
Abstract
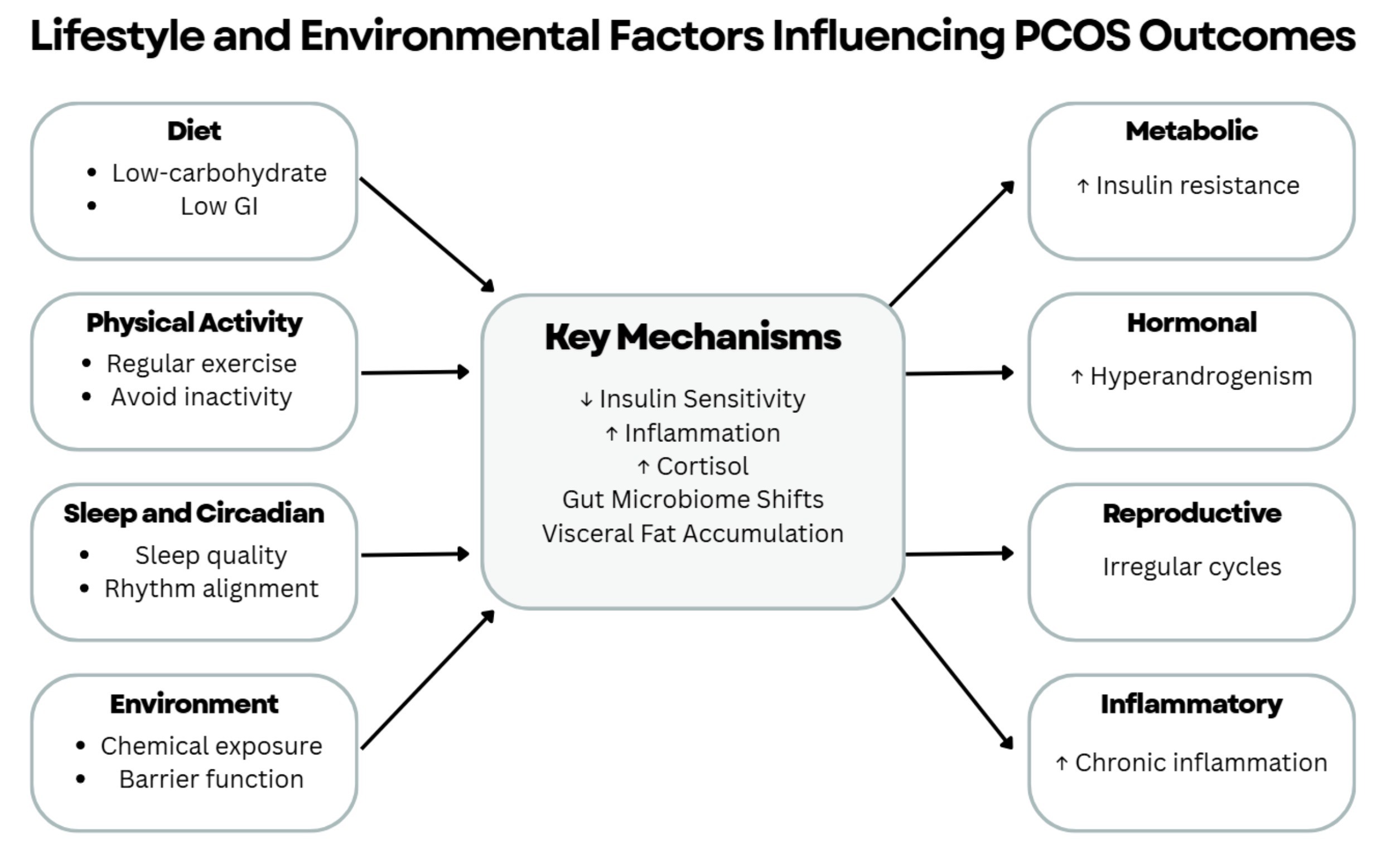
Polycystic Ovary Syndrome (PCOS) is an increasingly recognized condition that affects a significant portion of women worldwide. PCOS is presented by several features including metabolic, reproductive, and hormonal abnormalities. This review explores the extent to which modifiable lifestyle and environmental factors influence PCOS outcomes and identifies future directions for researchers in this area. Reproductive and metabolic health was improved through low-carbohydrate and high-monounsaturated fat diets, which were associated with meaningful reductions in insulin levels and improvements in metabolic outcomes across studies, though effects depend on intensity and consistency. Poor sleep and circadian rhythm disruption elevate cortisol and insulin resistance, while emerging evidence links chemical exposures to chronic inflammation and ovarian dysfunction, with improvements in inflammatory markers reported across studies. These findings demonstrate that integrated lifestyle modifications offer clinically meaningful improvements in metabolic and reproductive parameters. This review highlights that lifestyle and environmental factors are not secondary influences but appear as significant contributors to PCOS progression, offering clinically relevant targets for improving metabolic and reproductive outcomes.
