 interactin")
Abstract
Gut microbiota dysbiosis is a condition in which there is a lack of diversity in the microbes that colonize the gut microbiome. Mental health disorders like depression are one of the most prevalent diseases on a global scale. While there are a plethora of treatments for depression, none of these specifically target gut dysbiosis which has been implicated in the pathophysiology of depression. The gut-brain axis is the neural system that connects these two structures. Through the gut-brain axis, a healthy and diverse gut might stand to improve host brain health and minimize the risk of depression. The objective of this systematic review is to answer whether or not prebiotics or probiotics are a necessary intervention for depression through their impact on gut dysbiosis. From this review, it was uncovered that probiotics and prebiotics could be possible interventions for depression because of their ability to restore homeostasis in the gut which in turn eliminates pathogenic microbes that are involved in the process of synthesizing metabolites that tend to be elevated in depressed individuals. Additionally, these supplements may promote the growth of beneficial microbes involved in the synthesis of neurotransmitters that affect mood and mental health.
Introduction
The thousands of microorganisms that colonize the Gastrointestinal tract form what is known as the gut microbiome1. The gut microbiome is involved in modulating human metabolism, the digestive system, and immune function. A healthy and diverse gut microbiome works to recover energy from the metabolism of non-digestible fibers and helps to protect the host from pathogenic invasion and disease2. The microbiota is composed of archaea, viruses, eukaryotic, and prokaryotic microbes. Specifically, prokaryotic bacteria are especially abundant; there are roughly 500 to 1,000 unique species that contribute to nearly 2 million genes in the gut microbiome3. The common bacterial phyla in the gut microbiota are Firmicutes, Bacteroidetes, Actinobacteria, Proteobacteria, Fusobacteria, and Verrucomicrobia4.
Gut microbiome dysbiosis describes an imbalance in the diversity of microbes that colonize the gut. The gut microbiome is an ecosystem and like all ecosystems, requires biodiversity to maintain stability, resilience, and robustness5. The gut microbiota requires a diverse abundance of different bacterial species because a lack of diversity has been known to negatively affect the host. Gut microbiota dysbiosis is linked to host inflammation, and frailty, and has also been linked to multiple neurogenic disorders by causing motor deficits and microglial activation6.
All 500 to 1,000 unique species of bacteria are important, even if one taxa were to somehow be removed from the gut, the entire microbiota would have an entirely different composition as well as changes in its function7. One popular method in combating dysbiosis and sustaining diversity within the gut microbiota is through dietary supplementation. Examples of these include vitamins, prebiotics, and probiotics8.
Probiotics are manufactured sources of healthy microbes that benefit the host’s gut9. Probiotics’ main function is to populate the gut microbiota with healthy microbes that neutralize bad microbes and thus support overall gut microbiome diversity10. They are often used in succession to antibiotic treatment. Two common bacterial species in probiotics are the Lactobacillus species and the Bifidobacterium species11. By contrast, prebiotics are non-digestible food substances that stimulate the growth of specific bacteria in the gut microbiome. Prebiotics work in tandem with probiotic treatments to target gut dysbiosis. Common prebiotics include inulin, fructooligosaccharides, and lactulose12.
Recently, scientists have made a connection between the gut microbiome and the brain known as the gut-brain axis where both organs send signals to each other to support the health of the host13. Studies surrounding the gut-brain axis show that there are strong connections between the brain’s cognitive and affective functions and the gastrointestinal tract14. The gut-brain axis plays an important role in maintaining homeostasis, and thus dysbiotic gut health disrupts this homeostasis and has been linked to several mental health disorders like depression15.
Despite the well-known understanding of prebiotics and probiotics’ usage in treating gut dysbiosis , little is known about how prebiotics and probiotics’ effects on the gut can indirectly impact mental health. Depression is a growing urgent public health concern. Severe depression symptoms are often very distressing and can endure long periods often resulting in suicide in severe cases16. Depression is a mental disorder that can affect anyone of all ages and sex. In 2017, depression affected 322 million people worldwide and contributed to 8% of all years lived with a disability17. During 2020, one out of every ten adults were diagnosed with depression and one in every five adolescents and young adults were found with depression18. Depression is also starting to become a relevant issue among the elderly. In 2020, the expected rate of being diagnosed with depression amongst the elderly on a global scale was a staggering 31.74% which could increase to 40.78% in certain countries19.
There are a plethora of other treatments that one can consider that also are used to treat gut dysbiosis. For example, fecal microbiota transplantation (FMT) is often used to diversify microbial communities in the GI tract. Fecal microbiota transplantation involves the transfer of fecal matter from a healthy donor into the gut of a patient in need20. Unfortunately, FMT comes with its downsides being that FMT is not FDA-approved because of questions over its safety21. Additionally, FMT is extremely expensive and typically costs $1770 with some forms upwards to $400022. Probiotics and prebiotics are less invasive solutions as they are found in our everyday food as well as in prescribed treatments.
This research paper aims to identify if and how probiotics and prebiotics could be deployed as methods of depression treatments by analyzing their role in the gut microbiome and their relationship with the brain and overall mental health. A possible hypothesis to the previous prompt would be that probiotics and prebiotics should each be considered as depression treatments because of probiotics and prebiotics ability to cure gut dysbiosis which in turn leads to overall healthier mental health.
Methods
In this review article, numerous resources like peer-reviewed articles and books regarding probiotics and prebiotics, mental health, and gut microbiota diversity were selected and compiled using the search engines Pubmed and Google Scholar. Resources selected for this literature review have been last updated no earlier than 2010 to ensure accuracy. Sources that included the following keywords: ‘mental health”, “depression”, “gut microbiome”, “gut microbiota”, “Depression related dysbiosis”, and “Current forms of Pro and Prebiotic treatment”, amongst others were collected for this review. The main criteria rules for what resources that were chosen were the resource’s date of publishcation, it’s accuracy compared to other resources, and it’s overall clarity and understandability. The information was analyzed to determine whether or not the probiotics and prebiotics can alleviate depression by determining if neurotransmitters related to depression are connected to the function of bacterial microbes in the gut microbiome.
Mental Health
Poor mental health has been a growing public health concern. Mental health disorders are recognized by the Global Burden of Diseases Injuries and Risk Factors (GBD) study as a top 10 leading cause of burden worldwide23. Global number of disability-adjusted life-years (DALYs) is a measurement that combines the number of years an individual lived with that disability and the number of years that were considered lost because of that disability. The global number of DALYs due to mental disorders increased by 56% from 1990 to 201924. This indicates that even on a global scale, mental health is being recognized as a life-long deterrent to an individual.
Mental health disorders can be classified into the following groups: anxiety disorders, bipolar disorders, attention-deficit disorders, and depressive disorders. According to GBD depressive disorders are some of the most prevalent mental health disorders in the world24. There are five main classifications of depressive disorders. These include “Disruptive mood dysregulation disorder”, “Major depressive disorder (MDD)”, “Persistent depressive disorder”, “Premenstrual dysphoric disorder”, and additional depressive disorders resulting from other medical conditions25. Of the five, MDD is the most prevalent as it was the fourth leading cause of disabilities in 202026.
MDD is a pervasive disorder that is expected to be the most common mental health disease by 203027. There has been an increase in depression from 2015 to 2020 for individuals of all ages from 12 to 34 years old. Between 2015 and 2020, 12 to 17-year-olds experienced a 4.2% increase in prevalence of depression. For 18 to 25-year-olds, there was a 6.9% increase and there was a 2.4% increase for 25 to 34-year-olds28. On a global scale, MDD prevalence ranges from 2% in China to 11.5% in Europe. Specifically, France has a 21% lifetime prevalence of MDD26. With an increase in MDD prevalence around the world, society needs new operative treatments for this growing problem.
Major depressive disorder occurs from hyperactivity in the amygdala, striated nucleus, and limbic and subcortical regions in the brain29. For an individual to be diagnosed with Major Depressive Disorder, he/she must be experiencing five of nine MDD symptoms. The 9 symptoms are appetite change, persistently low moods, decreased interest in pleasurable activities, increase in feelings of guilt, lack of energy, sleep disturbances, suicidal thoughts, psychomotor retardation, and poor concentration30. Originally, scientists theorized that the root cause of MDD was an imbalance in different neurotransmitters such as serotonin. Serotonin levels have historically been low in suicidal individuals. MDD is now being linked to more complex neuroregulatory systems rather than a single neurotransmitter30. For instance, GABA is an amino acid that serves as a neurotransmitter that is linked to MDD. However, MDD isn’t linked to specifically only GABA but instead linked to a much larger, neuroregulator system called the Central Nervous System of which GABA is a part. GABA inhibits the activity of mesocortical and mesolimbic systems, contributing to its antidepressant effects. Thus, MDD patients are associated with having low GABA levels in the brain31.
There are two main categories of depression treatment. These include therapy and pharmaceutical treatments32. Cognitive behavioral therapy is a type of time-limited psychotherapy that helps people modify their broken thinking or behavior33. Pharmaceutical treatments, as the name entails, are typically pills, supplements, or prescribed medications.
Understanding to the extent of how much depression has been riddled throuhout all ages of human society puts into context the urgent need to find a permanent yet affordible treatment option for it. Additionally understanding the context of how certain depression disorders like MDD are caused and diagnosed can provide insight into how scientists can treat a specific depression disorder through the gut microbiome.
The Gut Microbiome
The gastrointestinal tract is the most colonized tract in the human body, with the colon containing over 70% of all human microbes34. With a 250 square meter surface area, the GI tract necessitates a diverse and heavily populated microbiota35. The trillions of microbial cells and other microorganisms that colonize the GI tract are known as the gut microbiome1. Bacteria in the gut microbiome perform many different functions including metabolizing nutrients from consumed foods, regulating the body’s immune system, and natural defense against infections36. The gut microbiome is home to over 1000 bacterial species that all have a symbiotic relationship with their host37. Despite having nearly 50 different phyla of bacteria, the gut microbiome is dominated by only two of them: Bacteroidetes and Firmicutes2.
Bacteroidetes’s main cellular components are lipopolysaccharides and flagellin and Bacteroidetes enhance immune reactions through cytokine synthesis38. Bacteroides, a species under the Bacteroidetes phyla, is usually used to metabolize polysaccharides and oligosaccharides, and metabolizing these substances allows for the Bacteroides to extract its nutrients and distribute them to other intestinal microbes throughout the gut microbiome39. Polysaccharides are a huge benefit to the gut microbiota as they serve as nutrient sources for the growth of other bacterial species in the microbiota while also having anti-inflammation and epithelial barrier protection properties that provide the host with overall strong intestinal health40. Mucin glucans, which are proteins produced by epithelial cells and can be found in gastric juices, are important to the fitness and stability of Bacteroides41. Specifically, Mucin-type- O-glycans is a mucin polysaccharide that directly influences Bacteroidetes’ interactions with the host’s GI tract by producing Short-chain fatty acids (SCFA) that provide an energy source for intestinal epithelial cells42. Additionally, B. thetaiotaomicron is used to break down the polysaccharides that the Bacteroides come in contact with. B. thetaiotaomicron can bind to mucins in the GI to regulate the genes that synthesize its outer capsule39. B. thetaiotaomicron can act as host polysaccharides when dietary polysaccharides are lacking. B. fragilis serves a similar function as it synthesizes polysaccharides to maintain optimal colonization in the gut39.
Firmicutes are the most common of the two and play a key role in maintaining homeostasis in the gut microbiome by synthesizing SCFAs and decreasing LDL cholesterol levels. High LDL cholesterol levels are shown to increase the risk of atherosclerosis as well as other conditions like coronary artery disease and peripheral arterial disease43. Having high LDL levels significantly increases the incidence of depressive moods in males44. Firmicutes are able to produce butyrate and SCFAs by breaking down polysaccharides via hydrolysis45. SCFAs are one of the main metabolites produced by the gut microbiota and modulate several metabolic pathways46. Specficaflly, the propionate and butyrate in SCFAs play a crucial role in gastrointestinal health. SCFAs also show vast amounts of biological effects on the host including anti-inflammatory and anti-diabetic properties47. SCFAs help with regulating epigenetic modification in the central nervous system which in turn alleviates and reduces depression syndromes44. Firmicute bacteria can communicate with other tissues and organs that regulate host hunger through their metabolic production of SCFAs38. SCFAs are involved in appetite and hunger by stimulating appetite-regulating hormones like peptide YY48. Firmicutes bacteria are divided into 3 classes: Bacilli, Clostridia, and Eryspielotrichia49.
