
Abstract
Currently, sleep quality and procrastination are two interrelated concerns increasingly affecting adolescent well-being in the globe, yet their relationship remains underexplored among Chinese secondary school students. This study examined the association between procrastination and sleep quality among 30 Chinese high school students (16 males, 14 females) aged 16 to 18 by using a mixed-method approach to combine the Aitken Procrastination Inventory (API) and the Pittsburgh Sleep Quality Index (PSQI) with qualitative interviews. Descriptive analysis revealed moderate procrastination levels and generally poor sleep quality across the sample, with daytime dysfunction and sleep latency identified as the most salient sleep concerns. Following Bonferroni correction for multiple comparisons (adjusted α = 0.006), there are observed no significant overall association between procrastination and sleep quality in the total sample (r=0.298, p>0.05). Gender-stratified analyses revealed that procrastination was significantly associated with sleep medication use among female students (r = 0.727, p = 0.003). Trend-level associations were also observed among females between procrastination and overall sleep quality, sleep latency, and daytime dysfunction, though these did not survive Bonferroni correction. These findings highlight the importance of gender-sensitive approaches in understanding and addressing the procrastination-sleep relationship among Chinese adolescents.
Keywords: Procrastination, Sleep Quality, Chinese Secondary Students, Pittsburgh Sleep Quality Index, Gender Differences
Introduction
Sleep quality has become an important global health concern, as it is a crucial physiological function necessary for human survival and overall health1. Both the amount and quality of sleep are vital for mental well-being, mood regulation, and the proper functioning of the cardiovascular, cerebrovascular, and metabolic systems2,3. Globally, poor sleep and sleep disorders are widespread, which contribute to a range of chronic health conditions. It has been estimated that approximately 50 to 70 million Americans suffer from poor quality of sleep1, while other research reported approximately about 40%-50% of global older adults experience poor sleep quality4,5.
Among adolescents specifically, there are also increasing concerns about their quality of sleep problems. Chronic sleep loss and associated sleepiness and daytime impairments in adolescence represent a serious public health concern, threatening academic success, health, and safety of young people6. Insufficient sleep in this population has been associated with impaired memory consolidation, reduced concentration, weakened decision-making capacity, and diminished academic performance, while all critical concerns for students facing high-stakes educational environments7. Adolescent sleep behaviour undergoes significant physiological maturation during this developmental period, with chronic sleep insufficiency being common and sleep playing a key role in supporting learning, memory, attention, and emotion processing6,7.
Apart from physical environmental factors (e.g. light, noise, temperature, and bedding) that influence sleep quality8, a growing body of research has examined the role of societal and psychological factors. Among these, procrastination has received increasing scholarly attention. Procrastination is broadly defined as the voluntary delay of an intended course of action despite expecting to be worse off for the delay9. A meta-analysis of procrastination based on 691 correlations identified it as a prevalent and pernicious form of self-regulatory failure, with strong and consistent predictors including task aversiveness, low self-efficacy, and impulsiveness9. In modern societies, increasing workloads and rising social pressures have contributed to a significant increase in procrastination behaviours or sleep quality, particularly among students facing intensifying academic demands9,10,11,12.
It is important to note that procrastination is not a unidimensional construct. Scholars have distinguished between trait procrastination, which refer to a dispositional tendency to delay tasks across multiple life domains9, and bedtime procrastination that is the specific behaviour of delaying going to bed without external obstacles11. The present study employs the Aitken Procrastination Inventory (API), which measures trait procrastination as a general behavioural tendency13,14, and this distinction is important when interpreting findings in relation to existing literature.
The theoretical basis for expecting a relationship between procrastination and sleep quality is grounded in the Procrastination-Health Model15. This model posits that procrastination contributes to poor health outcomes through stress as a key mediating mechanism, whereby habitual task delay generates accumulating stress and self-regulatory failure that disrupts processes necessary for healthy sleep. Sirois et al. empirically tested this model across two student samples, finding that stress mediated the association between procrastination and poorer sleep across multiple dimensions, including subjective sleep quality, sleep latency, sleep disturbance, and daytime drowsiness15. Building on this theoretical foundation, Kroese et al. found that bedtime procrastination was associated with insufficient sleep duration and declining sleep quality16, while Ma et al. demonstrated that bedtime procrastination predicted both the prevalence and severity of poor sleep quality among Chinese undergraduates17. Beyond procrastination specifically, Hysing et al. found a dose-response relationship between electronic device use at bedtime and shorter sleep duration and longer sleep onset latency among 9,846 adolescents aged 16 to 1918 — findings particularly relevant given that procrastinatory digital activities represent a key evening behavioural pathway linking task delay to disrupted sleep onset. Collectively, these studies provide convergent empirical support for a procrastination-sleep relationship, though it is important to note that the construct of bedtime procrastination studied in these works remains distinct from the trait procrastination measured in the present study, and their findings should therefore be interpreted with appropriate caution.
Despite this growing evidence, existing literature has focused predominantly on adult and undergraduate populations, with considerably less attention paid to secondary school adolescents. This gap is particularly significant in the Chinese educational context, where secondary school students aged 16 to 18 face intensifying academic demands driven by university entrance examination preparation, creating conditions of chronic stress and self-regulatory strain. Furthermore, gender differences in both procrastination and sleep quality have been reported in the literature yet remain underexplored among Chinese adolescent samples. Research indicates that female adolescents are more prone to rumination and worry, which are perpetuating features of insomnia, potentially making them more susceptible to sleep disturbances arising from unresolved cognitive and emotional stressors.
To address the gap, this research examine the relationship procrastination and sleep quality among Chinese high school students aged 16 to 18 who is facing intensifying academic demands and social pressures in the context of university entrance preparation. The research is guided by the overarching research question: “To what extent is procrastination associated with sleep quality, and does this association differ by gender”. Based on this, two sub-questions are proposed as: (RQ1) what are the levels of procrastination and sleep quality among Chinese secondary school students, and are there any gender differences? (RQ2) Is there a significant association between procrastination and overall sleep quality, and which specific sleep dimensions are most strongly related to procrastination, and do these association differ by gender? Further, differing from existing studies largely relied on quantitative analysis, the study applied a mixed method to combine qualitative and quantitative approach to generate a holistic understanding. As such, the research make contribution to existing literature in both empirical and methodological additions.
