AI nature to users to maintain trust40.
Wearable Technology and Biometric Monitoring
Wearable technology offers a unique opportunity to monitor a patient’s physiological state in real-time, providing valuable insights into their mental well-being. Devices like smartwatches and fitness trackers can continuously capture a wealth of biometric data, including heart rate variability (HRV), sleep patterns, and activity levels. These seemingly basic metrics can reveal a lot about a person’s stress and emotional state41. Changes in HRV can indicate increased stress or anxiety, while disrupted sleep patterns are often associated with depression. By continuously monitoring these physiological responses, healthcare providers and patients can gain real-time insights into mental health fluctuations. This allows for early detection of distress signals, enabling timely interventions.Collecting real-time data from wearable devices is highly valuable for tailoring support based on an individual’s physiological responses42. If a wearable detects a significant increase in stress indicators, the connected app could automatically suggest a brief relaxation exercise or prompt the user to journal about their feelings. This proactive and personalized approach aims to empower patients to manage their mental health effectively.
Biofeedback Systems take real-time monitoring a step further by training patients to control their physiological responses consciously. Through visual or auditory feedback, patients learn to regulate bodily functions like heart rate, muscle tension, or skin temperature, which are often involuntary responses to stress and anxiety. Studies suggest biofeedback can help manage stress and anxiety symptoms, and even chemotherapy-related side effects like nausea. Devices & Data Collected are helpful because wearables gather data like heart rate variability and sleep, now used by over 79% of providers for remote patient monitoring43. Real-time Monitoring is used to help detect early signs of stress or depression, allowing for timely interventions. Personalized Interventions are apps that respond to stress indicators with relaxation suggestions or journaling prompts. Biofeedback Systems teach patients to control physical responses to stress, improving mental well-being and reducing treatment-related side effects.
Below is a summarized chart of how wearable technology and biometric monitoring support mental health care in cancer patients:
| Category | Purpose & Benefits |
| Biofeedback Systems | Helps patients manage physical stress responses (e.g., anxiety, nausea) through training. |
| Personalized Interventions | Apps deliver exercises or prompts when stress markers rise, offering tailored support. |
| Real-Time Monitoring | Tracks HRV and sleep to detect early signs of stress or depression for timely intervention. |
| Devices & Data | Smartwatches and trackers collect HRV, sleep, and activity data. |
Biomarker-Based Strategies
Beyond digital and wearable tools, advancements in understanding the underlying molecular mechanisms of mental health are opening new avenues for biomarker-based strategies in oncology. Neuroimaging (e.g., fMRI, PET): Techniques like functional Magnetic Resonance Imaging (fMRI) and Positron Emission Tomography (PET) can help identify neural correlates of distress or treatment response. For instance, research using fMRI has shown that chemotherapy can lead to rapid and widespread changes in brain connectivity in breast cancer patients, particularly in regions linked to memory and decision-making, which could explain “chemo brain”44. Understanding these changes can help develop targeted interventions. PET scans are also gaining traction in neuro-oncology for both diagnosis and therapy, paving the way for integrated approaches45.
Researchers are exploring genetic predispositions or biological indicators (proteins, genes) of mental health issues in cancer patients. This involves looking at how individual genetic makeup or specific protein expressions might make someone more vulnerable to depression or anxiety during their cancer journey. Identifying these markers could lead to proactive screening and preventative strategies. Pharmacogenomics is a field focused on tailoring psychiatric medication based on an individual’s genetic profile. Since cancer treatments can interact with psychiatric medications, understanding a patient’s genetic response to drugs can optimize prescribing, ensuring greater efficacy and minimizing adverse side effects. This personalized medicine approach can be crucial for managing complex medication regimens in cancer patients.
While traditionally used in areas like neuro-oncology for integrated diagnosis and therapy of tumors45, the concept of “theranostics” holds potential for mental well-being too. This would involve using a diagnostic tool to identify specific mental health needs or biological markers, and then immediately following up with a tailored therapeutic intervention, all based on the same or analogous molecular targets. For instance, if a specific biomarker indicates a high risk for treatment-induced anxiety, a targeted intervention (pharmacological or digital) could be initiated promptly. This integrated diagnostic and therapeutic approach is still largely conceptual in mental health, but offers an exciting future direction.
Innovative Biotech Solutions for Mental Health in Oncology
Recent advancements in biotechnology are creating new opportunities to enhance mental health support for cancer patients. One promising direction is the integration of digital mental health interventions (DMHIs) with data collected from wearable devices.