Bacilli’s major role in the gut microbiome is to metabolize dietary components, xenobiotics, and drugs that maintain intestinal homeostasis. Lactobacillus, and Bacillus, are two of the most distributed Bacilli species in the gut50. Both are great aids to overall host health by preventing intestinal diseases like irritable bowel syndrome and colorectal cancer50. Bacillus can have positive effects on the colon area because of quorum sensing. Quorum sensing is a type of cell-to-cell communication that allows Bacillus bacteria species to exert important regulatory effects on the gut microbiome resulting in positive effects on the colon51. Additionally, a clinical study shows that mice with colorectal colitis have their gut microbiota microbes restored if taking Bacillus subtilis. Beneficial bacteria like Bifidobacterium and Lactobacillus are in higher abundance while negative bacteria like Ruminococcus and Clostridium are reduced50.
Gut Dysbiosis Mechanisms
Dysbiosis refers to a persistent change in the balance of the microbial species and an overall reduction in the diversity of the microorganisms within the gut microbiome. Gut microbiome dysbiosis has been linked to multiple diseases such as inflammatory bowel disease, diabetes, and cancer, and even has a close connection to an individual’s mental health and mood52. A high Bacteroidetes to Firmicutes ratio is highly abundant among Major Depressive Disorder (MDD) patients9. Specifically, there is an increase in the genus Eggerthella lenta and a decrease in the Sutterella, a species of bacteria from the Sutterellaceae family that has been frequently associated with inflammatory bowel disease9.
The gut microbiota and the brain communicate via the gut-brain Axis. This axis is bidirectional, indicating that the axis sends signals both from the gut and to the brain and vice versa53. In addition to connecting the gut microbiome to the brain, the gut-brain axis regulates homeostatic functions like food intake and sleep54. The gut-brain Axis works in close relation to the endocrine system and is composed of a plethora of nerves that transfer signals from the gut to the brain. The gut-brain axis also consists of metabolites derived from the gut microbiome55. Among the many nerves found in the gut-brain axis, the vagus nerve is the most notable. The vagus nerve is a key component of the parasympathetic nervous system and controls digestion in the gut microbiome56.
Another axis that is involved in the connection between gut dysbiosis and depression is the hypothalamic-pituitary-adrenal (HPA) axis. The mechanism behind the HPA axis and how it is linked to host mental health is the increase of pro-inflammatory cytokines connected to host stress. Similar to the gut-brain axis, the HPA axis runs bi-directionally. This means that depression may lead to perturbations in the gut microbiome, and vice versa. Thus this cyclical pathophysiology highlights the necessity for ensuring homeostasis on each end. Hyperactivity in the HPA axis results in an increase in nitrogen and oxygen-producing species that damage bacterial endotoxic lipopolysaccharides which leads to the activation of the inflammatory response system. Activating the inflammatory response system leads to an increase in multiple pro-inflammatory cytokines found in the gut microbiome that is connected to host stress57. For example, when the host experiences stress, the cytokine that is increased is interleukin-6. Interleukin-6 causes host inflammation through increasing permeability of the intestinal epithelial barrier. The increased permeability causes the translocation of pathogenic bacteria to colonic tissue which causes a dysregulated inflammatory response58. Thus the increase of pro-inflammatory cytokines in the HPA axis is related to host mental health problems like stress.
Additionally, inflammatory cytokines activate the enzyme indoleamine 2,3-dioxygenase which is known to decrease serotonin concentration within the brain59. Serotonin is a neurotransmitter produced by the gut microbiota that influences emotional behavior and regulates local gut physiology60. Low serotonin levels are involved in numerous diseases related to the central nervous system including anxiety, schizophrenia, Parkinson’s disease, and even depression61. Thus if there is Gut dysbiosis, it may cause hyperactivity in the HPA axis which leads to the activation of the inflammatory response system. The activation of the inflammatory response system increase pro-inflammatory cytokines which activates indoleamine 2,3-dioxygenase, an enzyme that decreases serotonin levels which have been linked to increasing the risk of depression.

90% of body serotonin is produced in intestinal epithelial cells with multiple microbial metabolites playing a roll in it’s regulation. Bacterial microbes in the gut regulate serotonin production through controlling the enzyme used to create and develop tryptophan, which is the precursor amino acid for serotonin. Clostridia bacteria is usually one type of bacteria that plays this role. Clostridia bacteria produced metabolites that have been identified as signaling molecules to increase the gene expression of tryptophan hydroxylase 1 (TPH1) in colonic cells63.TPH1 is used to catalyze tryptophan into 5-hydroxytryptophan which then goes through decarboxylation to produce serotonin64. Moreover, the decarboxylation can also be done by Staphylococcus, a genus of bacterial microbe found in the gut microbiota. Staphylococcus species that expresses the SadA gene, can perform the decarboxylation from the 5-hydroxytryptophan into serotonin65.

In addition to serotonin, there are molecules outside of neurotransmitters involved in the communication between the gut and the brain including secondary bile acids, Trimethylamine-N-oxide (TMAO), and metabolites that are produced from gut microbes67.
Patients with Major Depressive Disorder often lack high levels of secondary bile acids. High bile acid levels lead to an increase in other taxa of bacteria like Turicibacterales which have been linked to reducing depression-related symptoms68. TMAO is another major microbiota-derived metabolite that may be implicated in the development of neuropsychiatric disorders. Choline, an example of a source of TMAO, enters the brain through CTL1 and CTL2 proteins and increases TMAO levels throughout the mitochondria. From the mitochondria, an increased amount of TMAO levels leads to oxidative stress and neurodegeneration69. The bacteria in charge of the production of trimethylamine (TMA), which is a precursor to TMAO, from choline are typically a part of the Clostridium genus. These bacteria are found in the gut microbiome like Clostridium asparagiformis, C. hathewayi, and C. sporogenes. Additional microbes include Desulfovibrio desulfuricans70.
There has reportedly been a positive association between TMAO levels and depression severity, with an increase in TMAO in the gut microbiome linked to an increased risk of depression68. One big influence on TMAO levels in the gut microbiome is the host’s diet. The dietary intake of certain foods increases or decreases TMAO levels within the gut microbiota. For example, clinical studies indicate that the consumption of fish like cod or salmon leads to an increase in TMAO levels in urine71.
TMAO and other gut metabolites reach the brain by crossing the blood-brain barrier (BBB), unlike neurotransmitters like serotonin. Serotonin and other neurotransmitters are unable to cross the BBB because neurotransmitters like Serotonin are often too big. Only their precursor amino acids are able to penetrate into the brain63. While metabolites reach the brain via the BBB, neurotransmitters reach the brain via the vagus nerve and the enteric nervous system.
The enteric nervous system, often referred to as the “second brain” is a series of connected nerves in the Gastrointestinal tract that further serve as a communication line between the brain and the gut, containing over 600 million neurons. The vagus nerve is one of the key nerves that play a role in facilitating communication between the enteric nervous system and the brain during depression through the transmission of signals produced by the microbes in the gut, to the brain72. Stimulation of the vagus nerve, or vagus nerve stimulation (VNS) is a type of treatment used for depression. VNS, does not directly increase serotonin production, but instead alters the transmission of the neurotransmitter serotonin by increasing basal neurons that produce serotonin within the brainstem and dorsal raphe nucleus73.
Current Forms of Treatment
There are several treatment options available for depression. Treatment for mild stages or early stages of depression can be simply waiting for symptoms to resolve on their own without further treatment74. The three main phases in treatments for more severe depression are the acute, continuation, and maintenance phases74. The acute phase generally lasts for about two months and is the initial stage of depression treatment. The acute phase is when a psychiatrist starts to choose whatever initial treatment they believe would be best for their patient. Treatments during the acute phase include pharmacotherapy and psychotherapy amongst others74. Pharmaceutical medication may also be applied during the acute phase. Ultimately, the selection of the initial treatment is influenced by the severity of the symptoms that the patient is experiencing. The end goal of the acute phase treatment is to find a way to improve patient quality of life and functional capacity74.
During the continuation stage, the treatment that the psychiatrist chooses will be continuously applied by the patients. This phase keeps going until the treatment starts to alleviate more depression symptoms and finally starts to go away as a whole which can typically last up to 9 months. Further pharmaceutical or talk therapy will typically be implemented in patients during this stage if needed. For example, psychotherapy may be needed to prevent relapse of the same symptoms. If psychotherapy then fails, different treatment options like electroconvulsive therapy would be implemented74. Patients who enter the continuation treatment experience milder depressive symptom severity and improvement in other outcomes outside of depressive symptoms75. If patients are stable during the continuation stage, the next phase of treatment may not be necessary75.
In the maintenance phase, the main goal is to limit depressive symptoms that arise within the patient for the long-term future. Typically, the same treatment during the acute and continuation stages will be used during the maintenance phase. Occasionally, more medications may be prescribed during the maintenance phase74. Patients who have a high chance of recurring depression are often prescribed medication periodically throughout their lifetime16.
One popular depression treatment is Cognitive behavior therapy (CBT)16. CBT is a combination of both cognitive therapy and behavioral therapy. Cognitive therapy involves the identification and recognition of harmful beliefs that may be the cause of depression-related symptoms and reforming those beliefs. Cognitive therapy aims to help the patient recognize what activities the patient does and if it does or doesn’t cause depression. Behavioral therapy tries to associate how that said activity directly or indirectly causes depression and how the individual can change or prevent it. For example, individuals diagnosed with depression often give up their hobbies and thus feel isolated and unhappy. Cognitive therapy would help individuals recognize the fact that giving up hobbies is the activity that leads to depression. Behavioral therapy would be understanding that isolation and unhappiness are the behavioral underlying feelings of depression and the solution would be to engage in social activities and hobbies76.
CBT is a beneficial method for helping depression because it allows the patient to understand the root cause and make adjustments. However, CBT, compared to other psychological depression treatment options like psychoanalysis, isn’t as analytical. Thus, CBT may not be the best option for those who are looking to have a deeper understanding of the specific cause of their depression. CBT also requires a personalized therapist whom one must form a close relationship with which may be time-consuming and financially unsustainable long term77.
Aside from psychological treatment and talk therapy, pharmaceutical treatment is also another solution that physicists can prescribe to patients. Antidepressant pills are growing to be one of the most popular forms of pharmaceutical treatment, as prescriptions have more than tripled in usage from 1998 to 201878.
There are seven main classes of antidepressants and some of them like SSRI, SNRI, and tricylic antidepressants prevent the reuptake of monoamines into presynaptic neurons so that they remain in the synaptic cleft79. Monoamines are essentially a type of neurotransmitters like serotonin and dopamine that play a role in various cognitive processes like emotions and memory80. Preventing the reputaking of monoamines does not necessarily increase the total number of monoamines but instead redistributes monoamines throughout the brain81. This allows the monoamines to improve the communication between nerve cells as it increases the amount of signaling sent to different brain neurons throughout the brain81. The improvement in cell communication presumably correlated to helping the imbalances in brain function that contribute to depression. On the opposite end of the spectrum, the redistribution of monoamines will also possibly set up conditions that favor the depletion of monoamines if proper levels of nutrients are not administered81.
MAOIs are an antidepressant that is unique because instead of inhibiting the reuptake of monoamines, they inhibit the breakdown of monoamines. Preservation of monoamines presumably improves the efficiency of synaptic neurotransmission which may correct for neurophysiological deficits that underlie depression78. While antidepressants are effective treatments for patients with depressive disorders, antidepressants do come with a plethora of negative side effects. For example, common side effects when taking SSRIs include anxiety, insomnia, and sexual difficulties among other symptoms82. In rare cases, patients who take SSRIs have experienced extremely dangerous and near-fatal cutaneous reactions like Stevens-Johnson syndrome, erythema multiforme, and toxic epidermal necrolysis83.
