
Abstract
Background/Objective: Hemorrhagic shock necessitates rapid fluid resuscitation, where catheter choice critically impacts delivery speed. Standard triple-lumen central venous catheters (CTLs) offer essential multi-lumen access but have limited flow rates compared to peripheral catheters (P). This study aimed to evaluate whether shortening a CTL to create a novel modified triple-lumen large vessel catheter (MTL) could significantly enhance saline transfusion rates while preserving large vessel access utility, addressing the gap when high flow and large vessel access are concurrently needed.
Methods: An in vitro comparative study was conducted. Flow rates of 0.9% saline were measured for a 16-gauge P, a standard 7Fr/20cm CTL, and a novel 7Fr/10cm MTL (manually shortened CTL). Experiments varied applied pressure (gravity vs. 300 mmHg via a pressure bag), IV bag height (152.4 cm vs. 203.2 cm using a medical IV pole), and lumen usage (single distal vs. all three lumens for CTL/MTL). Time to collect 500 ml saline in a graduated cylinder was measured using an iPhone stopwatch, and flow rates (ml/min) were calculated (n=5 trials/condition). Paired t-tests assessed significance.
Results: The P catheter achieved the highest flow rate (237.0 ± 2.36 ml/min) under 300 mmHg pressure and 203.2 cm height. Compared to the CTL, the MTL demonstrated significantly higher flow rates under identical conditions: 31.7% higher using a single lumen (94.8 ± 1.12 vs 72.0 ± 0.263 ml/min, p<0.001) and 41.5% higher using triple lumens (169.8 ± 1.64 vs 120.0 ± 1.22 ml/min, p<0.001) at 300 mmHg / 203.2 cm. Applied pressure and multi-lumen use were major determinants of flow rates for CTL and MTL; height had a lesser effect.
Conclusions: Shortening a standard triple-lumen central venous catheter significantly increases achievable saline infusion rates in vitro, consistent with Poiseuille’s law. While peripheral catheters remain superior for maximal flow, the novel MTL offers a substantial improvement over standard CTLs, presenting a potentially valuable option for rapid resuscitation when large vessel access is required. Further investigation, including in vivo studies, is warranted due to the non-physiological in vitro system and manual modification variability.
Keywords: Hemorrhagic Shock; Fluid Resuscitation; Intravenous Catheters; Central Venous Catheter; Large Vessel Catheter; Peripheral Venous Catheter; Triple-Lumen Catheter; Flow Rate; Poiseuille’s Law; Catheter Modification; In Vitro Study; Critical Care; Emergency Medicine. (Abstract Word Count: Approx. 248 words)
Introduction
Background and Context
Hemorrhagic shock, resulting from significant blood loss, leads to inadequate tissue perfusion and oxygen delivery, representing a time-critical medical emergency1. Rapid restoration of intravascular volume, often initiated with isotonic crystalloids, is crucial to prevent irreversible organ damage and death until blood units have been procured from the blood bank. The efficiency of this fluid resuscitation is heavily influenced by the characteristics of the intravenous access device used2. Existing devices range from short, wide-bore peripheral catheters, designed for high flow rates in superficial veins, to longer, multi-lumen central venous catheters, designed for reliable access to large central veins and administration of multiple therapies but typically exhibiting lower flow rates3. A clinical challenge arises when patients require rapid fluid administration but have poor peripheral venous access, or when the need for reliable venous access (e.g., for vasopressors) coexists with the need for high-volume infusion4. During shock, peripheral vessels are hard to find due to vasoconstriction in the setting of hypovolemia, further complicating rapid fluid administration. Standard triple-lumen central catheters (CTLs), while offering necessary multi-port access, may provide inadequate flow rates for effective resuscitation due to their length and narrow lumen diameters, as predicted by Poiseuille’s law2. This study addresses the gap in catheter options for scenarios demanding both reliable access and improved flow rates compared to standard CTLs.
Significance and Purpose
This research investigates a potential solution by evaluating a simple modification – shortening – to a standard CTL. If shortening significantly enhances flow rates, this modified catheter could offer a valuable clinical tool, improving resuscitation capabilities in critical care, emergency medicine, and perioperative settings where standard options are suboptimal. The purpose of this study is to quantify the flow rate improvement achieved by shortening a CTL in an in vitro setting.
Objectives
The primary objective was to compare the saline flow rates of a novel, shortened modified triple-lumen large vessel catheter (MTL) against a standard-length CTL and a large-bore peripheral catheter (P) under varying conditions relevant to fluid resuscitation. Specifically, we aimed to quantify the effects of applied pressure, IV bag height, and single versus multi-lumen use on flow rates for each catheter type. We hypothesized that the MTL would demonstrate significantly higher flow rates than the CTL, particularly under pressure and with multi-lumen use.
Scope and Limitations
This study was conducted in vitro using 0.9% saline. It systematically varied catheter type, pressure, height, and lumen usage. The scope is limited to these parameters and does not account for physiological variables like blood viscosity or venous resistance. Limitations inherent to the in vitro design are discussed later.
