
Abstract
In many rural areas of the United States of America, patients are less likely to have any health insurance. Although this is a problem nationwide, the poverty rate in rural states is substantial. Rural states such as Vermont and North Dakota make it unmanageable for residents to find employment, achieve financial stability, and access transportation. In these regions across the U.S., access to affordable cancer treatment and medication is a major concern. Healthcare is crucial in all aspects for people across the country, but in certain parts of the US, like Vermont, North Dakota, and more, the lack of healthcare professionals, especially for cancer, is significant. Furthermore, the hospitals in these areas are outdated, and the healthcare infrastructure is limited. As a result, even if a particular treatment could help a patient, limited access can cause complications. Transportation is another major challenge, as many families can’t afford cars or live in an isolated area. This, in turn, makes getting screened for cancer quite rare and contributes to the high death rates. This study uses the Social Determinants of Health (SDOH) framework to examine socioeconomic, geographic, and other limitations that influence access to cancer care in rural and low-income areas in the U.S. Findings from the study highlight that rural patients are less likely to be insured, have financial strains due to the high cost of treatment, and have higher mortality rates compared to urban patients. New policies and government support can close the gap between patients and their healthcare. Structural barriers to access to cancer treatments and medications are the geographic, financial, and socioeconomic limitations that prevent equal cancer care. Health inequality refers to differences in health outcomes between urban and rural populations, driven by the barriers outlined in this article.
Introduction
Cancer remains one of the leading causes of mortality in the U.S., but there is still an unequal distribution of access to cancer treatments and medications in rural and low-income areas. Rural areas have limited access to healthcare due to geographic isolation, transportation limitations, financial barriers, and socioeconomic factors.
Research from the National Institutes of Health (NIH) displays that millions of rural cancer survivors have limited access to healthcare compared to their urban counterparts1. In addition to these barriers, poverty intensifies these disparities. Shortages of oncology specialists and limited public transportation contribute to delays in patient treatment and screening.
In this review, access refers to patients’ ability to obtain cancer care in their community. Previous studies have addressed these disparities individually, but there has been a lack of a systematic synthesis of these barriers using the Social Determinants of Health framework, which addresses the socioeconomic, geographic, and healthcare limitations that exist. The Social Determinants of Health framework analyzes how these barriers can overlap, causing their spread and influence to severely impact survival outcomes. This study is a narrative literature review that uses multiple peer-reviewed sources, reports, and data published between 2010 and 2025.
Literature Review
Cancer disparities between rural and urban populations are becoming increasingly prevalent. Existing research and literature demonstrate how patients living in low-income areas experience higher mortality, lower screening rates, delayed diagnoses due to lack of transportation and distance between hospitals, and have limited access to oncologists. Structural barriers, such as geographic isolation, transportation limitations, a limited number of oncologists, and a higher financial burden, are attributed to these disparities.
Many studies have displayed that the lack of hospital services in these areas greatly shapes cancer outcomes. For instance, Moscovice et al. found that rural hospitals greatly lack sufficient oncology specialists, which forces patients to travel large distances for treatments2. In addition, Hung et al. find that CAH or Critical Access Hospitals were substantially less able to provide oncology services like chemotherapy and radiation therapy compared to their urban counterparts3.
Financial barriers are also a major determinant of disparities in rural areas. Zahnd et al. add that rural cancer survivors report higher financial instability and problems compared to urban survivors4. Additionally, research from the American Cancer Society (ACS) displays that uninsured cancer patients often go through food insecurity, debt, and reduced medicine intake to reduce financial burden. This illustrates how financial instability influences the ability to access cancer treatments and survival outcomes.
Beyond these barriers, researchers are increasingly using the Social Determinants of Health framework to examine these disparities. For instance, social determinants like income, education, employment, transportation, and insurance can hinder access to cancer medication and treatments for lower-income patients. This is seen in the research done by Chu et al. where he discovers how rural patients with pancreatic adenocarcinoma had higher mortality rates compared to urban patients, displaying how socioeconomic disparities influence survival outcomes greatly5.