Probiotics and Prebiotics: An Overview
One of the functions of probiotics is to benefit host health by diversifying the gut microbiome due to containing non-pathogenic microbes such as bacteria which once released colonize and give diversity in the gut. Probiotics can aid in the prevention of multiple diseases including Crohn’s disease, cardiovascular and urogenital infections, cancer, and oral diseases11. The majority of probiotics include two genera: Lactobacillus and Bifidobacterium68.
L. salivarius in the adult diet enhances immune response by activating natural killer cells, monocytes, immunoglobulins, and IL-10 cytokines in the plasma. L.casei Shirota increases the expression of the CD96 activator marker T cells and killer cells which also further helps the host ward off pathogens. L. casei Shirota also improves the concentration of important cytokine receptors like IFN-γ84. IFN-γ enhances antigen recognition by cognate T-cell interactions and induces anti-viral responses. IFN-γ activity is able to destroy cancer cells and contribute to necessary effector cell activation and the creation of antibodies that are used to mediate bacterial infections like Chlamydia85.
The two main sources of probiotics are food and pharmaceutical supplements. Fermented foods in particular are rich in beneficial microbes86. Yogurt is a common fermented food that contains probiotic microorganisms like L. bulgaricus and Streptococcus thermophilus87. Some foods on the market are commercially engineered such that beneficial microbes are added in. However, these microorganisms typically do not reach the distal gut88. This is because they do not survive transit in the stomach and are unable to resist degradation in the small intestine by hydrolytic enzymes and bile salts88. However, naturally occurring probiotic strains that are typically found in yogurt do survive intestinal transit and can effectively reach the distal gut88.
Supplement forms of probiotics often have a wider variety of live microorganisms compared to the single strains found in the food versions88. Probiotic supplementation has been linked to better host health by improving bacteria concentration within the gut microbiome89. Supplemental probiotics improve stool consistency, bowel movement, and lipid blood profile89. A lipid profile measures the total concentration of cholesterol in the blood. This included both high-density lipoproteins (HDL) and low-density lipoproteins (LDL)90. LDL is much more detrimental to mental health compared to HDL. Borderline and high levels of LDL were significantly associated with depressive mood and behavior91. On the other hand, studies have shown that HDL levels are positively associated with mental health and overall cognitive function92. Thus, an improvement in lipid blood profile or higher concentration of HDL cholesterol and lower concentrations of LDL may be linked to better mental health outcomes.
Prebiotics also help mediate gut microbiota dysbiosis. The prebiotic concept was initially introduced in 1995 by Glenn Gibson and Marcel Roberfield93. Compared to probiotics, prebiotics’ main function is not to release microbial strains in the gut microbiota but to instead enhance the growth of these beneficial microbes and bacteria in the GI tract94. Prebiotics also help to improve activity against certain pathogens within the GI tract like Salmonella and Escherichia coli95.
To be considered a prebiotic, the following characteristics must be covered: resistance to acidic pH levels in the stomach, cannot be hydrolyzed by mammalian enzymes and cannot be absorbed within the GI tract, must be able to be fermented by the intestinal microbiota, and finally, growth of prebiotics must improve host health96. However, the World Health Organization defines prebiotics more broadly by calling prebiotics non-viable food substances that benefit host health through the modulation of the microbiota. The prebiotics that seem to universally fulfill all prebiotic requirements are bifidogenic oligosaccharides like inulin and galacto-oligosaccharides97.
Most oligosaccharides are non-digestible carbohydrates that are between monosaccharides and polysaccharides. Oligosaccharides typically are made up of less than a dozen monosaccharides while polysaccharides are composed of more than a dozen monosaccharides98. Oligosaccharides can be naturally sourced from foods like asparagus, garlic, chicory, onion, or banana99. Oligosaccharide’s ability to resist the acidic pH levels in the stomach, as well as being unable to be broken by mammalian enzymes allows it to successfully reach the distal gut. Thus, the bacteria in the gut microbiota can ferment and utilize oligosaccharides often and produce SCFAs100. A higher abundance of SCFAs in the gut microbiota improves the host’s in many ways including reducing host inflammatory responses and reducing the host’s blood pressure48.
Inulin promotes host health by regulating lipid metabolism, weight loss, and lower inflammatory symptoms, amongst other qualities101. Inulin is also the reason for prebiotics indigestible characteristics. The β-(2-1)-d- fructose bonds that are generated between the fructose units of inulin and the β-configuration of anomeric carbon make prebiotics indigestible in the small intestine. Prebiotics are instead fermented in the large intestine of the microflora through the production of several metabolites. For instance, SCFAs are produced which are essential for balancing redox reactions in the gut-microbiota102.
Similar to probiotics, prebiotics can be found in natural food sources. Fructooligosaccharide (FOS) is a prebiotic that is naturally occurring in many food products like garlic, onion, bananas, and leeks94. FOS fermentation positively impacts the host in many ways. For example, FOS fermentation leads to stronger bone health by potentially preventing the onset of osteoporosis. Fermentation of FOS releases SCFAs which in turn lower the pH levels in the lumen of the stomach. The drop in pH allows calcium phosphate ions to dissolve which promotes passive diffusion of calcium from the stomach to the bones103. An adequate intake of calcium is needed to promote general bone health104.
Fructosyltransferase is an essential enzyme that FOS from sucrose. Aspergillus niger and Auerobasidium pullans are two microorganisms that use sucrose as their main source of carbon that have demonstrated that they can produce FOS on an industrial scale95. Auerbasidium pullans have been abundant in fresh grapes and Aspergillus niger is abundantly found in numerous fruits and vegetables like onions or mangoes105.
Both treatments can be used at any time during the day, but probiotics are recommended to be used after meals. Neutralization of gastric acid after food enters the stomach makes it more conducive for probiotics to exhibit their effect106. Like any treatment, an overdose of probiotic treatment does not always equate to healthier host health. Overloading probiotics can lead to negative side effects like abdominal cramping, nausea, flatulence, and taste disturbance107.
While still new, prebiotics and probiotics as possible treatments for depression has already been looked into and have shown positive signs of becoming a necessary intervention for depression related to gut dysbiosis. Indeed, a 2019 clincal study showed that patients who received probitiocs and/or prebiotics have significantly improved symptoms of depression compared to those in a placebo group108.Regardless, more clinical trials and further research needs to be conducted in order for probiotics and prebiotics to be approved depressive treatment options.
Probiotic Intervention
The most common microbes that probiotics contain are a part of the Actinobacteria and the Firmicutes phylum of bacteria. This includes bacterial species from the Bifidobacterium and Lactobacillus genus102. Both Bifidobacteria and Lactobacilli are regarded as the main screening makers of intestinal health and screening markers for the identification of prebiotics within the GI tract109. Bifidobacterium is important in decreasing the growth of pathogenic bacteria and protecting against intestinal barrier dysfunction110. Bifidobacterium decreases the chances of inflammatory bowel species, aids digestion, increases resistance to infection while lessening constipation, and can reduce diarrhea102.
In metabolism, Bifidobacterium is used for the catabolism of monosaccharides. The catabolism of monosaccharides and other carbohydrates can be used to produce cell ATP through the 6-phosphate pathway, otherwise known as the bifid shunt111. The bifid shunt is run by the fructose 6-phosphate phosphoketolase (Xfp) enzyme. The Xfp enzyme has a dual substrate specificity with fructose 6-phosphate and xylulose 5-phosphate112.
Lactobacillus can provide intestinal barrier defense by enhancing mucous secretion. L. casei T21 regulates the MUC2 gene113. The MUC2 is a gel-forming mucin that provides a protective gel barrier for the colon114. In the absence of MUC2, bacteria can easily penetrate the crypts and can access the epithelial cell barrier of the stomach which leads to severe host inflammation115.
L. fermentum, L. corynifromis, and L. gasseri are able to reduce reactive oxygen species (ROS) concentrations within the gut microbiome116. This is important because if ROS levels are too high, it leads to metabolic problems, cancer, and other neurological conditions117. These species of Lactobacillus are able to decrease NADPH oxidase (NOX) –an enzyme that produces ROS –which ultimately lowers the enzymatic reactions and chemical processes that generate ROS in the first place118.
Through probiotics production of different Lactobacillus and Bifidobacterium genus in the gut microbiome, there has been reason to believe that probiotics can also play a role in alleviating depression as well. There are over 178 different species and subspecies of probiotics that can reduce the chance of depression, most of which fall under the Lactobacillus and Bifidobacterium genus. For example, L. helveticus, L. rhamnous, B. longum, and B. creve CCFM1025 are four species that have clinically been successful in the treatment of depression9. B. longum demonstrates anti-depressive effects through their fixation of diseases related to the gut microbiota dysbiosis. A clinical trial has shown that B. longum treatments used in individuals with irritable bowel syndrome also improve depression-related symptoms by lessening the limbic reactivity to negative emotional stimuli119.
An example of probiotics found in natural foods is L. plantarum, which is commonly found in traditional sourdough bread120. L. plantarum is a natural probiotic that could potentially improve systemic inflammation and help alleviate insulin resistance mediated by the gut microbiota121. Reducing insulin resistance can decrease the possible development of MDD122. Insulin resistance is the impaired biological response of target tissues to insulin stimulation123. Insulin regulates glucose metabolism. Insulin causes glucose to be deposited in the liver as glycogen, then releases the glycogen from the liver and into the rest of the body like the brain in the form of glucose124. If insulin resistance occurs, glucose is unable to reach other organs like the human brain, where a lack of glucose is correlated to individuals who are depressed122.
One way probiotics can potentially increase gut microbiome diversity is by vitamin production. Taking probiotic supplements that include the Bifidobacterium or Lactobacillus genus can produce vitamins B and K125. Vitamin B reduces gut microbiota dysbiosis by increasing multiple bacterial genus that are not limited to specific Lacotbacillus or Bifdiobacterium88. For example, taking biotin, or vitamin B7, increases the concentration of Ruminoccus gauvreauii and Coprococcus 3 bacteria126. The Coprococcus bacteria is typically associated with a higher quality of life. Individuals with depression often lack Coprococcus levels within the gut microbiota and reduced amount of Ruminoccus have been found in individuals with bipolar depression126.
Prebiotic Intervention
Prebiotics are a group of nutrients that can be degraded by the gut microbiota96. Prebiotics’s main characteristics are that they are nondigestible and also beneficially stimulate the growth and activity of gut bacteria. In modern society, prebiotics have developed a more broad characterization as they are simply being referred to as dietary components that can be used by the host’s microorganisms to improve health12. Thus, one may assume that prebiotics have a rather indirect impact compared to their probiotic counterpart.
For example, galactooligosaccharides are a form of prebiotic that is commonly used to promote the proliferation of Bifobdacterium, which again is one of the two major genera of bacteria that probiotics contain. In healthy infants, Bifidobacterium abundance was much higher when fed a baby formula containing galacto-oligosaccharides110. Additionally, Inulin-type fructans can serve as prebiotics that stimulate the metabolism of Bifidobacterium and Lactobacillus in the colon and GI tract110. It is imperative that prebiotics can help supplement the growth of these probiotic bacterial strains because the proper growth and reproduction probiotics would be most effective if prebiotics are also present110.
In addition to increasing healthy probiotic bacterial strains, prebiotics themselves can eliminate negative bacteria found in the gut flora by affecting the other genus that probiotics typically contain–the Lactobacillus species. Prebiotics can eliminate the production of the gram-negative bacteria Klebsiella pneumoniae127. All of this happens because adding prebiotics like inulin, lactulose, and fructooligosaccharides to the Lactobacillus species lowers the pH levels of the cell-free supernatant which increase the inhibitory percentage of Lactobacillus strains that produce Klebsiella pneumoniae127. Klebsiella pneumoniae is a negative gram bacteria that is the leading cause of healthcare-associated infections like pneumonia and urinary tract infections. A study has shown that a preexisting history of depression often increases the likelihood of a Klebsiella infection128. While there isn’t solid evidence to propose that the opposite is true, the fact that depression and Klebsiella pneumoniae are positively correlated indicates that Klebsiella pneumoniae is worthwhile to look into as a possible treatment option for depression.
