
Meera Yelamanchi, Sarah-Eve Dill1
1 Stanford University
Abstract
Poor mental health has been shown to impair academic achievement in youth. Can small changes in health behavior mitigate this relationship? This study examines the association between young adult mental health and academic achievement, and whether health behaviors—specifically routine doctor visits and health knowledge—moderate this relationship. We used data from the National Longitudinal Survey of Youth 1997, with mental health measured by Mental Health Inventory-5 and academic achievement measured using American College Testing scores. The main finding was that small changes in health behaviors do not significantly moderate the relationship between mental health and academic achievement. Because of the findings, we conducted an exploratory analysis focusing on high and low achievers. We found that for low achievers, routine doctor visits were associated with a difference in the relationship between mental health and academic achievement, while health knowledge did not significantly moderate this association. For high achievers, mental health was not meaningfully associated with academic performance, and neither doctor visits nor health knowledge moderated this relationship. Overall, this study suggests that variation in health behaviors alone may not significantly moderate the relationship between mental health and academic achievement. In the exploratory analysis, low achievers showed variation in the association between academic achievement and mental health.
Keywords: Mental Health, Academic Achievement, and Young Adults.
Introduction
Mental health issues are prevalent among young adults, and specifically, many struggle with anxiety, depression, and stress. Young adulthood is a critical time for the development of mental health disorders, as half of all lifetime cases start at the age of 14 and three-fourths by the age of 241. Poor mental health has been associated with impairments in “emotional, cognitive, and behavioral functioning, such as unsatisfying peer relationships, disruptive behavior, and decreased academic performance”2.
Additionally, mental health issues can harm youth performance in an academic setting. Poor mental health can make it challenging to concentrate, complete assignments, and stay motivated in school. Studies have shown that depressive symptoms are negatively correlated with academic engagement for medical students3. These findings demonstrate that poor mental health can interfere with the learning and motivation of students.
Do small differences in daily health behaviors, like doctor visits and health knowledge, influence mental health and academic performance? Questionnaires given during doctor visits may help identify young adults who are struggling with mental health issues. Specifically, the Patient Health Questionnaire (PHQ-9) is a common tool used to assist in recognizing symptoms of depression4. On the other hand, people with poor mental health may avoid visiting the doctor. According to Shim et al. (2011), a substantial gap exists between the prevalence of depression and actual treatment5. While doctor visits can help catch those who are struggling with mental health symptoms, they may not be enough to address the concerns. Similarly, health knowledge can impact mental health. Research indicates that positive traits and psychological assets can increase resilience and may reduce the development of psychological disorders6. Health knowledge can also make young adults more confident in seeking help, which can lessen feelings of anxiety and depression. However, knowledge does not always translate to behavior. Paakkari and Okan (2020) explain that “health literacy is not only about having knowledge, but about using it to promote personal well-being and resilience”7.
Even if routine doctor visits and health knowledge do not improve mental health directly, they may influence how mental health affects academic performance. For example, a doctor could refer young adults to counselors or therapists to help manage symptoms and stay focused in school8. This may allow a student to stay on track academically without directly treating the mental health issues. Similarly, health knowledge can help a student understand how to manage symptoms, such as stress, in healthy ways9. It can help them avoid unhealthy coping mechanisms that they may not otherwise understand the consequences of. Additionally, better physical health can improve academic success10. Having routine doctor checkups confirms that a student is healthy and that they are taking care of themselves. Having health knowledge may also allow young adults to take proper care of themselves on their own11.
Although previous research has shown the connections between mental health and academic achievement, few studies have examined how small behavior changes can influence this relationship. Many studies have shown a clear connection between mental health and academic performance. For example, research has shown that mental health issues like anxiety, depression, and stress can lower grades and test scores12. Other studies have shown that social support is significantly positively correlated with GPA13. Despite this, few studies have shown the role that routine doctor visits play in the relationship between mental health and academic achievement. Simple habits like routine doctor visits and health knowledge have not been studied as moderators. Understanding the role of these behaviors is important because they are often more accessible, affordable, and convenient than extensive treatments, which makes them a better option for supporting young adults’ mental health and academics.
The overall goal of this paper is to examine whether routine doctor checkups and improved health knowledge moderate the relationship between mental health and academic performance. Specifically, we aim to answer three questions: 1) How are routine doctor visits and health knowledge associated with mental health? 2) How are routine doctor visits and health knowledge associated with ACT score categories? 3) Do routine doctor visits and health knowledge moderate the relationship between mental health and ACT score categories? Answering these questions can help us understand the potential impact routine checkups can have on young adults’ health and learning. By exploring this relationship, we can identify the benefits of having access to healthcare and find direct and indirect ways that health behaviors may influence academic performance.
To answer these questions, we employ a cross-sectional study design and use linear and ordinal regression analyses to examine the relationship between mental health, health knowledge, doctor visits, and academic performance among 1,044 young adults aged 17-22 in the National Longitudinal Survey of the Youth 1997 (NLSY 1997). While this study cannot make causal claims about the effects of health behaviors on mental health or academic performance, this research design allows us to examine the potential moderating role of such health behaviors in the relationship between mental health and academic achievement.
Methods
Data
The data used in this study comes from round 6 (2001) of the NLSY-97. The NLSY-97 is a nationally representative sample of teens who were 12-16 years of age in 1997. Interviewers visited the selected homes and screened for eligible teens who met the study criteria: living in the US and born between 1980 and 1984. The final sample included a nationally representative sample of US teens, with an oversampling of Black and Hispanic teens. Initially, the teens were interviewed annually, then in 2012, it switched to biennial. The interviews were held in person or by phone. Some sensitive questions were privately asked on a computer. The survey collected information on the teens’ education, employment, family, health, behavior, and plans. To get our final analytical sample, we started with all respondents from round 6 (2001) of the NLSY-97 dataset. We then removed individuals who had missing MHI-5 scores, ACT scores, health knowledge scores, or missing doctor visit information. This resulted in a final sample of 1,044 individuals.
Measures
The main independent variable in the analysis is mental health. To measure mental health, we use the Mental Health Inventory-5 (MHI-5), a short 5-question survey that measures mental health. This survey has proven to be a reliable brief measure of mental health in previous research14. It focuses on identifying symptoms of depression, anxiety, and psychological distress. Each of the five questions in the survey is scored from 1 to 4, and some items are reverse-coded so that higher values consistently reflect better mental well-being. For example, participants are asked how often in the past month they felt nervous, calm, downhearted, happy, or depressed. Final scores range from 0 to 20, with higher scores indicating better mental health.