Integrated Digital and Wearable Platforms
Imagine combining helpful mental health apps with data from wearable devices like smartwatches. This creates a powerful system that can offer more personalized and proactive support. Digital mental health interventions (DMHIs) are already great at helping with things like depression and anxiety46,35. When we add wearables, these tools become incredibly responsive.
For example, an app could dynamically adapt its content by recommending a guided meditation, mindfulness practice, or cognitive behavioural therapy (CBT) exercise in response to real-time physiological signals. Elevated heart rate variability might prompt stress-management support, while poor sleep data could trigger reminders for relaxation or improved sleep hygiene strategies. Over time, these integrated systems can also generate valuable insights into trends in a patient’s mental health, providing a more holistic view of well-being.
This model functions much like a personalized digital mental health coach—delivering the right support at the right moment, and empowering both patients and healthcare providers to act on early signs of psychological distress. This personalized approach means support isn’t just generic; it’s delivered precisely when and how it’s most needed.
Biotech’s Role in Psychosocial Oncology Programs
Biotechnology can also significantly boost existing psychosocial oncology programs. These programs are essential because so many cancer patients face mental health challenges47,48. Digital platforms can make it simpler for patients, caregivers, and healthcare providers to connect. Secure messaging, virtual support groups, and telehealth appointments can remove geographical barriers and make it easier to access mental health professionals. This is a huge benefit for patients who might have trouble traveling or live in rural areas. When we collect anonymous data from these integrated platforms, we get valuable insights into what’s working in psychosocial programs. By looking at how patients engage, how their symptoms change, and what the outcomes of interventions are, we can figure out what’s most effective and where we can improve. This helps us continually refine programs, making sure they’re based on evidence and truly meet the evolving needs of cancer patients. For example, if data shows anxiety spikes during certain treatment phases, programs can proactively offer targeted support at those times. This data-driven approach helps us rethink mental health in cancer survivorship, moving towards more dynamic and responsive care49.
Ethical Considerations and Challenges
While innovative biotechnological solutions hold great promise for supporting the mental health of cancer patients, their implementation raises several important ethical considerations. Digital tools handle highly sensitive health information, making robust safeguards essential. Ensuring 27% data confidentiality requires stringent privacy protections, clear consent processes, and 45% transparent policies regarding data use and storage. Without these, patient trust and 27%professional integrity may be compromised. Increasing reliance on digital technologies risks exacerbating healthcare inequalities. Not all patients have access to smartphones, stable internet connections, or the digital literacy needed to engage with these tools. To prevent disparities in mental health support, strategies must include equitable access, the provision of low-tech alternatives, and resources to build digital capacity where needed.
Technological innovation often advances more rapidly than regulatory frameworks. Establishing clear guidelines for the development and clinical application of digital mental health tools is vital. This includes rigorous evaluation, such as randomized controlled trials, to ensure safety, efficacy, and suitability for oncology populations35. Regulatory systems must adapt to the pace of innovation, as seen with emerging technologies such as theranostics in neuro-oncology45. Although digital tools can provide scalable and convenient support, they cannot substitute the empathy and nuanced care offered by healthcare providers, therapists, and support networks. Biotechnological solutions should therefore complement, rather than replace, human-centered care. Striking a balance between digital convenience and authentic personal connection remains a key ethical challenge50.
Conclusion
Summary of Key Findings
Living with cancer places a significant and often overwhelming burden on a patient’s mental health. Our review consistently shows that psychological distress, including anxiety (up to 31% prevalence), depression (8-27% prevalence), fear of recurrence (59% moderate, 19% high), and PTSD-like symptoms (45%), is highly prevalent among cancer patients19,16,17. This distress isn’t just an emotional side effect; it profoundly impacts their quality of life, adherence to treatment, and even overall survival23,24. Sadly, traditional mental health support often falls short due to accessibility issues, scalability challenges, societal stigma, and a lack of integration with oncology care.