In addition to Klebsiella pneumoniae, a the prebiotic Glycomacropeptide (GMP) is able to reduce levels of Desulfovibrio bacterial speciesin the gut microbiome. GMP is able to do this by the production of SCFAs. GMP is able to produce SCFAs in the cecal area which disrupts the environment needed to produce Desulfovibrio by lowering intestinal pH levels129. Additionally, some propose that GMP reduces Desulfovibrio by altering the mucin synthesis. Desulfovibrio is typically found in the mucus gel layer of the colon130. This is likely because Desulfovibrio main job is to metabolize sulufate mucopolysacchrides that are found in the mucin. If, if GMP lower mucin production, it would also wipe out Desulfovibrio concentration. However, there has been little to no concrete studies of GMP affecting mucin production129.
Fructooligosaccharide (FOS) is a prebiotic that is naturally occurring in many food products like garlic, onion, bananas, and leeks94. FOS has been observed to alleviate depression-like behaviors by lowering corticosterone levels in the plasma and urine of rats131. Corticosterone in rats is similar to cortisol in humans. Studies have shown that high levels of cortisol in humans are associated with increases in the severity of MDD like psychotic and melancholic MDD132. Additionally, the rats receiving the FOS exhibited a higher diversity of beneficial bacteria like Acinetobacter, Barnesiella, and Dialister within the gut microbiota131. This indicates that the ability of FOS to improve gut dysbiosis may in turn reduce depression-like symptoms.
Fructooligosaccharides are an example of prebiotics found in food. On the opposite end would pharmaceutical prebiotic treatment, and although not exactly a pharmaceutical supplements, a new form of prebiotics is being discovered in the form of herbal medicine. Herbal medicine is considered a form of prebiotics because of their ability to modulate the gut microbiota and improve colonic epithelium function133. Herbal medicine as a whole like Triphala, which is a specific herb itself, or Ayurveda, which is a type of medical system that involves herbal medicine have been well documented to have benefits on gastrointestinal health. Herbal medicines are able to increase the abundance of bacterial species that are a part of both the Bifidobacterium and Lactobacillus genera. Additionally, another prebiotic trait that herbal medicine has is the ability to decrease the concentration of pathogenic bacterial species. The negative bacterial species that herbal medicine decreases are Citrobacter freundii and Klebsiella pneumoniae, both of which are linked to Leaky Gut syndrome133.
Discussion
Depression is an extremely well-known mental health disorder that has affected numerous individuals on a global scale. There are many treatments that scientists have concocted for depression. However, treatments for depression are currently targeted to the brain itself by working on neural networks. There is limited research tackling the efficacy of treating depression by targeting the gut brain connection. There are strong connections between gut dysbiosis and depression through multiple pathways that connect the gut to the brain like the HPA and the gut-brain axis. The gut in these bidirectional pathways produces many neurotransmitters that have a close affiliation with the brain and its numerous mental health disorders. Specifically, the bacterial microbes within the gut are responsible for the creation of these neurotransmitters, most notably the creation of serotonin amongst other substances. However, if gut dysbiosis occurs, this reduces the abundance of bacterial microbes which results in limited production of the neurotransmitters in this gut-brain communication.Hence, medications that specifically modulate gut dysbiosis may have the potential to double as a treatment for depression.
Prebiotics and probiotics sustain bacterial microbes that are involved in the creation of key neurotransmitters that connect the gut microbiota and depression. One such neurotransmitter is serotonin. Serotonin is a neurotransmitter linked to alleviating depression. Nearly all serotonin products in the body come from the gut microbiota. The Clostridia genusis one of the bacterial microbe that is used to promote serotonin. On the other hand, most probiotics are generally limited to containing strains of Lactobacillus and Bifidobacterium genera, not Clostridia. Considering this, one limitation of traditional food probiotics as possible treatments for depression may arise. To counteract the lack of Clostridium genus is conventional probiotoic, the idea of modifying these probiotics to contain more clostridia genus to produce more serotonin should be further researched and developed.
However, there is another form of probiotic treatment other than just food. Probiotic supplements, through the producint of different vitaminss can offer a wider variety of live microorganisms. For instance, vitamin B, a vitamin that certain genuses of bacteria found in probiotics can produce, can support the growth of Coprococcus 3 bacteria which is part of the Coprococcus genus. Thus, probiotic supplements are not limited to the Lactobacillus and Bifidobacterium genera. Therefore, they do have the potential to promote the growth of Clostridia bacteria which in turn can promote serotonin production and help to mitigate depression related symptoms.
In a similar fashion, prebiotics can also be used to alleviate depression through their interactions with metabolites produced by the gut microbiome that play a role in the HPA axis. One role that prebiotics have is the ability to reduce the negative, pathogenic bacterial microbes in the gut microbiome. When gut dysbiosis occurs, there is a shift towards higher abundance of pathogenic microbes. These pathogenic bacterial microbes convert choline derived from the diet to TMA which is further oxidized into TMAO. TMAO is a metabolite produced in the gut microbiome that serves as a form of communication between the gut and the brain by crossing the blood brain barrier. It is worth noting that high TMAO levels are often found in individuals suffering from depression. One of the pathogenic bacterial microbes that uses choline is Desulfovibrio desulfuricans. The prebiotic Glycomacropeptide is able to reduce Desulfovibrio bacterial microbes by lowering intestinal pH levels. Therefore, in theory, glycomacropeptide reducing Desulfovibrio desulfuricans would decrease the amount of total bacterial microbes available to covert choline into TMAO. Hence, the use of prebiotics and probiotics can allow for the restoration of homeostasis in the gut microbiome. This will result in the reduction of pathogenic microbes that produce molecules such as TMAO that have negative impacts on brain health. Therefore, reducing depression related symptoms.
Probiotics and prebiotics are individual supplements often taken separately. Synbiotics aren’t as well studied compared to probiotics and prebiotics and little is known about the differences between them. Synbiotics is another type of nutritional supplement and is the synergistic combination of both probiotics and prebiotics. An exploration of symbiotics would be beneficial in that it would provide insight into whether or not its use would provide the same benefits for treatment of depression as taking prebiotics and probiotics in their individual form.
Another topic that can be further explored is the use of natural vs manufactured probiotics and prebiotics found in food. Typically, natural probiotics are found in fermented foods like kimchi, which is Korean fermented cabbage. However, probiotics can also be added into food. This is typically done by food manufacturers to produce large amounts of food products at once for commercial use. These probiotics have been proposed to not have the same effects on host health, as they are typically only used to keep these food items fresh. Therefore, future research should explore the differential impact of prebiotics and probiotics derived from natural sources vs those that are commercially produced.
Regardless, a limitation in this study is simply the fact that the entire field of nutrional psychiatry, that is the field that connects nutrition to mental health and brain health has been a rather new field. There is still moer information left to be revealed about to how both the overall gut organ and the gut microbiome are related to brain health and mental health. Thus prebiotic and probiotic and their relationship to mental health can only be studied so much before the relationship between the gut and its microbiome is solidified and more scientifically researched.
However, because of probiotics and prebiotic’s popularity in the world of gut health and gut dyboisis, future research and field advancements regarding nutroinal psychiatry is on the upswing and is bound to happen to hopefully provide proper mental health and gut health for all.
Conclusion