Although prior research has identified and examined individual barriers to cancer care in these low-income areas, few studies have systematically analyzed these determinants. There is very little research, especially on how geographic isolation, transportation limitations, financial instability, healthcare shortages, and social and socioeconomic determinants collectively reproduce inequalities between rural communities. This literature review aims to analyze this further by seeing how these barriers and determinants contribute to unequal access of cancer treatments and medications in the United States.
Methodology
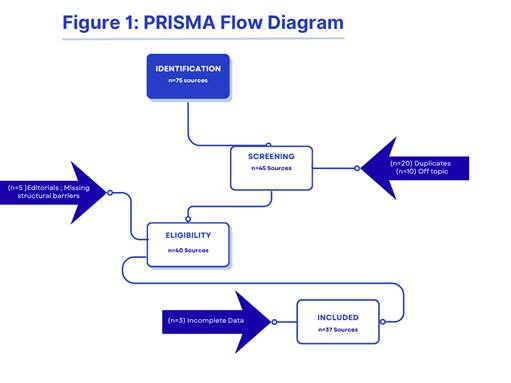
This study follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines to analyze and identify peer-reviewed literature examining disparities in access to cancer care between rural and urban populations in the U.S.
To investigate access to cancer medications for patients in rural areas, a comprehensive body of research was conducted. This review includes many peer-reviewed articles from PubMed, NIH publications, and the American Cancer Society. A total of 75 sources were initially identified through research. The articles included in this review were published from 2010 to 2025. It focuses on rural communities in the U.S. and provides findings relating to the geographic, financial, and socioeconomic barriers to cancer care. Of the n=75 sources identified, n=30 were removed as duplicates or off-topic. On top of that, n=5 sources were excluded during the eligibility stage because they were editorials or lacked structural barriers.
The studies were included if they were peer-reviewed and focused on the barriers affecting the outcomes of the rural population. In addition, they were included especially if they had quantitative data about one of the barriers/determinants, including insurance status, geographic isolation, socioeconomic limitations, etc. Studies were especially excluded if they were editorials, opinion-directed, or didn’t focus on one of the specific barriers.
A total of 37 articles were analyzed for this review. The data supported multiple topics, including insurance coverage, hospital limitations, transportation difficulties, and other barriers. Findings were organized into geographic, financial, institutional, and socioeconomic sections. This review aimed to incorporate all evidence addressing the factors in rural care.
Databases used included PubMed, NIH, Google Scholar, and more. Keywords used for research were “rural cancer disparities,” “geographic location to healthcare,” “financial status,” “telemedicine,” and “Social Determinants of Health.”
Data taken from every study included author information, publication details, population data, cancer type, geographical area, and outcomes related to access to treatment. Due to the diverse number of sources, this review was conducted as a narrative synthesis that identified patterns across studies.
In addition, the Social Determinants Framework of Health was consistently used throughout the review to analyze and interpret findings. The framework identifies the different topics into an organized outlook that includes financial instability, healthcare access, geographic location, and socioeconomic and social determinants that influence disparities between rural and urban areas.
Geographic Location and Screening
In rural, low-income areas, millions of people live in geographically isolated communities. This causes barriers in receiving treatments and medications, and creates difficulties for patients trying to find adequate resources to protect themselves from dangerous diseases such as cancer.
Many patients don’t comprehend that screening for cancer and going to get checked by a doctor are important for themselves and their families. Many families face the challenge of being unaware of healthcare resources and ways to protect themselves.
According to a study by the National Institutes of Health (NIH), many individuals cannot afford cancer screening due to financial constraints1. In fact, “Over half (50.5%) of rural cancer survivors reported financial problems due to cancer compared to 38.8% of urban survivors (p = 0.02)”.
Geographic location also plays a significant role in cancer screening. Rural patients often face transportation issues and must travel long distances to hospitals. The Division of Cancer Control and Population Sciences (DCCBS), a part of the National Cancer Institute, reports that “transportation challenges, fewer healthcare facilities, and financial obstacles (e.g., insufficient insurance coverage), contribute significantly to these higher incidence and mortality rates”6. In fact, only 7.4% of medical oncologists and 8.5% of radiation oncologists practice in these remote areas in 20197. For rural patients, this can cause adverse outcomes. If only a total of 15.9% of the population practices oncology, it indicates that many residents experience limited access to cancer care.