To measure health behaviors, we used doctor visits and health knowledge. Doctor visits are a binary variable; participants got a yes if they had visited the doctor for an annual check-up in the past year, and no if not. Routine doctor visits refer to visiting the doctor annually for general check-ups; this does not include visits for illness or injuries. For the purpose of this study, having one visit a year is considered a small change in health behavior. For health knowledge, participants were asked 10 questions about healthy behaviors, such as “What birth control best prevents sexually transmitted diseases?” and “Does having 5+ drinks increase the risk of liver damage?”. These items were selected because they reflect general awareness and understanding of preventative behaviors that can reduce the risk for health issues. We included all health knowledge questions provided by the NLSY-97 dataset for round 6. Participants got 1 point for each correctly answered question, with final scores ranging from 0-10. Higher scores indicate better health knowledge, which here refers to having a basic understanding of healthy behaviors and safety practices. In this study, achieving foundational health awareness, demonstrated through correctly answering several of the 10 questions, represents a small change. A reliability analysis of this health knowledge test found Cronbach’s alpha of 0.49. This suggests limited internal consistency, which may reflect the range of questions that measure different aspects of health knowledge included in the NLSY-97 survey. Despite the relatively low Cronbach’s alpha, the scale was used because it captures multiple areas of health knowledge and reflects a basic understanding of health-related behaviors.
The dependent variable of interest is academic performance. NLSY has multiple indicators for academic performance, but due to high non-response rates for other measures, we used American College Testing (ACT) scores as our only indicator of academic performance. The ACT is scored from 0-36; however, in the NLSY-97 dataset, the scores range from 1 to 6. Scores between 0-6 became 1, 7-12 became 2, 13-18 became 3, 19-24 became 4, 25-30 became 5, and 31-36 became 6.
Control Variables
In our analysis, we also include several self-reported demographic and socioeconomic control variables. These include gender (male or female), race/ethnicity (Black, Hispanic, Mixed Race, Non-Black/Non-Hispanic), age, household income, mother’s education (years of schooling), and father’s education (years of schooling).
Table 1 presents the characteristics of the final analytical sample of 1,044 participants from the NLSY-97 dataset. The statistics include mental health, health knowledge, ACT scores, age, gender, race/ethnicity, household income, and parental education. Overall, the sample has a roughly equal number of girls and boys and is predominantly non-Black/non-Hispanic.
| Variable | N = 1,0441 |
| Mental Health Score (MHI-5) | 15.29 (2.22) |
| Health Knowledge Score | 231 (22%) |
| ACT Score | |
| 1 | 1 (<0.1%) |
| 2 | 11 (1.1%) |
| 3 | 186 (18%) |
| 4 | 516 (49%) |
| 5 | 269 (26%) |
| 6 | 61 (5.8%) |
| Age (years) | |
| 17 | 13 (1.2%) |
| 18 | 170 (16%) |
| 19 | 230 (22%) |
| 20 | 248 (24%) |
| 21 | 235 (23%) |
| 22 | 148 (14%) |
| Gender | |
| Male | 469 (45%) |
| Female | 575 (55%) |
| Race/Ethnicity | |
| Black | 158 (15%) |
| Hispanic | 101 (9.7%) |
| Mixed Race (non-Black/non-Hispanic) | 8 (0.8%) |
| Non-Black/Non-Hispanic | 777 (74%) |
| Household Income | 72,935 (59,058) |
| Mother’s Education (Years) | 13.89 (2.63) |
| Father’s Education (Years) | 14.2 (3.0) |
| 1 Mean (SD); n (%) | |
Data analysis
To answer the first research question (Is mental health associated with health behaviors (regular doctor checkups and health knowledge) among young adults?), we ran a linear regression with mental health as the dependent variable and doctor visits and health knowledge as the independent variables. We conducted the linear regression both with and without control variables to examine whether the associations remained after accounting for things such as income, race, and sex. Variables in the linear regression analyses were kept in their original scales for interpretability.
To answer the second research question (Is academic achievement associated with health behaviors (regular doctor checkups and health knowledge) among young adults?), we ran an ordinal regression with academic performance as the dependent variable and doctor visits and health knowledge as the independent variables. As above, we conducted the linear regression both with and without control variables using the same method for both questions to allow for comparability. For the ordinal regression analysis, continuous predictor variables, including MHI-5 score, health knowledge, household income, and parental education, were standardized to improve comparability across coefficients.
To answer the third research question (Does having healthier behaviors (regular doctor checkups or better health knowledge) moderate the relationship between mental health and academic achievement?), we ran linear regressions examining the relationship between academic performance (dependent variable) and mental health (independent variable), with and without control variables. To assess the potential moderating effects of health behaviors, we also ran separate regressions, each with an interaction between mental health and one type of health behavior: one model with mental health × doctor visits, and another with mental health × health knowledge.
Separate regression models allow for clearer interpretations of how associations differ when additional variables or interactions are included. We conducted a power analysis for the multiple regression model using eight predictors and the final analytical sample. Assuming that there is a small effect size (f2=0.02) and a significance level of 0.05, the analysis indicated a power of 0.93. This suggests that the study is sufficiently powered to detect small main effects. However, interaction effects are typically smaller and require larger sample sizes to detect reliably. Therefore, the study may have lower statistical power for detecting moderation effects.
Results
Main analysis
Association of Doctor Visits and Health Knowledge with Mental Health
Figure 1 presents box plots of mental health scores by whether young adults had a doctor visit in the past year (Panel A) and by whether they had high or low health knowledge (Panel B).