Theoretical Framework
The study is grounded in the principles of fluid dynamics, specifically Poiseuille’s law: Q = (π * r⁴ * ΔP) / (8 * η * L). This law posits that flow rate (Q) is inversely proportional to length (L) and viscosity (η), and directly proportional to the pressure gradient (ΔP) and the fourth power of the radius (r). Our hypothesis—that shortening the catheter (decreasing L) increases flow—directly stems from this framework2.
Methods
This study employed a comparative in vitro experimental design to evaluate the effect of catheter type (peripheral vs. standard central vs. modified catheter), applied pressure, IV bag height, and lumen usage on saline infusion flow rates. This in vitro study used no human or animal participants.
Materials
- Catheters:
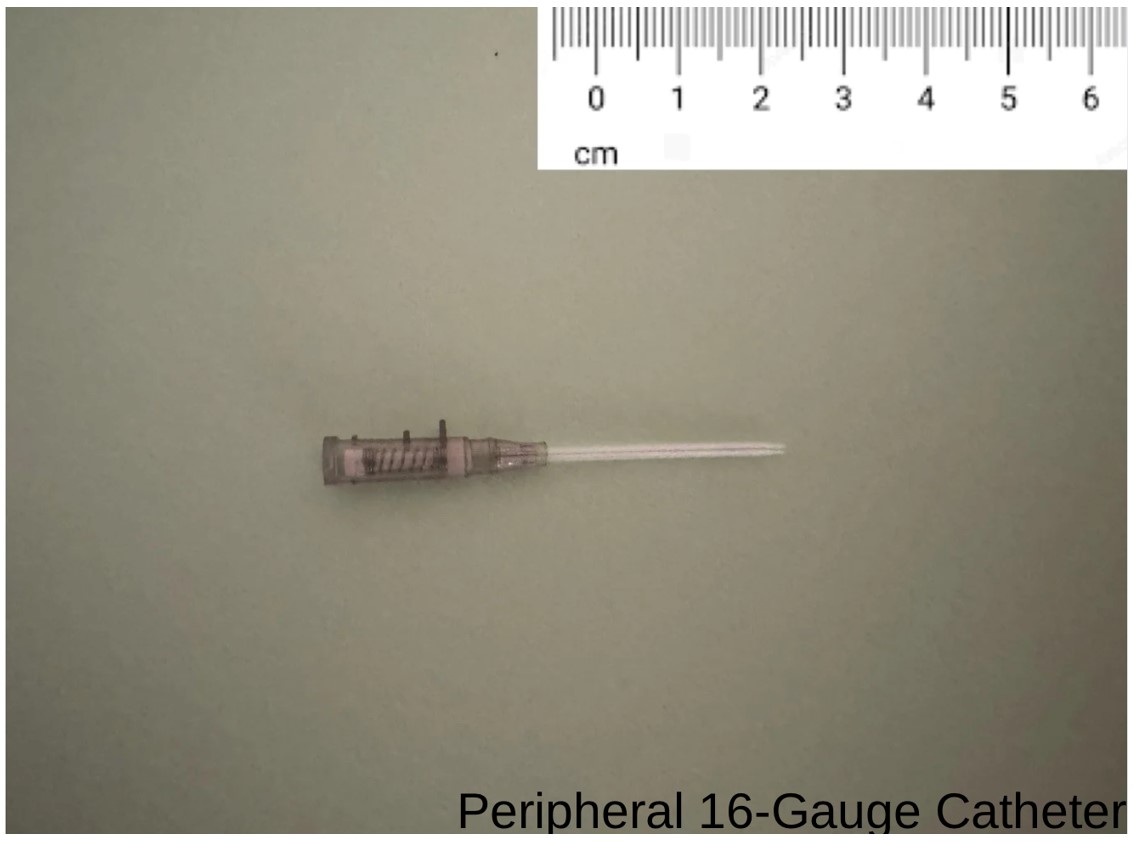
- Peripheral catheter (P): 16-gauge peripheral IV catheter, approx. 5 cm length (BD, Cat# 381447 or similar). (Photo1)
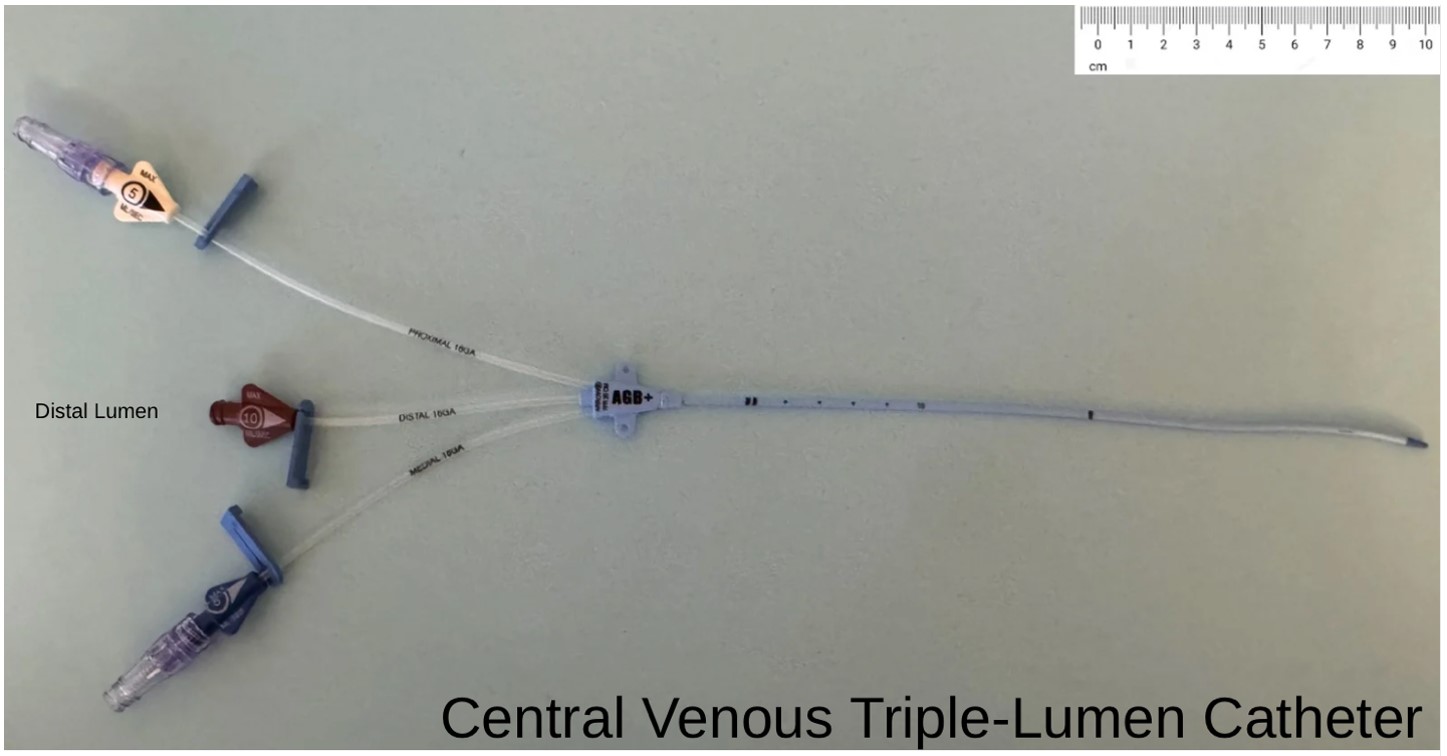
- Standard triple-lumen catheter (CTL): 7 French (Fr), 20 cm length Arrow® Triple-Lumen CVC Kit (Teleflex Medical, Wayne, PA, USA; Cat# AK-15703).(Photo2)
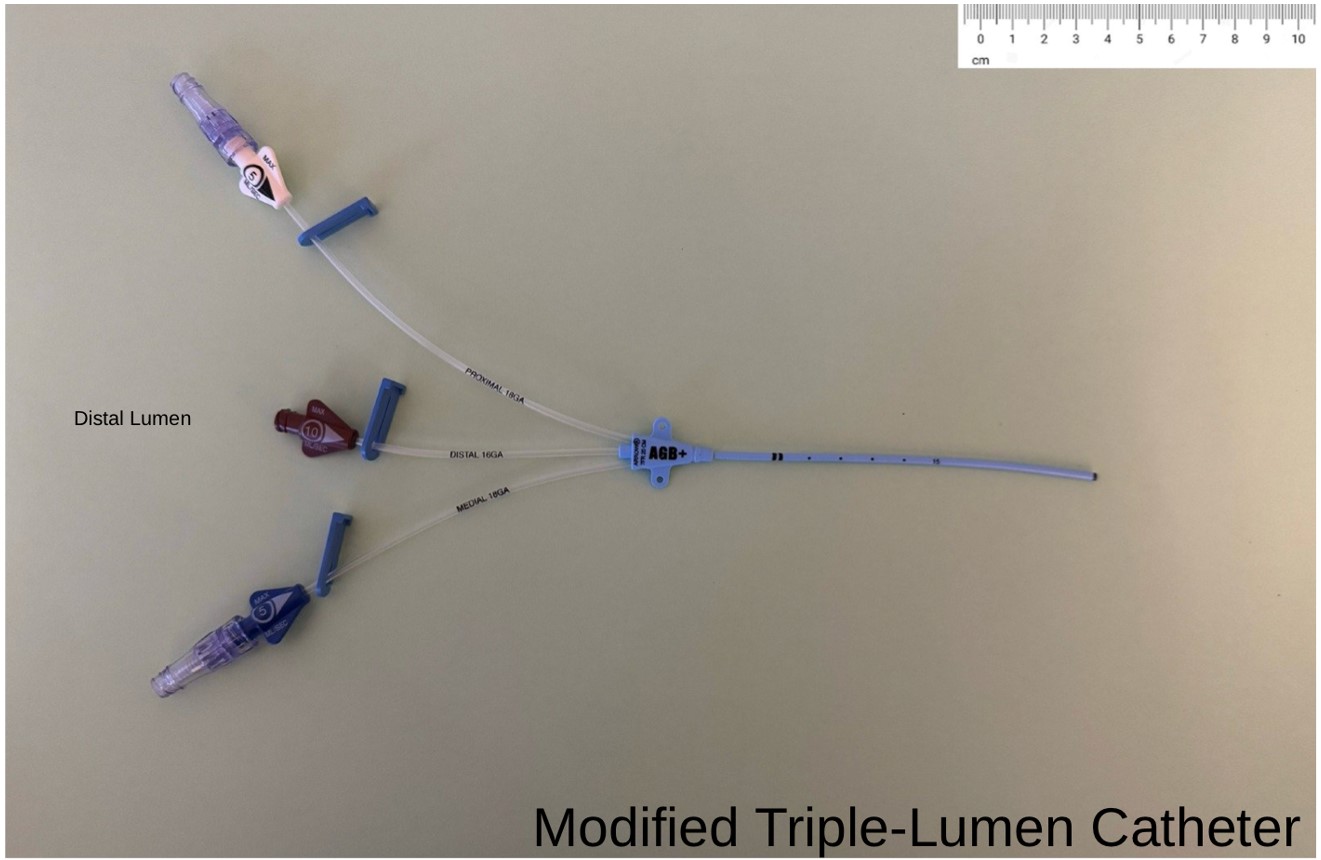
- Modified triple-lumen catheter (MTL): An identical Arrow® CTL (Cat# AK-15703) was manually shortened to 10 cm using sterile scissors. (Photo 3)
- Fluid: 500 ml bags of 0.9% Sodium Chloride Injection, USP (Saline) (Wallcur, San Diego, CA, USA).