According to the National Institutes of Health (NIH), about 14% of the population lives more than 180 minutes away from satellite facilities of the National Cancer Institute (NCI)8. Consequently, during an emergency, patients have difficulty getting to hospitals in time to save their loved ones.
Not only are utilities far from homes, but 6.8% of households do not own any vehicle9. This causes problems, especially during emergencies. Residents must find reliable transportation, yet in states like Louisiana, Kentucky, North Dakota, and South Dakota, among others, funding shortages are a significant issue. Public transportation is very limited in these areas. For instance, a study from the NIH states that, “Despite their lack of access to a car, a significantly smaller proportion of rural carless residents bike, walk, or take transit for work trips than their nonrural peers (38.9% vs. 74.6%), which may indicate infeasibility of sustainable modes in some rural areas”9. This reveals the limited transportation options in rural communities.
Overall, these geographic location disparities should be addressed. The lack of transportation can limit individuals’ access to cancer screening. Many families have to travel long distances to reach oncology centers and screening facilities2.
These barriers reduce the chance of early detection and are associated with poorer outcomes. Reinforcing these inequalities through government policies can bring positive changes. According to the SDOH framework, geographic location can be a structural determinant of healthcare access, preventive cancer services, and survival outcomes. Due to limited healthcare infrastructure and unequal access, the disparities between rural and urban populations are reinforced.
Limitations in Rural Hospitals
In the US, healthcare is essential, and you would expect hospitals to be equipped with the latest treatments and medications. However, in these outlying regions, many hospitals have been found to have “lower rates of comprehensive oncology care,” according to the American Hospital annual survey from the NIH10.
The CAH, or Critical Access Hospital, was established in 1997 to improve access to healthcare. CAH hospitals are often small healthcare facilities that include only 25 beds11. CAHs are reimbursed by Medicare based on a cost basis for patients. As these hospitals primarily operate in rural areas, uninsured and other insured individuals have to go to other hospitals that charge higher prices for the same treatments. It has been found that in these hospitals, cancer care professionals have limited delivery models for treatments. This is concerning, as this is the only treatment option for some patients. For instance, in a study of 135 CAHs, 95% offered at least one cancer screening service, while only 46% reported providing specific treatments such as chemotherapy, radiation, or surgery2. In fact, only 30% of CAHs offered chemotherapy and 2.9% offered radiation therapy compared to 64.4% and 43.8% in urban hospitals, respectively3. In addition, only 34% of respondents reported that a local oncologist at a CAH hospital helped them, and 28% reported involvement of a non-local oncologist using telemedicine2. This highlights that oncologists are only involved to the extent of one-third in these hospitals. This shows the growing disparity between urban and rural areas.
One more understanding of this problem is demonstrated by Liu et al., who find that the closure of rural hospitals decreases survival12. With a new structural barrier in place, patient outcomes worsen. Specifically, survival among patients with colorectal and lung cancer decreases, and mortality rates increase up to 5 years after.
Together, these studies demonstrate how individuals in rural areas have limited access to oncology treatment services and are likely to have less comprehensive cancer care. This is a huge barrier for cancer patients in rural areas. Patients in rural communities should have the same treatment options as those in urban areas. Closure of hospitals can significantly increase mortality rates in these areas as well. One way to get healthcare workers into rural areas is to add incentive programs. These programs will benefit both patients and workers.
Insurance Coverage, Financial Toxicity, and Economic Barriers
Throughout the US, many households struggle to afford healthcare. In non-urban and low-income areas, the lack of insurance can lead to large medical bills for families. According to the American Cancer Society, 23% of people with a cancer history live in rural areas; there is a significant need for better healthcare13.
Healthcare insurance often comes with high out-of-pocket costs and deductibles. However, low family incomes make it challenging to obtain insurance, especially when individuals are working two or three jobs just to survive. The lack of health insurance contributes to the high prices for cancer treatments like chemotherapy, immunotherapy, and surgery. The National Institutes of Health (NIH) has done previous research and found that 2.8 million rural cancer survivors live in the US. Rural survivors were more likely than urban survivors to lack health insurance14. This is a tremendous problem affecting a substantial number of individuals.
