
Abstract
Background: Traumatic lower-limb amputation has a significant impact on mobility, independence, and social participation and is on the increase, placing an added burden on rehabilitation services. This study investigates the impact of level of amputation on functional, psychological, economic, and vocational outcome for prosthetic SACH users in India because rehabilitation resources are limited and the SACH prostheses are often preferred.
Methods: A cross-sectional study of 20 patients (10 transfemoral, 10 transtibial) of a Narayan Seva Kendra facility was performed. Measures investigated were Comfort Score, Prosthesis Evaluation Questionnaire (PEQ), Extended Social and Community Scale (ESCS), walking speed, daily wear time, vocational, care burden (physiotherapy and repair numbers), and cost of maintenance. Non-parametric statistics compared outcomes across groups.
Results: The transtibial amputees demonstrated significantly greater comfort, mobility, limb health, well-being, and social engagement (p<0.05), as well as higher walking speed (0.70 ± 0.11 m/s vs. 0.58 ± 0.09 m/s; p=0.018). The trend of daily wear time was higher in BK group but was not statistically significant. The level of vocational reintegration was high in both groups (AK 90%, BK 80%). Measures of the care burden were similar, with BK users undergoing more repairs and slightly higher expense. Above-knee users frequently reported socket fit issues whereas, below-knee users described sensations of lightness, stability, and comfort.
Conclusions: Below-knee amputees exhibit better functional and psychosocial outcomes than above-knee amputees in a low-resource rehabilitation setting using SACH prostheses. These findings emphasize knee preservation and appropriate rehabilitation methods that emphasize comfort and ease of maintenance.
Keywords: Comfort, Limb health, Mobility, Prosthetic rehabilitation, Quality of life, Solid ankle cushion heel prosthesis, Transfemoral amputation, Transtibial amputation
Introduction
Amputation is one of the world’s major causes of long-term disability, having a significant impact on the mobility, independence, and social participation of people1,2,3. According to the results of the epidemiological studies, traumatic amputations alone accounted for an estimated 13.23 million new cases worldwide in 2019, equating to an age-standardized incidence rate of 171.23 per 100,000 population. Both the age-standardized incidence and prevalence rates have moderately decreased since 1990, but absolute prevalence has greatly increased-from 370.25 million cases in 1990 to 552.45 million cases in 2019-due to the development of population growth and increasing survival rates following severe trauma. The global burden of disability, expressed as YLDs, was estimated at 7.35 million in 2019, or an ASYR of 90.68 per 100,000 population, with men being disproportionately affected compared to women4. Global Burden of Disease estimates include partial hand, finger, and partial foot amputations in addition to major lower-limb amputations. These figures therefore reflect the overall global burden of amputation rather than incidence specific to lower-limb loss. India has the highest number of amputation cases in the world, with about 2.22 million new cases annually, and 75.6 million people live with limb loss. Traumatic amputation causes the highest rate of disabilities, a total of 1.45 million years lived with disabilities (YLDs) in the country4. The major sources include road traffic injuries, agricultural accidents, and railway-related traumas. Reports from the 1980s estimated approximately 500,000 amputees, with 23,500 new cases occurring every year5,6. Recent findings from Kolkata reported trauma as the major cause in 70.3% of cases, predominantly involving the lower limbs in 94.8% of cases6,7. Despite this alarming situation, prosthetic service coverage is low in India, with only approximately 5% of amputees having access to devices6,7,8. Loss of a limb due to various reasons results in massive biomechanical, functional, and psychosocial challenges that call for holistic rehabilitation with emphasis on mobility, independence, and quality of life. Lower-limb amputations considerably alter the mechanics of gait as well as energy demands; therefore, the design of the prosthesis, the fit of the socket, and integrated components are very important in influencing successful rehabilitation outcomes, including efficiency, comfort, and social participation9. Transtibial amputations were reported to constitute about 67.78% of lower-limb amputations, while about 18.84% were transfemoral amputations10. Given the considerable functional and psychosocial burden following the loss of a lower limb, functional outcomes across amputation levels are sorely needed to be compared for informed rehabilitation planning. The extent of knee preservation, that is, transtibial as opposed to transfemoral amputation, implies a lot in terms of gait biomechanics, mobility potential, energy expenditure, and ultimately, quality of life. It was reported that through-knee amputees maintain the gait parameters of hip range of motion and pelvic stability more like able-bodied walkers compared to their transfemoral amputee counterparts11. These findings emphasize the critical influence of amputation level on both short- and long-term functional outcomes.
One of the most significant factors that define the outcome of rehabilitation is design characteristics. Over the recent 20 years, there have been notable advancements that have produced energy-storing-and-return feet and powered ankle-foot systems that enhance push-off, gait symmetry, and minimize metabolic energy use12,13,14. These technologies are however out of reach to many low- and middle-income countries due to their high costs, lack of availability, and maintenance. Owing to these reasons, the SACH foot is the most recommended solution to individuals with lower-limb amputation in India and other resource-strained environments. While the SACH foot remains widely used in low-resource settings for its cost-effectiveness and simplicity, its rigid, non-energy-return design often delays foot-flat, limits push-off power, and increases compensatory demands, especially on uneven terrain or sloped surfaces. Amputation remains a major global cause of long-term disability, with transtibial amputees demonstrating significantly better functional mobility (e.g. higher Amputee Mobility Predictor scores) than transfemoral amputees, despite comparable daily living index outcomes15. The passive SACH foot, conventionally used in many clinical settings, changes the biomechanics of gait and is associated with compensatory muscle activity, such as increased activation of the hip extensors during stance16. While more advanced prosthetic feet, such as the Re-Flex VSP, clearly offer superior energy efficiency and gait performance not only during walking but also when running17,18, static postural stability under visual conditions seems to be comparable across foot types19. Given these limitations, outcome assessment in amputees with SACH prostheses remains relevant. Inasmuch as the SACH foot is the most common prosthesis used in India and other resource-constrained settings, comparison of functional performance among persons of different amputation levels, while holding the type of prosthesis constant, is informative of the independent contribution of level of amputation to mobility and quality of life.