Materials and Methods
Materials
1) Aitken Procrastination Inventory (API): Procrastination was assessed by using the API, which is a self-report measure designed to evaluate chronic and persistent procrastination behaviors. The original API13 was revised by Chen et al.14 to better reflect the characteristics of Chinese student populations. The revised version demonstrated acceptable internal consistency, with Cronbach’s α = 0.80. The scale consists of 19 items rated on a five-point Likert scale (1= strongly disagree to 5 = strongly agree). Nine items (Items 2, 4, 7, 11, 12, 14, 16, 17, and 18) are reverse-coded prior to calculating total scores. Higher total scores indicate greater levels of chronic procrastination. In the present study, which focused on an adolescent sample, the internal consistency of the API was satisfactory (Cronbach’s α = 0.79).
2) Pittsburgh Sleep Quality Index (PSQI): Sleep quality was measured by using the PSQI19, which is a widely used self-report instrument assessing sleep quality. The Chinese version revised by Liu et al.20 was used in the present study. The PSQI consists of 18 items that generate seven component scores: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleep medication, and daytime dysfunction. Each component is scored on a 4-point scale (0–3). The seven component scores are summed to produce a total score ranging from 0 to 21, with higher scores indicating poorer sleep quality. In the current sample, internal consistency was modest (Cronbach’s α = 0.65).
3) Open-ended questions: in complementary to above structured-questionnaire, 6 open-ended questions were designed for a short semi-structured interview to obtain in-depth of student behaviors in procrastination and sleep, as informed by Nauts et al.21. The topic of those questions covered: a) student routine in time management, b) students routine in delaying school-tasks as procrastination habits, c) whether delaying work affects sleep, d) bedtime routine and late-night habits, e) effects of staying up late as well as f) improvement to reduce procrastination or sleep better.
Procedure
1) Pre-testing: a pre-testing of API and PSQI was carried out in 10 selected high school participants with a gender balance, which was aimed to make sure the question is well understood and also to obtain an insight of time consuming in completing the questionnaires. After the pre-testing, a minor wording revision were made only in the introductory section of questionnaire to improve the clarify and readability, while the content remained unchanged from the validated version published by Chen et al. for API14 and Liu et al for PSQI20.
2) Formal questionnaire survey: This study received formal ethical approval from the institutional committee of Chinese World Academy (CWA) prior to data collection. The CWA also help to disseminate the call for participation within the school. The formal questionnaire survey was conducted with a total of 32 high school students, who were recruited for this study. Participants recruitment is based on an open call for voluntary participation through the schools’ internal website. The age group was targeted to 16 to 18, as students within this range are generally subject to higher academic workloads and are at a critical stage of development regulatory and time management skills within the Chinese educational context17. Following recruitment, informed consent was obtained from the participants and their guardians to ensure that they fully understood the research objectives, the use of the results, and the potential benefits and risks. Upon obtaining informed consent, the recruited participants received an email that included the formal consent form and a QR code providing access to the questionnaire on the “Tencent Questionnaire” platform (https://wj.qq.com), where they could complete the survey anonymously. A 94% completion rate resulted in 30 valid questionnaires, including 14 from female students and 16 from male students. Responses showing extreme patterns (e.g., identical answers to all items) or completed in an excessively short time (under 2 minutes) were excluded, as suggested by Wright22.
3) Semi-structured interviews: After the completion of the API and PSQI, approximately 20% of the total sample (n=6) were randomly selected for qualitative interviews, a proportion consistent with mixed-method protocol23. Of those invited, five were agreed to participate and respond to six open-ended questions. Interviews were conducted in Mandarin Chinese at garden in the school to ensure the comfort of interviewee. Each interview lasted approximately 15–20 minutes each, and were audio-recorded with participants’ consent. The qualitative data, as a complement to the quantitative survey, helped to enrich and strengthen the robustness of the empirical findings.
Data Analysis
The data analysis was carried out both quantitatively and qualitatively. Data generated from the questionnaire survey were processed using Microsoft Excel. Descriptive statistical analysis was performed to generate insights into the total scores of the API and PSQI. Independent-samples t-tests were conducted across gender to examine differences between male and female students on the API indicators and PSQI. To further understand the correlation between PSQI and API, Pearson correlation analysis was performed to test the significance of the relationships between total scores and across gender groups, which followed by a performance of Bonferroni multiple-testing for exact p-value. As for the qualitative analysis, the interview data were recorded, transcribed, and subjected to content analysis to uncover students’ delaying behaviors and sleep habits. The qualitative findings were further used to inform and interpret the quantitative results. This combination of quantitative and qualitative approaches generated a robust range of analyses, helping to better understand the patterns and relationships between procrastination and sleep quality.