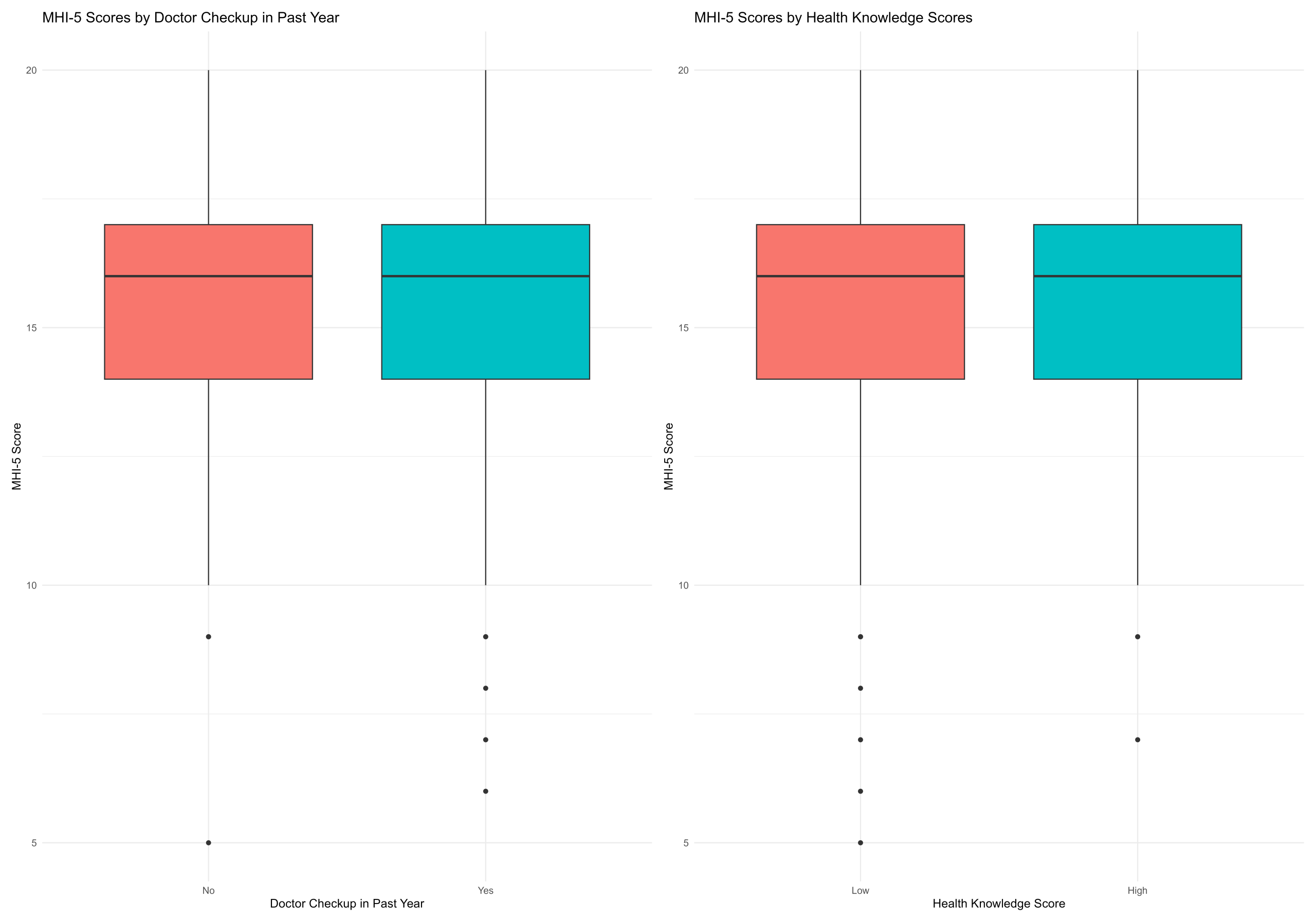
Table 2 shows the results from three regression models that examine how doctor visits and health knowledge relate to mental health. Column 1 shows the results with only doctor visits as an independent variable. The coefficient for doctor checkups is 0.046 (not statistically significant). Column 2 shows only health knowledge as an independent variable. The coefficient for health knowledge is -0.014 (not statistically significant). Column 3 includes doctor visits, health knowledge, and control variables (gender, race, income, and parent education). Doctor visits and health knowledge are not statistically significant. However, there were significant associations among the control variables. Females have lower MHI-5 scores (p<0.001). Mother’s education has a positive coefficient (p<0.05). Father’s education has a negative coefficient(p<0.05).
| Dependent variable: | |||
| MHI-5 Score | |||
| Doctor Visits Only | Health Knowledge Only | Full Model | |
| (1) | (2) | (3) | |
| Routine Doctor Checkup (Yes vs. No) | 0.046 (0.142) | 0.186 (0.144) | |
| Health Knowledge Score | -0.014 (0.020) | -0.017 (0.020) | |
| Female (ref: Male) | -0.704*** (0.141) | ||
| Hispanic (ref: Black) | -0.521 (0.283) | ||
| Mixed Race (ref: Black) | 0.036 (0.794) | ||
| Non-Black/Non-Hispanic (ref: Black) | -0.054 (0.196) | ||
| Household Income | -0.00000 (0.00000) | ||
| Mother’s Education | 0.074* (0.032) | ||
| Father’s Education | -0.057* (0.028) | ||
| Constant | 15.268*** (0.112) | 15.321*** (0.078) | 15.496*** (0.454) |
| Observations | 1,042 | 1,042 | 1,042 |
| R2 | 0.0001 | 0.0004 | 0.038 |
| Adjusted R2 | -0.001 | -0.001 | 0.030 |
| Residual Std. Error | 2.217 (df = 1040) | 2.217 (df = 1040) | 2.183 (df = 1032) |
| F Statistic | 0.105 (df = 1; 1040) | 0.466 (df = 1; 1040) | 4.556*** (df = 9; 1032) |
| Note: *p<0.05; **p<0.01; ***p<0.001 | |||
Association of Doctor Visits and Health Knowledge with Academic Achievement
Figure 2 presents box plots of academic achievement by whether young adults had a doctor visit in the past year (Panel A) and by whether they had high or low health knowledge (Panel B).
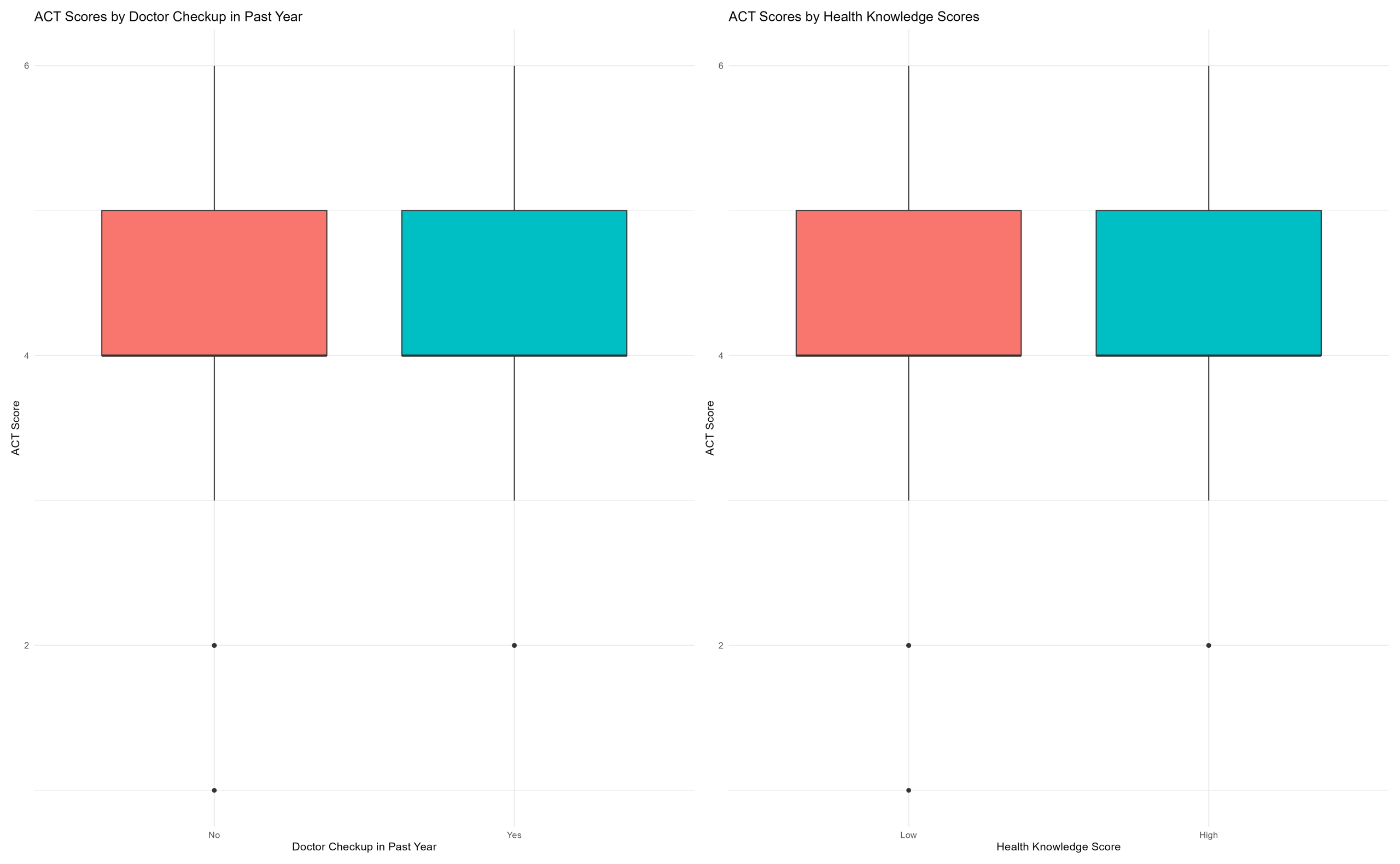
Table 3 shows the results from three regression models that examine how doctor visits and health knowledge relate to academic achievement levels. Column 1 shows the results with only doctor visits as an independent variable. The coefficient for doctor checkups is −0.053 (not statistically significant). Column 2 shows only health knowledge as an independent variable. The coefficient for health knowledge is −0.044 (not statistically significant). Column 3 includes doctor visits, health knowledge, and control variables (gender, race, income, and parent education). Doctor visits and health knowledge are not statistically significant. However, there were significant associations among the control variables. Hispanic participants have higher odds of being in higher ACT score categories (p<0.01). Non-Black/Non-Hispanic participants also have higher odds of being in higher ACT categories (p<0.01). Mother’s education has a positive coefficient (p<0.01). Father’s education has a positive coefficient (p<0.01).