In an individual case, the American Cancer Society13 shows Sarah Graves, a woman from South Dakota, who was diagnosed with chronic myeloid leukemia. As she did not have insurance, her initial medical bills rose to over $70,000, which affected her and her household tremendously. When she required a bone marrow transplant, she had to pay approximately $1,000,000. Her experience highlights the substantial financial burden rural residents go through for cancer care. These financial barriers contribute to the disparity between urban and rural residents and are highly prevalent. High cancer treatment costs cause many families to be unable to afford them, especially in rural areas like South Dakota.
For example, according to the ACS, 17.4% of individuals in rural areas have reported skipping, taking less, and delaying medications due to cost in the past 12 months13. Therefore, this significantly impacts the survival and the quality of life for those patients. Additionally, the ACS found that 26.2% reported experiencing difficulties paying medical bills in the past 12 months13. Given the high number of individuals facing financial difficulties highlighted by these studies, targeted policy interventions are needed to address this issue.
Not only does the high cost of healthcare cause financial problems, but there are reports that 43% experienced food insecurity13. The coverage gaps are an enormous issue. In fact, according to Figure 2 from the Centers for Disease Control and Prevention (CDC), 57.9% of cancer survivors have private insurance. Therefore, many have to rely on insurance companies that demand exorbitant amounts of money. Only 20.3% of cancer survivors have Medicaid, which is insufficient, as that demonstrates most have to use private companies to get insured. In addition, 14% of cancer survivors were uninsured, which shows how expensive healthcare is.
Beyond hospital limitations, the insurance instability further widens the disparity in access to cancer treatment. PPS, or a Prospective Payment System hospital, is a government hospital under Medicare and Medicaid11. In these hospitals, a fixed rate is used for each service rather than the actual cost. Although this helps, it does not cover all insurance, such as CAH hospitals. Still, there is hope, as some individuals with cancer can be covered with Medicaid if they meet certain conditions. Medicaid provides free and low-cost insurance coverage to people with low income or disabilities. Each state has different eligibility guidelines. However, this helps many patients obtain insurance and afford treatment15.
Figure 2 shows that only 20.3% of cancer survivors had Medicaid. Although there are some initiatives to help rural patients, they often struggle to afford the medications and treatments they need.
In addition, financial toxicity and instability are highly prevalent in rural areas. According to a study by Odahowski et al., in which 1419 rural and 1144 urban cancer survivors were surveyed, more rural cancer survivors reported financial hardship (rural: 23.9% vs. urban: 17.1%)16. Although the numerical difference appears moderate, the findings reveal substantial disparities between urban and rural populations. Deshmukh et al. add to this idea by conducting a study with 26 rural participants, of whom 42 percent were low-income, and 50 percent had high school or less education17. The results showed high comprehensive financial toxicity (14.0; range 0-38). A score of 14.0 for financial toxicity is pretty high and shows the instability experienced by rural cancer patients. This is also illustrated by Xu et al.’s study, which finds that “Rural patients younger than 50 years showed a statistically higher FT than urban patients…18”. These findings demonstrate that there is a difference in financial toxicity between urban and rural populations, leading to greater economic instability in rural areas.
Cancer care causes a huge economic burden throughout the U.S., with patients spending $21 billion in 2019 on cancer treatment and care costs5.
As income levels in rural areas are low and employment insurance is less available, gaps in insurance coverage can financially burden families. Many patients, as seen by Planey et al., report doing “…cost-coping strategies to reduce travel-associated costs, such as “stacking” appointments to reduce travel cost19”. These choices demonstrate the lack of government support in rural areas. Clearly, more government policies should be added to benefit families undergoing these difficulties. In addition, jobs should start accommodating insurance policies to reduce financial burden.
Using the SDOH framework, it is seen that insurance instability and financial toxicity can be understood as structural determinants and barriers that reduce access to cancer care in rural communities. Due to economic instability, limited employer insurance, and dependence on under-resourced healthcare systems, there is restricted access to cancer treatments. Furthermore, financial hardship overlaps with geographic isolation, intensifying healthcare disparities in rural areas. Abdullah et al. propose expanding Medicaid, increasing telemedicine and transportation, and increasing the use of SDOH in the screening and treatment of cancer patients20. This can be an important step to overcoming the gap between urban and rural areas of the U.S.