Results
API and PSQI: a Descriptive Overview and Gender Differences
Figure 1 present both descriptive overview of API and PSQI of total sample (n =30) as well as their gender difference analysis by T-testing. As shows, the mean API total score of 51.93 (SE = 1.78) falls below the theoretical midpoint of the scale (midpoint = 57, range 19–95), which suggest a moderate level of procrastination tendency within the sample13. As for the Regarding sleep quality, the mean PSQI total score was 6.70 (SE = 0.74). Given that a PSQI total score above 5 is commonly used as a cut-off point for poor sleep quality19, the average score suggests that students in this sample experienced relatively poor sleep quality. Interviews from student also qualitative indicated these findings, as quoted below:
“Procrastination forces me to continue working on homework assignments after school lights out. Sometimes I stay up very late, resulting in sleep deprivation and drowsiness during class the next day.” (Interviewee #2-2025)
“If I occasionally procrastinate, for example, by watching short videos instead of doing homework…it leads to me having to finish my tasks later. Consequently, my sleep time is reduced, and I feel quite tired the following day.” (Interviewee #3-2025)
“If I procrastinates, tasks will accumulate, and in the end I has no choice but to stay up late, which will have a certain impact on my sleep quality.” (Interviewee #5-2025)
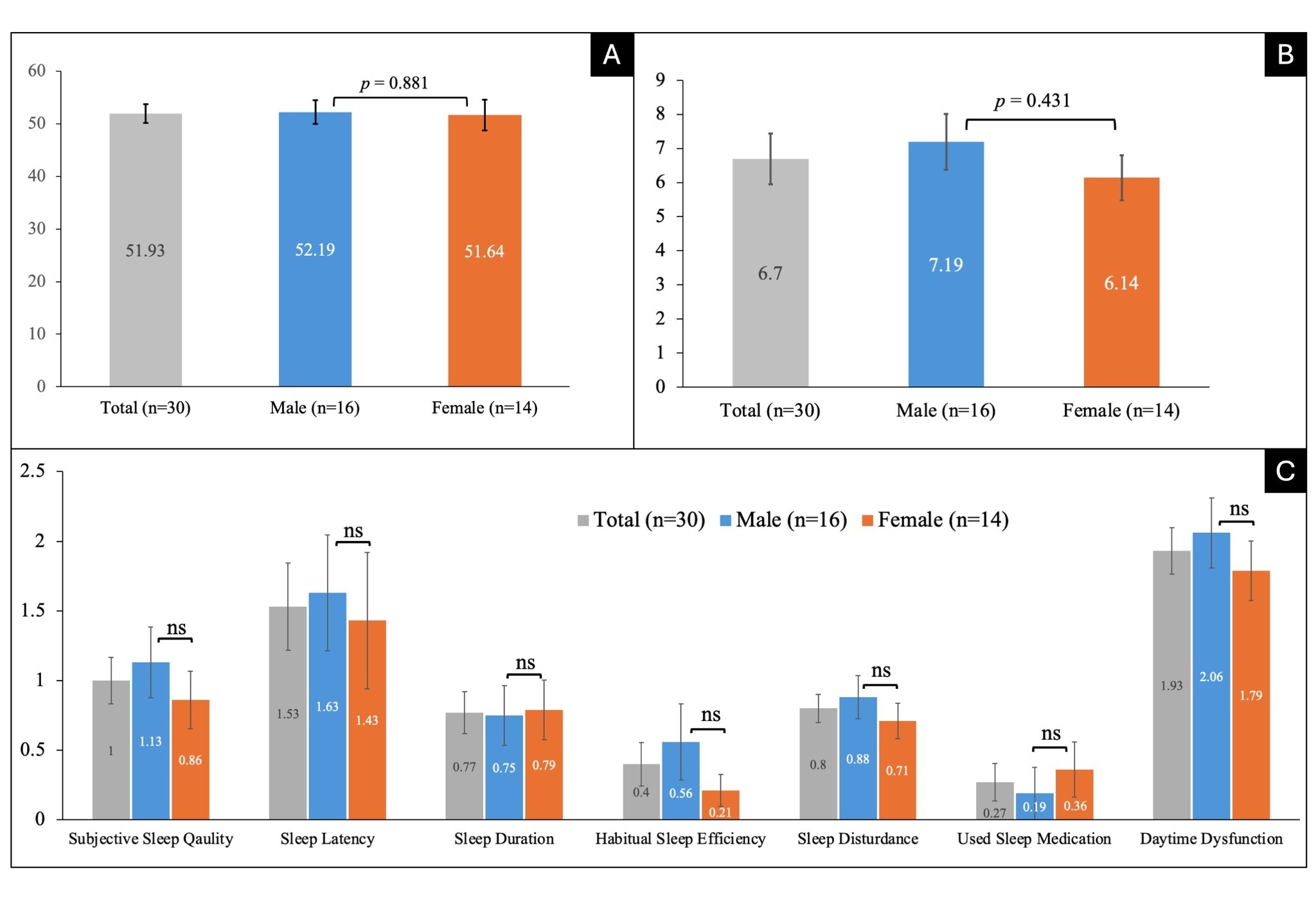
Note: A:mean and standard error of API in total sample and gender difference, B: mean and standard error of PSQI in total sample and gender difference, C: mean and standard of seven components of PSQI in total sample and gender difference; “ns” stand for non-significance, significance level defined as: *p < 0.05, **p < 0.01, ***p < 0.001.
Examining the seven individual dimensions of the PSQI provides a more nuanced picture of the sleep quality present in this sample. Daytime dysfunction was the most prominent concern, recording the highest mean score among all dimensions (M = 1.93, SE = 0.17), which indicate that students frequently experienced difficulties staying awake, maintaining enthusiasm, and functioning effectively during daytime hours. Sleep latency also registered a relatively elevated mean score (M = 1.53, SE = 0.31), which suggest that many students experienced difficulty of falling asleep within a reasonable timeframe. Subjective sleep quality returned a mean of 1.00 (SE = 0.17), which indicate that students generally rated their own sleep as somewhat poor on average.
Across the seven PSQI dimensions, none of the gender differences reached statistical significance (all p > 0.05). For subjective sleep quality, males (M = 1.13) scored slightly higher than females (M = 0.86), but the difference was not significant (t = −0.800, p = 0.431). In sleep latency, males (M = 1.63) reported marginally longer time to fall asleep than females (M = 1.43), yet this difference was also non-significant (t = −0.308, p = 0.761). Sleep duration was nearly identical between males (M = 0.75) and females (M = 0.79), t = 0.117, p = 0.907. For habitual sleep efficiency, males (M = 0.56) showed somewhat higher scores than females (M = 0.21), which suggest lower efficiency among males, but again the difference did not reach significance (t = −1.176, p = 0.253). Sleep disturbance scores were slightly higher for males (M = 0.88) than females (M = 0.71), t = −0.792, p = 0.435. Regarding use of sleep medication, females (M = 0.36) reported slightly more frequent use than males (M = 0.19), but this difference was not statistically significant (t=0.620, p = 0.540). Finally, daytime dysfunction was somewhat higher among males (M = 2.06) compared to females (M = 1.79), yet the difference was not significant (t = −0.829, p = 0.414). In alignment with those quantitative observation, qualitative interview has further observed that smartphone play a role that affect the procrastination, as statement from interviewee find below:
“I actually procrastinate quite frequently, especially with homework assignments that are difficult or unenjoyable. I tend to browse on my phone or do other things first. The primary reason is feeling that the tasks are too numerous or too difficult, leaving me unsure of where to begin.” (Interviewee #1-2025)
“I procrastinate fairly often, particularly when I find the homework boring. I will play games or scroll through Douyin [TikTok] first.” (Interviewee #4-2025)
In summary, the descriptive results indicate that while the level of procrastination was moderate, sleep quality problems were prevalent in this sample, particularly with daytime dysfunction and sleep latency being the most salient sleep concerns. Although small mean differences between male and female students were observed across several sleep-related variables, none of these differences were statistically significant. This suggests that procrastination and sleep quality problems were broadly similar across genders within this sample.
PSQI and API: Correlation Analysis
Table 1 presents the results of the correlation analysis between procrastination scores as measured by the API and overall sleep quality as well as its seven constituent dimensions as assessed by the PSQI. Correlations are reported for the total sample as well as separately for male and female students.