A false discovery rate (FDR) correction was applied to account for multiple testing across predictors in the ACT model. After adjustment, doctor visits and health knowledge remained non-significant, and most associations previously observed in the unadjusted model for the control variables were no longer statistically significant.
| 1|2 | -6.240*** |
| (<0.001) | |
| 2|3 | -3.700*** |
| (<0.001) | |
| 3|4 | -0.498* |
| (0.014) | |
| 4|5 | 2.045*** |
| (<0.001) | |
| 5|6 | 4.186*** |
| (<0.001) |
| Routine Doctor Checkup (Yes vs. No) | -0.055 |
| (0.662) | |
| Health Knowledge Score | -0.089 |
| (0.138) | |
| Female (ref: Male) | 0.024 |
| (0.844) | |
| Hispanic (ref: Black) | 0.876*** |
| (<0.001) | |
| Mixed Race (ref: Black) | 0.905 |
| (0.165) | |
| Non-Black/Non-Hispanic (ref: Black) | 1.504*** |
| (<0.001) | |
| Household Income | -0.000 |
| (0.521) | |
| Mother’s Education | 0.250*** |
| (<0.001) | |
| Father’s Education | 0.393*** |
| (<0.001) | |
| Num.Obs. | 1042 |
| AIC | 2399.6 |
| BIC | 2468.9 |
| RMSE | 3.90 |
| + p < 0.1, * p < 0.05, ** p < 0.01, *** p < 0.001 | |
Moderation Analysis of Health Behaviors on Mental Health and Academic Achievement
Although the main effects were not statistically significant, we tested moderation to examine whether the relationship varied across the levels of health behaviors. Table 4 shows the results from five regression models that examine how mental health is related to academic achievement levels. Column 1 shows the results with only MHI-5 scores as the independent variable. The coefficient is 0.019 (not statistically significant). Column 2 shows MHI-5 scores with added control variables. The coefficient is still 0.016 (not statistically significant). Column 3 shows the full model with MHI-5 scores, doctor visits, health knowledge, and control variables. The coefficient is 0.016 (not statistically significant). Columns 4 and 5 include interaction terms between mental health and doctor visits (Column 4) and mental health and health knowledge (Column 5). The interactions are also visualized in Figure 3. In both model specifications, the interaction terms are not significant.
| (1) | (2) | (3) | (4) | (5) | |
| 1|2 | -6.950*** | -6.139*** | -6.233*** | -6.183*** | -6.144*** |
| (<0.001) | (<0.001) | (<0.001) | (<0.001) | (<0.001) | |
| 2|3 | -4.454*** | -3.596*** | -3.690*** | -3.641*** | -3.603*** |
| (<0.001) | (<0.001) | (<0.001) | (<0.001) | (<0.001) | |
| 3|4 | -1.457*** | -0.397* | -0.484* | -0.440* | -0.394* |
| (<0.001) | (0.024) | (0.013) | (0.023) | (0.025) | |
| 4|5 | 0.769*** | 2.144*** | 2.061*** | 2.101*** | 2.156*** |
| (<0.001) | (<0.001) | (<0.001) | (<0.001) | (<0.001) | |
| 5|6 | 2.779*** | 4.283*** | 4.202*** | 4.241*** | 4.300*** |
| (<0.001) | (<0.001) | (<0.001) | (<0.001) | (<0.001) | |
| MHI-5 Mental Health Standardized Score | 0.068 | 0.069 | 0.069 | 0.040 | 0.067 |
| (0.250) | (0.252) | (0.253) | (0.677) | (0.268) | |
| Routine Doctor Checkup (Yes vs No) | 0.046 | 0.049 | 0.057 | 0.037 | |
| (0.709) | (0.695) | (0.647) | (0.762) | ||
| raceHispanic | 0.886*** | 0.893*** | 0.880*** | 0.897*** | |
| (<0.001) | (<0.001) | (<0.001) | (<0.001) | ||
| Health Knowledge Score | 0.897 | 0.905 | 0.898 | 0.943 | |
| (0.168) | (0.166) | (0.169) | (0.150) | ||
| MHI5 × Doctor Visit Interaction | 1.511*** | 1.507*** | 1.500*** | 1.527*** | |
| (<0.001) | (<0.001) | (<0.001) | (<0.001) | ||
| MHI5 × Health Knowledge Interaction | -0.049 | -0.039 | -0.048 | -0.037 | |
| (0.426) | (0.524) | (0.437) | (0.555) | ||
| Female (ref: Male) | 0.238** | 0.244*** | 0.240** | 0.237** | |
| (0.001) | (<0.001) | (0.001) | (0.001) | ||
| Hispanic (ref: Black) | 0.402*** | 0.399*** | 0.404*** | 0.401*** | |
| (<0.001) | (<0.001) | (<0.001) | (<0.001) | ||
| Mixed Race (ref: Black) | -0.061 | -0.064 | |||
| (0.630) | (0.611) | ||||
| Non-Black/Non-Hispanic (ref: Black) | -0.211 | ||||
| (0.142) | |||||
| Household Income | 0.050 | ||||
| (0.681) | |||||
| Mother’s Education (Years) | -0.087 | ||||
| (0.147) | |||||
| Father’s Education (Years) | 0.094 | ||||
| (0.109) | |||||
| Num.Obs. | 1042 | 1042 | 1042 | 1042 | 1042 |
| AIC | 2564.9 | 2398.7 | 2400.3 | 2402.3 | 2397.9 |
| BIC | 2594.6 | 2463.0 | 2474.5 | 2476.5 | 2472.2 |
| RMSE | 3.92 | 3.90 | 3.90 | 3.90 | 3.90 |
Table 4 | Associations of Mental Health with ACT Scores
Exploratory analysis
As an exploratory extension of the main analyses, we examined whether the associations between mental health, academic performance, and health behaviors differed across achievement levels. High-achieving students may use better coping mechanisms to deal with stress than low-achieving students because they are motivated and proactive in their activities and academics15. This approach may better moderate the relationship between mental health and academic performance for high achievers.