- Equipment:
- Intravenous administration sets (Baxter, Cat# 2C6401).
- Reusable pressure infusion bag (American Hospital Supply (AHS), McGaw Park, IL, USA; REF AHSPIB500).
- 500 ml Class B graduated cylinder (Fisher Scientific, Hampton, NH, USA; Cat# 08-572-5C).
- iPhone stopwatch function (Apple Inc., Cupertino, CA, USA) for timing.
- Intravenous (IV) pole (Drive Medical, Port Washington, NY, USA).
Data Analysis
Data were collected by measuring the time to infuse 500 ml of 0.9% saline through catheters using a graduated cylinder and an iPhone stopwatch, varying pressure, height, and lumen usage. For each condition, the five recorded times were averaged. The average flow rate (Q) was calculated: Q (ml/min) = 500 / Average Time (s) * 60. Percentage changes between conditions were calculated to compare the effects of variables. Paired t-tests compared CTL and MTL flow rates at 300 mmHg/203.2 cm for single and triple lumens, with p-values reported. Standard deviations (SD) were calculated to assess variability, and data were tabulated and prepared for graphical representation (bar charts) with error bars (±SD).
Variables and Measurements
Independent Variables: Catheter type (P, CTL, MTL), Applied Pressure (Gravity, 300 mmHg), IV Bag Height (152.4 cm, 203.2 cm), Lumen Usage (Single, Triple for CTL/MTL) [16-gauge vs. 16-, 18-, 18-gauge]. · Dependent Variable: Time (seconds) to collect 500 ml of saline. · Calculated Measurement: Flow Rate (ml/min).
Procedure
- The system (IV tubing, catheter lumen(s)) was primed with saline.
- The IV bag was set to the designated height.
- Pressure (0 mmHg or 300 mmHg) was applied as per the experimental condition.
- The catheter tip was positioned over the graduated cylinder.
- The roller clamp was fully opened, and timing was started simultaneously.
- Timing was stopped precisely when saline reached the 500 ml mark.
- Elapsed time was recorded.
- Steps 1-7 were repeated five times (n=5) for each unique condition, randomizing test order to minimize sequence bias in the last 2 trials. For multi-lumen tests, all three lumens were allowed to flow simultaneously.
Ethical Considerations
This was an in vitro bench study using non-biological materials; therefore, ethical approval and informed consent were not applicable. The study was conducted in accordance with the International Science and Engineering Fair guidelines5.
Results
We performed three distinct experimental series to quantify the influence of applied pressure, lumen utilization, and IV bag height on the flow rates achievable with Peripheral (P), standard Central Triple-Lumen (CTL), and Modified Triple-Lumen large vessel (MTL) catheters using 0.9% saline.