Probiotics and prebiotics are two forms of treatment for dysbiosis of the gut microbiome through their ability to repopulate and sustain the growth of bacterial microbes in the gut microbiome. Through diversifying the gut, it has a possible inadvertent effect in also treating depression and boosting brain health. This review article aimed to answer if this possible inadvertent effect should be further looked into as a necessary intervention for depression related to gut dysbiosis. Through the analysis of the sources gathered for this review article, probiotics and prebiotics should be further discussed as possible treatment options for depression because of their work in the gut microbiome. Probiotics and prebiotics have the ability to support the growth of healthy bacteria that produce molecules connected to depression. They also possess the ability to reduce pathogenic bacteria that produce molecules that may increase risk of depression. Thus, both of these supplements may be possible interventions for depression that may be connected to gut microbiota dysbiosis. Though the evidence for the use of prebiotics and probiotics as treatments for depression may be encouraging, further studies need to be conducted to fully confirm their therapeutic potential.
References
- Jandhyala SM, Talukdar R, Subramanyam C, Vuyyuru H, Sasikala M, Nageshwar Reddy D. Role of the normal gut microbiota. World J Gastroenterol. 2015 Aug 7;21(29):8787-803. doi:10.3748/wjg.v21.i29.8787. PMID: 26269668; PMCID: PMC4528021 [↩] [↩]
- Bull MJ, Plummer NT. Part 1: The Human Gut Microbiome in Health and Disease. Integr Med (Encinitas). 2014 Dec;13(6):17-22. PMID: 26770121; PMCID: PMC4566439. [↩] [↩]
- Gilbert JA, Blaser MJ, Caporaso JG, Jansson JK, Lynch SV, Knight R. Current understanding of the human microbiome. Nat Med. 2018 Apr 10;24(4):392-400. doi: 10.1038/nm.4517. PMID: 29634682; PMCID: PMC7043356. [↩]
- Rinninella E, Raoul P, Cintoni M, Franceschi F, Miggiano GAD, Gasbarrini A, Mele MC. What is the Healthy Gut Microbiota Composition? A Changing Ecosystem across Age, Environment, Diet, and Diseases. Microorganisms. 2019 Jan 10;7(1):14. doi: 10.3390/microorganisms7010014. PMID: 30634578; PMCID: PMC6351938. [↩]
- Heiman ML, Greenway FL. A healthy gastrointestinal microbiome is dependent on dietary diversity. Mol Metab. 2016 Mar 5;5(5):317-320. doi: 10.1016/j.molmet.2016.02.005. PMID: 27110483; PMCID: PMC4837298.; Linhares Y, Kaganski A, Agyare C, Kurnaz IA, Neergheen V, Kolodziejczyk B, Kędra M, Wahajuddin M, El-Youssf L, Dela Cruz TE, Baran Y, Pešić M, Shrestha U, Bakiu R, Allard PM, Rybtsov S, Pieri M, Siciliano V, Flores Bueso Y. Biodiversity: the overlooked source of human health. Trends Mol Med. 2023 Mar;29(3):173-187. doi: 10.1016/j.molmed.2022.12.002. Epub 2022 Dec 28. PMID: 36585352. [↩]
- Deng F, Li Y, Zhao J. The gut microbiome of healthy long-living people. Aging (Albany NY). 2019 Jan 15;11(2):289-290. doi: 10.18632/aging.101771. PMID: 30648974; PMCID: PMC6366966. [↩]
- Sprockett, D. D., & Coyte, K. Z. (2023). When microbes go missing: Understanding the impact of diversity loss within the gut microbiome. Cell Host & Microbe, 31(8), 1249–1251. https://doi.org/10.1016/j.chom.2023.07.006 [↩]
- Dale HF, Lied GA. Gut microbiota and therapeutic approaches for dysbiosis in irritable bowel syndrome: recent developments and future perspectives. Turk J Med Sci. 2020 Nov 3;50(SI-2):1632-1641. doi: 10.3906/sag-2002-57. PMID: 32222124; PMCID: PMC7672353. [↩]
- Liu, L., Wang, H., Chen, X., Zhang, Y., Zhang, H., & Xie, P. (2023). Gut microbiota and its metabolites in depression: From pathogenesis to treatment. eBioMedicine, 90. https://doi.org/10.1016/j.ebiom.2023.104527 [↩] [↩] [↩] [↩]
- Amara AA, Shibl A. Role of Probiotics in health improvement, infection control and disease treatment and management. Saudi Pharm J. 2015 Apr;23(2):107-14. doi: 10.1016/j.jsps.2013.07.001. Epub 2013 Jul 18. PMID: 25972729; PMCID: PMC4421088. [↩]
- Bodke H, Jogdand S. Role of Probiotics in Human Health. Cureus. 2022 Nov 9;14(11):e31313. doi: 10.7759/cureus.31313. PMID: 36514580; PMCID: PMC9733784. [↩] [↩]
- Ji J, Jin W, Liu SJ, Jiao Z, Li X. Probiotics, prebiotics, and postbiotics in health and disease. MedComm (2020). 2023 Nov 4;4(6):e420. doi: 10.1002/mco2.420. PMID: 37929014; PMCID: PMC10625129. [↩] [↩]
- Cryan JF, O’Riordan KJ, Cowan CSM, Sandhu KV, Bastiaanssen TFS, Boehme M, Codagnone MG, Cussotto S, Fulling C, Golubeva AV, Guzzetta KE, Jaggar M, Long-Smith CM, Lyte JM, Martin JA, Molinero-Perez A, Moloney G, Morelli E, Morillas E, O’Connor R, Cruz-Pereira JS, Peterson VL, Rea K, Ritz NL, Sherwin E, Spichak S, Teichman EM, van de Wouw M, Ventura-Silva AP, Wallace-Fitzsimons SE, Hyland N, Clarke G, Dinan TG. The Microbiota-Gut-Brain Axis. Physiol Rev. 2019 Oct 1;99(4):1877-2013. doi: 10.1152/physrev.00018.2018. PMID: 31460832. [↩]
- Faraj J, Takanti V, Tavakoli HR. The Gut-Brain Axis: Literature Overview and Psychiatric Applications. Fed Pract. 2021 Aug;38(8):356-362. doi: 10.12788/fp.0159. PMID: 34733087; PMCID: PMC8560095. [↩]
- Mayer, E. A., Nance, K., & Chen, S. (2022). The gut–brain axis. Annual Review of Medicine, 73(Volume 73, 2022), 439–453. https://doi.org/10.1146/annurev-med-042320-014032; Xiong RG, Li J, Cheng J, Zhou DD, Wu SX, Huang SY, Saimaiti A, Yang ZJ, Gan RY, Li HB. The Role of Gut Microbiota in Anxiety, Depression, and Other Mental Disorders as Well as the Protective Effects of Dietary Components. Nutrients. 2023 Jul 23;15(14):3258. doi: 10.3390/nu15143258. PMID: 37513676; PMCID: PMC10384867. [↩]
- InformedHealth.org [Internet]. Cologne, Germany: Institute for Quality and Efficiency in Health Care (IQWiG); 2006-. Depression: Learn More – Treatments for depression. [Updated 2020 Jun 18]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK279282/ [↩] [↩] [↩]
- Moreno-Agostino, D., Wu, Y.-T., Daskalopoulou, C., Hasan, T., Huisman, M., & Prina, M. (2021). Global trends in the prevalence and incidence of depression:a Systematic review and meta-analysis. Journal of Affective Disorders, 281, 235–243. https://doi.org/10.1016/j.jad.2020.12.035 [↩]
- Goodwin RD, Dierker LC, Wu M, Galea S, Hoven CW, Weinberger AH. Trends in U.S. Depression Prevalence From 2015 to 2020: The Widening Treatment Gap. Am J Prev Med. 2022 Nov;63(5):726-733. doi: 10.1016/j.amepre.2022.05.014. Epub 2022 Sep 19. PMID: 36272761; PMCID: PMC9483000. [↩]
- Zenebe Y, Akele B, W/Selassie M, Necho M. Prevalence and determinants of depression among old age: a systematic review and meta-analysis. Ann Gen Psychiatry. 2021 Dec 18;20(1):55. doi: 10.1186/s12991-021-00375-x. PMID: 34922595; PMCID: PMC8684627. [↩]
- Kim KO, Gluck M. Fecal Microbiota Transplantation: An Update on Clinical Practice. Clin Endosc. 2019 Mar;52(2):137-143. doi: 10.5946/ce.2019.009. Epub 2019 Mar 26. PMID: 30909689; PMCID: PMC6453848. [↩]
- Merrick B, Allen L, Masirah M Zain N, Forbes B, Shawcross DL, Goldenberg SD. Regulation, risk and safety of Faecal Microbiota Transplant. Infect Prev Pract. 2020 Sep;2(3):100069. doi: 10.1016/j.infpip.2020.100069. Epub 2020 Jun 9. PMID: 34316559; PMCID: PMC7280140. [↩]
- Arbel LT, Hsu E, McNally K. Cost-Effectiveness of Fecal Microbiota Transplantation in the Treatment of Recurrent Clostridium Difficile Infection: A Literature Review. Cureus. 2017 Aug 23;9(8):e1599. doi: 10.7759/cureus.1599. PMID: 29067223; PMCID: PMC5652885. [↩]
- Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. (2022). The Lancet Psychiatry, 9(2), 137–150. https://doi.org/10.1016/S2215-0366(21)00395-3 [↩]
- Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. (2022). The Lancet Psychiatry, 9(2), 137–150. https://doi.org/10.1016/S2215-0366(21)00395-3 [↩] [↩]
- Chand SP, Arif H. Depression. [Updated 2023 Jul 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430847/ [↩]
- Gutiérrez-Rojas L, Porras-Segovia A, Dunne H, Andrade-González N, Cervilla JA. Prevalence and correlates of major depressive disorder: a systematic review. Braz J Psychiatry. 2020 Nov-Dec;42(6):657-672. doi: 10.1590/1516-4446-2020-0650. PMID: 32756809; PMCID: PMC7678895. [↩] [↩]
- Malhi GS, Mann JJ. Depression. Lancet. 2018 Nov 24;392(10161):2299-2312. doi: 10.1016/S0140-6736(18)31948-2. Epub 2018 Nov 2. PMID: 30396512. [↩]
- RD, Dierker LC, Wu M, Galea S, Hoven CW, Weinberger AH. Trends in U.S. Depression Prevalence From 2015 to 2020: The Widening Treatment Gap. Am J Prev Med. 2022 Nov;63(5):726-733. doi: 10.1016/j.amepre.2022.05.014. Epub 2022 Sep 19. PMID: 36272761; PMCID: PMC9483000. [↩]
- Trifu SC, Trifu AC, Aluaş E, Tătaru MA, Costea RV. Brain changes in depression. Rom J Morphol Embryol. 2020 Apr-Jun;61(2):361-370. doi: 10.47162/RJME.61.2.06. PMID: 33544788; PMCID: PMC7864313. [↩]
- Bains N, Abdijadid S. Major Depressive Disorder. [Updated 2023 Apr 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559078 [↩] [↩]
- Allen MJ, Sabir S, Sharma S. GABA Receptor. [Updated 2023 Feb 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526124/ [↩]
- InformedHealth.org [Internet]. Cologne, Germany: Institute for Quality and Efficiency in Health Care (IQWiG); 2006-. Depression: Learn More – Treatments for depression. [Updated 2020 Jun 18]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK279282/ [↩]
- Melton L. Brief Introduction to Cognitive Behavioral Therapy for the Advanced Practitioner in Oncology. J Adv Pract Oncol. 2017 Mar;8(2):188-193. doi: 10.6004/jadpro.2017.8.2.6. Epub 2017 Mar 1. PMID: 29900026; PMCID: PMC5995489. [↩]