To explore these potential differences, we divide the sample into high and low achievers and re-conduct our analyses. Low achievers were defined as participants with ACT scores of 0-18 (1-3), while high achievers were defined as those with scores of 19-36 (4-6). This cutoff was selected to allow a comparison of results specifically for high- and low-achieving participants. This grouping simplifies the continuous measuring of the ACT scores into two groups for the exploratory analysis.
Table 5 shows the results from five regression models that examine how mental health is related to academic achievement for high achievers. Column 1 shows the results with only MHI-5 scores as the independent variable. The coefficient is 0.017. Column 2 shows MHI-5 scores with added control variables. The coefficient is still 0.017, and the p-value is greater than 0.05. Column 3 shows the full model with MHI-5 scores, doctor visits, health knowledge, and control variables. The coefficient is 0.018. Columns 4 and 5 include interaction terms between mental health and doctor visits (Column 4) and mental health and health knowledge (Column 5) in the full model. In both model specifications, the interaction terms are non-significant. Figure 3 also visualizes the interaction.
| Dependent variable: | |||||
| ACT Score | |||||
| MHI5 Only | MHI5 + Controls | Full | Full + MHI5 × Doctor Visit | Full + MHI5 × Health Knowledge | |
| (1) | (2) | (3) | (4) | (5) | |
| HI-5 Mental Health Score | 0.017 (0.010) | 0.017 (0.010) | 0.018 (0.010) | 0.013 (0.016) | 0.015 (0.011) |
| Routine Doctor Checkup | -0.031 (0.044) | -0.152 (0.316) | -0.031 (0.044) | ||
| Health Knowledge Score | 0.001 (0.006) | 0.001 (0.006) | -0.017 (0.044) | ||
| MHI5 × Doctor Visit Interaction | 0.008 (0.020) | ||||
| MHI5 × Health Knowledge Interaction | 0.001 (0.003) | ||||
| Female (ref: Male) | -0.073 (0.239) | -0.078 (0.240) | -0.074 (0.240) | -0.076 (0.240) | |
| Hispanic (ref: Black) | 0.217** (0.070) | 0.212** (0.070) | 0.212** (0.070) | 0.213** (0.070) | |