Keywords: Polycystic ovary syndrome, insulin resistance, diet, exercise, circadian rhythm, inflammation, environmental exposures
Introduction
PCOS is a common endocrinopathy that affects approximately 6-10% of women of reproductive age worldwide, making it one of the most prevalent endocrine disorders in this population1. The exact cause of PCOS is unknown, but it is suggested that genetic predisposition plays a significant role1. Prevalent physical PCOS manifestations include hyperandrogenism (characterized by elevated androgen levels leading to hirsutism, acne, and male-pattern hair loss), irregular or absent menstruation, insulin resistance, infertility, and metabolic complications such as obesity and type 2 diabetes mellitus. Chronic low-grade systemic inflammation is a key feature of PCOS and contributes to hormonal and metabolic dysfunction by impairing insulin sensitivity and disrupting endocrine regulation2. Inflammation can fluctuate based on a multitude of factors, including dietary composition, physical activity levels, sleep duration and quality, stress exposure, and gut microbiome composition. These factors collectively influence PCOS severity2,3.
Emerging evidence suggests that lifestyle and environmental factors greatly impact the development and severity of PCOS, including the role of endocrine-disrupting chemicals such as bisphenol A (BPA) and phthalates in promoting hyperandrogenism4,5, the contribution of circadian rhythm disruption to insulin resistance and hormonal dysregulation6,7, and the potential of dietary interventions and exercise to substantially reverse these metabolic deficits8,9. PCOS is also associated with psychological conditions, including anxiety and depression, which reduce quality of life3. Despite the widespread reliance on pharmacological treatments, modifiable lifestyle and environmental factors remain underutilized in PCOS management, even though emerging evidence suggests they play a critical role in disease progression and symptom severity.
Despite this fact, PCOS remains underexplored in terms of modifiable lifestyle factors that could alleviate symptoms. Several factors may explain this research gap: (1) the historical underrepresentation of women in clinical trials, limiting the evidence base for female-specific conditions3; (2) heterogeneity in PCOS diagnostic criteria across studies, such as the differences between Rotterdam and NIH criteria, which makes it difficult to aggregate findings, a limitation acknowledged across the reviewed literature2,1; (3) the multisystem complexity of PCOS, spanning endocrine, metabolic, reproductive, and psychological domains, making well-controlled lifestyle intervention studies particularly challenging to design3; and (4) traditional research emphasis on pharmaceutical rather than lifestyle-based interventions3. Notably, the period from 2005 onward saw an acceleration in PCOS-specific lifestyle research, coinciding with wider adoption of the Rotterdam diagnostic criteria (2003) and increasing recognition of insulin resistance as a central pathological mechanism, which together created a more standardized and productive research environment.
This review addresses the influence of lifestyle and environmental factors on PCOS by synthesizing recent literature on how diet, physical activity, sleep, and environmental exposures impact PCOS through mechanisms of inflammation and insulin resistance. The evidence suggests that structured dietary modification, supervised exercise, sleep optimization, and reduction of chemical exposures can each independently improve key PCOS outcomes, with combined interventions potentially reducing fasting insulin by 30-40%, improving insulin sensitivity by 20-35%, and lowering inflammatory markers by 15-25%8,9,6. These magnitudes are clinically comparable to, and in some cases exceed, the effects of commonly used pharmacological interventions such as metformin, underscoring the importance of integrating lifestyle strategies into standard PCOS management. Understanding these factors provides an opportunity to broaden therapeutic strategies beyond pharmacological interventions.
Methods
Study Design
This narrative review systematically synthesized literature on lifestyle and environmental influences on PCOS outcomes. The review protocol was designed following PRISMA guidelines for systematic reviews, though this is a narrative rather than systematic review with meta-analysis.
Inclusion Criteria
Articles were included if they were published in English between 2005 and 2025. This timeframe was selected for two principal reasons: (1) the Rotterdam criteria for PCOS diagnosis were formally established in 2003, and the years immediately following saw a marked increase in standardized, diagnostically consistent research; and (2) contemporary lifestyle and environmental exposure patterns, including modern dietary trends, sedentary behavior, and the proliferation of endocrine-disrupting chemicals in consumer products, are best reflected in literature from this period, making pre-2005 studies less directly applicable to current clinical and public health contexts. Included articles investigated lifestyle or environmental influences on PCOS and reported findings related to metabolic, inflammatory, or hormonal outcomes. Both original research, narrative, and systematic reviews were considered. Where PCOS-specific primary evidence was limited, particularly in the physical activity and sleep domains, mechanistic or translational studies from related populations (e.g., metabolic dysfunction, athletic cohorts, animal models) were also included to provide biological plausibility, and are clearly identified as such throughout the Results and Discussion sections. Although studies drew from diverse populations, variability in diagnostic criteria, study designs, and intervention duration represents a limitation.