In line with this technological context, there has been emergence of new service delivery models in India to address the rehabilitation needs of amputees that have not been addressed previously. Narayan Seva Sansthan, one of the leading non-profit organizations in Udaipur, provides free corrective surgeries, prosthetic fitting, rehabilitation, and socio-economic assistance to needy people. This mission is complemented by its Narayan Seva Kendra project which intends to set up 50 Advanced Kendras in 40 cities. Each will incorporate physiotherapy units, limb workshops and vocational training facilities, with at least 10 centres being opened in a year. Such infrastructure not only increases access to prosthetic services but also offers a unique opportunity to systematically evaluate prosthetic outcomes in real-world, resource-constrained environments.
Despite evidence of consistent superior functional mobility and satisfaction of transtibial amputees compared to transfemoral amputees, limited context-specific comparisons exist regarding functional mobility and satisfaction in India and other low middle income countries (LMICs). To fill this gap the current study intends to assess and compare functional performance of above-knee and below-knee amputees with SACH feet, on patient data collected in a Narayan Seva Kendra. The assessment incorporates both patient-reported outcomes, such as comfort, mobility, the health of the residual limb, well-being, and social participation, and performance outcomes, such as walking speed and day-wear time. Besides this, the study involves the analysis of vocational reintegration, care burden markers (e.g., waiting times, physiotherapy sessions), repairs frequency, maintenance costs, and qualitative feedback on the occurrence of the complications with the prosthetics, and design characteristics.
Materials and Methods
Study Design and Participants
The present research is a cross-sectional observational study involving 20 participants with lower-limb amputations who underwent prosthetic rehabilitation at the Narayan Seva Kendra center, India. Two groups were created according to the level of amputation: an Above Knee (AK) group (10 transfemoral amputees) and a Below Knee (BK) group (10 transtibial amputees) with or without preservation of knee.
Prosthesis Fabrication and Components
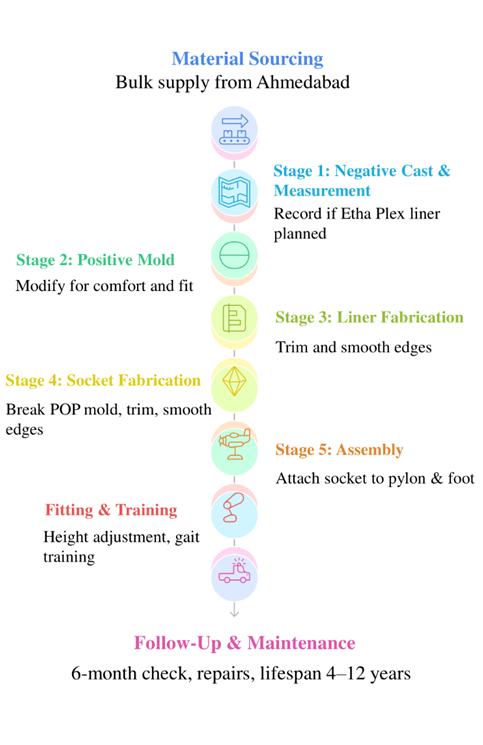
Material Sourcing
- Socket: Polypropylene sheets, sourced from private suppliers in Ahmedabad, chosen for aesthetics, low maintenance, and cost-effectiveness.
- Liner: Etha Plex sheets (thermoplastic elastomer) were heated and vacuum-formed over the limb mold to provide a soft interface.
- Pylon: Aluminum tubes, lightweight and cost-effective, supplied from Ahmedabad.
- Foot: Wooden prosthetic feet (SACH type), sourced from Ahmedabad.
- Sourcing Model & Cost: Materials purchased in bulk for the central fabrication unit. Total cost per limb is ~₹10,000 INR. No recycled materials were used.
Fabrication Process
- Negative Cast & Measurement: Length and circumference of the residual limb measured at the essential points to clarify correct socket fit. Wet plaster of Paris (POP) was used to make a negative cast.
- Positive Mold: Negative cast filled with POP to create a positive mold. Pressure-relief modifications were applied (~1 hour).
- Liner Fabrication: Etha Plex sheets were heated and vacuum-formed over the positive mold; thickness and fit were verified.
- Socket Fabrication: Polypropylene sheets were vacuum-formed over the mold at temperatures of 170–180°C and then the edges of the mold were trimmed and smoothed.
- Assembly: Socket adapter attached to the pylon; pylon connected to foot via foot adapter; nylon straps secured for suspension. Modular design allows individual component replacement.
Fitting & Training
- Initial fitting included height, foot alignment, and stability checks, with minor adjustments as needed.
- Training involved 1–2 days of physiotherapy and gait training (typically 4 hours/day).
Follow-Up & Maintenance
- First follow-up at 6 months. The most common problems were socket looseness caused by changes in residual limb volume and foot/mold wear over 2–3 years.
- Prosthesis lifespan: 4–5 years, potentially up to 10–12 years depending on use. Repair costs ranged from ₹1,000 to ₹10,000 INR. Figure 1 gives a summary of the process. Fit and functional follow-up after 6 months is anticipated.
Data Collection
Baseline demographic and clinical information was collected, including age, sex, amputation level, side, cause of amputation, and liner use. Patient-reported outcome measures included the Comfort Score, the Prosthesis Evaluation Questionnaire (PEQ) subdomains (mobility, residual limb health, and wellbeing), and the Extended Social and Community Scale (ESCS). Verbal administration of all instruments was done in Hindi by trained personnel; questions were paraphrased as required to make them linguistically understandable. Pilot testing was used to prove cultural validation; reliability in the scoring was improved through the use of standard wording, interviewer training, and a standard 0-10 numeric scale. In the case of the PEQ subscales, scoring was done by averaging items per domain. ESCS employed 0-10 scale on appearance, function, durability, and index of activity. Comfort Score used a 0-10 scale (0 = very uncomfortable, 10 = fully comfortable). Functional outcomes included walking velocity (m/s), measured over a 10-meter indoor walkway. Timing started with the first forward step and stopped when both feet crossed the finish line. Two attempts were made and the scores averaged. Subjects were allowed to use their usual assistance devices. Daily prosthesis use (hours/day) was self-reported. Vocational outcomes and cost burden were measured. Successful vocational integration was defined as return to preamputation employment or engagement in new employment/educational activities for ≥20 hours per week within 6 months postprosthesis fitting. Cost burden refers to direct costs related to prosthesis payments, repairs, and transportation, reported in INR.