For the total sample, procrastination scores were not significantly correlated with overall PSQI scores (r = 0.298, p = 0.109), which indicate that procrastination tendencies did not demonstrate a statistically significant relationship with overall sleep quality. When examining specific PSQI dimensions, most correlations with API were statistically non-significant. For example, API was not significantly related to subjective sleep quality (r = 0.047, p = 0.807), sleep latency (r = 0.249, p = 0.184), sleep duration (r = 0.258, p = 0.169), habitual sleep efficiency (r = 0.198, p = 0.295), sleep disturbance (r = −0.067, p = 0.726), or daytime dysfunction (r = 0.124, p = 0.513). Use of sleep medication showed a statistically significant positive correlation with API scores (r = 0.390, p <0.05), which indicate that students who reported higher levels of procrastination were more likely to rely on sleep medication. However, this association did not survive Bonferroni Correction (p = 0.033 > adjusted α = 0.006) and should therefore be interpreted cautiously as a trend-level observation. Although the overall frequency of sleep medication use in adolescents is typically low, this finding suggests a potential behavioral link between procrastination and attempts to manage sleep difficulties pharmacologically. In the qualitative interviews, some students reported using melatonin to improve their sleep quality, particularly when facing increasing stress from their academic workload, which support this interpretation.
| Variables | Total (n=30) | Male (n=16) | Female (n=14) | |||
| r | p | r | p | r | p | |
| API Total & PSQI Total | 0.298 | 0.109 | -0.013 | 0.963 | 0.677 | 0.080 |
| API & Subjective sleep quality | 0.047 | 0.807 | -0.053 | 0.844 | 0.167 | 0.567 |
| API & Sleep latency | 0.249 | 0.184 | -0.071 | 0.795 | 0.526 | 0.054 |
| API & Sleep Duration | 0.258 | 0.169 | 0.197 | 0.464 | 0.325 | 0.257 |
| API & Habitual Sleep Efficiency | 0.198 | 0.295 | 0.247 | 0.357 | 0.167 | 0.569 |
| API & Sleep Disturbance | -0.067 | 0.726 | -0.235 | 0.380 | 0.126 | 0.660 |
| API & Used Sleep Medication | 0.390 | 0.033* | 0.054 | 0.843 | 0.727 | 0.003**† |
| API & Daytime Dysfunction | 0.124 | 0.513 | -0.217 | 0.419 | 0.527 | 0.053 |
Note: * p < 0.05 (uncorrected); ** p < 0.01 (uncorrected); † denotes the only result surviving Bonferroni correction at adjusted α = 0.006 (0.05 ÷ 8 comparisons). Bold values indicate the sole statistically robust finding after correction. All p-values are two-tailed.
Gender-stratified analyses revealed some differences. Among male students (n = 16), no statistically significant correlations were observed between API scores and either overall PSQI scores (r = -0.013, p = 0.963) or any of the seven sleep quality dimensions, either before or after Bonferroni correction. Correlation coefficients for males were generally small and in varying directions, with sleep disturbance showing a modest negative association (r = -0.235, p = 0.380) and habitual sleep efficiency showing a modest positive one (r = 0.247, p = 0.357), though neither approached statistical significance. These findings suggest that procrastination may not be a predictor of sleep quality among male secondary students in this sample.
In contrast, the pattern observed among female students (n = 14) was notably different and stronger. While procrastination scores showed a large positive correlation with overall PSQI scores (r = 0.677, p = 0.080), this association did not reach either the uncorrected or Bonferroni-corrected significance threshold and should be regarded as a trend-level finding warranting further investigation. At the dimension level, use of sleep medication show the stronger and only statistically robust association with API scores (r = 0.727, p = 0.003), surviving Bonferroni correction at the adjusted threshold of α = 0.006, which indicate that procrastinating female students were considerably more likely to use medication to manage their sleep difficulties. Additionally, sleep latency (r = 0.526, p =0.054) and daytime dysfunction (r = 0.527, p = 0.053) approached but did not reach the uncorrected 0.05 statistical significance, which suggest a trend whereby higher procrastination may be linked to longer time to fall asleep and greater daytime impairment among female students, though these observations require replication in larger samples before firm conclusions can be drawn.
In sum, following Bonferroni correction for multiple comparisons, only one association survived the adjusted significance threshold — the relationship between procrastination and sleep medication use among female students (r = 0.727, p = 0.003). All other associations, including the trend-level finding between procrastination and overall sleep quality among females (r = 0.677, p = 0.080), did not survive correction and should be interpreted as exploratory observations. Nonetheless, the consistency of the gender-differentiated pattern suggests that the association between procrastination and poor sleep outcomes may be more pronounced among female students than male students, highlighting the importance of gender-sensitive approaches when examining this relationship in adolescent populations.
Discussions
This study examined the relationship between procrastination and sleep quality among Chinese secondary school students using a mixed-method approach combining the API and PSQI with qualitative interviews. Drawing from the research findings, three key aspects offer several implications to existing literature.
First, the descriptive results indicated that students in this sample demonstrated moderate levels of trait procrastination alongside generally poor sleep quality, with a mean PSQI score of 6.70 exceeding the established clinical threshold of 519. This finding is alignment with broader literature documenting the prevalence of sleep difficulties among student populations facing heightened academic demands as well as effects of increasing use of smartphone18,24. Lund et al. similarly found that over 60% of college students aged 17 to 24 were classified as poor-quality sleepers by the PSQI, with students overwhelmingly reporting that emotional and academic stress negatively impacted their sleep25. Daytime dysfunction emerged as the most prominent sleep concern in the present study, with students reporting difficulties maintaining alertness and enthusiasm during the day. This is consistent with evidence that chronic sleep loss and associated daytime impairments in adolescence represent a serious threat to academic success, health, and safety, and constitute an important public health concern6. Students who are unable to maintain alertness and enthusiasm during the day are likely to experience compounding cycles of reduced productivity, increased stress, and further procrastination, as also suggested by Sirois et al.15. Furthermore, research has demonstrated that both daytime and bedtime use of electronic devices among adolescents are associated with shorter sleep duration, longer sleep onset latency, and increased sleep deficiency, with a dose-response relationship observed between device use and risk of very short sleep — a pattern consistent with qualitative interview data in the present study where students reported using Douyin (TikTok) and other social media platforms instead of completing academic tasks18.
Second, following Bonferroni correction for multiple comparisons (adjusted α = 0.006), no associations between trait procrastination and overall sleep quality survived the adjusted significance threshold in the total sample. The previously observed association between procrastination and sleep medication use (r = 0.390, p = 0.033) did not survive correction and should therefore be interpreted as a trend-level observation requiring replication in larger samples. It is important to acknowledge that the construct measured in this study — trait procrastination as assessed by the API — differs from the bedtime procrastination constructs examined by Kroese et al.16 and Ma et al.17. Bedtime procrastination is defined as failing to go to bed at the intended time while no external circumstances prevent a person from doing so11, and represents a situationally specific construct distinct from the dispositional tendency to delay tasks across multiple life domains that trait procrastination captures9. While both constructs share an underlying self-regulatory failure mechanism as theorised within the Procrastination-Health Model15, direct comparisons between the present findings and those of bedtime procrastination studies should be made with caution. The non-significant overall findings in the total sample may therefore partly reflect this construct distinction, in addition to the limited statistical power arising from the small sample size.