Search Criteria
A literature search was conducted using PubMed, Google Scholar, and ScienceDirect. Keywords included “PCOS,” “inflammation,” “insulin resistance,” “diet,” “exercise,” “circadian rhythm,” and “environmental exposures.” Studies were selected based on relevance to the review’s themes, with priority given to peer-reviewed articles published between 2005 and 2025 reporting findings related to metabolic, inflammatory, or hormonal outcomes in the context of PCOS. As this is a narrative rather than systematic review, a formal PRISMA screening process was not applied; however, 25 studies meeting these criteria were identified and included in the final analysis.
Data Extraction
For each included article, key information was recorded: authors, year, journal, lifestyle factor studied, and primary findings. Extracted data were organized thematically into four categories: diet, physical activity, sleep/circadian rhythm, and environmental/allergy-related factors. This narrative synthesis approach allowed comparison of findings across studies.
Results
| Factor | No. of Studies | Study Types | Main Finding | Effect Size (if available) |
| Diet | 6 | 1 RCT, 2 observational, 2 meta-analyses, 1 case-control | Low-carb/low-GI and Mediterranean diets improve insulin sensitivity and reproductive outcomes | Fasting insulin decreases 30-40% |
| Physical Activity | 6 | 2 systematic reviews/meta-analysis, 1 RCT pilot, 1 animal model, 2 mechanistic studies | Exercise improves insulin sensitivity; vigorous intensity most effective; inactivity induces insulin resistance | Insulin sensitivity increases 20-35% |
| Sleep/Circadian Rhythm | 6 | 2 systematic reviews/meta-analyses, 2 mechanistic studies, 1 narrative review, 1 cohort | Poor sleep worsens insulin resistance; PCOS linked to altered melatonin and elevated evening cortisol | Modest sleep improvement; inflammatory markers NS |
| Environmental Exposures | 7 | 3 systematic reviews, 2 observational, 1 review, 1 mechanistic study | BPA, phthalates linked to PCOS; barrier dysfunction and chemical exposures linked to inflammation | Positive association in 19/22 BPA studies |
Studies are organized below by strength of evidence, with PCOS-specific research prioritized over mechanistic or translational studies.
Diet
Evidence from PCOS-Specific Studies
The following findings are synthesized from published studies reviewed for this paper; they represent the current state of literature rather than results of a new primary analysis. Dietary patterns stand as one of the strongest influences on PCOS progression. In women diagnosed with PCOS, high carbohydrate intake and hyperinsulinemia were consistently associated with worsening metabolic and hormonal dysfunction2,1. Dietary interventions such as low carbohydrate, high monounsaturated fat diets were shown to lower fasting insulin and triglycerides in women with PCOS, suggesting nutrition can be a powerful therapeutic tool8. A systematic review and meta-analysis of eight trials reported that a low glycemic index diet improved several clinical outcomes in women with PCOS, including emotional health, hirsutism, and infertility, underscoring the potential of glycemic-focused dietary modification to improve both metabolic and reproductive profiles10. Adherence to the Mediterranean diet, characterized by high fiber, complex carbohydrates, monounsaturated fats, and omega-3s, was found to be lower in women with PCOS compared to BMI-matched controls, and lower adherence correlated with higher testosterone, CRP, and HOMA-IR, suggesting that diet quality rather than caloric intake alone is associated with PCOS severity11. A systematic review and meta-analysis of 15 ketogenic diet studies in women with PCOS found significant reductions in BMI, waist circumference, and insulin resistance, as well as improvements in LH levels and menstrual regularity, though heterogeneity across studies warrants cautious interpretation12.
Mechanistic Evidence from Related Populations
Visceral adiposity, often resulting from excess caloric intake, was also strongly associated with glucose intolerance, elevated inflammatory markers, and hormonal imbalance13,14. Although the following study was not conducted specifically in women with PCOS, it provides mechanistic insight into the relationship between fat distribution and insulin resistance that may be applicable to PCOS pathophysiology. In a study of Asian Indian adults across normal glucose tolerance, impaired glucose tolerance, and type 2 diabetes mellitus, it was reported that visceral fat, but not subcutaneous fat, was strongly associated with insulin resistance and inflammatory markers including hs-CRP, TNF-α, and oxidized LDL. These markers were accompanied by reduced adiponectin and increased carotid intima-media thickness13. This mechanistic evidence suggests a link between fat distribution, metabolic inflammation, and cardiovascular risk that may be particularly relevant to PCOS given the condition’s association with central obesity.