However, our exploration highlights the remarkable potential of biotechnological interventions to bridge these existing gaps. We’ve identified several promising solutions that are already making a difference or show immense future promise: Digital Mental Health Interventions (DMHIs), particularly mobile applications and telehealth platforms, offer accessible, convenient, and cost-effective support37,38. Studies show they can significantly reduce anxiety (e.g., SMD = -0.80 for e-health in breast cancer) and depression51. AI-powered chatbots also offer immediate, albeit limited, support. Wearable technology and biometric monitoring enable real-time insights into a patient’s physiological state, allowing for personalized interventions. With over 79% of patients now using remote patient monitoring, these tools are becoming increasingly integrated into care, offering proactive support based on data like heart rate variability and sleep patterns43. Biomarker-based strategies, while still emerging in mental health oncology, hold the key to truly personalized care. Neuroimaging, genomic markers, and pharmacogenomics could allow us to understand individual predispositions to distress and tailor psychiatric treatments based on a patient’s unique biological profile. The concept of theranostics offers an exciting glimpse into integrated diagnostic and therapeutic approaches for mental well-being45.
Implications for Clinical Practice and Future Research
The findings of this review have significant implications for how we deliver cancer care. Integrating these interventions into routine oncology care is the next crucial step. This means moving beyond fragmented services and embedding mental health support directly into the patient’s treatment protocol. Envision oncology clinics where patients are routinely screened for distress through digital platforms, receive personalized app-based support, and have their wearable data integrated into individualized psychosocial care plans. Achieving this model would require: Education and Training: Equipping oncology teams with the knowledge and skills to understand and utilize these biotechnological tools. Clear Referral Pathways: Establishing seamless connections between digital platforms, wearable data, and human mental health professionals. Interoperability: Ensuring that different technological solutions can communicate and share data securely to create a cohesive patient record.
Interdisciplinary collaboration is essential. Mental health professionals, oncologists, nurses, data scientists, and engineers must work hand-in-hand to design, implement, and refine these interventions. This synergy will ensure that solutions are not only technologically sound but also clinically relevant and patient-centered.
While the potential is clear, there are still significant areas for future research: Longitudinal Studies: More research is needed to track the long-term effectiveness of these interventions on mental health outcomes and quality of life in diverse cancer populations. Cost-Effectiveness Analyses: Understanding the economic impact of integrating these technologies into care is crucial for widespread adoption and policy decisions. Comparative Effectiveness Research: Studies comparing different biotechnological interventions against each other, and against traditional care, will help to validate these tools and to identify the most impactful approaches. Ethical Considerations in Practice: Continued research into data privacy, digital equity, and the balance between technology and human connection is vital as these tools become more pervasive. Specific Cancer Types and Treatment Phases: Tailored research is needed to determine how effective certain interventions are for particular cancer types or during specific treatment phases (e.g., active treatment vs. survivorship).
Final Statement
Ultimately, the journey through cancer is deeply personal and encompasses far more than just the physical disease. For optimal cancer patient outcomes, we must wholeheartedly embrace a holistic approach to care that equally prioritizes both physical and mental well-being. Biotechnological innovations are not just tools; they are powerful allies in ensuring that no patient walks this path alone, and that their emotional and psychological needs are met with the same dedication as their medical ones.
Advocacy for Policy Change
Given the compelling evidence for the efficacy and necessity of biotechnological interventions in supporting mental health in oncology, there is a clear and urgent need for policy modernization. Existing healthcare policies and guidelines, such as those from the NHS, while acknowledging the importance of mental health, often struggle with inconsistent implementation, resource constraints, and a lack of proactive integration52.
This article advocates for revisions to existing care policies to formally integrate and fund digital, wearable, and biomarker-based mental health interventions as standard components of comprehensive cancer care. Such a policy shift should: Mandate comprehensive distress screening using validated digital tools at key points in the cancer journey, followed by clear, accessible referral pathways. Allocate dedicated funding for the development, validation, and widespread implementation of evidence-based biotechnological mental health solutions within oncology services. Establish national standards for data security and interoperability for all digital health interventions, ensuring patient privacy and seamless information flow. Promote training and education for healthcare professionals on the effective use and integration of these new technologies. Incentivize research into the long-term effectiveness and equitable access of these interventions, ensuring they benefit all patients regardless of socioeconomic status or geographical location.
By officially embracing and supporting these innovative biotechnologies, policymakers can ensure that cancer care truly becomes holistic, responsive, and ultimately, more compassionate for every patient.
Limitations of the Research
Mental health challenges in cancer are multifaceted. They may stem from pre-existing psychiatric conditions, a predisposition to mental illness, or treatment-induced effects such as depression triggered by certain cancer medicines (e.g., interferon). They may also arise from the psychological impact of diagnosis and the physical, emotional, and financial burdens associated with cancer. This paper does not address the first two categories but focuses on mental health challenges arising from the cancer journey. The paper also focuses on how to leverage biotechnological tools in bridging the gap in mental health disorders and cancer treatment. It is important to note that mental health support and psychosocial care, or well-being, are used interchangeably in this research.