Third, the gender-stratified analyses produced interesting findings of the study. While no significant associations were observed among male students, the association between procrastination and sleep medication use among female students (r = 0.727, p = 0.003) survived Bonferroni correction, representing the sole statistically robust finding of this study. Trend-level associations were also observed between procrastination and overall sleep quality (r = 0.677, p = 0.080), for sleep latency (r=0.526, p =0.054) and daytime dysfunction (r=0.527, p = 0.053) among females, though none of these survived the corrected threshold and should be interpreted as exploratory observations. Research suggests that female adolescents engage in more rumination and worry than their male counterparts, and that these cognitive processes are well-established perpetuating features of insomnia, with pubertal maturation being particularly significant for girls in regard to sleep disturbance26. This may partly explain why sleep disturbances among female students appear more strongly linked to psychological stressors such as unfinished academic tasks. The qualitative interview data in the present study lend contextual support to this interpretation, with students reporting that unfinished schoolwork and academic pressure contributed to difficulty disengaging from wakeful activity at night. The qualitative interview data further enriched this interpretation, with students reporting that unfinished schoolwork and academic pressure contributed to their difficulty in disengaging from wakeful activity at night.
Limitations
This study has several limitations. First, as constraints from timing and fundings as well as operational feasibility, this study was based on a relatively small sample (n = 30) drawn from a single high school, which limited both statistical power and sample diversity. While 30-participants meets the minimum threshold for basic statistical analysis, it undermines the power of subgroup analyses and comparisons, where cell sizes become particularly constrained. The homogeneous context further restricts the generalizability of findings to broader Chinese adolescent populations or other cultural settings. Thus, the findings should be interpreted as exploratory rather than definitive. As such, future research should employ larger, multi-school samples to yield more robust and conclusive conclusions. Second, all measures relied on self-report questionnaires. Self-report data may be influenced by social desirability bias, recall bias, or subjective perception differences. The internal consistency of the PSQI in this sample was modest (α = 0.65) fall slightly lower than conventional level 0.70. However, similar reliability estimates have been reported in previous studies using the Chinese version of the PSQI with adolescent samples18, suggesting that this level of reliability is consistent with comparable contexts. Third, the cross-sectional design prevents causal inference. While procrastination may contribute to poor sleep, it is also possible that poor sleep impairs self-regulation and increases procrastination. Longitudinal research is needed to clarify the directionality of effects. Fourth, the study did not account for potentially important confounding variables such as stress levels, mobile phone use, and lifestyle factors, all of which may independently influence both procrastination and sleep quality. Future studies should incorporate these variables, ideally through validated instruments, to better isolate the independent contribution of procrastination to sleep outcome.
Conclusion
This study provides preliminary evidence that procrastination is associated with aspects of poor sleep quality among Chinese secondary school students, with the relationship being particularly pronounced among female students. While there are non-significant association observed in the overall relationship between procrastination and sleep quality, a gender-stratified analysis revealed the significant association between procrastination and sleep medication use among female students. Further, trend-level associations with overall sleep quality, sleep latency, and daytime dysfunction among females suggest a broader pattern warranting further investigation. It is important to note that all findings should be interpreted as associational rather than causal, given the cross-sectional design of the study. The mixed-method design strengthened the robustness of findings by allowing qualitative insights to contextualize and enrich quantitative patterns. These findings underscore the importance of gender-sensitive approaches in both research and school-based interventions targeting adolescent sleep health and procrastination behavior. Given the limitation of a single-school with relatively small sample size, future studies with larger, more representative samples and longitudinal designs are warranted to establish causal pathways and further illuminate the mechanisms through which procrastination shapes sleep outcomes in adolescent populations.
Appendix 1. Final Questionnaire in Chinese and English
亲爱的同学:
您好!感谢您参与本次调查。本问卷旨在了解青少年在日常学习和生活中的时间管理与任务完成情况。您的回答将帮助我们更好地研究这一现象,并探索可能的影响因素。
本问卷为匿名填写,所有数据仅用于学术研究,不会泄露您的个人信息。请根据真实情况和感受作答,没有对错之分,您的诚实回答对研究至关重要。
填答时,请仔细阅读每一道题目,并选择最符合您实际情况的选项。整个问卷预计需要约5-10分钟完成。
祝学习愉快!
问卷一
| 不符合 | 基本不符合 | 不确定 | 基本符合 | 符合 | |
| 1我总是等到最后一刻才开始做事情。 | 1 | 2 | 3 | 4 | 5 |
| 2.我很注意按时归还图书馆的书。 | 1 | 2 | 3 | 4 | 5 |
| 3即便某件事情非做不可,我也不会立即开始做。 | 1 | 2 | 3 | 4 | 5 |
| 4.我总是能按要求的进度完成每天的任务。 | 1 | 2 | 3 | 4 | 5 |
| 5.我很愿意去参加一个关于如何改变拖延行为的研修班。 | 1 | 2 | 3 | 4 | 5 |
| 6.约会和开会时,我常常迟到。 | 1 | 2 | 3 | 4 | 5 |
| 7.我会利用课间的空闲时间来完成晚上要做的事情。 | 1 | 2 | 3 | 4 | 5 |
| 8.做事情时我总是开始得太迟以至于不能按时完成。 | 1 | 2 | 3 | 4 | 5 |
| 9.我常常会在最后期限到来之前拼命的赶任务。 | 1 | 2 | 3 | 4 | 5 |
| 10.我开始做一件事情之前总是要磨蹭很久。 | 1 | 2 | 3 | 4 | 5 |
| 11.当我认为必须做某样工作时,我不会拖延。 | 1 | 2 | 3 | 4 | 5 |
| 12.如果有一个很重要的作业,我会尽可能快的开始。 | 1 | 2 | 3 | 4 | 5 |
| 13.当考试期限逼近时,我常发现自己仍在忙别的事。 | 1 | 2 | 3 | 4 | 5 |
| 14.我总是能按时完成任务。 | 1 | 2 | 3 | 4 | 5 |
| 15.我总是要在最后期限即将来临时才会认真做这件事。 | 1 | 2 | 3 | 4 | 5 |
| 16.当有一个重要约会时,我会提前一天把要穿的衣服准备好。 | 1 | 2 | 3 | 4 | 5 |
| 17.我在参加学校的活动时,一般都到的比较早。 | 1 | 2 | 3 | 4 | 5 |
| 18.我通常能按时上课。 | 1 | 2 | 3 | 4 | 5 |
| 19.我会过高地估计自己在指定时间内完成大量工作的能力。 | 1 | 2 | 3 | 4 | 5 |
问卷二
下面的问题反映您过去一月的睡眠情况,请您选择符合您最
近一个月实际情况的答案。非常感谢!