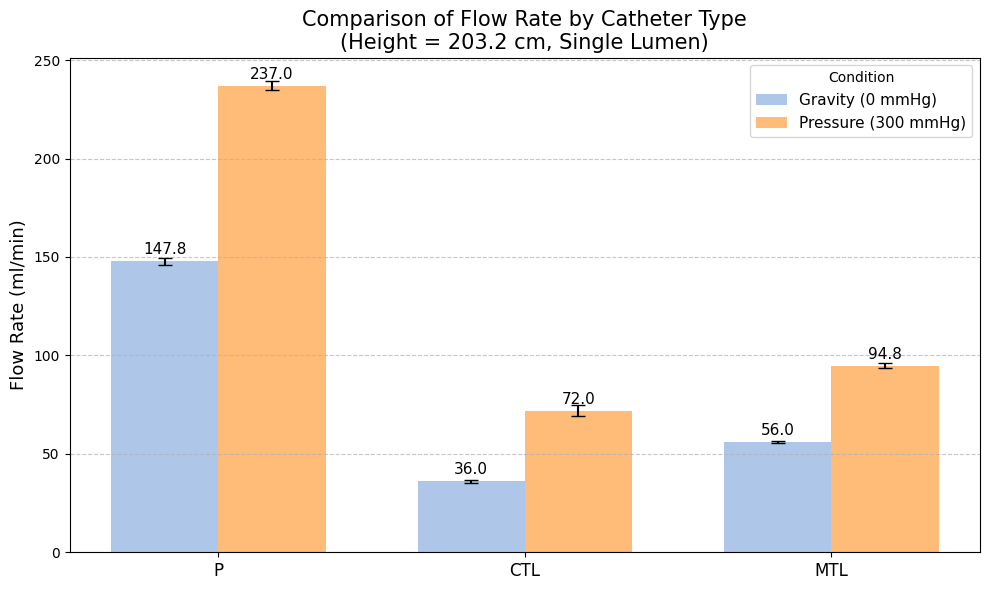
Experiment 1: Effect of Pressure on Flow Rate
In this experiment, flow rates were measured using a single lumen (distal for CTL/MTL) with the IV bag positioned at a height of 203.2 cm. We compared flow driven solely by gravity against flow augmented by 300 mmHg of applied pressure. As detailed in Table 1 and visualized in Figure 1, the application of 300 mmHg pressure resulted in substantial increases in flow rates for all catheter types compared to gravity infusion. The P catheter exhibited a 60% increase in flow, rising from 147.8 ± 1.92 ml/min under gravity to 237.0 ± 2.36 ml/min under pressure. The CTL demonstrated the largest relative increase (100%), although its absolute flow rates remained the lowest, increasing from 36.0 ± 0.70 ml/min to 72.0 ± 2.63 ml/min. The MTL showed a robust 69% improvement, with flow increasing from 56.0 ± 0.71 ml/min to 94.8 ± 1.12 ml/min. Across both pressure conditions, the P catheter maintained the highest flow rate, followed by the MTL, which consistently outperformed the CTL. The MTL outperformed the CTL by 31.7% at 300 mmHg (p<0.001). This clearly establishes applied pressure as a major determinant of flow rate.
| Catheter | Flow Rate under Gravity (ml/min) | SD under Gravity | Flow Rate at 300 mmHg (ml/min) | SD at 300 mmHg | % Change with Pressure | p-value (vs. CTL) |
| P | 147.8 | 1.923538 | 237.0 | 2.359378 | 60.351827 | 0.0 |
| CTL | 36.0 | 0.707107 | 72.0 | 2.631313 | 100.000000 | — |
| MTL | 56.0 | 0.707107 | 94.8 | 1.125463 | 69.285714 | 0.0 |
Experiment 2: Effect of Lumen Usage on Flow Rate
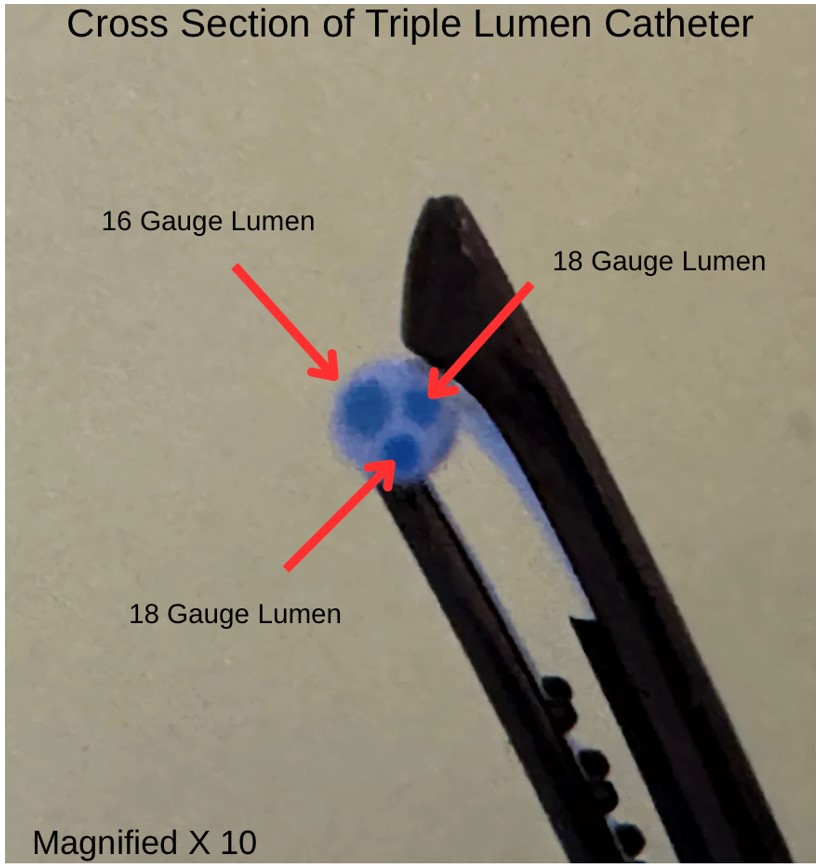
Focusing on the multi-lumen central catheters (CTL and MTL), we investigated the impact of utilizing all three lumens simultaneously compared to using only the single distal lumen. These trials were conducted under high-flow conditions (300 mmHg pressure, 203.2 cm height). The results, presented in Table 2 and Figure 2, demonstrate that engaging all three lumens significantly boosted the aggregate flow rate for both catheter types. The CTL’s flow rate increased by 66%, from 72.0 ± 2.63 ml/min with a single lumen to 120.0 ± 1.22 ml/min when all three lumens were active. The MTL experienced an even greater enhancement, with a 79% increase in flow rate, surging from 94.8 ± 1.13 ml/min (single lumen) to 169.8 ± 1.64 ml/min (triple lumen). The MTL’s triple-lumen flow was 41.5% higher than the CTL’s (p<0.001). This highlights the additive benefit of using multiple parallel channels for infusion and shows the MTL benefits more substantially from this strategy compared to the longer CTL under these conditions. Lumen contributions were estimated: ~50% from the 16-gauge distal lumen, ~25% each from the 18-gauge proximal lumens (Photo 4). Thus, when all three lumens are used simultaneously, the distal 16-gauge lumen generally contributes the majority of total flow—often in the range of 50–60%—with each 18-gauge lumen contributing approximately 20–25% of the total, though these proportions can vary depending on infusion pressure, fluid viscosity, and adjuncts such as tubing and valves, according to the manufacturer’s information package5.
