
Abstract
Immigration continues to reshape the demographic landscape of the United States, with immigrants facing unique challenges at the intersection of economic opportunity and psychological adaptation. This study investigated the relationships between economic hardship, healthcare access barriers, and mental health outcomes among immigrant populations, guided by Pearlin’s Stress Process Model. The sample consisted of 57 participants (M age = 33.19 years, 67.9% female) representing diverse immigrant backgrounds. Participants completed validated measures assessing economic strain, depression (PHQ-9), anxiety (GAD-7), healthcare access barriers (HCAB), and social support (MSPSS). Hierarchical regression analyses revealed that economic stress significantly predicted depression symptoms (β = .23, p = .02) but not anxiety symptoms when demographic covariates were controlled. Mediation analyses using bootstrap procedures demonstrated that healthcare access barriers, particularly financial barriers, significantly mediated the relationship between economic stress and both depression (mediated effect = .21, 95% CI [.06, .35]) and anxiety (ACME = .25, 95% CI [.07, .46]). Financial barriers accounted for approximately 89% of the total effect of economic stress on depression. Contrary to expectations, social support did not demonstrate significant protective effects in controlled analyses. Demographic factors emerged as important predictors, with age showing protective effects against depression and significant racial/ethnic differences in mental health outcomes. These findings highlight the critical role of healthcare access barriers in linking economic hardship to poor mental health among immigrants. The results suggest that interventions targeting healthcare accessibility, particularly financial barriers, may be effective in promoting mental health equity among economically disadvantaged immigrant populations. Limitations include the cross-sectional design and sample characteristics that may limit generalizability.
Keywords: Economic hardship, immigrants, mental health, healthcare access, mediation analysis
Introduction
Immigration continues to reshape the demographic landscape of the United States, with immigrants and their U.S.-born children now comprising 26.8% of the total population1. An immigrant is generally defined as an individual who relocates from their country of origin to another nation, either temporarily or permanently, to live, work, or seek refuge. Among the immigrant population, Latinos make up the largest share at approximately 44%, followed by Asian immigrants at around 27%, White immigrants at 17%, and Black immigrants at about 10%2. Recent data indicates that approximately 46.2 million immigrants live in the United States as of 2022, with nearly one in four being undocumented3. A significant portion of recent immigrants, especially from Asia and Africa, are arriving through employment-based or humanitarian pathways, reflecting changing global migration patterns. This growing population faces unique challenges at the intersection of economic opportunity, social mobility, and psychological adaptation4.
The process of immigration and settlement can be understood through Pearlin’s Stress Process Model5. This framework helps explain how economic hardships create cascading effects on mental health and functional outcomes through both direct pathways and secondary stressors such as healthcare access barriers. The model posits that primary stressors (such as economic strain) can proliferate into secondary stressors (such as inability to access healthcare), which then combine to influence psychological wellbeing. These stressors often differ by ethnicity and immigration status. For instance, undocumented immigrants and refugees face heightened vulnerability to deportation fears and legal exclusion, adding layers of chronic stress. This theoretical lens is particularly relevant for understanding immigrant experiences, as economic challenges often intersect with structural barriers in the healthcare system to compound mental health risks. While immigration often promises improved economic prospects, the reality for many immigrants involves significant challenges that can impact both mental health6.
The combination of Pearlin’s Stress Process Model and Berry’s Acculturation Theory offer the most comprehensive methodology in understanding how immigration affects mental health. Stressors associated with immigration to a new country include acculturative stress such as language barriers, differing cultural values, and decreased familiarity with institutions. These stressors may compound the effects of increased economic hardship and lead to increased levels of psychological distress. The use of both Pearlin & Berry’s Theories creates a better understanding of how immigrants experience and cope with structural economic stressors created by the immigration process as well as the additional acculturative stress created when settling into American society. Both theories complement, rather than contradict, each other and provide a complete outline of how socioeconomic, cultural, and structural barriers interact to shape the mental health outcomes of immigrants.
Economic Factors in Immigration
Immigration patterns to the United States are shaped by both push and pull factors that create complex migration dynamics. Push factors frequently include political instability, authoritarian regimes, and economic depression in origin countries7. These conditions often combine to create untenable situations where migration becomes necessary for survival and prosperity. For example, an instance where migration has been catalyzed by precarious situations in home countries includes mass immigration from Venezuela due to President Nicolás Maduro’s electoral manipulation and censorship8. Analysts attribute migratory outflows to political repression or socioeconomic hardship, though peer-reviewed quantitative estimates remain limited, for example, President Canel Díaz’s inability to provide for Cuban citizens in the face of natural disasters and the Covid-19 Pandemic, and President Ortega’s bloody crackdowns on political dissent and human rights violations. Global cities serve as powerful pull factors, offering economic opportunities and higher wages while enabling transnational connections9. This economic draw is further complicated by remittance systems, which create complex financial relationships between immigrants and their countries of origin. While remittances, which reached $548 billion globally in 2019, can provide crucial financial support to families in their home countries, they may also perpetuate economic strain for home countries as well4. Most notably, in several Caribbean countries and to a smaller effect in South America, remittances were found to have caused a brain-drain effect which weakens the economic growth and potential of home countries10.