| Mixed Race (ref: Black) | -0.00000 (0.00000) | -0.00000 (0.00000) | -0.00000 (0.00000) | -0.00000 (0.00000) | |
| Non-Black/Non-Hispanic (ref: Black) | 0.017 (0.010) | 0.017 (0.010) | 0.017 (0.010) | 0.017 (0.010) | |
| Household Income | 0.039*** (0.009) | 0.039*** (0.009) | 0.040*** (0.009) | 0.039*** (0.009) | |
| Mother’s Education | -0.035 (0.043) | -0.028 (0.044) | -0.028 (0.044) | -0.028 (0.044) | |
| Father’s Education | 0.114 (0.098) | 0.111 (0.098) | 0.112 (0.098) | 0.111 (0.098) | |
| Constant | 4.205*** (0.159) | 3.253*** (0.222) | 3.260*** (0.222) | 3.330*** (0.289) | 3.294*** (0.237) |
| Observations | 845 | 845 | 845 | 845 | 845 |
| R2 | 0.003 | 0.072 | 0.073 | 0.073 | 0.073 |
| Adjusted R2 | 0.002 | 0.063 | 0.062 | 0.061 | 0.061 |
| Residual Std. Error | 0.627 (df = 843) | 0.607 (df = 836) | 0.608 (df = 834) | 0.608 (df = 833) | 0.608 (df = 833) |
| F Statistic | 2.683 (df = 1; 843) | 8.153*** (df = 8; 836) | 6.563*** (df = 10; 834) | 5.973*** (df = 11; 833) | 5.976*** (df = 11; 833) |
| Note: *p<0.05; **p<0.01; ***p<0.001 | |||||
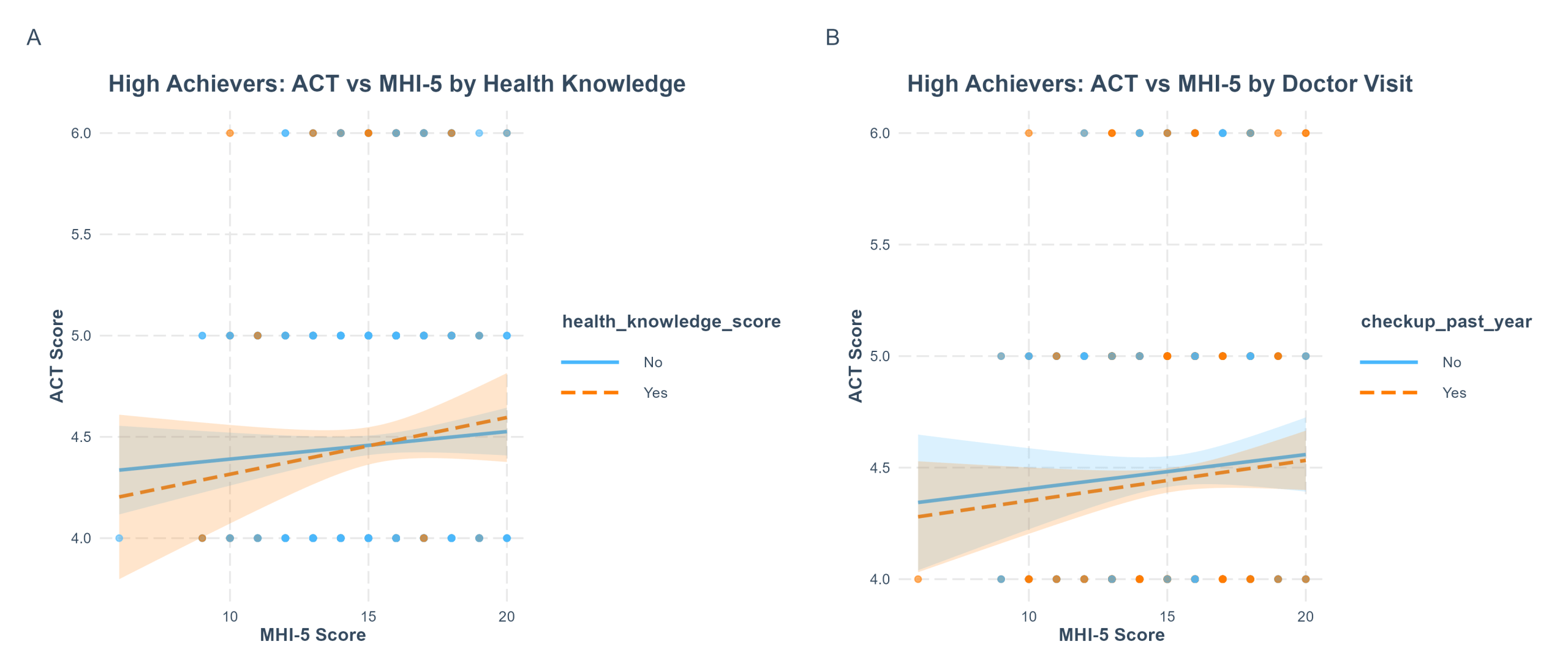
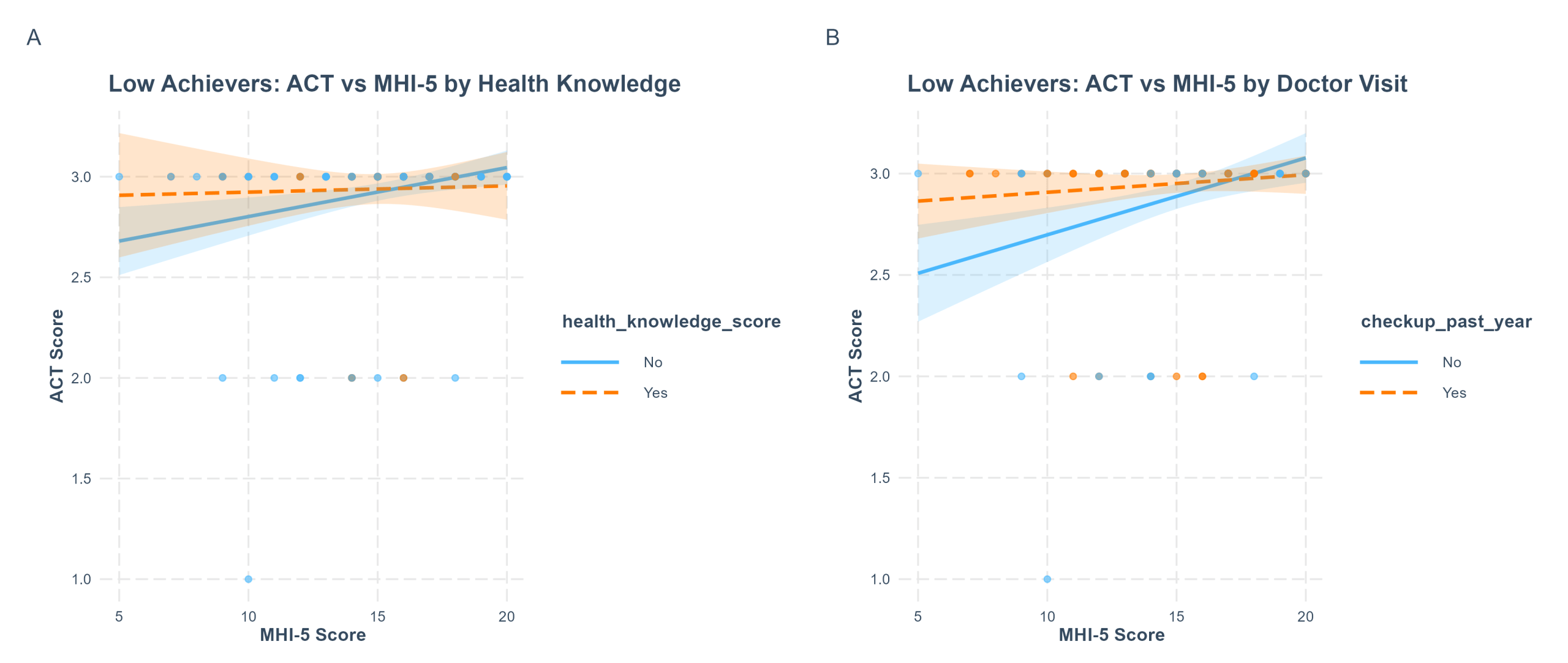
Table 6 shows the results from five regression models that examine how mental health is related to academic achievement for low achievers. Column 1 shows the results with only MHI-5 scores as the independent variable. The coefficient is 0.020 and is statistically significant (p< 0.01). Column 2 shows MHI-5 scores and control variables such as gender, race, income, and parent education. The coefficient is 0.015 and remains statistically significant (p< 0.05). Column 3 shows the full model with MHI-5 scores, doctor visits, health knowledge, and control variables. The coefficient is 0.015. Columns 4 and 5 add interaction terms for doctor visits (column 4) and health behaviors (column 5), and Figure 4 presents these interactions visually. Among underachievers, the interaction term between MHI-5 and doctor visits is statistically significant (p<0.05). The interaction term for health knowledge is not statistically significant.