| Catheter | Flow Rate – Single Lumen (ml/min) | SD – Single Lumen | Flow Rate – Triple Lumen (ml/min) | SD – Triple Lumen | % Change with Triple Lumens | p-value (vs. CTL) |
| CTL | 72.0 | 2.631313 | 120.0 | 1.224745 | 66.666667 | 0.0 |
| MTL | 94.8 | 1.125463 | 169.8 | 1.643168 | 79.113924 | 0.0 |

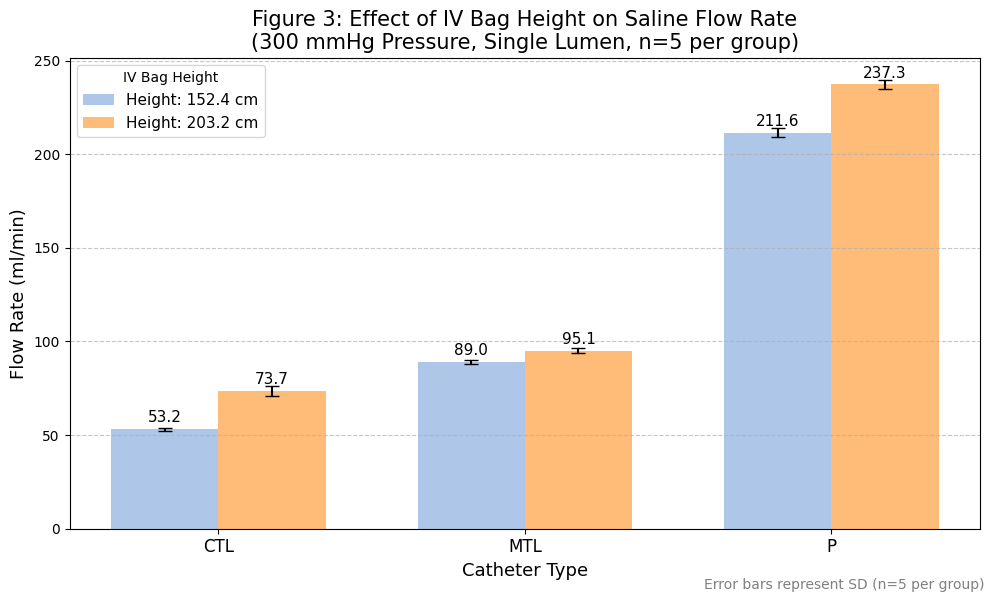
Experiment 3: Effect of IV Bag Height on Flow Rate
To assess the contribution of hydrostatic pressure, flow rates were compared with the IV bag height set at 152.4 cm versus 203.2 cm. These tests were conducted using a single lumen for each catheter type under 300 mmHg applied pressure. Increasing the IV bag height by approximately 51 cm (20 inches) resulted in modest increases in flow rates for all catheters, as shown in Table 3 and Figure 3. The P catheter’s flow rate increased by 12% (from 211.6 ± 2.30 ml/min to 237.6 ± 2.36 ml/min). The CTL showed the largest relative benefit from increased height with a 35% flow increase (from 53.2 ± 0.84 ml/min to 72.0 ± 0.71 ml/min), potentially reflecting its higher overall resistance being more sensitive to changes in hydrostatic head. The MTL flow rate improved by a smaller margin of 7% (from 89.0 ± 1.22 ml/min to 94.8 ± 1.10 ml/min). These findings suggest that while increasing IV height does improve flow, its impact, especially under conditions of high applied pressure, is considerably less pronounced than the effect of applied pressure itself or multi-lumen usage.