1.近 1 个月,晚上上床睡觉通常( )点。
2.近 1 个月,从上床到入睡通常需要( )分钟。
3.近 1 个月,通常早上( )点起床。
4.近 1 个月,每夜通常实际睡眠( )小时(不等于卧床时间)。
对下列问题请选择 1 个最适合您的答案。
5.近 1 个月,因下列情况影响睡眠而烦恼:
a.入睡困难(30 分钟内不能入睡)
(1)无 (2)<1 次/周 (3)1-2 次/周 (4)≥3 次/周
b.夜间易醒或早醒
(1)无 (2)<1 次/周 (3)1-2 次/周 (4)≥3 次/周
c.夜间去厕所
(1)无 (2)<1 次/周 (3)1-2 次/周 (4)≥3 次/周
d.:呼吸不畅
(1)无 (2)<1 次/周 (3)1-2 次/周 (4)≥3 次/周
e.咳嗽或鼾声高
(1)无 (2)<1 次/周 (3)1-2 次/周 (4)≥3 次/周
f.感觉冷
(1)无 (2)<1 次/周 (3)1-2 次/周 (4)≥3 次/周
g.感觉热
(1)无 (2)<1 次/周 (3)1-2 次/周 (4)≥3 次/周
h.做噩梦
(1)无 (2)<1 次/周 (3)1-2 次/周 (4)≥3 次/周
i.疼痛不适
(1)无 (2)<1 次/周 (3)1-2 次/周 (4)≥3 次/周
j.其他影响睡眠的事情
(1)无 (2)<1 次/周 (3)1-2 次/周 (4)≥3 次/周
6.近 1 个月,总的来说,您认为自己的睡眠质量
(1)很好 (2)较好 (3)较差 (4)很差
7.近 1 个月,您用药物催眠的情况
(1)无 (2)<1 次/周 (3)1-2 次/周 (4)≥3 次/周
8.近 1 个月,您常感到困倦吗
(1)无 (2)<1 次/周 (3)1-2 次/周 (4)≥3 次/周
9.近 1 个月,您做事情的精力不足吗
(1)没有 (2)偶尔有 (3)有时有 (4)经常有
最后请告诉我您的:
年级___________
年龄___________
生理性别: 男/女
(English Translation)
Hello! Thank you for participating in this survey. This questionnaire aims to understand adolescents’ time management and task completion in their daily study and life. Your responses will help us better study this phenomenon and explore potential influencing factors.
This questionnaire is anonymous. All data will be used solely for academic research and your personal information will not be disclosed. Please answer based on your actual situation and feelings; there are no right or wrong answers. Your honest responses are crucial to this research.
When filling out the questionnaire, please read each question carefully and select the option that best fits your actual situation. The entire questionnaire is expected to take about 5–10 minutes to complete.
Wishing you happy learning!
Questionnaire 1
| Question | disagree | Basically disagree | Not sure | Basically agree | agree |
| I always wait until the last moment to start doing things. | 1 | 2 | 3 | 4 | 5 |
| I pay great attention to returning library books on time. | 1 | 2 | 3 | 4 | 5 |
| Even if something must be done, I won’t start immediately. | 1 | 2 | 3 | 4 | 5 |
| I always complete daily tasks according to the required schedule. | 1 | 2 | 3 | 4 | 5 |
| I am willing to attend a workshop on how to overcome procrastination. | 1 | 2 | 3 | 4 | 5 |
| I am often late for appointments and meetings. | 1 | 2 | 3 | 4 | 5 |
| I use free time between classes to complete tasks for the evening. | 1 | 2 | 3 | 4 | 5 |
| I often start tasks too late, which results in not completing them on time. | 1 | 2 | 3 | 4 | 5 |
| I often rush to complete tasks just before the deadline. | 1 | 2 | 3 | 4 | 5 |
| Before I start doing something, I always need to think about it for a long time. | 1 | 2 | 3 | 4 | 5 |
| When I believe something must be done, I won’t procrastinate. | 1 | 2 | 3 | 4 | 5 |
| If I have an important assignment, I start working on it as early as possible. | 1 | 2 | 3 | 4 | 5 |
| When exam deadlines approach, I often find myself busy with other things. | 1 | 2 | 3 | 4 | 5 |
| I am able to complete tasks on time. | 1 | 2 | 3 | 4 | 5 |
| I always wait until the deadline is near before starting a task. | 1 | 2 | 3 | 4 | 5 |
| If I have an important meeting, I prepare my clothes a day in advance. | 1 | 2 | 3 | 4 | 5 |
| When participating in school activities, I usually arrive early. | 1 | 2 | 3 | 4 | 5 |
| I usually arrive at class on time. | 1 | 2 | 3 | 4 | 5 |
| I am good at estimating how much work I can complete within a given time. | 1 | 2 | 3 | 4 | 5 |
Questionnaire 2
Instructions:
Hello, the following questions reflect your sleep conditions in the past month. Please choose the answer that best matches your actual situation. Thank you!
1. In the past month, at what time do you usually go to bed at night? ( )
2. In the past month, how many minutes does it usually take for you to fall asleep after going to bed? ( )
3. In the past month, at what time do you usually wake up in the morning? ( )
4. In the past month, how many hours of actual sleep do you usually get each night (excluding time in bed)? ( )
For the following questions, please choose the most appropriate answer:
a. Difficulty falling asleep (unable to sleep within 30 minutes)