References
- R. Siegel, T. Kratzer, A. Giaquinto, H. Sung, A. Jemal. Cancer statistics. CA Cancer J Clin. Vol. 75(1), pg. 10–45, 2025, doi: 10.3322/caac.21871. [↩]
- F. Bray, M. Laversanne, H. Sung, J. Ferlay, R. Siegel, I. Soerjomataram, A. Jemal. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. Vol. 74(3), pg. 229–263, 2024, doi: 10.3322/caac.21834. [↩] [↩]
- R. Mehta, A. Kommalapati, R. Kim. The impact of ramucirumab treatment on survival and quality of life in patients with gastric cancer. Cancer Manag Res. Vol. 12, pg. 51–57, 2020, doi: 10.2147/CMAR. [↩]
- J. Graham. Breast cancer: The psychological impact of diagnosis, treatment, and remission. Cureus. Vol. 16(10), pg. e70814, 2024, doi: 10.7759/cureus.70814. [↩]
- M. J. Fisch, F. Zhao, A. M. O’Mara, X. S. Wang, D. Cella, C. S. Cleeland. Predictors of significant worsening of patient-reported fatigue over a 1-month timeframe in ambulatory patients with common solid tumors. Cancer. Vol. 120, pg. 442–450, 2014, doi: 10.1002/cncr.28437. [↩]
- S. McManus, J. Olson, M. F. Miller, K. Clark, K. Stein. Prostate cancer-related quality of life and risk for anxiety and depression. J Clin Oncol. Vol. 37, pg. 41–41, 2019, doi: 10.1200/JCO.2019.37.7_suppl.41. [↩] [↩]
- X. Chen, L. Wang, L. Liu, M. Jiang, W. Wang, X. Zhou, J. Shao. Factors associated with psychological distress among patients with breast cancer during the COVID-19 pandemic: A cross-sectional study in Wuhan, China. Support Care Cancer. Vol. 29(9), pg. 4773–4782, 2021, doi: 10.1007/s00520-021-06004-2. [↩]
- X. Chen, L. Wang, L. Liu, M. Jiang, W.Wang, X.Zhou, J. Shan. Factors associated with psychological distress during the COVID-19 pandemic: A cross-sectional study in Wuhan, China. Support Care Cancer. Vol. 29, pg. 4773-4782, 2021, doi: 10.1007/s00520-021-06004-2. [↩]
- Y. Wang, J. Li, J. Shi, J. Que, J. Liu, J. Lappin, J. Leung, A. Ravindran, W. Chen, Y. Qiao, J. Shi, L. Lu, Y. Bao. Depression and anxiety in relation to cancer incidence and mortality: A systematic review and meta-analysis of cohort studies. Mol Psychiatry. 25, 1487–1499, 2020. doi: 10.1038/s41380-019-0595-x. [↩] [↩]
- A. J. Mitchell, M. Chan, H. Bhatti, M. Halton, L. Grassi, C. Johansen, N. Meader. Prevalence of depression, anxiety, and adjustment disorder in oncological, haematological, and palliative-care settings: A meta-analysis of 94 interview-based studies. Lancet Oncol. Vol. 12, pg. 160-174, 2011, doi: 10.1016/S1470-2045(11)70002-X. [↩]
- A. Pitman, S. Suleman, N. Hyde, A. Hodgkiss. Depression and anxiety in patients with cancer. BMJ. Vol. 361, pg. k1415, 2018, doi: 10.1136/bmj.k1415. [↩]
- L. E. Carlson, B. D. Bultz. Benefits of psychosocial oncology care: Improved quality of life and medical cost offset. Health Qual Life Outcomes. Vol. 1, pg. 8, 2003, doi: 10.1186/1477-7525-1-8. [↩]
- J. C. Holland, M. Watson, J. Dunn. The IPOS new international standard of quality cancer care: Integrating the psychosocial domain into routine care. Psycho-Oncology. Vol, 22, pg. 1437–1439, 2013, doi: 10.1002/pon.3308. [↩]
- C. Hollis, C. J. Falconer, J.L. Martin, C. Whittington, S. Stockton, C. Glazebrook, & E. B. Davies. Annual Research Review: Digital health interventions for children and young people with mental health problems – a systematic and meta-review. Journal of Child Psychology and Psychiatry, Vol. 58(4), pg. 474–503, 2017, doi: https://doi.org/10.1111/jcpp.12663. [↩]