| Dependent variable: | |||||
| ACT Score | |||||
| MHI5 Only | MHI5 + Controls | Full | Full + MHI5 × Doctor Visit | Full + MHI5 × Health Knowledge | |
| (1) | (2) | (3) | (4) | (5) | |
| MHI-5 Mental Health Score | 0.020** (0.007) | 0.015* (0.007) | 0.015* (0.007) | 0.034** (0.011) | 0.016* (0.008) |
| Routine Doctor Checkup | 0.042 (0.039) | 0.518* (0.214) | 0.043 (0.039) | ||
| Health Knowledge Score | 0.003 (0.005) | 0.004 (0.005) | 0.015 (0.031) | ||
| MHI5 × Checkup Interaction | -0.031* (0.014) | ||||
| MHI5 × Health Knowledge Interaction | -0.001 (0.002) | ||||
| Female (ref: Male) | 0.085 (0.251) | 0.072 (0.252) | 0.102 (0.250) | 0.068 (0.253) | |
| Hispanic (ref: Black) | 0.062 (0.040) | 0.065 (0.040) | 0.068 (0.040) | 0.064 (0.041) | |
| Mixed Race (ref: Black) | 0.00000 (0.00000) | 0.00000 (0.00000) | 0.00000 (0.00000) | 0.00000 (0.00000) | |
| Non-Black/Non-Hispanic (ref: Black) | 0.014 (0.008) | 0.014 (0.008) | 0.014 (0.008) | 0.014 (0.008) | |
| Household Income | 0.014 (0.007) | 0.014 (0.007) | 0.016* (0.007) | 0.014 (0.007) | |
| Mother’s Education | 0.062 (0.037) | 0.052 (0.038) | 0.059 (0.038) | 0.051 (0.038) | |
| Father’s Education | -0.058 (0.058) | -0.058 (0.058) | -0.046 (0.058) | -0.058 (0.058) | |
| Constant | 2.634*** (0.109) | 2.256*** (0.143) | 2.232*** (0.145) | 1.908*** (0.202) | 2.214*** (0.153) |
| Observations | 197 | 197 | 197 | 197 | 197 |
| R2 | 0.038 | 0.180 | 0.188 | 0.210 | 0.188 |
| Adjusted R2 | 0.033 | 0.145 | 0.144 | 0.163 | 0.140 |
| Residual Std. Error | 0.264 (df = 195) | 0.248 (df = 188) | 0.249 (df = 186) | 0.246 (df = 185) | 0.249 (df = 185) |
| F Statistic | 7.738** (df = 1; 195) | 5.168*** (df = 8; 188) | 4.298*** (df = 10; 186) | 4.462*** (df = 11; 185) | 3.903*** (df = 11; 185) |
| Note: *p<0.05; **p<0.01; ***p<0.001 | |||||
Discussion
The goal of the study was to understand how maintaining healthy habits (regular doctor visits or better health knowledge) changes the relationship between mental health and academic achievement. My first hypothesis was that participants who maintained healthy habits in the last year would have higher MHI-5 scores than those who did not. Previous studies have demonstrated that students who follow healthy habits present the least clinical symptoms of mental health16. However, the findings showed that those who maintained healthy habits had the same MHI-5 scores as those who did not. My second hypothesis was that young adults who maintained healthy habits in the past year would have higher test scores than those who did not. Past research has found that students who follow healthy lifestyles and do healthy behaviors have higher academic achievement17. Still, my findings were that healthy habits were not significantly associated with test scores. I also hypothesized that young adults with higher MHI-5 scores (better mental health) would have higher test scores. The finding was that those with higher MHI-5 had the same test scores as those who did not. Lastly, I predicted that for young adults who maintained healthy habits in the past year, the relationship between mental health and academic performance would be weaker. This is based on the idea that general doctor check-ups and health knowledge could allow for early detection of mental health issues and increase awareness of coping strategies for stress, which may help weaken the association between mental health and academic achievement without directly improving either outcome. Evidence from prior studies suggests that routine doctor visits can lead to early recognition of mental health symptoms and referrals to specialists18. This might help reduce its negative impacts on academic performance. Young adults with greater health knowledge may be aware of coping strategies that potentially buffer the effect of poor mental health on academic achievement. These habits do not directly enhance mental health and academic achievement, but may allow the relationship between them to weaken. Despite this conceptual reasoning, the finding was that maintaining healthy habits does not have a significant correlation with the relationship between mental health and academic performance.
In the exploratory analysis, however, I found that low achievers showed a statistically significant association between mental health, academic performance, and health behavior, whereas high achievers did not. Specifically, for low academic achievers, better mental health was significantly associated with better academic performance; and maintaining healthy habits, like having annual doctor checkups and high health knowledge, significantly moderated the relationship between mental health and academic performance such that young adults who maintained healthy habits (such as having regular doctor visits) showed a weaker relationship between mental health and academic performance than those who did not maintain healthy habits.
Why do small health behavior changes have limited impacts?
Our main finding was that small health behavior changes are not associated with changes in mental health and academic performance, which contradicted our hypothesis. This result also contradicts the results of other papers. According to Reuter and Forster (2020), there are significant associations between healthy behaviors and better academic outcomes; specifically, substance abuse was associated with lower GPA, and students who reported regular physical activity had higher GPAs19. Similarly, Lederer et al. (2025) say “protective behaviors corresponded with higher GPAs…most risk behaviors with lower GPAs”20. This difference may be because the changes measured in our study were too minor to have measurable effects. Previous research shows that significant health behaviors are linked with better academic outcomes, but small, infrequent behaviors may not be sufficient to have a measurable effect.
Additionally, this study was cross-sectional and could not assess how long-term consistency with these habits would affect the outcome. It is possible that continuing these healthy habits and applying health knowledge over time may be more closely associated with changes in mental health and academic performance.
Plus, these small health behaviors may not be effective on their own. Having health knowledge does not directly correspond to applying it. Young adults may be aware of healthy practices they should follow, but outside factors may influence them to act differently21. Consistently applying knowledge in daily life may lead to different outcomes than knowledge alone. It also may be necessary for young adults to receive more consistent healthcare support beyond routine checkups. Although regular checkups can provide health knowledge, information alone may not be sufficient to elicit meaningful behavioral or academic changes.
Furthermore, these outside factors, such as parental education and socioeconomic status, may have a stronger effect on the outcomes. For instance, young adults from families with higher parental education and greater financial resources often have better access to educational materials and extracurricular opportunities, which can directly improve academic performance and well-being22.
Exploratory analysis: High vs Low Achievers
The main finding of the exploratory analysis was that low achievers showed statistically significant associations between mental health, academic performance, and health behaviors, whereas high achievers did not. This is consistent with prior research; in a study by Hogberg et al. (2024), the authors say, “low‑achieving students had by far the highest risks of internalizing disorders”23. This may reflect differences in the risks of mental health issues across achievement levels. Small healthy habits were associated with differences in the relationship between mental health and academic performance for low achievers.
Strengths
The strengths of the research include the large sample size of 1,044 individuals, which is from the NLSY-97 dataset. Using a substantial sample size from a well-regarded, nationally representative dataset increases the reliability and generalizability of the findings. In addition, the exploratory analysis suggests a potential benefit of health behaviors for underachievers, which contributes to our knowledge on identifying interventions that may help underachievers improve outcomes through accessible health behaviors.
Limitations
The main limitation of this study is that the analyses show correlations rather than causal relationships. Another limitation is that the health behaviors measured may have weak signals, contributing to the null findings in the main analysis. Additionally, due to the lack of data in other academic performance measures, ACT scores were the available measure, which may not fully show the participants’ overall academic performance. In the future, studies should explore the causal relationship between health behaviors, academic achievement, and mental health rather than just correlations to understand if small health behaviors directly impact student outcomes. Future research should also include multiple academic performance measures in the analyses, such as grade point averages, course grades, and teacher evaluations, to capture participants’ overall academic ability. Plus, because of the binned ACT scores, the reliability of the linear regression in the exploratory analyses is limited by a restricted range. In the low-achievers subgroup, ACT scores are heavily concentrated in one category, indicating limited variation in academic performance. For this reason, the exploratory analysis results should be interpreted with caution and in this context. Lastly, the binary coding of doctor checkups oversimplifies healthcare access. The binary coding of doctor visits was limited by the structure of the NLSY-97 variable, which measured whether respondents had a routine checkup within the past year. We acknowledge that this measure may not fully capture the complexity of healthcare access, including frequency, quality, consistency, or barriers to care.
Implications
Overall, this study shows that small healthy habits alone may not be enough to noticeably improve mental health or academic performance for young adults. These findings indicate that long-term factors may play a larger role in these outcomes than small health behaviors. Exploring more beneficial and effective healthy habits is important to understand the routines that young adults should follow to improve their lives. However, for low achievers, even these small changes may be associated with differences in the relationship between academic achievement and mental health. This suggests that promoting healthy routines and health literacy might be effective, particularly for young adults struggling academically. Schools and healthcare systems may benefit from providing students with basic health knowledge and support for healthy routines, even if they may not have the same impact across students.