Back to PCOS-Specific Evidence
Dahan and Reaven (2019) evaluated insulin resistance in women with PCOS in comparison to ovulatory controls using a gold-standard insulin suppression test. The authors found that PCOS subjects had overall higher steady-state plasma glucose (SSPG) levels, indicating increased insulin resistance. The difference was mild in lean women and became more pronounced with obesity, particularly when BMI ≥30 kg/m²14.
Physical Activity
PCOS-Specific Evidence
Physical activity demonstrated similarly important effects. A systematic review and meta-analysis of 33 studies covering 777 women with PCOS found that exercise, particularly vigorous-intensity training, significantly improved VO₂peak, HOMA-IR, BMI, and waist circumference, suggesting that exercise intensity may matter more than total duration9. A 20-week home-based aerobic exercise intervention in 60 women with PCOS found significant reductions in fasting glucose, fasting insulin, HOMA-IR, and hs-CRP compared to controls, connecting exercise to both metabolic and inflammatory improvement simultaneously15.
Mechanistic Evidence from Related Populations
Further mechanistic insight comes from animal and non-PCOS human studies; as noted in the Methods section, these were included to provide biological plausibility where direct PCOS evidence is limited, and should not be interpreted as direct evidence of effect in PCOS populations. Regular exercise improved insulin sensitivity and reduced inflammation in general populations and women with metabolic dysfunction1. Martin et al. (2025) studied gut microbiota from endurance athletes and found that, despite reduced bacterial diversity, these microbiota were enriched in short-chain fatty acids and improved insulin sensitivity when transplanted into mice16. While this study was not specific to PCOS, it demonstrates the impact of exercise on microbial shifts that may influence metabolic dysfunction central to PCOS. Similarly, Gratas-Delamarche et al. (2013) demonstrated that physical inactivity induced early insulin resistance by activating an oxidative inflammatory loop in skeletal muscle, even after only a few days of reduced activity17. These mechanistic studies from non-PCOS populations suggest that both muscle metabolic pathways and exercise-driven gut microbiome shifts may enhance insulin regulation, providing biological plausibility for exercise benefits in PCOS, though direct PCOS-specific evidence is needed. A PCOS rat model study using DHEA induction found that 12 weeks of HIIT improved insulin sensitivity, reduced HOMA-IR, lowered skeletal muscle IL-6, and improved ovarian tissue morphology, providing further biological plausibility for exercise benefits in PCOS18. It is important to note that not all exercise interventions are equally beneficial. Short-term unsupervised interventions had limited impact in metabolic populations, and vigorous activity can paradoxically worsen glucose regulation in some individuals due to increased cortisol response and acute inflammatory stress, particularly in sedentary individuals beginning high-intensity exercise without proper progression17. Therefore, structured, long-term, and supervised physical activity programs remain the most reliable approach.
Sleep and Circadian Rhythms
PCOS-Relevant Findings
Sleep and circadian rhythms were identified as critical regulators of both metabolic and hormonal stability. Poor sleep quality is associated with heightened cortisol activity and insulin resistance, while aerobic exercise was shown to improve sleep quality and lower inflammatory markers. Burt Solorzano et al. (2018) examined insulin-resistant peripubertal girls and discovered that free testosterone levels correlated with insulin sensitivity and luteinizing hormone (LH) concentrations, but not with circulating insulin19, suggesting that insulin resistance may be associated with androgen excess through enhanced LH secretion rather than through hyperinsulinemia directly, highlighting a critical neuroendocrine mechanism relevant to PCOS pathophysiology. A systematic review and meta-analysis of 16 studies covering 1,100 women with PCOS found that women with PCOS had altered melatonin levels, higher evening cortisol, and lower sleep efficiency compared to controls, providing direct biomarker evidence that circadian rhythm disruption is associated with PCOS6. A review of clock gene disruption and hypothalamic-pituitary-ovarian axis regulation further explained how circadian misalignment may contribute to insulin resistance, glucose dysregulation, and hormonal imbalance in PCOS, and introduced chronotherapy as a potential future strategy7.