Statistical Analysis
Data analysis was conducted in IBM SPSS Statistics (version 27). The distribution of continuous variables was determined using the Shapiro–Wilk test. Normally distributed variables are presented as mean ± standard deviation (SD); non-normally distributed data are presented as median with interquartile range (IQR). Categorical variables are summarized as frequencies and percentages. Between-group comparisons (AK vs. BK) were made using the Mann–Whitney U test. A two-tailed p-value < 0.05 was considered statistically significant. Effect sizes (r) were calculated using the formula r = Z/√N (N = 20). Because of sample size limitations, multivariable adjustment for confounders including age, cause of amputation, time since amputation, and other comorbidities could not be performed. These statistics have been reported alongside p-values to enhance interpretability. A limited sensitivity analysis was conducted for the one participant who was initially classified as transtibial but was, in fact, a knee-disarticulation case. After this participant had been excluded, the primary outcome variables were re-analyzed: Comfort Score, PEQ mobility, PEQ residual limb health, PEQ wellbeing, and ESCS. The p-values (Table S1) that resulted from this did not meaningfully differ from those of the primary analysis, and therefore, this participant’s misclassification did not materially affect group comparisons.
Results
Baseline Characteristics
A total of 20 patients were included, evenly divided between AK and BK prosthesis users. The cohort was relatively young, with a mean age of 29.0 ± 6.1 years, and comparable age distribution across groups. The majority were male (75%). By design, all transfemoral amputations were managed with AK prostheses, whereas almost all BK cases were transtibial (including one knee-preserving case). Road traffic accidents accounted for the predominant cause of amputation (70%), followed by less frequent etiologies such as congenital absence (5%) and miscellaneous traumatic or electrical injuries (25%). Right-sided amputations were marginally more common than left-sided (55% vs. 45%). Notably, liner use differed substantially by prosthesis type, being universal among below-knee users but rare in the above-knee group (10%). Where applied, the liner was composed of Etha-Flex. All members of this cohort were fit with polypropylene sockets except for a single transfemoral user who was provided an SDPE socket. Information on the type of pylon used was available and was aluminum for all; all the feet were SACH. Baseline demographic and clinical characteristics of the study subjects are outlined in Table 1 for AK and BK amputation levels.
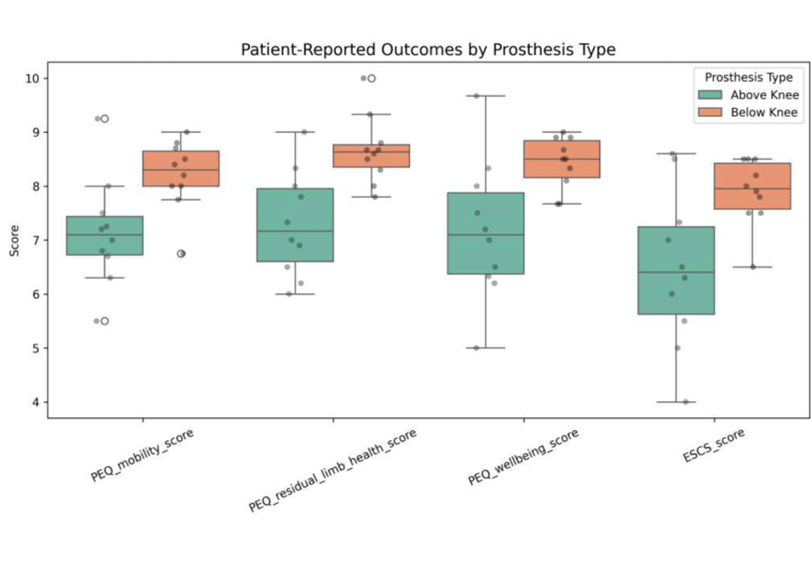
Patient-Reported Outcomes
Patients with BK prostheses outperformed AK users in all domains assessed (Table 2, Figure 2). They were significantly more comfortable, mobile, and had better residual limb health and wellbeing, and these differences reached statistical significance. Even social participation, as quantified by ESCS scores, was favorable for BK users. To correspond with the patient self-reported outcomes, performance-based measures indicated that walking speed was significantly higher in the BK group, confirming indeed that patients within this group had more efficient gait mechanics. Although daily prosthesis wear time was longer in BK users, the differences did not reach statistical significance. Taken together, the results indicate that BK prostheses have functional and psychosocial advantages over AK devices.
| Outcome | Above Knee (Mean ± SD) | Above Knee (Median [IQR]) | Below Knee (Mean ± SD) | Below Knee (Median [IQR]) | Effect Size | p-value |
| Comfort score | 6.5 ± 1.08 | 6.5 [5.75–7.25] | 8.5 ± 0.71 | 9 [8–9] | 0.76 | <0.001* |
| PEQ mobility score | 7.15 ± 1.00 | 7.1 [6.60–7.63] | 8.21 ± 0.65 | 8.3 [7.94–8.73] | 0.54 | 0.015* |
| PEQ residual limb health score | 7.31 ± 0.97 | 7.17 [6.43–8.08] | 8.67 ± 0.63 | 8.64 [8.23–8.93] | 0.63 | 0.005* |
| PEQ wellbeing score | 7.17 ± 1.30 | 7.1 [6.30–8.08] | 8.42 ± 0.48 | 8.5 [7.99–8.9] | 0.58 | 0.009* |
| ESCS score | 6.47 ± 1.46 | 6.4 [5.38–7.62] | 7.89 ± 0.62 | 7.95 [7.5–8.5] | 0.49 | 0.028* |
| Walking Speed (m/s) | 0.58 ± 0.09 | 0.55 [0.51-0.68] | 0.70 ± 0.11 | 0.70 [0.62-0.82] | 0.53 | 0.018* |
| Daily use (hours) | 7.30 ± 2.21 | 7 [5.75-8.50] | 11.50 ±12.87 | 8 [7-8.25] | 0.27 | 0.231 |
| * Represents statistically significant association computed via Mann–Whitney U test. r = Z/√N | ||||||
Mann–Whitney U statistics and corresponding effect sizes supported the significant differences across comfort and PEQ domains (U = 6.5–21.0; r = 0.49–0.76), indicating medium to large effects (Table S2).