– (1) Never (2) <1 time/week (3) 1-2 times/week (4) ≥3 times/week
b. Waking up frequently or too early
– (1) Never (2) <1 time/week (3) 1-2 times/week (4) ≥3 times/week
c. Getting up to use the bathroom at night
– (1) Never (2) <1 time/week (3) 1-2 times/week (4) ≥3 times/week
d. Difficulty breathing at night
– (1) Never (2) <1 time/week (3) 1-2 times/week (4) ≥3 times/week
e. Coughing or snoring loudly
– (1) Never (2) <1 time/week (3) 1-2 times/week (4) ≥3 times/week
f. Feeling cold at night
– (1) Never (2) <1 time/week (3) 1-2 times/week (4) ≥3 times/week
g. Feeling hot at night
– (1) Never (2) <1 time/week (3) 1-2 times/week (4) ≥3 times/week
h. Having nightmares
(1) Never (2) <1 time/week (3) 1-2 times/week (4) ≥3 times/week
i. Experiencing pain or discomfort
(1) Never (2) <1 time/week (3) 1-2 times/week (4) ≥3 times/week
j. Other factors affecting sleep
(1) Never (2) <1 time/week (3) 1-2 times/week (4) ≥3 times/week
6. In the past month, how would you rate your overall sleep quality?
(1) Very good (2) Fairly good (3) Fairly poor (4) Very poor
7. In the past month, how often have you used sleeping medication?
(1) Never (2) <1 time/week (3) 1-2 times/week (4) ≥3 times/week
8. In the past month, how often have you felt sleepy during the day?
(1) Never (2) <1 time/week (3) 1-2 times/week (4) ≥3 times/week
9. In the past month, how often have you felt lacking in energy while doing things?
-(1) Never (2) Occasionally (3) Sometimes (4) Often
Appendix 2: Instruction for scoring PSQI and API in both Chinese and English
第一份:PSQI 匹兹堡睡眠质量指数 计分说明(中英对照)
中文计分说明
一、量表概况
匹兹堡睡眠质量指数(PSQI)用于评定受试者近1个月的睡眠质量,共19个自评条目,组合为7个因子维度:主观睡眠质量、入睡潜伏期、睡眠时间、睡眠效率、睡眠障碍、催眠药物、日间功能障碍。
二、计分规则
1. 7个维度每个维度按0–3分计分,总分由7个维度得分相加,总分范围0~21分,分值越高代表睡眠质量越差。
2. 各维度计分方式
- 主观睡眠质量:由第9题直接评分,0、1、2、3分。
- 入睡潜伏期:由第2题+5a题得分合计后换算为0–3分。
- 睡眠时间:由第4题按时长标准赋值0–3分。
- 睡眠效率:由上床时间、起床时间、实际睡眠时间计算睡眠效率,按百分比区间赋值0–3分。
- 睡眠障碍:由5b–5j共9个条目得分累加后换算为0–3分。
- 催眠药物:由第7题直接赋值0–3分。
- 日间功能障碍:由第8题、第9题得分累加后换算为0–3分。
三、结果判定标准
- 0~5分:睡眠质量良好
- 6~10分:睡眠质量一般
- 11~15分:睡眠质量较差
- 16~21分:睡眠质量极差
- 临床临界值:总分>7分 判定存在明显睡眠质量问题
English Scoring Instruction of PSQI
1. General Introduction
The Pittsburgh Sleep Quality Index (PSQI) is used to evaluate sleep quality over the past one month. It consists of 19 self-report items, divided into 7 components: Subjective Sleep Quality, Sleep Latency, Sleep Duration, Sleep Efficiency, Sleep Disturbance, Use of Sleep Medication, Daytime Dysfunction.
2. Scoring Rules
1. Each of the 7 components is scored from 0 to 3 points. The total score is the sum of seven component scores, ranging from 0 to 21. Higher scores indicate poorer sleep quality.
2. Component scoring:
- Subjective Sleep Quality: scored directly by Item 9 (0–3).
- Sleep Latency: sum scores of Item 2 and Item 5a, then converted to 0–3.
- Sleep Duration: scored by Item 4 according to actual sleep hours (0–3).
- Sleep Efficiency: calculated by bedtime, get-up time and actual sleep duration; graded by percentage range (0–3).
- Sleep Disturbance: sum scores of Item 5b–5j, then converted to 0–3.
- Sleep Medication: scored directly by Item 7 (0–3).
- Daytime Dysfunction: sum scores of Item 8 and Item 9, then converted to 0–3.
3. Interpretation Standard
- 0–5: Good sleep quality
- 6–10: Average sleep quality
- 11–15: Poor sleep quality
- 16–21: Very poor sleep quality
- Clinical cutoff: Total score > 7 indicates clinically significant sleep problems.
第二份:api aitken拖延行为量表 计分说明(中英对照)
中文计分说明
一、量表概况
Aitken拖延问卷(API)共19个条目,采用5点李克特计分:1=完全不符合,2=基本不符合,3=不确定,4=基本符合,5=完全符合。为单维度拖延倾向测评量表。
二、反向计分条目
反向题共9题:第2、4、7、11、12、14、16、17、18题
反向计分公式:转换分 = 6 − 原始得分
其余题为正向题,直接采用原始得分。
三、总分计算
将19题所有正向得分与反向转换得分相加,总分范围 19~95分,分数越高代表拖延行为倾向越严重。
四、评分等级划分
- 19–39分:无明显拖延倾向
- 40–59分:轻度拖延
- 60–79分:中度拖延
- 80–95分:重度拖延
English Scoring Instruction of Aitken Procrastination Inventory (API)
1. General Introduction
The Aitken Procrastination Inventory (API) contains 19 items with a 5-point Likert scale: 1=Strongly Disagree, 2=Disagree, 3=Neutral, 4=Agree, 5=Strongly Agree. It is a single-dimension scale for evaluating procrastination tendency.
2. Reverse Scoring Items
Reverse items (9 items): Item 2,4,7,11,12,14,16,17,18
Reverse scoring formula: Converted score = 6 − Original score
All other items are positive-scored and use original scores directly.
3. Total Score Calculation
Sum all original positive scores and converted reverse scores.
Total score range: 19-95. Higher scores mean more severe procrastination tendency.