Evidence from Athletic and General Populations
Nobari et al. (2023) found that in athletes, performance peaks in the late afternoon, with exercise timing, diet, and sleep-wake cycles influencing hormonal regulation and immune function20. A meta-analysis of 11 RCTs by Rubio-Valles and Ramos-Jimenez (2025) found that aerobic exercise modestly improved sleep outcomes but did not significantly reduce inflammatory markers IL-6 or TNF-a21. While these studies were not PCOS-specific, they suggest that sleep and circadian alignment may influence metabolic and hormonal regulation relevant to PCOS. Chronic stress further contributed to worsening metabolic function, underscoring the need to address stress management in PCOS care22.
Environment
Primary PCOS-Specific Evidence on Endocrine-Disrupting Chemicals
Environmental and immunologic factors are emerging as important influences on PCOS. Unlike diet and exercise, direct primary evidence linking environmental exposures to PCOS-specific outcomes has historically been limited. However, recent systematic reviews now provide more direct human evidence. A systematic review of 22 human studies including 1,682 PCOS patients found that 19 of 22 studies reported a positive association between bisphenol A (BPA) exposure and PCOS, with BPA frequently linked to hyperandrogenism and carbohydrate metabolism disorders; notably, women with PCOS had higher BPA levels independent of BMI in 15 studies, suggesting a relationship beyond obesity-related metabolic changes4. A broader systematic review of non-persistent endocrine-disrupting chemicals found that BPA, phthalates, and octocrylene were positively associated with PCOS, while results for triclosan were inconclusive and parabens did not show a clear association5. A wider review of emerging pollutants, including pharmaceuticals and personal care products, microplastics, and nanoparticles, proposed that these exposures may contribute to PCOS through endocrine disruption, oxidative stress, and reactive oxygen species production, expanding the pollutant burden of concern beyond a single chemical class23.
Mechanistic and Indirect Evidence
Epithelial barrier dysfunction was linked to systemic hormonal imbalance and immune dysregulation in children with allergic diseases24. However, direct evidence that barrier dysfunction causes ovarian dysfunction in PCOS was not established in the reviewed literature. Separately, Patel (2018) discussed frequent exposure to chemical-heavy consumer products as a potential contributor to PCOS through inflammatory pathways, though primary evidence directly linking consumer product chemicals to PCOS onset or progression was not provided in that review3.
PCOS-Specific Observational Evidence
Ghosh et al. (2025) examined PCOS in women from different religious communities in Kolkata, reporting that waist circumference and body fat patterning predicted premenstrual symptoms and menstrual dysfunction, demonstrating that environmental and cultural factors influencing body composition may affect PCOS symptom severity25 . Hormonal dysregulation was identified as a systematic feature of allergic diseases by Berdnikovs et al. (2017), who found that children with asthma, atopic dermatitis, or food allergy had decreased insulin and C-peptide, but elevated triiodothyronine and growth hormone, which correlated with epithelial barrier dysfunction and allergic inflammation24. While this finding was not from PCOS patients, it suggests a potential mechanistic link between barrier dysfunction, inflammation, and endocrine disruption that warrants further investigation in PCOS.
Discussion
Taken together, the evidence reviewed in this study suggests a consistent pattern: insulin resistance is a central feature of PCOS pathophysiology, and each of the four lifestyle and environmental domains examined in this review converges on insulin resistance as both a shared mechanism and a shared therapeutic target.
The dietary evidence most directly illustrates this pattern. Low-carbohydrate and low-glycemic index diets reduced fasting insulin by 30-40% in women with PCOS8,10, while poor diet quality, characterized by lower Mediterranean diet adherence, was associated with higher testosterone, CRP, and HOMA-IR11, suggesting that hyperinsulinemia directly amplifies androgen production. This is consistent with the findings of Dahan and Reaven (2019), who demonstrated that insulin resistance in PCOS is relatively mild in lean women but becomes substantially more severe with obesity (BMI ≥ 30 kg/m²)14, and with the mechanistic evidence from Indulekha et al. showing that visceral fat accumulation is specifically associated with the inflammatory markers most relevant to PCOS13. In PCOS, where hyperinsulinemia amplifies androgen production, excess visceral fat may contribute to worsening metabolic and reproductive dysfunction.
Physical activity reflects the same relationship from a different angle. Rather than simply reducing weight, vigorous-intensity exercise independently improved HOMA-IR and VO2peak in women with PCOS9, and a 20-week aerobic intervention simultaneously reduced both insulin resistance and the inflammatory marker hs-CRP15. The mechanistic studies from non-PCOS populations, including the gut microbiome transplant findings of Martin et al.16 and the rapid-onset insulin resistance documented by Gratas-Delamarche et al. after just days of inactivity17, suggest that exercise exerts its benefits through multiple pathways: microbial metabolite production, muscle oxidative stress reduction, and direct improvement of insulin signaling. The PCOS-specific HIIT rat model study of Kocak et al. (2025) corroborates this, showing improvements in insulin sensitivity, IL-6 reduction, and ovarian histopathology following structured exercise18, though the authors acknowledged that animal model findings require validation in human PCOS populations, a limitation that applies to several mechanistic studies in this review.