Return to Work and Functionality
Vocational reintegration was broadly favorable in both groups. In the AK group, 60% were employed, 20% were students, and 20% were unemployed prior to prosthesis fitting. Following rehabilitation, 70% were employed and 20% remained students. One individual who had been unemployed before amputation subsequently entered education; however, this case was coded as not applicable in the return-to-work analysis, as it represented a transition from unemployment to studying rather than re-engagement with prior vocational or educational activities. Overall, 9 of 10 patients (90%) were recorded as having successfully reintegrated into work or education. The study found that in the BK group, 90 per cent of patients were employed and 10 per cent were students at the time of receiving the prosthesis. After prosthesis installation, 70% of them continued to work and 10% of them went back to school, and two of them (20%) shifted to unemployment despite their previous exposure to employment. The overall result was 8 out of 10 patients (80%) became successfully reintegrated into work or education.
Care and Economic Outcomes
The waiting time in patients who received AK prostheses was marginally higher than that of patients who received BK prostheses (3.00 [2.00-3.00] days versus 2.50 [1.75-3.00] days), but the difference was not significant (p = 0.305, r = 0.23). Similarly, there was no significant differences in physiotherapy sessions between the AK and BK, with the former having 3.00 [2.00-3.25] and the latter 2.50 [1.75-4.75] physiotherapy sessions (p = 0.846, r = 0.04). Regarding the repairs of the devices, most of the patients in each group did not need any intervention; nevertheless, repair needs were more frequent and intense in case of BK users. Four patients in the AK group and six patients in the BK group needed repairs (1-4 times each and 1-6 times), respectively. The median [IQR] number of repair was 0.00 [0.00-1.25] in the AK group relative to 1.00 [0.00-2.50] in the BK group. Although this trend was towards increased burden, the difference was not statistically significant (p = 0.370, r = 0.20). Maintenance costs also had significant variation. Maintenance costs also showed substantial variation. Above Knee users reported a median [IQR] of 150.00 [0.00–1700.00] INR compared to 400.00 [0.00–6500.00] INR in the BK group; however, the difference was not statistically significant (p = 0.572, r = 0.13). Overall, these results imply that though there was overall similarity in care burden in terms of waiting days and physiotherapy sessions among groups, BK prostheses were related to more variability in repairs and higher maintenance prices, but these findings were not statistically significant (Table S3).
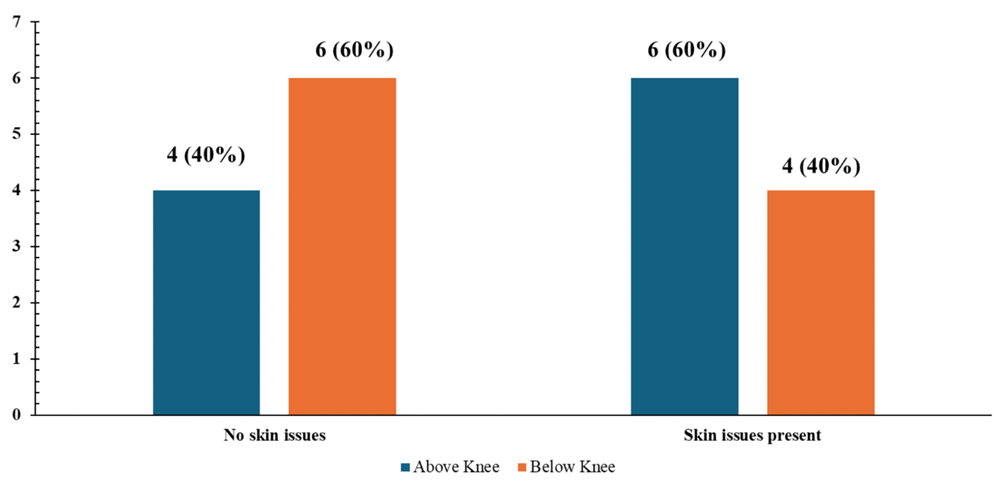
Prosthesis-Related Complications and User Experience
Skin problems were frequently reported but were of mild nature. Above Knee complaints included recent irritation, redness occasionally, seasonal rashes, or blisters during initial use, discomfort following long use was reported by some of the participants. In comparison, the users of BK were less often affected, and the issues were mostly restricted to redness or blisters post-long days of activity. Most BK users did not complain of persistent skin problems (Figure 3). Additional context was given by qualitative feedback. Among AK users, the primary issue was associated with weight, socket fit, and liner comfort. Particular concerns were the difficulty in weight (heavy, yet durable), the loosening of the socket in hot weather, and the necessity of soft liners. However, there were positive experiences described by some AK patients, including comfort in long walks and stability. BK users experienced more positive feedback, and some mentioned the prosthesis as lightweight, natural and suitable for long distances. Nevertheless, there were also certain limitations reported, such as a desire to move the foot more often, a feeling of heaviness of certain types of socks, and difficulties with adjustments initially (especially with the bent-knee version).
Together, BK prostheses were associated with more positive user experiences, whereas AK users frequently noted device weight and comfort challenges. These qualitative findings complement the quantitative outcomes, underscoring the functional and psychosocial differences between prosthesis types.
Discussion
The present study assessed functional and psychosocial differences between above-knee and below-knee prosthesis users, where all subjects were fitted with SACH feet. In settings where evidence on patient-reported outcomes with conventional prostheses is limited, these findings help clarify how the level of amputation affects comfort, mobility, and daily reintegration when device type is kept consistent. Our observations align with long-standing clinical patterns: individuals with BK amputations generally report better comfort, mobility, and overall satisfaction than those with AK amputations. In this cohort, the mean comfort score was 8.5 for BK users compared with 6.5 for AK users (p<0.001), representing an approximate 2-point, or 23%, difference. Prior studies have also shown that transtibial amputees perceive less weight burden and express higher satisfaction with their prostheses than transfemoral users20,21,22. Although BK participants in our study showed a tendency to report longer wear times and higher comfort ratings, not all the differences reached statistical significance; therefore, this represents a consistent trend but does not provide conclusive evidence across all measures.