- S. Amiri. The prevalence of anxiety symptoms/disorders in cancer patients: A meta-analysis. Front Psychiatry. Vol. 15, pg. 1422540, 2024, doi: 10.3389/fpsyt.2024.1422540. [↩]
- M. Massie. Prevalence of depression in patients with cancer. J Natl Cancer Inst Monogr. Vol. 32, pg. 57–71, 2004, doi: 10.1093/jncimonographs/lgh014. [↩] [↩] [↩]
- Y. Luigjes-Huizer, N. Tauber, G. Humphris, N. Kasparian, W. Lam, S. Label, M. van der Lee. What is the prevalence of fear of cancer recurrence in cancer survivors and patients? A systematic review and individual participant data meta-analysis. Psycho-Oncology. Vol. 31(6), pg. 879–892, 2022, doi: 10.1002/pon.5913. [↩] [↩] [↩]
- P. Santiago, R. Ursano, C. Gray, R. Pynoos, D. Spiegel, R. Lewis-Fernandez, M. Friedman, C. Fullerton. A Systematic Review of PTSD Prevalence and Trajectories in DSM-5 Defined Trauma Exposed Populations. PLoS ONE. Vol. 8(4), pg. e59236, 2013, doi: 10.1371/journal.pone.0059236. [↩]
- P. Arnaboldi, C. Lucchiari, L. Santoro, C. Sangalli, A. Luini, & G. Pravettoni. PTSD symptoms as a consequence of breast cancer diagnosis: clinical implications. SpringerPlus, 3(1), pg.392, 2014, doi: https://doi.org/10.1186/2193-1801-3-392. [↩] [↩]
- M. Henry, J. Albert, S. Frenkiel, M. Hier, A. Zeitouni, K. Kost, A. Mlynarek, M. Black, C. MacDonald, K. Richardson, M. Mascarella, G. Morand, G. Chartier, N. Sadeghi, C. Lo, Z. Rosberger. Body image concerns in patients with head and neck cancer: A longitudinal study. Front Psychol. Vol. 13, pg. 816587, 2022, doi: 10.3389/fpsyg.2022.816587. [↩]
- M. Thakur, R. Sharma, A. Mishra, B. Gupta. Body image disturbances among breast cancer survivors: A narrative review of prevalence and correlates. Cancer Res Stat Treat. Vol. 5(1), pg. 90–96, 2022, doi: https://doi.org/10.4103/crst.crst_170_21. [↩]
- W. Chang, A. Lai. Cumulative burden of psychiatric disorders and self-harm across 26 adult cancers. Nat Med. Vol. 28(4), pg. 860–870, 2022, doi: 10.1038/s41591-022-01740-3. [↩] [↩]
- D. Haywood, R. Kotov, R. F. Krueger, A. G. C. Wright, M. K. Forbes, E. Dauer, F. D. Baughman, S. L. Rossell, N. H. Hart. Reconceptualizing mental health in cancer survivorship. Trends in Cancer. Vol. 10, pg. 677–686, 2024, doi: 10.1016/j.trecan.2024.05.008. [↩] [↩]
- A. Fernando. Mental health and cancer: Why it is time to innovate and integrate—a call to action. Eur Urol Focus. Vol. 6, pg. 1165–1167, 2020, doi: 10.1016/j.euf.2020.06.025. [↩] [↩]
- D. Nair. Measuring and Modifying Psychological Distress in CKD: New Insights and Next Steps. Kidney Medicine. Vol. 1(4), pg. 147–149, 2019, doi: 10.1016/j.xkme.2019.07.003. [↩]
- C. Chang, R. Hayes, M. Broadbent, M. Hotopf, E. Davies, H. Møller, R. Stewart. A cohort study on mental disorders, stage of cancer at diagnosis, and subsequent survival. BMJ Open. Vol. 4(1), pg. e004295, 2014, doi: 10.1136/bmjopen-2013-004295. [↩] [↩]
- Y. Pan, Y. Lin. Systematic Review and Meta-Analysis of Prevalence of Depression Among Caregivers of Cancer Patients. Front Psychiatry. Vol. 13, pg. 817936, 2022, doi: 10.3389/fpsyt.2022.817936. [↩]
- A. Gupta, C. Hurley, R. Mangal, A. Daniel, L. Ganti. Cancer caregivers are primarily motivated by love and a sense of duty. Health Psychology Research. Vol. 12, pg. 92643, 2024, doi: 10.52965/001c.92643. [↩]