Telemedicine
Telemedicine is the use of virtual technology, such as video calls and audio, to access healthcare. After COVID-19, its use has increased to reduce barriers for cancer patients. However, evidence shows that its adoption and effective use are limited, displaying disparities in access to cancer care.
According to a study done by PubMed, “Telemedicine usage varied across rural areas, with 41.4% of rural cancer survivors using telemedicine compared with 57.5% of cancer survivors in large metropolitan areas (p < 0.001)21”. This shows that although telemedicine is widely used in rural areas, its use remains deficient. In addition to this, the study also highlights that cancer survivors were “0.56 times less likely” to use telemedicine compared to their urban counterparts with “0.69 times21”. This suggests that structural barriers may also limit digital healthcare access. Johannes et al. add on this showing that, “…rurality is associated with lower rates and lower odds of telehealth compared to urban older adults22”. This demonstrates that telemedicine is used less in rural areas than in urban areas.
Similarly, Curtis et al. find that oncology telemedicine during COVID was “…lower in the proportion of outpatient visits performed via telehealth23”. Specifically, only 11% of oncology outpatient visits were conducted via telemedicine, compared with in-person clinic visits. This underuse of telemedicine shows the limitations of cancer care in resource-constrained rural settings.
Holtz et al. expand on the limitations of telehealth in their study, showing that cancer peer support groups in rural areas increased survival. Although there was satisfaction with telehealth, many reported that there was “…[a] lack of interpersonal connection, internet access, and technical difficulties24”. This shows that although telehealth helps patients in rural areas, its availability and efficiency are limited. While telemedicine is effective when used, limited access to it is due to technological and infrastructural barriers. In addition to this, Ma et al. conducts a study and results show that, “Compared with in-person visits, telemedicine was felt to be inferior in establishing a personal connection during consultation (90%) and assessing for toxicity while on-treatment (88%) and during follow-up (70%)25”. This supports that although telemedicine is a possible solution in solving the disparities between rural and urban areas, there is less “personal connection” during consultation and less assessing for toxicity. This can be fatal especially as cancer patients require support and effective care. This might be a vital reason backed by Mackwood et al. that “In 2020, compared with patients residing in metropolitan areas, small town/rural-residing patients were less likely to use telemedicine (1.28 visits v 2.34)26”. Overall, although telemedicine is a viable option, limited interaction with it due to technological disadvantages, infrastructural barriers, and less connection with consultants is leading to its downfall in rural areas.
Another important factor influencing telemedicine is the presence of adverse SDOH. A study by Alcaraz et al. found that patients with fewer than one adverse SDOH were more likely to use telehealth. However, it was also discovered that patients with more than one adverse SDOH were not associated with telehealth use27.This suggests how telemedicine can improve access to healthcare, but overlapping barriers can prevent patients from benefiting from its use.
Through the Social Determinants of Health framework, telemedicine disparities reflect the broader structural barriers to access to technology and healthcare infrastructure. Although it has started to increase access to oncologists and cancer treatments, without technological readiness, it is not efficient for every rural resident. As a result, rural cancer patients are disadvantaged even with telemedicine. Although telemedicine is a valuable solution, it is not sufficient for addressing the cancer care disparities in these low-income areas without investments in digital infrastructure and equal access to technology.
Social Determinants
Although it is often overlooked, some patients are more likely to die because of their social determinants, including age, sex, race, education, and socioeconomic class28.
From a study done by the NIH (Social determinants of health associated with poor outcome for rural patients following resected pancreatic cancer), where white and black rural and urban patients underwent treatment for pancreatic adenocarcinoma, professionals found that patients that had an annual income of <$48,000 had a 16 to 23% higher chance of dying compared to patients who had an annual income of ≥$63,0005. Also, patients who had a lower educational attainment had a 9 to 21% higher risk of mortality. This disparity happened, according to the article, because “rural patients tend to be poorer, less likely to attain higher levels of education, more underinsured, more likely to be treated at a community cancer program, and more likely to travel a long distance for their care5”.