The sleep and circadian evidence demonstrates how the insulin resistance-androgen cycle can be triggered from a third direction. Heydari and Ramdass (2025) found that women with PCOS exhibit higher evening cortisol, altered melatonin, and reduced sleep efficiency compared to controls6, and Somala et al. (2025) traced this to clock gene dysfunction in the hypothalamic-pituitary-ovarian axis7. Burt Solorzano et al. (2018) provided a critical mechanistic link: in insulin-resistant peripubertal girls, it is tissue-specific insulin sensitivity rather than circulating insulin levels that drives testosterone elevation through enhanced LH secretion19. This suggests a pathway from circadian disruption to cortisol dysregulation, to insulin resistance, to elevated LH, and ultimately to hyperandrogenemia. Both Heydari and Ramdass6 and Somala et al.7 acknowledged that their observational designs preclude causal claims, and called for longitudinal intervention studies to establish directionality.
The environmental findings fit this pattern as well. BPA exposure was positively associated with PCOS in 19 of 22 human studies, independent of BMI4, and BPA is known to act as an endocrine disruptor that can impair insulin signaling and promote hyperandrogenism, mechanisms that parallel those seen across the dietary, exercise, and sleep domains. Phthalates and octocrylene showed similar associations5, and broader emerging pollutants including microplastics may further compound this endocrine burden23. The authors of these systematic reviews uniformly noted that causality cannot yet be established, as most studies are cross-sectional and exposure measurement may not reflect long-term cumulative burden. These are important gaps that future primary PCOS studies with longitudinal designs should address.
What connects these four domains is a shared biological mechanism: diet, inactivity, sleep disruption, and chemical exposure can each independently impair insulin signaling, and PCOS appears to be particularly vulnerable to the compounding of these insults. This has important implications for treatment, as addressing any single factor in isolation likely underestimates the potential benefit of combined lifestyle modification, and future research should prioritize multi-component intervention designs.
Several limitations of the reviewed literature should be acknowledged. Many dietary studies relied on small samples and short intervention durations, which the authors themselves noted as constraints on long-term inference8,10,12. Diagnostic criteria for PCOS varied across studies, limiting comparability, a concern raised explicitly in several of the systematic reviews included here2,4. Self-reported dietary and lifestyle measures introduce recall bias, and underrepresentation of diverse populations continues to limit the generalizability of findings. The scope of this review was also narrowed by limited access to paywalled journals. These findings should therefore be interpreted with appropriate caution.
Conclusion
PCOS is increasingly being recognized as a condition heavily influenced by lifestyle and environmental factors, with insulin resistance serving as a central pathway through which these influences converge. Dietary composition is a primary contributor to insulin sensitivity. Diets low in carbohydrate and high in monounsaturated fats were shown to reduce fasting insulin and triglycerides, while low-glycemic index and Mediterranean diets also demonstrated benefits for metabolic and reproductive outcomes. Ketogenic diets showed promising but heterogeneous results. High-carbohydrate diets worsened hyperinsulinemia and androgen excess. Physical activity improved metabolic outcomes, with vigorous-intensity exercise showing the strongest benefits, though effects varied depending on duration, intensity, and supervision. Sleep quality and circadian rhythm regulation emerged as essential regulators of hormonal and metabolic health, as poor sleep was linked to cortisol elevation, amplified insulin resistance, and ultimately hyperandrogenemia through LH-mediated pathways. Emerging evidence, now supported by primary human studies, linked BPA and phthalate exposure to PCOS independent of BMI, while broader pollutant exposures suggest additional environmental contributors, though direct causal evidence in PCOS populations is still needed. These findings highlight the multifactorial nature of PCOS and suggest that lifestyle interventions may substantially improve metabolic and reproductive outcomes.
This review highlights the need for integrated management approaches combining dietary, behavioral, and environmental strategies. Future research should investigate long-term multi-component interventions, the role of circadian regulation as a therapeutic target, and the effects of environmental exposures through primary PCOS-specific studies with longitudinal designs. Addressing PCOS requires more than pharmacological management. Lifestyle and environmental modifications provide important, patient-centered strategies that can reduce systemic inflammation, improve metabolic outcomes, and enhance quality of life.
Acknowledgements
I would like to thank Christina Ambrosino for her guidance and feedback throughout the development of this paper. I am also grateful to my family for their encouragement and support.