| Catheter | Flow Rate at 152.4 cm (ml/min) | SD at 152.4 cm | Flow Rate at 203.2 cm (ml/min) | SD at 203.2 cm | % Change with Height | p-value (vs. CTL) |
| P | 211.6 | 2.302173 | 237.0 | 2.359378 | 12.003781 | 0.0 |
| CTL | 53.2 | 0.836660 | 72.0 | 2.631313 | 35.338346 | — |
| MTL | 89.0 | 1.224745 | 94.8 | 1.125463 | 6.516854 | 0.0 |
Discussion
This in vitro investigation confirmed that a 16-gauge peripheral catheter (P) provides the highest saline flow rates among the tested devices. Crucially, it demonstrated that a novel modified triple-lumen large vessel catheter (MTL), created by shortening a standard 20 cm CTL to 10 cm, achieves significantly higher flow rates than the standard CTL. This advantage was evident under both gravity and pressure infusion and was particularly pronounced when utilizing all three lumens simultaneously, where the MTL outperformed the CTL by 41.5% under 300 mmHg pressure (p<0.001). Applied pressure and multi-lumen use were the most influential factors enhancing flow for the central catheters. The findings show trends consistent with the inverse relationship between catheter length and flow rate predicted by Poiseuille’s law2, though this relationship is limited by the law’s assumptions of laminar, steady, non-pulsatile flow through a rigid, cylindrical, Newtonian system. Real catheters, including the MTL and CTL, feature non-uniform internal geometries, side holes, and variable compliance, which may deviate from these ideal conditions. The significantly improved flow rates of the MTL compared to the standard CTL carry important clinical implications. In situations demanding both reliable venous access and rapid fluid delivery, where peripheral access is inadequate or unavailable4, the MTL could facilitate more effective resuscitation than currently possible with standard CTLs. This simple modification offers the potential to bridge a critical gap in vascular access options, potentially improving outcomes in trauma, major hemorrhage, and other critical care scenarios1. However, insertion feasibility remains a concern, as the 10 cm MTL may not reliably reach central vessels, a challenge supported by Pikwer et al. who reported a 3.3% malposition rate for central venous catheters, with higher risks (9.1%) via the right subclavian vein6, suggesting that shortened catheters like the MTL may be better suited for proximal large vessel access rather than central venous placement. Additionally, trimming catheter tips is a common practice, especially in neonatal and pediatric patients when the manufacturer-supplied lengths do not align with patient anatomy7. Inserra et al, using electron microscopy surface scans, found that scalpel trimming results in a smoother tip surface compared to scissors, potentially lowering the risk of long-term complications7. These findings may guide future improvements to the MTL’s manual trimming process to enhance both safety and performance.
Connection to Objectives: The study successfully met its objective of quantifying and comparing flow rates across the three catheter types under varied conditions. The results directly support our hypothesis: the shortened MTL demonstrated significantly higher flow rates than the standard CTL, confirming the substantial impact of length reduction on central catheter performance. The relative contributions of pressure, height, and lumen usage were also clearly delineated.
Recommendations: Based on these promising in vitro findings, further research is strongly recommended. Future directions should include testing with fluids mimicking blood viscosity to obtain more clinically relevant flow estimates, utilizing precisely manufactured shortened catheters to eliminate variability from manual modification, conducting in vivo studies (animal models or clinical trials) to assess performance under physiological conditions, evaluate insertion safety and feasibility, and determine actual clinical impact9, investigating optimal and safe infusion pressures for clinical use and exploring other design modifications (e.g., lumen diameter optimization) to further enhance flow.
Limitations: The findings must be interpreted considering the study’s limitations. The in vitro model using saline does not replicate physiological conditions like blood viscosity, venous back-pressure, or vessel characteristics8. Therefore, absolute flow rates observed here may not directly translate to clinical practice. The use of 300 mmHg pressure, while maximizing flow in vitro, may carry clinical risks requiring careful safety evaluation. The manual shortening of the MTL introduces potential inconsistencies, and the limited number of trials (n=5) restricts statistical power. Potential minor measurement inaccuracies in timing or volume could exist, e.g., residual air bubbles, though the system was re-primed and standardized between trials with fixed tubing length. The limitations of in vitro systems using saline instead of blood or colloids, the absence of venous compliance, and the lack of shear stress modeling are well supported in the medical literature. Saline has a viscosity of approximately 1 centipoise, whereas blood has a viscosity of about 3–4 centipoise, and this difference significantly impacts flow predictions, especially in small lumens, as described by Poiseuille’s law. The clinical relevance of these differences is demonstrated by Berman et al. showed that packed red blood cells have a viscosity 4.5 times that of normal saline, resulting in markedly reduced flow rates through catheters, and that the choice of fluid and adjuncts can substantially alter flow characteristics in simulated environments2. Eckmann et al. further quantified that hemodilution with saline or albumin decreases blood viscosity more than with plasma or hydroxyethyl starch, and that viscosity is highly sensitive to hematocrit, temperature, and shear rate, all of which are not replicated in simple saline-based in vitro models9. Ko et al. confirmed that the viscosity of colloids such as 6% hetastarch is 2.6 times that of saline, and that flow regulators calibrated for saline can overestimate flow rates when used with more viscous fluids10. Additionally, Sirs demonstrated that blood is non-Newtonian and that its flow in small vessels deviates from predictions based on Newtonian fluids like saline, with effective viscosity increasing in small lumens due to the Fahraeus-Lindqvist effect and other hemorheological properties11. These findings collectively highlight the non-physiological aspects of in vitro systems using saline, limiting the direct translatability of such results to clinical practice. Given the estimated Reynolds numbers of ~1500–2000 during high-pressure (300 mmHg) infusion with all lumens open, which falls in the transitional flow regime, turbulent flow could potentially occur, particularly in the MTL and CTL, though this was not directly measured and warrants further investigation. Finally, this study did not quantify the individual contributions of applied pressure and lumen usage using a structured multivariate or factorial framework. Future work should incorporate normalized flow metrics to better isolate the specific impact of catheter shortening.