Similar findings have been described in Rwanda, where, 62.2% of transtibial prosthesis users reported satisfaction with their device23. Berk and colleagues reported overall satisfaction from 91% of transtibial and 78% transfemoral amputees with their prostheses24. In Cambodia, it was demonstrated that LLPU average ~4470 steps/day and wear the device for 13.4 hours/day, demonstrating significant daily use of the device25. More recently, a large number of people using inexpensive prosthetic devices in Malawi and Sierra Leone reported regular mobility, including walking more than one kilometer26. These reports indicate that even simple prosthesis provision can result in significantly improved functional outcomes in resourcepoor contexts. The same trend is evident in mobility results: in one comparison, BK users demonstrated faster self-selected gait speeds (0.70 versus 0.58 m/s, p=0.018) and higher Prosthetic Evaluation Questionnaire mobility scale scores (8.21 versus 7.15, p=0.015). Results are consistent with observational studies and systematic reviews that report individuals with distal (transtibial) amputations are generally more able to improve their walking capacity and engage more easily in daily activities than individuals with proximal (transfemoral) amputations27,28. Sinha and colleagues also reported that transtibial amputees rated the weight of their prostheses more favorably than transfemoral users; this difference reached statistical significance29. Field-based research in low-resource settings underlines these findings, demonstrating that transfemoral users experience additional difficulty with chair transfers, stair climbing, and navigating uneven terrain, as well as wearing their prostheses for fewer hours per day22,23,24,25,26,27,28,29,30. Daily-use data underscore this difference. A meta-analysis described significantly longer wear times among distal amputees (13.2 vs. 10.8 hours/day, p<0.001)31. Indeed, field studies of both adolescents and adults have described higher step counts among BK users, including 4,577 versus 2,551 steps/day in post-earthquake settings25,26,27,28,29,30,31,32 This difference, although suggesting a real difference between BK and AK amputee mobility, did not reach statistical significance; this is most likely due to limited sample size rather than an absence of any real effect.
Patient-reported residual-limb health and psychosocial well-being also strongly favored the BK group (PEQ limb health: 8.67 vs 7.31, p = 0.005; PEQ well-being: 8.42 vs 7.17, p = 0.009). The uneven distribution of liners was another major confounder for limb health and comfort. All BK users had an uneven distribution, whereas only one AK user did. Liners contribute to the comfort of the socket, skin protection, and pressure distribution. Therefore, this could be a reason for the inequality between the two groups. These findings corroborate previous physiological and biomechanical studies. Rink et al. established a non-invasive technique for skin health assessment in amputees showing compromised skin barrier function, especially in transfemoral users, due to socket fitting problems and increased soft tissue stress33.
Correspondingly, Baumann et al. found that better socket fit enhanced soft-tissue outcomes and reduced stump pain, advantages more easily achieved with BK prostheses, emphasizing that residual-limb health and comfort are linked to well-being overall34. Consistently, clinical studies and reviews have compared the health-related quality of life of transtibial amputees as generally better compared to that of transfemoral amputees. For instance, in an older amputee population, it was observed that individuals with transtibial amputations had a better quality of life than those with transfemoral amputations35. Despite the lower age of our population, the general trend held true: there are significant psychological and physical benefits to the preservation of the knee joint. It was later discovered that one person previously classified as “transtibial (knee preserved)” had undergone a knee-disarticulation amputation. Stability of these findings is illustrated by the fact that a sensitivity analysis excluding this subject did not change the direction or statistical significance of our findings. Improved mobility and comfort likely also contributed to higher self-reported social participation scores on the ESCS for BK prosthetics. By contrast, AK participants frequently cited socket discomfort, heat buildup, and excessive weight in open comments, well-documented limitations of conventional transfemoral prostheses22,23,24,25,26,27,28,29.
Objective gait analyses confirm the biomechanical and functional benefits of BK prostheses over AK devices. Quantitative analyses have shown significantly lower gait variability and greater symmetry in transtibial amputees compared with transfemoral amputees, with the performance of the former approaching that of healthy controls36. It is plausible that these biomechanical advantages are the underlying cause of the better psychosocial outcomes and the increased social participation score in our BK cohort. Conversely, socket discomfort, heat build-up, and heavy prostheses were common in the open comments of AK participants and are ongoing limitations connected to traditional transfemoral fittings. Together with these self-reports, randomized trials and clinical observations have shown that although socket design has a minimal effect on skeletal kinematics, it is one of the most important factors contributing to user comfort and satisfaction37. Our study also reported a high rate of vocational reintegration (80–90% back to work or school), which was higher than the previous reported estimates of 43-70%38,39. This probably corresponds to our younger and trauma-healing generation in conjunction with the intensive-rehabilitation measures. In fact, the initial longitudinal investigations have shown that civilian traumatic amputees tend to resume employment similar to the general population 52-70% in the U.S. and more than 95% in select Europe, based on the health care and vocational support offered40,41,42 ,43 ,44 . In our study, the reintegration in both BK and AK groups was high with slight discrepancy, 90% in AK and 80% vocational return in our setting is less influenced by amputation level than by social and rehabilitation factors.
Return-to-work (RTW) after lower-limb amputation involves multiple interrelated factors. Older age at the time of amputation, lower educational attainment, pre-amputation employment in physically demanding jobs, poor prosthetic comfort, and limited ability to adapt to less strenuous roles all tend to reduce the likelihood of successful re-employment45,46. In general amputee populations, documented RTW rates remained around 79%, with comfort of prosthetic fit and higher education emerging as consistent predictors of better reintegration46. Thai cohort data report the occupational reintegration rate for trauma and lower limb cases to be 66.7%. Factors related to RTW include younger age, more prosthetic comfort, and the use of gait aids47. In the Netherlands, stump-related complications and problems of wound healing usually postpone RTW for an average of 11.5 months. Half of the amputees return to different or modified jobs due to physical limitations48.
In terms of prosthetic care, there was no significant difference in the initial wait time or physiotherapy requirements in both groups of our study. There was a tendency to increase repair requirements and maintenance expenses among BK users (median INR 400 vs. INR 150), but no statistically significant results were observed. The burden of repair by the level of amputation has not been widely studied. Increased daily use in more active BK users may lead to more wear, although evidence is limited. In both groups, waiting times for their devices were reasonable, medians of ~2–3 days, with minimal numbers of rehab sessions, 2–3, hence service delivery was efficient and equitably provided. Prosthesis complications were as expected: 60% of AK users and 40% of BK users reported skin issues, including irritation and blistering. However, they are still moderate as compared to reported prevalence: in one survey in 73.9% of amputees, skin complications were reported49, and among the military, long-term follow-ups showed 48.2% with stump dermatoses, and 55.6% with effects on prosthesis use and great discomfort50. BK users have a lower incidence which is probably due to the lighter load in the below-knee prostheses. Most of the problems found in our cohort were mild and limited to the initial adaptation period. The added complexity and interface space of above-knee prostheses was also reflected in socket weight and fit during use AK users also reported weight and fit problems. Findings indicated that about 36-63% of lower-limb prosthesis patients suffered skin damage, and ill-fitting sockets had been reported as significant factors leading to discomfort, skin breakdown and subsequent prosthesis abandonment51,52,53. On the other hand, BK users reported the natural sensation and perceived stability of their artificial limbs, but some reported limited ankle movement and difficulty in initial adjustment with reduced proprioception and equilibrium54,55. The findings from the present work suggest that BK prostheses confer quantifiable benefits for comfort, mobility, limb health, and overall well-being. This is in line with the current worldwide evidence showing increased physical quality of life and gait function at lower levels of amputation.