Patients in these regions have many disparities compared to urban patients29. As cancer is an unaffordable, disadvantageous, and highly deadly disease, it can be challenging for rural cancer patients to survive. For instance, a case study about cancer in rural America concludes that in non-urban areas, there is a cancer mortality rate of 240.3 per 100,000 for males compared to 217.6 per 100,000 in large metropolitan areas29.
Every year, the cancer mortality gap between remote and metropolitan patients is growing, causing issues for so many families around the nation28. Results from Shen et al., who performed research in rural communities about access to cancer care for prostate cancer patients, show that rural patients were treated differently. He discovers that rural patients were treated differently. They were less likely (40.8% vs 47.6%) to have multidisciplinary consultants. In addition, it was found that rural patients had less surveillance and observation (22.6% vs 28.7%)30.This demonstrates a significant difference in the treatment of rural patients.
Beyond geographic location, insurance, and limits in hospitals, social determinants play a critical role in access to affordable cancer treatment and medications in rural areas. Socioeconomic determinants such as net income can determine the cancer outcome for many patients. These differences should be addressed to fit society’s needs. The American Society of Clinical Oncology emphasizes the importance of the use of SDOH (social determinants of health) in cancer care by advancing scientific knowledge, improving patient outcomes, and articulating their use in clinical practice31.
Cancer-Specific Disparities in Rural Populations
Regarding the access to cancer care in rural states such as Kansas and Vermont32, there aren’t uniform disparities across all cancer types. The existing literature suggests that differences in cancer treatment across cancer types in screening and treatment outcomes are structurally influenced.
For instance, Hashtarkhani et al. highlight that for breast cancer, screening rates were lower in the central and midwestern regions of the U.S. compared to the eastern and northern parts33. These findings indicate that breast cancer screening is influenced by geographic and structural determinants of health.
Similarly, Ose et al. at the University of Utah Huntsman Cancer Institute found significant differences in patient-reported outcomes. The study highlights disparities in fatigue and physical function between different cancer types. The study also reports specific differences (eg, depression, fatigue, pain interference, and physical function) in oral cavity and pharynx cancer, colorectal cancer, and uterine cancer34. These differences between cancer types go beyond geographical location, insurance type, and financial toxicity, showing the disparities between different cancer types. These findings show cancer types are associated with distinct symptoms affecting quality of life outcomes.
Specifically, non-small-cell lung cancer has higher mortality rates in rural areas. Atkins et al. find that rural patients with stage I non-small cell lung cancer had shorter survival. This indicates disparity in access to surgical care35. This can be fatal, especially in low-income areas, and displays a lack of healthcare. Logan et al. also find increased mortality rates for patients with non-small-cell lung cancer, especially those who were surgically treated36. Using the National Cancer Database, they find that through 366,373 surgical patients in rural towns, survival outcomes were worse at 1 year (85% vs. 87%), 5 years (48% vs. 54%), and 10 years (26% vs. 31%)36. This shows that there is an increased risk for death in rural areas, specifically non-small-cell lung cancer that was treated surgically.
Thompson et al. add on to this argument, finding cancer disparities based on the type in rural Kansas and Missouri. He finds, “..rural residence is not a simple risk factor but rather appears to play a complex role in cancer outcome disparities. Specifically, rural residence is associated with higher stage at diagnosis and increased survival hazards for colon cancer but decreased risk for lung cancer compared to urban residenc37”.This shows that there are specific disparities in cancer types between rural and urban areas.
Another perspective on this problem is in a study done by Liu et al., where they discovered, “rural hospital closures are significantly associated with worse survival among patients with colorectal and lung cancer, but not among those with breast or prostate cancer12”. This directly shows how different cancers respond differently to the same barrier.
Overall, these studies emphasize that cancer disparities in rural populations vary by cancer type, which can reflect the differences in screening, treatment, and access to oncology care. Through the Social Determinants of Health framework, these differences show how structural factors like healthcare, socioeconomic conditions, and access interact differently depending on the cancer type, which ultimately shapes survival outcomes.
Conclusion
Overall, this review highlights the financial and physical challenges rural patients face in accessing treatment and medications. Many patients were reported to use less medication than prescribed, simply to lower costs. Patients were worried that they would burden their families and make their lives demanding for them, and they avoided cancer screenings. Others did not recognize the risks and symptoms of different cancers13.