- Saus E, Iraola-Guzmán S, Willis JR, Brunet-Vega A, Gabaldón T. Microbiome and colorectal cancer: Roles in carcinogenesis and clinical potential. Mol Aspects Med. 2019 Oct;69:93-106. doi: 10.1016/j.mam.2019.05.001. Epub 2019 May 24. PMID: 31082399; PMCID: PMC6856719. [↩]
- Thursby E, Juge N. Introduction to the human gut microbiota. Biochem J. 2017 May 16;474(11):1823-1836. doi: 10.1042/BCJ20160510. PMID: 28512250; PMCID: PMC5433529. [↩]
- Al Bander Z, Nitert MD, Mousa A, Naderpoor N. The Gut Microbiota and Inflammation: An Overview. Int J Environ Res Public Health. 2020 Oct 19;17(20):7618. doi: 10.3390/ijerph17207618. PMID: 33086688; PMCID: PMC7589951. [↩]
- Fujisaka S, Watanabe Y, Tobe K. The gut microbiome: a core regulator of metabolism. J Endocrinol. 2023 Jan 19;256(3):e220111. doi: 10.1530/JOE-22-0111. PMID: 36458804; PMCID: PMC9874984. [↩]
- Stojanov S, Berlec A, Štrukelj B. The Influence of Probiotics on the Firmicutes/Bacteroidetes Ratio in the Treatment of Obesity and Inflammatory Bowel disease. Microorganisms. 2020 Nov 1;8(11):1715. doi: 10.3390/microorganisms8111715. PMID: 33139627; PMCID: PMC7692443. [↩] [↩]
- Zafar H, Saier MH Jr. Gut Bacteroides species in health and disease. Gut Microbes. 2021 Jan-Dec;13(1):1-20. doi: 10.1080/19490976.2020.1848158. PMID: 33535896; PMCID: PMC7872030. [↩] [↩] [↩]
- Gan L, Wang J, Guo Y. Polysaccharides influence human health via microbiota-dependent and -independent pathways. Front Nutr. 2022 Nov 9;9:1030063. doi: 10.3389/fnut.2022.1030063. PMID: 36438731; PMCID: PMC9682087. [↩]
- Kang Y, Park H, Choe BH, Kang B. The Role and Function of Mucins and Its Relationship to Inflammatory Bowel Disease. Front Med (Lausanne). 2022 May 6;9:848344. doi: 10.3389/fmed.2022.848344. PMID: 35602503; PMCID: PMC9120656. [↩]
- Zhang Y, Wang L, Ocansey DKW, Wang B, Wang L, Xu Z. Mucin-Type O-Glycans: Barrier, Microbiota, and Immune Anchors in Inflammatory Bowel Disease. J Inflamm Res. 2021 Nov 13;14:5939-5953. doi: 10.2147/JIR.S327609. PMID: 34803391; PMCID: PMC8598207. [↩]
- Huff T, Boyd B, Jialal I. Physiology, Cholesterol. [Updated 2023 Mar 6]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470561/ [↩]
- Cheng J, Hu H, Ju Y, Liu J, Wang M, Liu B, Zhang Y. Gut microbiota-derived short-chain fatty acids and depression: deep insight into biological mechanisms and potential applications. Gen Psychiatr. 2024 Feb 19;37(1):e101374. doi: 10.1136/gpsych-2023-101374. PMID: 38390241; PMCID: PMC10882305. [↩] [↩]
- Fusco W, Lorenzo MB, Cintoni M, Porcari S, Rinninella E, Kaitsas F, Lener E, Mele MC, Gasbarrini A, Collado MC, Cammarota G, Ianiro G. Short-Chain Fatty-Acid-Producing Bacteria: Key Components of the Human Gut Microbiota. Nutrients. 2023 May 6;15(9):2211. doi: 10.3390/nu15092211. PMID: 37432351; PMCID: PMC10180739. [↩]
- Portincasa P, Bonfrate L, Vacca M, De Angelis M, Farella I, Lanza E, Khalil M, Wang DQ, Sperandio M, Di Ciaula A. Gut Microbiota and Short Chain Fatty Acids: Implications in Glucose Homeostasis. Int J Mol Sci. 2022 Jan 20;23(3):1105. doi: 10.3390/ijms23031105. PMID: 35163038; PMCID: PMC8835596. [↩]
- Xiong RG, Zhou DD, Wu SX, Huang SY, Saimaiti A, Yang ZJ, Shang A, Zhao CN, Gan RY, Li HB. Health Benefits and Side Effects of Short-Chain Fatty Acids. Foods. 2022 Sep 15;11(18):2863. doi: 10.3390/foods11182863. PMID: 36140990; PMCID: PMC9498509. [↩]
- Nogal A, Valdes AM, Menni C. The role of short-chain fatty acids in the interplay between gut microbiota and diet in cardio-metabolic health. Gut Microbes. 2021 Jan-Dec;13(1):1-24. doi: 10.1080/19490976.2021.1897212. PMID: 33764858; PMCID: PMC8007165. [↩] [↩]
- Seong CN, Kang JW, Lee JH, Seo SY, Woo JJ, Park C, Bae KS, Kim MS. Taxonomic hierarchy of the phylum Firmicutes and novel Firmicutes species originated from various environments in Korea. J Microbiol. 2018 Jan;56(1):1-10. doi: 10.1007/s12275-018-7318-x. Epub 2018 Jan 4. PMID: 29299839. [↩]
- Ilinskaya ON, Ulyanova VV, Yarullina DR, Gataullin IG. Secretome of Intestinal Bacilli: A Natural Guard against Pathologies. Front Microbiol. 2017 Sep 1;8:1666. doi: 10.3389/fmicb.2017.01666. PMID: 28919884; PMCID: PMC5586196. [↩] [↩] [↩]
- Catinean A, Neag AM, Nita A, Buzea M, Buzoianu AD. Bacillus spp. Spores-A Promising Treatment Option for Patients with Irritable Bowel Syndrome. Nutrients. 2019 Aug 21;11(9):1968. doi: 10.3390/nu11091968. PMID: 31438618; PMCID: PMC6770835. [↩]
- Martin SE, Kraft CS, Ziegler TR, Millson EC, Rishishwar L, Martin GS. The Role of Diet on the Gut Microbiome, Mood and Happiness. medRxiv [Preprint]. 2023 Mar 21:2023.03.18.23287442. doi: 10.1101/2023.03.18.23287442. PMID: 36993403; PMCID: PMC10055576. [↩]
- Carabotti M, Scirocco A, Maselli MA, Severi C. The gut-brain axis: interactions between enteric microbiota, central and enteric nervous systems. Ann Gastroenterol. 2015 Apr-Jun;28(2):203-209. PMID: 25830558; PMCID: PMC4367209. [↩]
- Mayer, E. A., Nance, K., & Chen, S. (2022). The gut–brain axis. Annual Review of Medicine, 73(Volume 73, 2022), 439–453. https://doi.org/10.1146/annurev-med-042320-014032 [↩]
- Fleming MA 2nd, Ehsan L, Moore SR, Levin DE. The Enteric Nervous System and Its Emerging Role as a Therapeutic Target. Gastroenterol Res Pract. 2020 Sep 8;2020:8024171. doi: 10.1155/2020/8024171. PMID: 32963521; PMCID: PMC7495222. [↩]
- Breit S, Kupferberg A, Rogler G, Hasler G. Vagus Nerve as Modulator of the Brain-Gut Axis in Psychiatric and Inflammatory Disorders. Front Psychiatry. 2018 Mar 13;9:44. doi: 10.3389/fpsyt.2018.00044. PMID: 29593576; PMCID: PMC5859128. [↩]
- Sonali S, Ray B, Ahmed Tousif H, Rathipriya AG, Sunanda T, Mahalakshmi AM, Rungratanawanich W, Essa MM, Qoronfleh MW, Chidambaram SB, Song BJ. Mechanistic Insights into the Link between Gut Dysbiosis and Major Depression: An Extensive Review. Cells. 2022 Apr 16;11(8):1362. doi: 10.3390/cells11081362. PMID: 35456041; PMCID: PMC9030021. [↩]
- Shahini A, Shahini A. Role of interleukin-6-mediated inflammation in the pathogenesis of inflammatory bowel disease: focus on the available therapeutic approaches and gut microbiome. J Cell Commun Signal. 2023 Mar;17(1):55-74. doi: 10.1007/s12079-022-00695-x. Epub 2022 Sep 16. PMID: 36112307; PMCID: PMC10030733. [↩]
- Miller AH, Haroon E, Raison CL, Felger JC. Cytokine targets in the brain: impact on neurotransmitters and neurocircuits. Depress Anxiety. 2013 Apr;30(4):297-306. doi: 10.1002/da.22084. Epub 2013 Mar 6. PMID: 23468190; PMCID: PMC4141874. [↩]
- Bamalan OA, Moore MJ, Al Khalili Y. Physiology, Serotonin. [Updated 2023 Jul 30]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK545168/ [↩]
- De Deurwaerdère P, Di Giovanni G. Serotonin in Health and Disease. Int J Mol Sci. 2020 May 15;21(10):3500. doi: 10.3390/ijms21103500. PMID: 32429111; PMCID: PMC7278959. [↩]
- https://www.mdpi.com/cells/cells-13-01436/article_deploy/html/images/cells-13-01436-g001.png [↩]
- Chen Y, Xu J, Chen Y. Regulation of Neurotransmitters by the Gut Microbiota and Effects on Cognition in Neurological Disorders. Nutrients. 2021 Jun 19;13(6):2099. doi: 10.3390/nu13062099. PMID: 34205336; PMCID: PMC8234057. [↩] [↩]
- Maffei ME. 5-Hydroxytryptophan (5-HTP): Natural Occurrence, Analysis, Biosynthesis, Biotechnology, Physiology and Toxicology. Int J Mol Sci. 2020 Dec 26;22(1):181. doi: 10.3390/ijms22010181. PMID: 33375373; PMCID: PMC7796270.; Wilson N, Robb E, Gajwani R, Minnis H. Nature and nurture? A review of the literature on childhood maltreatment and genetic factors in the pathogenesis of borderline personality disorder. J Psychiatr Res. 2021 May;137:131-146. doi: 10.1016/j.jpsychires.2020.12.025. Epub 2020 Dec 11. PMID: 33677217. [↩]
- Luqman A, Nega M, Nguyen MT, Ebner P, Götz F. SadA-Expressing Staphylococci in the Human Gut Show Increased Cell Adherence and Internalization. Cell Rep. 2018 Jan 9;22(2):535-545. doi: 10.1016/j.celrep.2017.12.058. PMID: 29320746. [↩]
- https://www.frontiersin.org/files/Articles/259363/fncel-11-00074-HTML/image_m/fncel-11-00074-g001.jpg [↩]
- Liu, L., Wang, H., Chen, X., Zhang, Y., Zhang, H., & Xie, P. (2023). Gut microbiota and its metabolites in depression: From pathogenesis to treatment. eBioMedicine, 90. https://doi.org/10.1016/j.ebiom.2023.104527; Mudimela S, Vishwanath NK, Pillai A, Morales R, Marrelli SP, Barichello T, Giridharan VV. Clinical significance and potential role of trimethylamine N-oxide in neurological and neuropsychiatric disorders. Drug Discov Today. 2022 Nov;27(11):103334. doi: 10.1016/j.drudis.2022.08.002. Epub 2022 Aug 23. PMID: 35998800; PMCID: PMC10392962. [↩]
- Liu, L., Wang, H., Chen, X., Zhang, Y., Zhang, H., & Xie, P. (2023). Gut microbiota and its metabolites in depression: From pathogenesis to treatment. eBioMedicine, 90. https://doi.org/10.1016/j.ebiom.2023.104527 [↩] [↩] [↩]
- Mudimela S, Vishwanath NK, Pillai A, Morales R, Marrelli SP, Barichello T, Giridharan VV. Clinical significance and potential role of trimethylamine N-oxide in neurological and neuropsychiatric disorders. Drug Discov Today. 2022 Nov;27(11):103334. doi: 10.1016/j.drudis.2022.08.002. Epub 2022 Aug 23. PMID: 35998800; PMCID: PMC10392962. [↩]