4. Grade Interpretation
- 19–39: No obvious procrastination
- 40–59: Mild procrastination
- 60–79: Moderate procrastination
- 80–95: Severe procrastination
References
- H. R. Colten, B. M. Altevogt, edited. Sleep Disorders and Sleep Deprivation: An Unmet Public Health Problem. Washington. DC: National Academies Press (US). 2006, https://doi.org/10.17226/11617 [↩] [↩]
- N. F. Watson, M. S. Badr, G. Belenky, D. L. Bliwise, O. M. Buxton, E. Tasali. Joint consensus statement of the American Academy of Sleep Medicine and Sleep Research Society on the recommended amount of sleep for a healthy adult: methodology and discussion. Journal of Clinical Sleep Medicine, Vol. 11, pg. 931-952, 2015, https://doi.org/10.5664/jcsm.4950 [↩]
- N. Truong, H. Nguyen, T. Pham, D. Chu, L. Bui. Sleep quality by clinical training status among medical students and its associated factors: a cross-sectional study in Da Nang, Vietnam. Scientific Reports, Vol. 15, pg. 33671, 2025, https://doi.org/10.1038/s41598-025-18256-8 [↩]
- J. Vanderlinden, F. Boen, J. G. Z. van Uffelen. Effects of physical activity programs on sleep outcomes in older adults: a systematic review. International Journal of Behavioral Nutrition and Physical Activity, Vol. 17, pg. 11, 2020, https://doi.org/10.1186/s12966-020-0913-3 [↩]
- P. Kavousi, E. Mali, N. Seifhashemi, M. Souri, L. Pakravan, F. Khalili. Worldwide prevalence of poor sleep quality in older adults: a systematic review and meta-analysis. Iranian Journal of Psychiatry, Vol. 20, pg. 265, 2025, https://doi.org/10.18502/ijps.v20i2.18207 [↩]
- J. Owens, Adolescent Sleep Working Group, Committee on Adolescence. Insufficient sleep in adolescents and young adults: An update on causes and consequences. Pediatrics, Vol. 134, pg. e921-e932, 2014, https://doi.org/10.1542/peds.2014-1696 [↩] [↩] [↩]
- L. Tarokh, J. M. Saletin, M. A. Carskadon. Sleep in adolescence: Physiology, cognition and mental health. Neuroscience and Biobehavioral Reviews, Vol. 70, pg. 182-188, 2016, https://doi.org/10.1016/j.neubiorev.2016.08.008 [↩] [↩]
- S. Dobing, N. Frolova, F. McAlister, J. Ringrose. Sleep quality and factors influencing self-reported sleep duration and quality in the general internal medicine inpatient population. PloS One, Vol. 11, pg. e0156735, 2016, https://doi.org/10.1371/journal.pone.0156735 [↩]
- P. Steel. The nature of procrastination: A meta-analytic and theoretical review of quintessential self-regulatory failure. Psychological Bulletin, Vol. 133, pg. 65-94, 2007, https://doi.org/10.1037/0033-2909.133.1.65 [↩] [↩] [↩] [↩] [↩]
- M. M. Clegg-Kraynok, A. L. McBean, H. E. Montgomery-Downs. Sleep quality and characteristics of college students who use prescription psychostimulants nonmedically. Sleep Medicine, Vol. 12, pg. 598-602, 2011, https://doi.org/10.1016/j.sleep.2011.01.012 [↩]
- F. M. Kroese, D. T. D. De Ridder, C. Evers, M. A. Adriaanse. Bedtime procrastination: Introducing a new area of procrastination. Frontiers in Psychology, Vol. 5, Article 611, 2014, https://doi.org/10.3389/fpsyg.2014.00611 [↩] [↩] [↩]
- P. Steel, D. Taras, A. Ponak, J. Kammeyer-Mueller. Self-regulation of slippery deadlines: the role of procrastination in work performance. Frontiers in Psychology, Vol. 12, pg. 783789, 2022, https://doi.org/10.3389/fpsyg.2021.783789 [↩]
- M. E. Aitken. A personality profile of the college student procrastinator. PhD Dissertations, Pittsburgh: University of Pittsburgh. 1982. [↩] [↩] [↩]
- X. L. Chen, X. Y. Dai, Q. Dong. Research on the application of the Aitken Procrastination Inventory among college students. Chinese Journal of Clinical Psychology, Vol. 76, pg. 22-23, 2008, https://doi.org/10.16128/j.cnki.1005-3611.2008.01.009 [↩] [↩] [↩]
- F. M. Sirois, W. van Eerde, M. I. Argiropoulou. Is procrastination related to sleep quality? Testing an application of the procrastination-health model. Cogent Psychology, Vol. 2, pg. 1074776, 2015, https://doi.org/10.1080/23311908.2015.1074776 [↩] [↩] [↩] [↩]
- F. M. Kroese, C. Evers, M. A. Adriaanse, D. T. de Ridder. Bedtime procrastination: a self-regulation perspective on sleep insufficiency in the general population. Journal of Health Psychology, Vol. 21, pg. 853-862, 2016, https://doi.org/10.1177/1359105314540014 [↩] [↩]
- X. Ma, D. Meng, L. Zhu, H. Xu, J. Guo, L. Yang, L. Yu, Y. Fu, L. Mu. Bedtime procrastination predicts the prevalence and severity of poor sleep quality of Chinese undergraduate students. Journal of American College Health, Vol. 70, pg. 1104-1111, 2022, https://doi.org/10.1080/07448481.2020.1785474 [↩] [↩] [↩]
- M. Hysing, S. Pallesen, K. M. Stormark, R. Jakobsen, A. J. Lundervold, B. Sivertsen. Sleep and use of electronic devices in adolescence: Results from a large population-based study. BMJ Open, Vol. 5, e006748, 2015, https://doi.org/10.1136/bmjopen-2014-006748 [↩] [↩] [↩] [↩]
- D. J. Buysse, C. F. Reynolds III, T. H. Monk, S. R. Berman, D. J. Kupfer. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Research, Vol. 28, pg. 193-213, 1989, https://doi.org/10.1016/0165-1781(89)90047-4 [↩] [↩] [↩]
- X. C. Liu, M. Q. Tang, L. Hu, A. Wang, H. Wu, G. Zhao, C. Gao, W. Li. Reliability and validity of the Pittsburgh Sleep Quality Index. Chinese Journal of Psychiatry, Vol. 2, pg. 103-107, 1996. [↩] [↩]
- S. Nauts, B. A. Kamphorst, W. Stut, D. T. De Ridder, J. H. Anderson. The explanations people give for going to bed late: a qualitative study of the varieties of bedtime procrastination. Behavioral Sleep Medicine, Vol. 17, pg. 753-762, 2019, https://doi.org/10.1080/15402002.2018.1491850 [↩]
- K. B. Wright. Researching internet-based populations: Advantages and disadvantages of online survey research, online questionnaire authoring software packages, and web survey services. Journal of Computer-Mediated Communication, Vol. 10, pg. JCMC1034, 2005, https://doi.org/10.1111/j.1083-6101.2005.tb00259.x [↩]
- S. K. Ahmed. Sample size for saturation in qualitative research: Debates, definitions, and strategies. Journal of Medicine, Surgery, and Public Health, Vol. 5, pg. 100171, 2025, https://doi.org/10.1016/j.glmedi.2024.100171 [↩]
- A. U. Agu, E. A. Esom, S. C. Chime, P. S. Anyaeji, G. E. Anyanwu, E. N. Obikili. Impact of sleep patterns on the academic performance of medical students of College of Medicine, University of Nigeria. International Journal of Medicine and Health Development, Vol. 26, pg. 31-36, 2021, https://doi.org/10.4103/ijmh.IJMH_32_20 [↩]
- H. G. Lund, B. D. Reider, A. B. Whiting, J. R. Prichard. Sleep patterns and predictors of disturbed sleep in a large population of college students. Journal of Adolescent Health, Vol. 46, pg. 124-132, 2010, https://doi.org/10.1016/j.jadohealth.2009.06.016 [↩]
- S. H. Li, A. Werner-Seidler. Gender differences in adolescent sleep disturbance and treatment response to smartphone app-delivered cognitive behavioral therapy for insomnia: exploratory study. JMIR Formative Research, Vol. 5, pg. e22498, 2021, https://doi.org/10.2196/22498 [↩]


and Physical and Mental State for Healthy Youth")
{kind=link}