The limitation of the present study is that the sample size is very small, which limits the generalization and prevented the multivariation of the study by adjustment of possible confounding variables like the age, cause of amputation, and comorbidities. A BK group participant was misclassified as transtibial (knee kept) but represented a knee-disarticulation case; sensitivity analysis revealed that omission of this participant did not change outcomes significantly. Also, the asymmetrical distribution of the prosthetic liners (100% in BK and 10% in AK) might have contributed to the effect on comfort, health of the residual limb, and functional results. With the sample size and number of outcomes assessed, there is a greater risk of Type I error. No correction for multiple comparisons has been applied, as the purpose of this paper is exploratory in nature, and results should be considered accordingly. Further research on large and more balanced samples is required to validate these results and enhance external validity.
Conclusion
The present study shows that the BK (transtibial) amputees equipped with standardised SACH-foot prosthesis and polypropylene sockets have enhanced comfort, mobility, limb health, well-being, social participation, and more efficient gait compared to their AK counterparts. Both groups achieved high rates of vocational reintegration, underscoring the strong impact of prompt prosthetic rehabilitation. Although BK patients tended to require repairs and maintenance slightly more often, these factors did not diminish their functional advantages. Skin complications were mild in general and well-managed. Overall, the results point to the functional benefits of preserving the knee joint when this is possible. Among participants with transfemoral amputations, enhanced socket design, the liner technologies, and prosthetic knee mechanics could all play a role in reducing residual functional limitations as much as possible.
Appendix
A Comparative Analysis of Functional, Economic, and Vocational Outcomes in Transtibial vs. Transfemoral Amputees within a Non-Profit Rehabilitation Framework
| Variable | U | Z | p-value | r |
| Comfort score | 6.50 | –3.22 | 0.001 | 0.74 |
| PEQ Mobility Score | 17.0 | -2.290 | 0.022 | 0.53 |
| PEQ Residual Limb Health | 12.0 | -2.697 | 0.007 | 0.62 |
| PEQ Wellbeing Score | 14.0 | -2.534 | 0.011 | 0.58 |
| ESCS Score | 19.5 | -2.088 | 0.037 | 0.48 |
| Walking Speed | 14.0 | -2.545 | 0.011 | 0.58 |
| Daily Use Hours | 25.5 | -1.634 | 0.102 | 0.37 |
| Effect size (r) was calculated using r = Z/√N, where . N=19 | ||||
| Outcome | Group | 95% CI (Lower–Upper) | U | Z | Effect size and Magnitude |
| Comfort score | AK | 5.50 – 7.00 | 6.5 | –3.378 | 0.76 (Large) |
| BK | 8.00 – 9.00 | ||||
| PEQ mobility | AK | 6.50 – 7.50 | 18.0 | –2.423 | 0.54 (Medium-large) |
| BK | 8.00 – 8.70 | ||||
| PEQ residual limb health | AK | 6.50 – 8.07 | 13.0 | –2.800 | 0.63 (Large) |
| BK | 8.30 – 8.80 | ||||
| PEQ wellbeing | AK | 6.27 – 8.00 | 15.5 | –2.612 | 0.58 (Large) |
| BK | 8.10 – 8.90 | ||||
| ESCS score | AK | 5.25 – 7.33 | 21.0 | –2.202 | 0.49 (Medium-large) |
| BK | 7.50 – 8.50 | ||||
| Walking Speed (m/s) | AK | 0.51 – 0.68 | 19.0 | –2.357 | 0.53 (Large) |
| BK | 0.61 – 0.82 | ||||
| Daily Use (hours) | AK | 5.50 – 8.00 | 34.5 | –1.199 | 0.27 (Small-medium) |
| BK | 7.00 – 8.00 | ||||
| bootstrapped 95% CIs for medians Effect size (r) was calculated using r = Z/√N, where . N=20 | |||||
| Outcome | Group | 95% CI (Lower–Upper) | U | Z | Effect size and Magnitude |
| Waiting days | AK | 2.00 – 3.00 | 37.5 | -1.026 | 0.23 (Small-medium) |
| BK | 1.50 – 3.00 | ||||
| Physiotherapy sessions | AK | 2.00 – 3.50 | 47.5 | -0.194 | 0.04 (Negligible / Small) |
| BK | 1.50 – 5.00 | ||||
| Device repairs | AK | 0.00 – 1.50 | 39.0 | -0.897 | 0.20 (Small) |
| BK | 0.00 – 2.49 | ||||
| Maintenance cost (INR) | AK | 0.00 – 2798.73 | 43.0 | -0.566 | 0.13 (Small) |
| BK | 0.00 – 6000.00 | ||||
| Bootstrapped 95% CIs for medians Effect size (r) was calculated using r = Z/√N, where . N=20 | |||||
References
- Tasnim F. Impact of social participation of the patient with amputation. Bangladesh Health Professions Institute, Faculty of Medicine, the University …; 2023. [↩]
- Al-Eqabi Q, Niazy S, Radhi M. Amputation-related factors influencing activities of daily living among amputees. Iranian Journal of War and Public Health. 2024;16(2):123-9. [↩]
- Liu Z, Wang M, Liu Q, Huang B, Teng Y, Li M, et al. Global trends and current status of amputation: Bibliometrics and visual analysis of publications from 1999 to 2021. Prosthetics and Orthotics International. 2024;48(5):603-15. [↩]
- Yuan B, Hu D, Gu S, Xiao S, Song F. The global burden of traumatic amputation in 204 countries and territories. Frontiers in public health. 2023;11:1258853. [↩] [↩]
- Mohan D. A report on amputees in India. Orthot Prosthet. 1986;40(1):16-32. [↩]
- Swarnakar R, Yadav SL, Surendran D. Lower limb amputation rehabilitation status in India: A review. World Journal of Clinical Cases. 2023;11(30):7261. [↩] [↩] [↩]
- Pooja GD, Sangeeta L. Prevalence and aetiology of amputation in Kolkata, India: A retrospective analysis. Hong Kong Physiotherapy Journal. 2013;31(1):36-40. [↩] [↩]