- Arias N, Arboleya S, Allison J, Kaliszewska A, Higarza SG, Gueimonde M, Arias JL. The Relationship between Choline Bioavailability from Diet, Intestinal Microbiota Composition, and Its Modulation of Human Diseases. Nutrients. 2020 Aug 5;12(8):2340. doi: 10.3390/nu12082340. PMID: 32764281; PMCID: PMC7468957. [↩]
- Hagen IV, Helland A, Bratlie M, Midttun Ø, McCann A, Sveier H, Rosenlund G, Mellgren G, Ueland PM, Gudbrandsen OA. TMAO, creatine and 1-methylhistidine in serum and urine are potential biomarkers of cod and salmon intake: a randomised clinical trial in adults with overweight or obesity. Eur J Nutr. 2020 Aug;59(5):2249-2259. doi: 10.1007/s00394-019-02076-4. Epub 2019 Aug 10. PMID: 31401679. [↩]
- Han Y, Wang B, Gao H, He C, Hua R, Liang C, Zhang S, Wang Y, Xin S, Xu J. Vagus Nerve and Underlying Impact on the Gut Microbiota-Brain Axis in Behavior and Neurodegenerative Diseases. J Inflamm Res. 2022 Nov 9;15:6213-6230. doi: 10.2147/JIR.S384949. PMID: 36386584; PMCID: PMC9656367. [↩]
- Kong J, Fang J, Park J, Li S, Rong P. Treating Depression with Transcutaneous Auricular Vagus Nerve Stimulation: State of the Art and Future Perspectives. Front Psychiatry. 2018 Feb 5;9:20. doi: 10.3389/fpsyt.2018.00020. PMID: 29459836; PMCID: PMC5807379.; Carabotti M, Scirocco A, Maselli MA, Severi C. The gut-brain axis: interactions between enteric microbiota, central and enteric nervous systems. Ann Gastroenterol. 2015 Apr-Jun;28(2):203-209. PMID: 25830558; PMCID: PMC4367209. [↩]
- Gautam S, Jain A, Gautam M, Vahia VN, Grover S. Clinical Practice Guidelines for the management of Depression. Indian J Psychiatry. 2017 Jan;59(Suppl 1):S34-S50. doi: 10.4103/0019-5545.196973. PMID: 28216784; PMCID: PMC5310101. [↩] [↩] [↩] [↩] [↩] [↩]
- Zisook S, Johnson GR, Hicks P, Chen P, Beresford T, Michalets JP, Rao S, Thase ME, Wilcox J, Sevilimedu V, Mohamed S. Continuation phase treatment outcomes for switching, combining, or augmenting strategies for treatment-resistant major depressive disorder: A VAST-D report. Depress Anxiety. 2021 Feb;38(2):185-195. doi: 10.1002/da.23114. Epub 2020 Nov 22. PMID: 33225492. [↩] [↩]
- InformedHealth.org [Internet]. Cologne, Germany: Institute for Quality and Efficiency in Health Care (IQWiG); 2006-. In brief: Cognitive behavioral therapy (CBT) [Updated 2022 Jun 2]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK279297/; InformedHealth.org [Internet]. Cologne, Germany: Institute for Quality and Efficiency in Health Care (IQWiG); 2006-. Depression: Learn More – Treatments for depression. [Updated 2020 Jun 18]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK279282/ [↩]
- InformedHealth.org [Internet]. Cologne, Germany: Institute for Quality and Efficiency in Health Care (IQWiG); 2006-. In brief: Cognitive behavioral therapy (CBT) [Updated 2022 Jun 2]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK279297/ [↩]
- Bogowicz P, Curtis HJ, Walker AJ, Cowen P, Geddes J, Goldacre B. Trends and variation in antidepressant prescribing in English primary care: a retrospective longitudinal study. BJGP Open. 2021 Aug 24;5(4):BJGPO.2021.0020. doi: 10.3399/BJGPO.2021.0020. PMID: 33985965; PMCID: PMC8450889. [↩] [↩]
- Hillhouse TM, Porter JH. A brief history of the development of antidepressant drugs: from monoamines to glutamate. Exp Clin Psychopharmacol. 2015 Feb;23(1):1-21. doi: 10.1037/a0038550. PMID: 25643025; PMCID: PMC4428540.; Andrade C, Rao NS. How antidepressant drugs act: A primer on neuroplasticity as the eventual mediator of antidepressant efficacy. Indian J Psychiatry. 2010 Oct;52(4):378-86. doi: 10.4103/0019-5545.74318. PMID: 21267376; PMCID: PMC3025168. [↩]
- Yousuf MS, Kerr BJ. The Role of Regulatory Transporters in Neuropathic Pain. Adv Pharmacol. 2016;75:245-71. doi: 10.1016/bs.apha.2015.12.003. Epub 2016 Jan 21. PMID: 26920015. [↩]
- Hinz M, Stein A, Uncini T. Monoamine depletion by reuptake inhibitors. Drug Healthc Patient Saf. 2011;3:69-77. doi: 10.2147/DHPS.S24798. Epub 2011 Oct 20. Retraction in: Drug Healthc Patient Saf. 2020 Dec 16;12:269. doi: 10.2147/DHPS.S296327. PMID: 22171164; PMCID: PMC3237392. [↩] [↩] [↩]
- Ramic E, Prasko S, Gavran L, Spahic E. Assessment of the Antidepressant Side Effects Occurrence in Patients Treated in Primary Care. Mater Sociomed. 2020 Jun;32(2):131-134. doi: 10.5455/msm.2020.32.131-134. PMID: 32843862; PMCID: PMC7428926. [↩]
- Edinoff AN, Akuly HA, Hanna TA, Ochoa CO, Patti SJ, Ghaffar YA, Kaye AD, Viswanath O, Urits I, Boyer AG, Cornett EM, Kaye AM. Selective Serotonin Reuptake Inhibitors and Adverse Effects: A Narrative Review. Neurol Int. 2021 Aug 5;13(3):387-401. doi: 10.3390/neurolint13030038. PMID: 34449705; PMCID: PMC8395812. [↩]
- Youssef M, Ahmed HY, Zongo A, Korin A, Zhan F, Hady E, Umair M, Shahid Riaz Rajoka M, Xiong Y, Li B. Probiotic Supplements: Their Strategies in the Therapeutic and Prophylactic of Human Life-Threatening Diseases. Int J Mol Sci. 2021 Oct 19;22(20):11290. doi: 10.3390/ijms222011290. PMID: 34681948; PMCID: PMC8537706. [↩]
- Kak G, Raza M, Tiwari BK. Interferon-gamma (IFN-γ): Exploring its implications in infectious diseases. Biomol Concepts. 2018 May 30;9(1):64-79. doi: 10.1515/bmc-2018-0007. PMID: 29856726. [↩]
- Syngai GG, Gopi R, Bharali R, Dey S, Lakshmanan GM, Ahmed G. Probiotics – the versatile functional food ingredients. J Food Sci Technol. 2016 Feb;53(2):921-33. doi: 10.1007/s13197-015-2011-0. Epub 2015 Nov 9. PMID: 27162372; PMCID: PMC4837740. [↩]
- Savaiano DA, Hutkins RW. Yogurt, cultured fermented milk, and health: a systematic review. Nutr Rev. 2021 Apr 7;79(5):599-614. doi: 10.1093/nutrit/nuaa013. PMID: 32447398; PMCID: PMC8579104. [↩]
- Office of Dietary Supplements – Probiotics. (n.d.). Health Professional Fact Sheet. Retrieved September 20, 2024, from https://ods.od.nih.gov/factsheets/Probiotics-HealthProfessional/ [↩] [↩] [↩] [↩] [↩]
- Khalesi S, Bellissimo N, Vandelanotte C, Williams S, Stanley D, Irwin C. A review of probiotic supplementation in healthy adults: helpful or hype? European Journal of Clinical Nutrition. 2018;73(1):24-37. doi:10.1038/s41430-018-0135-9 [↩] [↩]
- Parhofer KG, Laufs U. Lipid Profile and Lipoprotein(a) Testing. Dtsch Arztebl Int. 2023 Sep 4;120(35-36):582-588. doi: 10.3238/arztebl.m2023.0150. PMID: 37403458; PMCID: PMC10552634. [↩]
- Kim EJ, Hong J, Hwang JW. The Association between Depressive Mood and Cholesterol Levels in Korean Adolescents. Psychiatry Investig. 2019 Oct;16(10):737-744. doi: 10.30773/pi.2019.03.24. Epub 2019 Sep 3. PMID: 31474090; PMCID: PMC6801315. [↩]
- Hui L, Yin XL, Chen J, Yin XY, Zhu HL, Li J, Yin GZ, Xu XW, Yang XN, Qian ZK, Jiang CX, Tang Z, Yang HB, Cheung EFC, Chan RCK, Jia QF. Association between decreased HDL levels and cognitive deficits in patients with bipolar disorder: a pilot study. Int J Bipolar Disord. 2019 Nov 25;7(1):25. doi: 10.1186/s40345-019-0159-7. PMID: 31761966; PMCID: PMC6875532. [↩]
- Hutkins RW, Krumbeck JA, Bindels LB, Cani PD, Fahey G Jr, Goh YJ, Hamaker B, Martens EC, Mills DA, Rastal RA, Vaughan E, Sanders ME. Prebiotics: why definitions matter. Curr Opin Biotechnol. 2016 Feb;37:1-7. doi: 10.1016/j.copbio.2015.09.001. Epub 2015 Sep 29. PMID: 26431716; PMCID: PMC4744122. [↩]
- Chow J. Probiotics and prebiotics: A brief overview. J Ren Nutr. 2002 Apr;12(2):76-86. doi: 10.1053/jren.2002.31759. PMID: 11953920. [↩] [↩] [↩]
- Bamigbade GB, Subhash AJ, Kamal-Eldin A, Nyström L, Ayyash M. An Updated Review on Prebiotics: Insights on Potentials of Food Seeds Waste as Source of Potential Prebiotics. Molecules. 2022 Sep 13;27(18):5947. doi: 10.3390/molecules27185947. PMID: 36144679; PMCID: PMC9505924. [↩] [↩]
- Davani-Davari D, Negahdaripour M, Karimzadeh I, Seifan M, Mohkam M, Masoumi SJ, Berenjian A, Ghasemi Y. Prebiotics: Definition, Types, Sources, Mechanisms, and Clinical Applications. Foods. 2019 Mar 9;8(3):92. doi: 10.3390/foods8030092. PMID: 30857316; PMCID: PMC6463098. [↩] [↩]
- KR, Naik SR, Vakil BV. Probiotics, prebiotics and synbiotics- a review. J Food Sci Technol. 2015 Dec;52(12):7577-87. doi: 10.1007/s13197-015-1921-1. Epub 2015 Jul 22. PMID: 26604335; PMCID: PMC4648921. [↩]
- Lebrilla CB, Liu J, Widmalm G, et al. Oligosaccharides and Polysaccharides. In: Varki A, Cummings RD, Esko JD, et al., editors. Essentials of Glycobiology [Internet]. 4th edition. Cold Spring Harbor (NY): Cold Spring Harbor Laboratory Press; 2022. Chapter 3. Available from: https://www.ncbi.nlm.nih.gov/books/NBK579972/ doi: 10.1101/glycobiology.4e.3 [↩]
- Fan R, Burghardt JP, Huang J, Xiong T, Czermak P. Purification of Crude Fructo-Oligosaccharide Preparations Using Probiotic Bacteria for the Selective Fermentation of Monosaccharide Byproducts. Front Microbiol. 2021 Jan 26;11:620626. doi: 10.3389/fmicb.2020.620626. PMID: 33584587; PMCID: PMC7874009. [↩]
- Chen YJ, Sui X, Wang Y, Zhao ZH, Han TH, Liu YJ, Zhang JN, Zhou P, Yang K, Ye ZH. Preparation, structural characterization, biological activity, and nutritional applications of oligosaccharides. Food Chem X. 2024 Mar 15;22:101289. doi: 10.1016/j.fochx.2024.101289. PMID: 38544933; PMCID: PMC10966145. [↩]
- Qin YQ, Wang LY, Yang XY, Xu YJ, Fan G, Fan YG, Ren JN, An Q, Li X. Inulin: properties and health benefits. Food Funct. 2023 Apr 3;14(7):2948-2968. doi: 10.1039/d2fo01096h. PMID: 36876591. [↩]