- A. E. Usher, J. Bell, L. A. Beckett, J. G. Joseph, B. J. Zebrack, & F. J. Meyers. Psychosocial outcomes and care utilization among rural and nonrural cancer patients. Journal of Clinical Oncology, Vol. 37, pg. 79–79, 2019, doi: https://doi.org/10.1200/jco.2019.37.31_suppl.79. [↩]
- V. Zimmermann-Schlegel, M. Hartmann, H. Sklenarova, W. Herzog, & M. W. Haun, . Accessibility, Availability, and Potential Benefits of Psycho-Oncology Services: The Perspective of Community-Based Physicians Providing Cancer Survivorship Care. The Oncologist, Vol. 22(6), pg. 719–727, 2017, doi: https://doi.org/10.1634/theoncologist.2016-0245. [↩]
- C. Yigitbas, & A. Bulut. Exploring psychological help-seeking behaviors and stigma perception among cancer patients: a study on their impact on psychosocial adjustment. Supportive Care in Cancer, Vol. 32(10), pg. 649, 2022, https://doi.org/10.1007/s00520-024-08870-z. [↩]
- Y. Yang, T. Wang, D. Wang, M. Liu, S. Lun, S. Ma, J. Yin. Gaps between current practice in perinatal depression screening and guideline recommendations. General Hospital Psychiatry. Vol. 89, pg. 1–10, 2024, doi: 10.1016/j.genhosppsych.2024.04.011. [↩]
- Z. Wu, F. Luo, S. Wang, X. Hu, M. Chen. Digital interventions and mental health outcomes in patients with cancer: Systematic review and meta-analysis. JMIR Cancer. Vol. 11, pg. e64754, 2025, doi: 10.2196/64754. [↩]
- J. Atkins, R. Joseph. Stigma and Access to Mental Healthcare among US Veterans. Cureus. Vol. 18(1), pg. 102713, 2026, doi: 10.7759/cureus.102713. [↩]
- C. Zhong, X. Luo, M. Tan, J. Chi, B. Guo, J. Tang, Z. Guo, S. Deng, Y. Zhang, Y. Wu. Digital health interventions to improve mental health in patients with cancer: Umbrella review. J Med Internet Res. Vol. 27, pg. e69621, 2025, doi: 10.2196/69621. [↩] [↩] [↩]
- M. Kim, K. Kang, S. Ryu. Effects of web-based interventions on anxiety and depression in patients with breast cancer: A systematic review and meta-analysis of randomized controlled trials. Psycho-Oncology. Vol. 34(1), pg. e70167, 2025, doi: 10.1002/pon.70167. [↩]
- M. Khosravi, & G. Azar. A systematic review of reviews on the advantages of mhealth utilization in mental health services: a viable option for large populations in low-resource settings. Global Mental Health, Vol. 11, pg. e43, 2024, doi: https://doi.org/10.1017/gmh.2024.39. [↩] [↩]
- C. Zhong, X. Luo, M. Tan, J. Chi, B. Guo, J. Tang, Z. Guo, S. Deng, Y. Zhang, Y. Wu. Digital health interventions to improve mental health in patients with cancer: Umbrella review. J Med Internet Res. Vol. 27, pg. e69621, 2025, doi: 10.2196/69621. [↩] [↩]
- A. Mitsis, P. Filis, G. Karanasiou, E. Georga, D. Mauri, K. Naka, A. Constantinidou, K. Keramida, D. Tsekoura, K. Mazzocco, A. Alexandraki, E. Kampouroglou, Y. Goletsis, A. Papakonstantinou, A. Antoniades, C. Brown, V. Bouratzis, E. Matos, K. Marias, M. Tsiknakis, D. Fotiadis. Impact of e-health interventions on mental health and quality of life in breast cancer patients: A systematic review and meta-analysis of randomized controlled trials. Cancers. Vol. 17(11), pg. 1780, 2025, doi: 10.3390/cancers17111780. [↩]
- J. Chow, K. Li. Ethical considerations in human-centered AI: Advancing oncology chatbots through large language models. JMIR Bioinform Biotechnol. Vol. 5, pg. e64406, 2024, doi: 10.2196/64406. [↩] [↩]