- Seymour R. Prosthetics and orthotics: lower limb and spinal. Lippincott Williams & Wilkins; 2002. [↩]
- Lathouwers E, Diaz MA, Maricot A, Tassignon B, Cherelle C, Cherelle P, et al. Therapeutic benefits of lower limb prostheses: a systematic review. Journal of NeuroEngineering and Rehabilitation. 2023;20(1):4. [↩]
- Singh G, Pithawa A, VSM GR. Study of disabled treated at artificial limb centre. Medical Journal Armed Forces India. 2009;65(3):232-4. [↩]
- Panhelleux B, Silverman A, McGregor A. Lower limb kinematics and kinetics of people with through-knee amputation compared to individuals with transfemoral amputation and able-bodied controls during walking. Journal of Biomechanics. 2025;184:112649. [↩]
- LeMoyne R. Energy Storage and Return (ESAR) Prosthesis. Advances for Prosthetic Technology: From Historical Perspective to Current Status to Future Application. Springer; 2016. p. 69-76. [↩]
- Ventura JD, Klute GK, Neptune RR. The effect of prosthetic ankle energy storage and return properties on muscle activity in below-knee amputee walking. Gait & posture. 2011;33(2):220-6. [↩]
- Mazzarini A, Fagioli I, Eken H, Livolsi C, Ciapetti T, Maselli A, et al. Improving walking energy efficiency in transtibial amputees through the integration of a low-power actuator in an ESAR foot. IEEE Transactions on Neural Systems and Rehabilitation Engineering. 2024;32:1397-406. [↩]
- Seker A, Kara A, Camur S, Malkoc M, Sonmez MM, Mahirogullari M. Comparison of mortality rates and functional results after transtibial and transfemoral amputations due to diabetes in elderly patients-a retrospective study. Int J Surg. 2016;33 Pt A:78-82. doi: 10.1016/j.ijsu.2016.07.063. [↩]
- Winter DA, Sienko SE. Biomechanics of below-knee amputee gait. J Biomech. 1988;21(5):361-7. doi: 10.1016/0021-9290(88)90142- x. [↩]
- Hsu MJ, Nielsen DH, Yack HJ, Shurr DG. Physiological measurements of walking and running in people with transtibial amputations with 3 different prostheses. J Orthop Sports Phys Ther. 1999;29(9):526-33. doi: 10.2519/jospt.1999.29.9.526. [↩]
- Houdijk H, Wezenberg D, Hak L, Cutti AG. Energy storing and return prosthetic feet improve step length symmetry while preserving margins of stability in persons with transtibial amputation. Journal of neuroengineering and rehabilitation. 2018;15(Suppl 1):76. [↩]
- Arifin N, Abu Osman NA, Ali S, Wan Abas WAB. The effects of prosthetic foot type and visual alteration on postural steadiness in below-knee amputees. Biomedical engineering online. 2014;13(1):23. [↩]
- Baars EC, Schrier E, Dijkstra PU, Geertzen JH. Prosthesis satisfaction in lower limb amputees: a systematic review of associated factors and questionnaires. Medicine. 2018;97(39):e12296. [↩]
- Manz S, Valette R, Damonte F, Avanci Gaudio L, Gonzalez-Vargas J, Sartori M, et al. A review of user needs to drive the development of lower limb prostheses. Journal of neuroengineering and rehabilitation. 2022;19(1):119. [↩]
- Magnusson L, Ramstrand N, Fransson EI, Ahlström G. Mobility and satisfaction with lower-limb prostheses and orthoses among users in Sierra Leone: a cross-sectional study. Journal of rehabilitation medicine. 2014;46(5):438-46. [↩] [↩] [↩]
- Butoya P, de Dieu Rukundo J, Gatsinzi JM, Ngulube DJ, Kemigisha J, Izere D, et al. Satisfaction with Prosthesis and Walking Ability among Trans-Tibial Prosthesis Users from Two Selected Rehabilitation Hospitals in Rwanda. Rwanda Journal of Medicine and Health Sciences. 2025;8(1):75-88. [↩] [↩] [↩]
- 2009;41(8):593-603Berke GM, CP F, L-CPO JH, Nguyen V. Comparison of satisfaction with current prosthetic care in veterans and servicemembers from Vietnam and OIF/OEF conflicts with major traumatic limb loss. Journal of rehabilitation research and development. 2010;47(4):361. [↩] [↩] [↩]
- Diment L, Nguon R, Seng S, Sit V, Lors P, Thor P, et al. Activity, socket fit, comfort and community participation in lower limb prosthesis users: a Cambodian cohort study. Journal of neuroengineering and rehabilitation. 2022;19(1):42. [↩] [↩] [↩] [↩]
- Magnusson L, Ahlström G. Patients’ Satisfaction with Lower-limb Prosthetic and Orthotic Devices and Service delivery in Sierra Leone and Malawi. BMC Health Serv Res. 2017;17(1):102. doi: 10.1186/s12913-017-2044-3. [↩] [↩] [↩] [↩]
- Sansam K, Neumann V, O’Connor RJ, Bhakta B. Predicting walking ability following lower limb amputation: a systematic review of the literature. Journal of rehabilitation medicine. 2009;41(8):593-603. [↩] [↩] [↩] [↩]
- Kahle JT, Highsmith MJ, Schaepper H, Johannesson A, Orendurff MS, Kaufman K. Predicting walking ability following lower limb amputation: an updated systematic literature review. Technology & Innovation. 2016;18(2-3):125-37. [↩] [↩] [↩] [↩]
- Sinha R, van den Heuvel WJ, Arokiasamy P. Adjustments to amputation and an artificial limb in lower limb amputees. Prosthetics and orthotics international. 2014;38(2):115-21. [↩] [↩] [↩] [↩]
- Magnusson L, Ahlström G. Patients’ satisfaction with lower-limb prosthetic and orthotic devices and service delivery in Sierra Leone and Malawi. BMC health services research. 2017;17(1):102. [↩] [↩]