References
- Kessler, Ronald C et al. “Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication.” Archives of general psychiatry vol. 62,6 (2005): 593-602. doi:10.1001/archpsyc.62.6.593 [↩]
- Lin, J., & Guo, W. (2024). The Research on Risk Factors for Adolescents’ Mental Health. Behavioral sciences (Basel, Switzerland), 14(4), 263. https://doi.org/10.3390/bs14040263 [↩]
- Sinval, Jorge, et al. “Exploring the Impact of Depression, Anxiety, Stress, Academic Engagement, and Dropout Intention on Medical Students’ Academic Performance: A Prospective Study.” Journal of Affective Disorders, 2024, https://doi.org/10.1016/j.jad.2024.09.116 [↩]
- K. Kroenke, R. Spitzer, J. Williams. The PHQ-9: validity of a brief depression severity measure. Journal of General Internal Medicine. Vol. 16, pg. 606–613, 2001. https://doi.org/10.1046/j.1525-1497.2001.016009606 [↩]
- R. Shim, P. Baltrus, J. Ye, G. Rust. Prevalence, treatment, and control of depressive symptoms in the United States: results from the National Health and Nutrition Examination Survey (NHANES), 2005–2008. Journal of the American Board of Family Medicine. Vol. 24, pg. 33–38, 2011. https://doi.org/10.3122/jabfm.2011.01.100121 [↩]
- R. Kobau, M. E. Seligman, C. Peterson, E. Diener, M. M. Zack, D. Chapman, W. Thompson. Mental health promotion in public health: perspectives and strategies from positive psychology. American Journal of Public Health. Vol. 101, pg. e1–e9, 2011, https://doi.org/10.2105/AJPH.2010.300083 [↩]
- L. Paakkari, O. Okan. COVID-19: health literacy is an underestimated problem. The Lancet Public Health. Vol. 5, pg. e249–e250, 2020, https://doi.org/10.1016/S2468-2667(20)30086-4 [↩]
- Power, T. J., Blum, N. J., Guevara, J. P., Jones, H. A., & Leslie, L. K. (2013). Coordinating Mental Health Care Across Primary Care and Schools: ADHD as a Case Example. Advances in school mental health promotion, 6(1), 68–80. https://doi.org/10.1080/1754730X.2013.749089 [↩]
- Sergeyev, N., Bodek, H., Krishnan, A., Rabin, L., Fasano, K., Jones, J., & Miles, R. (2025). The impact of mental health literacy on resource utilization for academic stress in a diverse student cohort. BMC psychology, 13(1), 851. https://doi.org/10.1186/s40359-025-03142-9 [↩]
- Redondo-Flórez, L., Ramos-Campo, D. J., & Clemente-Suárez, V. J. (2022). Relationship between Physical Fitness and Academic Performance in University Students. International journal of environmental research and public health, 19(22), 14750. https://doi.org/10.3390/ijerph192214750 [↩]
- Pulimeno, M., Piscitelli, P., Colazzo, S., Colao, A., & Miani, A. (2020). School as ideal setting to promote health and wellbeing among young people. Health promotion perspectives, 10(4), 316–324. https://doi.org/10.34172/hpp.2020.50 [↩]
- M. Rožman, I. Vrečko, P. Tominc. Psychological factors impacting academic performance among business studies’ students. Education Sciences. Vol. 15, pg. 121, 2025, https://doi.org/10.3390/educsci15020121 [↩]
- Dong, Xue et al. “The Mental Health and Grade Point Average among College Students from Lower Socioeconomic Status Based on Healthcare Data Analysis.” Journal of healthcare engineering vol. 2021 2378202. 30 Nov. 2021, doi:10.1155/2021/2378202 [↩]
- Friedman, B., Heisel, M., & Delavan, R. (2005). Validity of the SF-36 five-item Mental Health Index for major depression in functionally impaired, community-dwelling elderly patients. Journal of the American Geriatrics Society, 53(11), 1978–1985. https://doi.org/10.1111/j.1532-5415.2005.00469 [↩]
- Caindoy, Ernilson C. “Stress and Coping Strategies of High Performing and Low Performing Students in Hyblend Space: Basis for Psychosocial Support Program.” Psychology and Education: A Multidisciplinary Journal, vol. 23, no. 10, 2024, pp. 1213-31, https://doi.org/10.5281/zenodo.13341539 [↩]
- Ruiz-Hernández, José Antonio, et al. “Mental Health and Healthy Habits in University Students: A Comparative Associative Study.” European Journal of Investigation in Health, Psychology and Education, vol. 12, no. 2, 2022, pp. 114-126, https://doi.org/10.3390/ejihpe12020010 [↩]
- Stea, T. H., and M. K. Torstveit. “Association of Lifestyle Habits and Academic Achievement in Norwegian Adolescents: A Cross-Sectional Study.” BMC Public Health, vol. 14, no. 829, 2014, https://doi.org/10.1186/1471-2458-14-829 [↩]
- Pfoh, E. R., Janmey, I., Anand, A., Martinez, K. A., Katzan, I., & Rothberg, M. B. (2020). The Impact of Systematic Depression Screening in Primary Care on Depression Identification and Treatment in a Large Health Care System: A Cohort Study. Journal of general internal medicine, 35(11), 3141–3147. https://doi.org/10.1007/s11606-020-05856-5 [↩]
- P. R. Reuter, B. L. Forster. Student health behavior and academic performance. PeerJ. Vol. 9, pg. e11107, 2021, https://doi.org/10.7717/peerj.11107. [↩]
- A. M. Lederer, S. B. Oswalt, M. T. Hoban, M. N. Rosenthal. Health-related behaviors and academic achievement among college students. American Journal of Health Promotion. Vol. 38, pg. 1129–1139, 2024, https://doi.org/10.1177/08901171241255768 [↩]
- Nagy-Pénzes, Gabriella et al. “Does Better Health-Related Knowledge Predict Favorable Health Behavior in Adolescents?.” International journal of environmental research and public health vol. 17,5 1680. 4 Mar. 2020, doi:10.3390/ijerph17051680 [↩]
- M. Vukojević, A. Zovko, I. Talić, M. Tanović, B. Rešić, I. Vrdoljak, B. Splavski. Parental socioeconomic status as a predictor of physical and mental health outcomes in children – literature review. Acta Clinica Croatica. Vol. 56, pg. 742–748, 2017, https://doi.org/10.20471/acc.2017.56.04.23 [↩]
- B. Högberg, M. Strandh, S. Petersen, K. Nilsson. Associations between academic achievement and internalizing disorders in Swedish students aged 16 years between 1990 and 2018. European Child & Adolescent Psychiatry. Vol. 34, pg. 1661–1671, 2025, https://doi.org/10.1007/s00787-024-02597-2 [↩]



{kind=link}