- Yoo S, Jung SC, Kwak K, Kim JS. The Role of Prebiotics in Modulating Gut Microbiota: Implications for Human Health. Int J Mol Sci. 2024 Apr 29;25(9):4834. doi: 10.3390/ijms25094834. PMID: 38732060; PMCID: PMC11084426. [↩] [↩] [↩]
- Hill D, Sugrue I, Arendt E, Hill C, Stanton C, Ross RP. Recent advances in microbial fermentation for dairy and health. F1000Res. 2017 May 26;6:751. doi: 10.12688/f1000research.10896.1. PMID: 28649371; PMCID: PMC5464223. [↩]
- Cano A, Chedraui P, Goulis DG, Lopes P, Mishra G, Mueck A, Senturk LM, Simoncini T, Stevenson JC, Stute P, Tuomikoski P, Rees M, Lambrinoudaki I. Calcium in the prevention of postmenopausal osteoporosis: EMAS clinical guide. Maturitas. 2018 Jan;107:7-12. doi: 10.1016/j.maturitas.2017.10.004. Epub 2017 Oct 3. PMID: 29169584. [↩]
- Onetto CA, Borneman AR, Schmidt SA. Investigating the effects of Aureobasidium pullulans on grape juice composition and fermentation. Food Microbiol. 2020 Sep;90:103451. doi: 10.1016/j.fm.2020.103451. Epub 2020 Feb 4. PMID: 32336373.; Martínez J, Nevado A, Suñén E, Gabriel M, Vélez-Del-Burgo A, Sánchez P, Postigo I. The Aspergillus niger Major Allergen (Asp n 3) DNA-Specific Sequence Is a Reliable Marker to Identify Early Fungal Contamination and Postharvest Damage in Mangifera indica Fruit. Front Microbiol. 2021 Jun 28;12:663323. doi: 10.3389/fmicb.2021.663323. PMID: 34262539; PMCID: PMC8273346. [↩]
- Wang Y, Wen L, Tang H, Qu J, Rao B. Probiotics and Prebiotics as Dietary Supplements for the Adjunctive Treatment of Type 2 Diabetes. Pol J Microbiol. 2023 Mar 24;72(1):3-9. doi: 10.33073/pjm-2023-013. PMID: 36929892; PMCID: PMC10280329. [↩]
- Doron S, Snydman DR. Risk and safety of probiotics. Clin Infect Dis. 2015 May 15;60 Suppl 2(Suppl 2):S129-34. doi: 10.1093/cid/civ085. PMID: 25922398; PMCID: PMC4490230. [↩]
- Zhang Q, Chen B, Zhang J, Dong J, Ma J, Zhang Y, Jin K, Lu J. Effect of prebiotics, probiotics, synbiotics on depression: results from a meta-analysis. BMC Psychiatry. 2023 Jun 29;23(1):477. doi: 10.1186/s12888-023-04963-x. PMID: 37386630; PMCID: PMC10308754 https://pubmed.ncbi.nlm.nih.gov/37386630/ [↩]
- Lai HC, Young J, Lin CS, et al. Impact of the gut microbiota, prebiotics, and probiotics on human health and disease. Biomedical Journal. 2014;37(5):259. doi:10.4103/2319-4170.138314 [↩]
- You S, Ma Y, Yan B, Pei W, Wu Q, Ding C, Huang C. The promotion mechanism of prebiotics for probiotics: A review. Front Nutr. 2022 Oct 5;9:1000517. doi: 10.3389/fnut.2022.1000517. PMID: 36276830; PMCID: PMC9581195. [↩] [↩] [↩] [↩]
- Gupta RS, Nanda A, Khadka B. Novel molecular, structural and evolutionary characteristics of the phosphoketolases from bifidobacteria and Coriobacteriales. PLoS One. 2017 Feb 17;12(2):e0172176. doi: 10.1371/journal.pone.0172176. PMID: 28212383; PMCID: PMC5315409. [↩]
- Glenn K, Ingram-Smith C, Smith KS. Biochemical and kinetic characterization of xylulose 5-phosphate/fructose 6-phosphate phosphoketolase 2 (Xfp2) from Cryptococcus neoformans. Eukaryot Cell. 2014 May;13(5):657-63. doi: 10.1128/EC.00055-14. Epub 2014 Mar 21. PMID: 24659577; PMCID: PMC4060483. [↩]
- Dempsey E, Corr SC. Lactobacillus spp. for Gastrointestinal Health: Current and Future Perspectives. Front Immunol. 2022 Apr 6;13:840245. doi: 10.3389/fimmu.2022.840245. PMID: 35464397; PMCID: PMC9019120. [↩]
- Yao D, Dai W, Dong M, Dai C, Wu S. MUC2 and related bacterial factors: Therapeutic targets for ulcerative colitis. EBioMedicine. 2021 Dec;74:103751. doi: 10.1016/j.ebiom.2021.103751. Epub 2021 Dec 10. PMID: 34902790; PMCID: PMC8671112. [↩]
- Johansson ME, Hansson GC. Mucus and the goblet cell. Dig Dis. 2013;31(3-4):305-9. doi: 10.1159/000354683. Epub 2013 Nov 14. PMID: 24246979; PMCID: PMC4282926. [↩]
- Vasquez EC, Pereira TMC, Peotta VA, Baldo MP, Campos-Toimil M. Probiotics as Beneficial Dietary Supplements to Prevent and Treat Cardiovascular Diseases: Uncovering Their Impact on Oxidative Stress. Oxid Med Cell Longev. 2019 May 7;2019:3086270. doi: 10.1155/2019/3086270. PMID: 31205584; PMCID: PMC6530239. [↩]
- Afzal S, Abdul Manap AS, Attiq A, Albokhadaim I, Kandeel M, Alhojaily SM. From imbalance to impairment: the central role of reactive oxygen species in oxidative stress-induced disorders and therapeutic exploration. Front Pharmacol. 2023 Oct 18;14:1269581. doi: 10.3389/fphar.2023.1269581. PMID: 37927596; PMCID: PMC10622810. [↩]
- Vermot A, Petit-Härtlein I, Smith SME, Fieschi F. NADPH Oxidases (NOX): An Overview from Discovery, Molecular Mechanisms to Physiology and Pathology. Antioxidants (Basel). 2021 Jun 1;10(6):890. doi: 10.3390/antiox10060890. PMID: 34205998; PMCID: PMC8228183. [↩]
- Johnson D, Letchumanan V, Thum CC, Thurairajasingam S, Lee LH. A Microbial-Based Approach to Mental Health: The Potential of Probiotics in the Treatment of Depression. Nutrients. 2023 Mar 13;15(6):1382. doi: 10.3390/nu15061382. PMID: 36986112; PMCID: PMC10053794. [↩]
- Bartkiene E, Özogul F, Rocha JM. Bread Sourdough Lactic Acid Bacteria-Technological, Antimicrobial, Toxin-Degrading, Immune System-, and Faecal Microbiota-Modelling Biological Agents for the Preparation of Food, Nutraceuticals and Feed. Foods. 2022 Feb 3;11(3):452. doi: 10.3390/foods11030452. PMID: 35159602; PMCID: PMC8834576. [↩]
- Zhao L, Shen Y, Wang Y, Wang L, Zhang L, Zhao Z, Li S. Lactobacillus plantarum S9 alleviates lipid profile, insulin resistance, and inflammation in high-fat diet-induced metabolic syndrome rats. Sci Rep. 2022 Sep 15;12(1):15490. doi: 10.1038/s41598-022-19839-5. PMID: 36109620; PMCID: PMC9478128. [↩]
- Mehdi S, Wani SUD, Krishna KL, Kinattingal N, Roohi TF. A review on linking stress, depression, and insulin resistance via low-grade chronic inflammation. Biochem Biophys Rep. 2023 Nov 1;36:101571. doi: 10.1016/j.bbrep.2023.101571. PMID: 37965066; PMCID: PMC10641573. [↩] [↩]
- Lee SH, Park SY, Choi CS. Insulin Resistance: From Mechanisms to Therapeutic Strategies. Diabetes Metab J. 2022 Jan;46(1):15-37. doi: 10.4093/dmj.2021.0280. Epub 2021 Dec 30. PMID: 34965646; PMCID: PMC8831809. [↩]
- Nakrani MN, Wineland RH, Anjum F. Physiology, Glucose Metabolism. [Updated 2023 Jul 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK560599/ [↩]
- Barkhidarian B, Roldos L, Iskandar MM, Saedisomeolia A, Kubow S. Probiotic Supplementation and Micronutrient Status in Healthy Subjects: A Systematic Review of Clinical Trials. Nutrients. 2021 Aug 28;13(9):3001. doi: 10.3390/nu13093001. PMID: 34578878; PMCID: PMC8472411. [↩]
- Reininghaus EZ, Platzer M, Kohlhammer-Dohr A, Hamm C, Mörkl S, Bengesser SA, Fellendorf FT, Lahousen-Luxenberger T, Leitner-Afschar B, Schöggl H, Amberger-Otti D, Wurm W, Queissner R, Birner A, Falzberger VS, Painold A, Fitz W, Wagner-Skacel J, Brunnmayr M, Rieger A, Maget A, Unterweger R, Schwalsberger K, Reininghaus B, Lenger M, Bastiaanssen TFS, Dalkner N. PROVIT: Supplementary Probiotic Treatment and Vitamin B7 in Depression-A Randomized Controlled Trial. Nutrients. 2020 Nov 8;12(11):3422. doi: 10.3390/nu12113422. PMID: 33171595; PMCID: PMC7695208. [↩] [↩]
- Tang HJ, Chen CC, Lu YC, Huang HL, Chen HJ, Chuang YC, Lai CC, Chao CM. The effect of Lactobacillus with prebiotics on KPC-2-producing Klebsiella pneumoniae. Front Microbiol. 2022 Dec 7;13:1050247. doi: 10.3389/fmicb.2022.1050247. PMID: 36569071; PMCID: PMC9767986. [↩] [↩]
- Rao K, Patel A, Sun Y, Vornhagen J, Motyka J, Collingwood A, Teodorescu A, Baang JH, Zhao L, Kaye KS, Bachman MA. Risk Factors for Klebsiella Infections among Hospitalized Patients with Preexisting Colonization. mSphere. 2021 Jun 30;6(3):e0013221. doi: 10.1128/mSphere.00132-21. Epub 2021 Jun 23. PMID: 34160237; PMCID: PMC8265626. [↩]
- Sawin EA, De Wolfe TJ, Aktas B, Stroup BM, Murali SG, Steele JL, Ney DM. Glycomacropeptide is a prebiotic that reduces Desulfovibrio bacteria, increases cecal short-chain fatty acids, and is anti-inflammatory in mice. Am J Physiol Gastrointest Liver Physiol. 2015 Oct 1;309(7):G590-601. doi: 10.1152/ajpgi.00211.2015. Epub 2015 Aug 6. PMID: 26251473; PMCID: PMC4593820. [↩] [↩]
- Earley H, Lennon G, Balfe A, Kilcoyne M, Clyne M, Joshi L, Carrington S, Martin ST, Coffey JC, Winter DC, O’Connell PR. A Preliminary Study Examining the Binding Capacity of Akkermansia muciniphila and Desulfovibrio spp., to Colonic Mucin in Health and Ulcerative Colitis. PLoS One. 2015 Oct 22;10(10):e0135280. doi: 10.1371/journal.pone.0135280. PMID: 26491870; PMCID: PMC4619660. [↩]
- Chi L, Khan I, Lin Z, Zhang J, Lee MYS, Leong W, Hsiao WLW, Zheng Y. Fructo-oligosaccharides from Morinda officinalis remodeled gut microbiota and alleviated depression features in a stress rat model. Phytomedicine. 2020 Feb;67:153157. doi: 10.1016/j.phymed.2019.153157. Epub 2019 Dec 23. PMID: 31896054. [↩] [↩]
- Nandam LS, Brazel M, Zhou M, Jhaveri DJ. Cortisol and Major Depressive Disorder-Translating Findings From Humans to Animal Models and Back. Front Psychiatry. 2020 Jan 22;10:974. doi: 10.3389/fpsyt.2019.00974. PMID: 32038323; PMCID: PMC6987444. [↩]
- Peterson CT, Sharma V, Uchitel S, Denniston K, Chopra D, Mills PJ, Peterson SN. Prebiotic Potential of Herbal Medicines Used in Digestive Health and Disease. J Altern Complement Med. 2018 Jul;24(7):656-665. doi: 10.1089/acm.2017.0422. Epub 2018 Mar 22. PMID: 29565634; PMCID: PMC6065514. [↩] [↩]



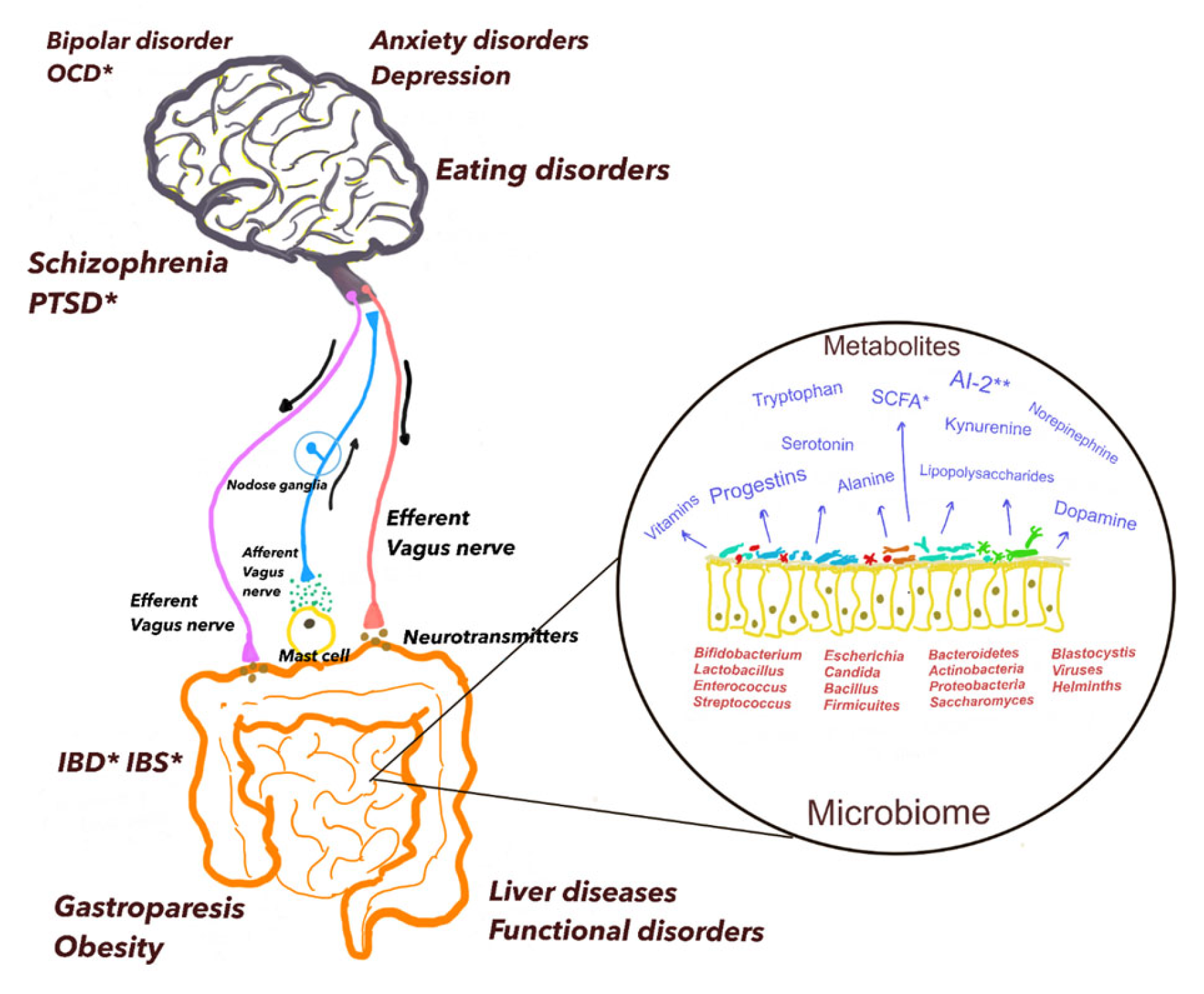{kind=link}