- Paquette R, Highsmith MJ, Carnaby G, Reistetter T, Phillips S, Hill O. Duration, frequency, and factors related to lower extremity prosthesis use: systematic review and meta-analysis. Disability and rehabilitation. 2024;46(20):4567-85. [↩] [↩]
- Chu CKG, Wong MS. Comparison of prosthetic outcomes between adolescent transtibial and transfemoral amputees after Sichuan earthquake using Step Activity Monitor and Prosthesis Evaluation Questionnaire. Prosthetics and orthotics international. 2016;40(1):58-64. [↩]
- Rink CL, Wernke MM, Powell HM, Tornero M, Gnyawali SC, Schroeder RM, et al. Standardized approach to quantitatively measure residual limb skin health in individuals with lower limb amputation. Advances in Wound Care. 2017;6(7):225-32. [↩]
- Baumann M, Price C, Brousseau L, Loftsgaarden M, Powell J, Sanders J, et al. The relationship between residual limb health, motion within the socket, and prosthetic suspension. PM&R. 2023;15(4):510-21. [↩]
- Brunelli S, Bonanni C, Foti C, Traballesi M. A literature review of the quality of life, health status and prosthesis satisfaction in older patients with a trans-tibial amputation. Canadian prosthetics & orthotics journal. 2020;2(1):33640. [↩]
- Keklicek H, Kirdi E, Yalcin A, Topuz S, Ulger O, Erbahceci F, et al. Comparison of gait variability and symmetry in trained individuals with transtibial and transfemoral limb loss. Journal of orthopaedic surgery. 2019;27(1):2309499019832665. [↩]
- Kahle J, Miro RM, Ho LT, Porter M, Lura DJ, Carey SL, et al. The effect of the transfemoral prosthetic socket interface designs on skeletal motion and socket comfort: A randomized clinical trial. Prosthetics and orthotics international. 2020;44(3):145-54. [↩]
- Penn-Barwell JG. Outcomes in lower limb amputation following trauma: a systematic review and meta-analysis. Injury. 2011;42(12):1474-9. [↩]
- Burger H, Marinček Č. Return to work after lower limb amputation. Disability and rehabilitation. 2007;29(17):1323-9. [↩]
- Pezzin LE, Dillingham TR, MacKenzie EJ. Rehabilitation and the long-term outcomes of persons with trauma-related amputations. Archives of physical medicine and rehabilitation. 2000;81(3):292-300. [↩]
- Georgiadis GM, Behrens FF, Joyce MJ, Earle AS, Simmons AL. Open tibial fractures with severe soft-tissue loss. Limb salvage compared with below-the-knee amputation. JBJS. 1993;75(10):1431-41. [↩]
- Puno RM, Grossfeld SL, Henry SL, Seligson D, Harkess J, Tsai TM. Functional outcome of patients with salvageable limbs with grades III‐B and III‐C open fractures of the tibia. Microsurgery: Official Journal of the International Microsurgical Society and the European Federation of Societies for Microsurgery. 1996;17(3):167-73. [↩]
- Francel TJ, Vander Kolk CA, Hoopes JE, Manson PN, Yaremchuk MJ. Microvascular soft-tissue transplantation for reconstruction of acute open tibial fractures: timing of coverage and long-term functional results. Plastic and reconstructive surgery. 1992;89(3):478-87. [↩]
- Livingston DH, Keenan D, Kim D, Elcavage J, Malangoni MA. Extent of disability following traumatic extremity amputation. Journal of Trauma and Acute Care Surgery. 1994;37(3):495-9. [↩]
- Darter BJ, Hawley CE, Armstrong AJ, Avellone L, Wehman P. Factors Influencing Functional Outcomes and Return-to-Work After Amputation: A Review of the Literature. J Occup Rehabil. 2018;28(4):656-65. doi: 10.1007/s10926-018-9757-y. [↩]
- Schoppen T, Boonstra A, Groothoff JW, van Sonderen E, Göeken LN, Eisma WH. Factors related to successful job reintegration of people with a lower limb amputation. Arch Phys Med Rehabil. 2001;82(10):1425-31. doi: 10.1053/apmr.2001.26074. [↩] [↩]
- Dajpratham P, Tantiniramai S, Lukkapichonchut P, Kaewnaree S. Factors associated with vocational reintegration among the Thai lower limb amputees. J Med Assoc Thai. 2008;91(2):234-9. [↩]
- Bruins M, Geertzen J, Groothoff J, Schoppen T. Vocational reintegration after a lower limb amputation: a qualitative study. Prosthetics and orthotics international. 2003;27(1):4-10. [↩]
- Koc E, Tunca M, Akar A, Erbil AH, Demiralp B, Arca E. Skin problems in amputees: a descriptive study. International journal of dermatology. 2008;47(5):463-6. [↩]
- Yang NB, Garza LA, Foote CE, Kang S, Meyerle JH. High prevalence of stump dermatoses 38 years or more after amputation. Archives of dermatology. 2012;148(11):1283-6. [↩]
- Meulenbelt HE, GEERTzEN JH, JONkMAN MF, DIJkSTRA PU. Skin problems of the stump in lower limb amputees: 1. A clinical study. Acta dermato-venereologica. 2011;91(2):173-7. [↩]
- Meulenbelt HE, GEERTzEN JH, JONkMAN MF, Dijkstra PU. Skin problems of the stump in lower limb amputees: 2. influence on functioning in daily life. Acta dermato-venereologica. 2011;91(2):178-82. [↩]
- Dudek NL, Marks MB, Marshall SC, Chardon JP. Dermatologic conditions associated with use of a lower-extremity prosthesis. Archives of physical medicine and rehabilitation. 2005;86(4):659-63. [↩]
- Turner S, McGregor AH. Perceived effect of socket fit on major lower limb prosthetic rehabilitation: a clinician and amputee perspective. Archives of rehabilitation research and clinical translation. 2020;2(3):100059. [↩]
- Lyon CC, Kulkarni J, Zimersonc E, Van Ross E, Beck MH. Skin disorders in amputees. Journal of the American Academy of Dermatology. 2000;42(3):501-7. [↩]



{kind=link}