References
- Y. Xu, J. Qiao. Association of insulin resistance and elevated androgen levels with polycystic ovarian syndrome (PCOS): A review of literature. J Healthc Eng. 2022, 9240569 (2022). https://doi.org/10.1155/2022/9240569 [↩] [↩] [↩] [↩] [↩]
- A. J. Duleba, A. Dokras. Is PCOS an inflammatory process? Fertility Steril. 97, 7–12 (2012). https://doi.org/10.1016/j.fertnstert.2011.11.023 [↩] [↩] [↩] [↩] [↩]
- S. Patel. Polycystic ovary syndrome (PCOS), an inflammatory, systemic, lifestyle endocrinopathy. J of Steroid Biochem Mol Biol. 182, 27–36 (2018). https://doi.org/10.1016/j.jsbmb.2018.04.008 [↩] [↩] [↩] [↩] [↩] [↩]
- L. A. M. L. Urbanetz, J. M. Soares-Junior, R. D. S. Simões, G. A. R. Maciel, M. C. P. Baracat, E. C. Baracat. Bisphenol A and Polycystic Ovary Syndrome in Human: A Systematic Review. Int. J. Gynaecol. Obstet. 166, 190–203 (2024). https://doi.org/10.1002/ijgo.15349 [↩] [↩] [↩] [↩]
- M. Ozga, J. Jurewicz. Environmental Exposure to Selected Non-Persistent Endocrine Disrupting Chemicals and Polycystic Ovary Syndrome: A Systematic Review. Int. J. Occup. Med. Environ. Health 38, 98–121 (2025). https://doi.org/10.13075/ijomeh.1896.02551 [↩] [↩] [↩]
- T. Heydari, P. V. A. K. Ramdass. Circadian Rhythm Disruption and Polycystic Ovary Syndrome: A Systematic Review and Meta-Analysis. AJOG Glob. Rep. 5, 100479 (2025). https://doi.org/10.1016/j.xagr.2025.100479 [↩] [↩] [↩] [↩] [↩]
- C. S. Somala, T. Anand, K. M. Saravanan, D. C. Mathangi. Polycystic Ovary Syndrome and the Circadian Clock: Understanding the Link Between Metabolism, Hormones, and Sleep. Human Gene 46, 201497 (2025). https://doi.org/10.1016/j.humgen.2025.201497 [↩] [↩] [↩] [↩]
- C. C. Douglas, B. A. Gower, B. E. Darnell, F. Ovalle, R. A. Oster, R. Azziz. Role of diet in the treatment of polycystic ovary syndrome. Fertility Steril. 85, 679–688 (2006). https://doi.org/10.1016/j.fertnstert.2005.08.045 [↩] [↩] [↩] [↩] [↩]
- R. K. Patten, R. A. Boyle, T. Moholdt, I. Kiel, W. G. Hopkins, C. L. Harrison, N. K. Stepto. Exercise Interventions in Polycystic Ovary Syndrome: A Systematic Review and Meta-Analysis. Front. Physiol. 11, 606 (2020). https://doi.org/10.3389/fphys.2020.00606 [↩] [↩] [↩] [↩]
- N. Saadati, F. Haidari, M. Barati, R. Nikbakht, G. Mirmomen, F. Rahim. The effect of low glycemic index diet on the reproductive and clinical profile in women with polycystic ovarian syndrome: a systematic review and meta-analysis. Heliyon. 7(11), e08338 (2021). https://doi.org/10.1016/j.heliyon.2021.e08338 [↩] [↩] [↩]
- L. Barrea, A. Arnone, G. Annunziata, G. Muscogiuri, D. Laudisio, C. Salzano, G. Pugliese, A. Colao, S. Savastano. Adherence to the Mediterranean Diet, Dietary Patterns and Body Composition in Women with Polycystic Ovary Syndrome (PCOS). Nutrients 11, 2278 (2019). https://doi.org/10.3390/nu11102278 [↩] [↩]
- E. Arsenaki, D. Stathi, K. K. Triantafyllidis, Y. Seldon, S. Bobotis, G. Lockett, S. Haran, M. Kyrgiou, S. Saso, K. S. Kechagias. The Effects of Ketogenic Diet on Polycystic Ovary Syndrome: A Systematic Review and Meta-Analysis. Clin. Nutr. 56, 106535 (2026). https://doi.org/10.1016/j.clnu.2025.11.019 [↩] [↩]
- K. Indulekha, R. M. Anjana, J. Surendar, V. Mohan. Association of visceral and subcutaneous fat with glucose intolerance, insulin resistance, adipocytokines and inflammatory markers in Asian Indians (CURES-113). Clin Biochem. 44, 281–287 (2011). https://doi.org/10.1016/j.clinbiochem.2010.12.015 [↩] [↩] [↩]