Rural patients are often uninsured because either their job does not provide insurance (similar to the case of Sarah Graves) or many families cannot afford insurance. Another issue is transportation, as patients have to drive long distances to reach a clinic, and some families do not have a vehicle. Even going to a hospital means high costs for families, causing problems with access to treatment. In addition, hospitals are outdated and do not offer the latest treatments and medications, creating significant disparities for urban patients.
This study has many limitations that should be acknowledged. The data collected from the studies were limited to a few rural states, potentially leaving gaps in knowledge across other rural areas. Additionally, the study includes data from self-reported rural patients, which may introduce bias. Despite these limitations, this study examines the structural, geographic, and economic barriers to accessing affordable cancer treatments and medications in low-income areas. For future research, studies should provide a broader view, include more rural regions, and evaluate data more effectively.
Future work should focus on reducing disparities between remote and urban patients and on increasing access to clinics and hospitals, particularly in remote and isolated areas. For instance, adding mobile screening clinics would make it easier for patients, even in off-the-map areas2. The low number of oncologists should be addressed, and the workforce should be expanded to meet the growing demand. One way to address this issue is to develop incentive programs that encourage more oncologists to practice in rural areas7. Furthermore, hospitals should be up to date and offer all available treatments, no matter where they are. Finally, the government could help low-income patients by expanding insurance coverage for more families13. Ensuring patients across the country have access to healthcare should be a national priority.
References
- National Institutes of Health (NIH). Annual Report to the Nation Part 2: Patient Economic Burden of Cancer Care More than $21 Billion in the United States in 2019. 2021 [↩] [↩]
- Moscovice, Ira S., et al. Availability of Cancer Care Services and the Organization of Care Delivery at Critical Access Hospitals. Cancer Medicine, 2023 [↩] [↩] [↩] [↩] [↩]
- P. Hung, et al. Trends in Cancer Treatment Service Availability across Critical Access Hospitals and Prospective Payment System Hospitals. Medical Care, 2021 [↩] [↩]
- W. E. Zahnd, et al. Rural-Urban Differences in Financial Burden among Cancer Survivors: An Analysis of a Nationally Representative Survey. Supportive Care in Cancer, 2019 [↩]
- Chu, Q. D., St. Hill, C., Hsieh, M. C., et al. (2021). Social determinants of health associated with poor outcome for rural patients following resected pancreatic cancer. Journal of Gastrointestinal Oncology. [↩] [↩] [↩] [↩]
- National Cancer Institute. Rural Cancer Control. Cancer.gov, 2020 [↩]
- Bates, James Edward, and Christina Henson. Rural Cancer Care Access in the United States: A Worsening Problem? Journal of Clinical Oncology, 2022 [↩] [↩]
- Onega, T., et al. Population-based geographic access to parent and satellite National Cancer Institute Cancer Center facilities. Cancer, 2017 [↩]
- Wang, Weijing, et al. Rural–Nonrural Divide in Car Access and Unmet Travel Need in the United States. Transportation, 2023 [↩] [↩]
- National Institutes of Health (NIH). American Hospital Annual Survey on Oncology Care Availability, 2020 [↩]
- Medicare Payment Advisory Commission. Critical Access Hospitals Payment System. 2023 [↩] [↩]
- Liu, Zhaoli, et al. Impact of Rural Hospital Closures on Survival among Medicare Beneficiaries Diagnosed with Colorectal, Lung, Breast, and Prostate Cancer. The Journal of Rural Health, 2026 [↩] [↩]
- The Costs of Cancer in Rural Communities. American Cancer Society Cancer Action Network, 19 Oct. 2022. [↩] [↩] [↩] [↩] [↩] [↩] [↩]