- H. Pappot, E. B. Steen-Olsen, C. Holländer-Mieritz. Experiences with wearable sensors in oncology during treatment: Lessons learned from feasibility research projects in Denmark. Diagnostics (Basel). Vol. 14, pg. 405, 2024, doi: 10.3390/diagnostics14040405. [↩]
- D. Presby, S. Jasinski, E. Capodilupo, K. E. Holmes, W. von Hippel, G. J. Grosicki, & V. Lee. Inter- and Intrapersonal Associations Between Physiology and Mental Health: A Longitudinal Study Using Wearables and Mental Health Surveys. Journal of Medical Internet Research, Vol. 27, pg. E64955–e64955, 2025, doi: https://doi.org/10.2196/64955. [↩]
- M. Fortunato, S. Adusumalli, N. Chokshi, J. Harrison, C. Rareshide, M. Patel. Usability of Wearable Devices to Remotely Monitor Sleep Patterns Among Patients With Ischemic Heart Disease. JMIR Formative Research. Vol. 4(4), pg. e14508, 2020, doi: 10.2196/14508. [↩] [↩]
- O. Kardan, P. A. Reuter-Lorenz, S. Peltier, S. W. Churchill, B. Misic, M. K. Askren, M. S. Jung, B. Cimprich, & M. G. Berman. Brain connectivity tracks effects of chemotherapy separately from behavioral measures. NeuroImage: Clinical, Vol. 21, pg. 101654, 2019, oi: https://doi.org/10.1016/j.nicl.2019.101654. [↩]
- N. Tolboom, A. Verger, N. Albert, F. Fraioli, E. Guedj, T. Traub-Weidinger, S. Morbelli, K. Herrmann, P. Zucchetta, S. Plasschaert, I. Yakushev, M. Weller, M. Glas, M. Preusser, D. Cecchin, H. Barthel, D. Van Weehaeghe. Theranostics in neurooncology: Heading toward new horizons. J Nucl Med. Vol. 65(2), pg. 167–173, 2024, doi: 10.2967/jnumed.123.266205. [↩] [↩] [↩] [↩]
- E. G. Lattie, E. C. Adkins, N. Winquist, C. Stiles-Shields, Q. E. Wafford, A. K. Graham. Digital mental health interventions for depression, anxiety, and enhancement of psychological well-being among college students: Systematic review. J Med Internet Res. Vol. 21, pg. e12869, 2019, doi: 10.2196/12869. [↩]
- J. Fortin, M. Leblanc, G. Elgbeili, M. J. Cordova, M. F. Marin, A. Brunet. The mental health impacts of receiving a breast cancer diagnosis: A meta-analysis. Br J Cancer. Vol. 125, pg. 1582–1592, 2021, doi: 10.1038/s41416-021-01542-3. [↩]
- L. Johannsen, M. Brandt, W. Frerichs, L. Inhestern, C. Bergelt. The impact of cancer on the mental health of patients’ parenting minor children: A systematic review of quantitative evidence. Psychooncology. Vol. 31, pg. 869–878, 2022, doi: 10.1002/pon.5912. [↩]
- D. Haywood, R. Kotov, R. Krueger, A. Wright, M. Forbes, E. Dauer, F. Baughman, S. Rossell, N. Hart. Reconceptualizing mental health in cancer survivorship. Trends in Cancer. Vol. 10(8), pg. 677–686, 2024, doi: 10.1016/j.trecan.2024.05.008. [↩]
- A. Fernando. Mental health and cancer: Why it is time to innovate and integrate—a call to action. Eur Urol Focus. Vol. 6(6), pg. 1165–1167, 2020, doi: 10.1016/j.euf.2020.06.025. [↩]
- F. Ibrahim, I. Petkov, M. Al‐Jabri, A. Hammoud, M. Khasawneh, S. Ahmed, G. Shahrour. Efficacy of Digital Mental Health Interventions for Depression and Anxiety in Older Adults. Worldviews on Evidence-Based Nursing. Vol. 23(1), pg. 1–15, 2026, doi: 10.1111/wvn.70119. [↩]
- A. Gagliardi, M. Brouwers. Do Guidelines Offer Implementation Advice to Target Users? A Systematic Review of Guideline Applicability. BMJ Open. Vol. 5(2), pg. e007047, 2015, doi: 10.1136/bmjopen-2014-007047. [↩]



{kind=link}