- M. H. Dahan, G. Reaven. Relationship among obesity, insulin resistance, and hyperinsulinemia in the polycystic ovary syndrome. Endocrine. 64, 685–689 (2019). https://doi.org/10.1007/s12020-019-01899-9 [↩] [↩] [↩]
- U. Pandit, M. Singh, R. Ranjan, V. Gupta. The Effect of Exercise Training on Body Composition, Insulin Resistance and High Sensitivity C-reactive Protein (Hs-CRP) in Women With Polycystic Ovary Syndrome: A Pilot Study From North India. Cureus 14, e23994 (2022). https://doi.org/10.7759/cureus.23994 [↩] [↩]
- D. Martin, M. Bonneau, L. Orfila, M. Horeau, M. Hazon, R. Demay, E. Lecommandeur, R. Boumpoutou, A. Guillotel, P. Guillemot, M. Croyal, P. Cressard, C. Cressard, A. Cuzol, V. Monbet, F. Derbré. Atypical gut microbial ecosystem from athletes with very high exercise capacity improves insulin sensitivity and muscle glycogen store in mice. Cell Rep. 44, 115448 (2025). https://doi.org/10.1016/j.celrep.2025.115448 [↩] [↩]
- A. Gratas-Delamarche, F. Derbré, S. Vincent, J. Cillard. Physical inactivity, insulin resistance, and the oxidative-inflammatory loop. Free Rad Res. 48, 93–108 (2013). https://doi.org/10.3109/10715762.2013.847528 [↩] [↩] [↩]
- S. Koçak, H. Çalışkan, G. Ömercioğlu, F. Akat, D. Billur, İ. İnanç, H. Fıçıcılar, M. Baştuğ. The Impact of High-Intensity Interval Training on Insulin Resistance, Oxidative Stress, and Muscle Function in a PCOS Rat Model. Physiol. Behav. 291, 114794 (2025). https://doi.org/10.1016/j.physbeh.2024.114794 [↩] [↩]
- C. M. Burt Solorzano, K. L. Knudsen, A. D. Anderson, E. G. Hutchens, J. S. Collins, J. T. Patrie, J. C. Marshall, C. R. McCartney. Insulin resistance, hyperinsulinemia, and LH: relative roles in peripubertal obesity-associated hyperandrogenemia. The J Clin Endocrinol Metab. 103, 2571–2582 (2018). https://doi.org/10.1210/jc.2018-00131 [↩] [↩]
- H. Nobari, S. Azarian, S. Saedmocheshi, P. Valdés-Badilla, T. García Calvo. Narrative review: The role of circadian rhythm on sports performance, hormonal regulation, immune system function, and injury prevention in athletes. Heliyon. 9, e19636 (2023). https://doi.org/10.1016/j.heliyon.2023.e19636 [↩]
- M. Rubio-Valles, A. Ramos-Jimenez. Effects of aerobic exercise on sleep quality, insomnia, and inflammatory markers: a systematic review and meta-analysis. Curr Issues Mol Biol. 47, 572 (2025). https://doi.org/10.3390/cimb47070572 [↩]
- J. Rong, Y. Wang, N. Liu, L. Shen, Q. Ma, M. Wang, B. Han. Chronic stress induces insulin resistance and enhances cognitive impairment in AD. Brain Res Bull. Online ahead of print (2024). https://doi.org/10.1016/j.brainresbull.2024.111083 [↩]
- R. Gautam, A. M. Prambil, A. K. Patel, T. Arora. Emerging Pollutants in Etiology and Pathophysiology of Polycystic Ovary Syndrome. Reprod. Toxicol. 123, 108515 (2024). https://doi.org/10.1016/j.reprotox.2023.108515 [↩] [↩]
- S. Berdnikovs, H. Abdala-Valencia, L. F. Loffredo, K. Erickson, M. Browning, R. Saber, R. P. Schleimer, A. M. Singh. Systemic imbalance in hormone levels associates with epithelial barrier dysfunction in allergic disease. J Allergy and Clin Immunol. 139, AB263 (2017). https://doi.org/10.1016/j.jaci.2016.12.849 [↩] [↩]
- T. Ghosh, B. Pal, S. Maji, M. Goswami. Understanding polycystic ovarian syndrome and its association with menstrual dysfunction and body fat distribution: A comparative study. Health Med. Online ahead of print (2025). https://doi.org/10.1016/j.hmedic.2025.100215 [↩]



{kind=link}