- Weaver, Kathryn E., et al. “Rural-Urban Disparities in Health Status among US Cancer Survivors.” Cancer, vol. 119, no. 5, 23 Oct. 2012. [↩]
- Uscher, J. (2025, July 21). Managing cancer costs without health insurance: Options for coverage. Breastcancer.org. [↩]
- Odahowski, Cassie L., et al. “Financial Hardship among Rural Cancer Survivors: An Analysis of the Medical Expenditure Panel Survey.” Preventive Medicine, vol. 129, Dec. 2019. [↩]
- Deshmukh, Y., et al. “Self-Reported Financial Toxicity among Rural Cancer Patients Treated with Radiotherapy.” Advances in Radiation Oncology. [↩]
- Xu, Richard Huan, et al. “Urban–Rural Differences in Financial Toxicity and Its Effect on Cancer Survivors’ Health-Related Quality of Life and Emotional Status: A Latent Class Analysis.” Supportive Care in Cancer. [↩]
- Planey, Arrianna Marie, et al. “Navigating Dual Burdens: Financial Burdens and Travel Burdens among Rural-Dwelling Cancer Survivors.” Cancer Control. [↩]
- Abdullah, Abiha, et al. “From Diagnosis to Survivorship: The Role of Social Determinants in Cancer Care.” Cancers. [↩]
- Lee, Minjee, et al. “Rural-Urban Disparities in Telemedicine Use among U.S. Adults with Cancer”. Telemedicine and E-Health, 2 Feb. 2024. [↩] [↩]
- Johannes, Bobbie L., et al. “Rural-Urban Differences in Telehealth Utilization and Delayed Care during the COVID-19 Pandemic.” Telemedicine Journal and E-Health. [↩]
- Curtis, Kevin, et al. “Pandemic Use of Telehealth by Oncology at a Rural Academic Medical Center.” Telemedicine Journal and E-Health. [↩]
- Holtz, Bree E., et al. “Perceptions of Telehealth-Based Cancer Support Groups at a Rural Community Oncology Program. [↩]
- Ma, Ting Martin, et al. “Experience of Telemedicine Visits in Radiation Oncology during the COVID-19 Pandemic: A US National Survey and Lessons Learned for Incorporating Telemedicine Post-COVID-19.” Advances in Radiation Oncology, Dec. 2022. [↩]
- Mackwood, Matthew, et al. “Comparing Trends in Telemedicine Use and Geographic Disparities in Utilization among Patients with Cancer in the United States.” JCO Oncology Practice. [↩]
- Alcaraz, Kassandra I., et al. “Telehealth Use and Nonuse among Cancer Survivors in the United States and Associations with Adverse Social Determinants of Health. [↩]
- MacCormack, Terry. “Which Social Determinants of Health Have the Greatest Impact on Rural–Urban Colorectal Cancer Mortality Disparities?” Wiley.com, 2020. [↩] [↩]
- Unger, J. M., Moseley, A., Symington, B., & Hershman, D. L. (2025). Cancer in rural America: Improving access to clinical trials and quality of oncologic care. CA: A Cancer Journal for Clinicians. [↩] [↩]
- Shen, Xinglei, et al. “Differences in Rural versus Urban Patients with Prostate Cancer in Diagnosis and Treatment: An Analysis of a Population-Based Cohort.” JCO Oncology Practice. [↩]
- Tucker-Seeley, Reggie, et al. “Social Determinants of Health and Cancer Care: An ASCO Policy Statement.” JCO Oncology Practice. [↩]
- World Population Review. “Most Rural States in the U.S.” World Population Review, 28 Oct. 2025. [↩]
- Hashtarkhani, Soheil, et al. “Analyzing Geospatial and Socioeconomic Disparities in Breast Cancer Screening among Populations in the United States: Machine Learning Approach.” JMIR Cancer. [↩]
- Ose, Dominik J., et al. “Rural–Urban Disparities in Cancer Care—Analyzing Routinely Collected Patient‐Reported Outcomes. A Cross‐Sectional Study.” Cancer Medicine. [↩]
- Atkins, Graham T., et al. “Residence in Rural Areas of the United States and Lung Cancer Mortality. Disease Incidence, Treatment Disparities, and Stage-Specific Survival.” Annals of the American Thoracic Society. [↩]
- Logan, Charles D., et al. “Rural‐Urban Survival Disparities for Patients with Surgically Treated Lung Cancer.” Journal of Surgical Oncology. [↩] [↩]
- Thompson, Jeffrey A., et al. “The Need to Study Rural Cancer Outcome Disparities at the Local Level: A Retrospective Cohort Study in Kansas and Missouri.” BMC Public Health. [↩]



{kind=link}