Conclusion
This study demonstrated that the 16-gauge peripheral catheter (P) delivered the highest saline flow rates, while the modified triple-lumen large vessel catheter (MTL), shortened from a 20 cm central venous catheter (CTL) to 10 cm, significantly outperformed the CTL, achieving 31.7% and 41.5% higher flow rates for single and triple lumens, respectively, at 300 mmHg (p<0.001 in both). These findings, aligned with Poiseuille’s law, highlight the MTL’s potential to enhance fluid resuscitation in critical care scenarios requiring large vessel access, offering a transformative approach to vascular access strategies that could improve patient outcomes in emergency settings. Future research should test blood-mimicking fluids, use precision-manufactured MTLs, and conduct in vivo trials. This catheter modification shows promise for revolutionizing emergency care, urging clinical validation.
Acknowledgments
I thank my biology teacher, Dr. Joykutty for her invaluable guidance and support throughout this project and my AP Physics 1 teacher, Mrs. MacNamara for deepening my understanding of fluid dynamics.
Figures
References
- N. Kupchik. Principles of resuscitation. Crit Care Nurs Clin North Am. 33, 225–244 (2021). DOI:10.1016/j.cnc.2021.05.001. [↩] [↩]
- D. J. Berman, A. Schiavi, S. M. Frank, S. Duarte, D. A. Schwengel, C. R. Miller. Factors that influence flow through intravascular catheters: The clinical relevance of Poiseuille’s law. Transfusion. 60(7), 1410–1417 (2020). DOI:10.1111/trf.15898. [↩] [↩] [↩] [↩]
- S. Traylor, A. Bastani, N. Butris-Daut, M. Christensen, P. Marsack, L. Rodgers, B. Todd. Are three ports better than one? An evaluation of flow rates using all ports of a triple lumen central venous catheter in volume resuscitation. Am J Emerg Med. 36(5), 739–740 (2018). DOI:10.1016/j.ajem.2017.09.058. [↩]
- M. Bilal, O. Alhajjar, M. Madisetty, V. Kantamaneni, S. Singh, M. Babich, A. Kapetanos. Adherence to two large-bore intravenous lines in acute gastrointestinal bleeding is low. Dig Dis Sci. 64(3), 627–631 (2019). DOI: 10.1007/s10620-019-5455-7. [↩] [↩]
- Arrow-Howes Multi-Lumen Central Venous Catheter with Blue FlexTip®. TeleFlexVascular, www.teleflexvascular.com/files/lidstock/IC-12703-130A.pdf. Accessed 29 June 2025. Infographic. [↩]
- A. Pikwer, L. Bååth, B. Davidson, I. Perstoft, J. Akeson. The incidence and risk of central venous catheter malpositioning: a prospective cohort study in 1619 patients. Anaesth Intensive Care. 36(1), 30–37 (2008). DOI:10.1177/0310057X0803600106. [↩]
- A. Inserra, et al. Trimming long-term tunneled central venous catheters in pediatric patients. Pediatr Blood Cancer. (2012). DOI: 10.1002/pbc.24310. [↩] [↩]
- M. H. Hu, W. H. Chan, Y. C. Chen, C. H. Cherng, C. K. Lin, C. S. Tsai, Y. C. Chou, G. S. Huang. Effect of external pressure and catheter gauge on flow rate, kinetic energy, and endothelial injury during intravenous fluid administration in a rabbit model. Shock. 45(1), 98–103 (2016). DOI: 10.1097 SHK.0000000000000464. [↩]
- D. M. Eckmann, S. Bowers, M. Stecker, A. T. Cheung. Hematocrit, Volume Expander, Temperature, and Shear Rate Effects on Blood Viscosity. Anesthesia and Analgesia. 2000;91(3):539-45. DOI:10.1097/00000539-200009000-00007. [↩]
- E. Ko, Y. J. Song, K. Choe, et al. The Effects of Intravenous Fluid Viscosity on the Accuracy of Intravenous Infusion Flow Regulators. Journal of Korean Medical Science. 2022;37(9):e71. DOI:10.3346/jkms.2022.37.e71. [↩]
- J. A. Sirs. The Flow of Human Blood Through Capillary Tubes. The Journal of Physiology. 1991;442:569-83. DOI:10.1113/jphysiol.1991.sp018809. [↩]



{kind=link}