Mental Health Challenges and Healthcare Access
The mental health of immigrant populations presents a nuanced picture, characterized by what researchers term the “immigrant paradox.” Despite facing numerous stressors, first-generation immigrants often demonstrate better mental health outcomes than their U.S.-born counterparts6. However, this advantage can be undermined by various barriers to healthcare access, particularly among undocumented immigrants11.
Research reveals substantial heterogeneity in mental health outcomes across racial and ethnic groups within immigrant populations12. Some Hispanic, Black, and Asian immigrants groups report lower reports of mental illness than White populations13. However, scholars caution that these apparent advantages may reflect cultural stigma surrounding mental health disclosure, systematic underdiagnosis due to cultural misunderstanding by providers, or genuine cultural protective factors that buffer against psychological distress. Despite potentially lower prevalence rates, significant disparities persist in mental health service utilization, with Latin American, Asian, and African immigrant groups accessing services at substantially lower rates than other immigrant groups and White populations, even when experiencing comparable levels of psychological distress.
Generational patterns further complicate these relationships. Among Black immigrants, first-generation individuals and Caribbean populations demonstrate lower rates of psychiatric disorders compared to U.S.-born Black Americans, illustrating how nativity status interacts with racial identity to influence mental health outcomes14. Similarly, different effects of acculturation and nativity on mental health outcomes have been observed from studies in the Latino, Asian, and Black communities, which produces even more complexity to the generalization of phenomena like the immigrant paradox15. In summary, some immigrant groups show mental health resilience, while other groups are at higher risk. Ultimately, culturally competent care and cultural adaptation of treatment needs to be a primary ethical responsibility of providers.
Healthcare access barriers create additional layers of complexity in immigrant mental health, as financial constraints and lack of insurance coverage create significant obstacles to receiving regular care. Many immigrants also avoid seeking healthcare due to fears of deportation and legal consequences. Language and cultural barriers further complicate access to appropriate care, while limited knowledge of available services prevents utilization of existing resources. Additionally, experiences of discrimination within healthcare settings often discourage immigrants from seeking necessary medical attention. The intersection of these barriers with economic hardship creates a particularly challenging environment for maintaining psychological wellbeing. A qualitative study of 26 undocumented and uninsured Mexican women found that their experience seeking healthcare was ignored and was marred by a lack of acknowledgement of their suffering and a degradation of their human rights16. Furthermore, eleven percent of papers diagnosed the feeling of shame and stigma as a barrier for accessing healthcare. Undocumented immigrants felt that they would be a burden on the system or believed that they would be stigmatized if they sought services11
The convergence of structural, socioeconomic, and cultural barriers creates significant obstacles to accessing mental healthcare, potentially exacerbating existing psychological stressors and creating secondary stress processes that compound the effects of initial migration-related challenges17.
Social Support Networks: Assets and Vulnerabilities
Social support systems play a complex role in immigrant mental health, functioning simultaneously as protective resources and sources of vulnerability. Research demonstrates that immigrant communities typically rely on three primary support networks: family connections, friendship networks, and faith-based communities. These networks serve critical functions in providing emotional support, practical assistance, and cultural continuity during the challenging process of adaptation to a new society18.
Family networks represent the most fundamental source of support for many immigrant populations. Strong family bonds and intergenerational connections often serve as primary buffers against acculturation stress and economic hardship. Faith communities also play a key role: places of worship commonly house clinics, food pantries, and counseling programs that provide trusted “safe harbor” for immigrants19. In this way, strong family bonds and community cohesion act as protective cultural assets in immigrant neighborhoods.
However, structural factors can significantly strain these traditionally protective networks. Compared to U.S.-born adults, immigrants report substantially lower levels of emotional support, with many indicating they “rarely” or “never have someone to confide in”18. This paradox reflects how migration disrupts established social networks while simultaneously creating barriers to developing new supportive relationships. Stressors including poverty, language barriers, and anti-immigrant policies often weaken support systems precisely when they are most needed20.
The vulnerability of immigrant support networks becomes particularly pronounced among older immigrants. Research indicates that elderly immigrants depend almost entirely on spouses for assistance but maintain significantly fewer friendships and extended family connections compared to native-born elders, substantially increasing risks of social isolation21. Thus, this pattern suggests that while immigrants may maintain strong immediate family bonds, broader social integration often remains limited, creating precarious support structures that may not withstand major stressors such as economic hardship or health crises.
Cultural factors: Protective assets and adaptation challenges
Cultural characteristics brought from countries of origin create both protective factors and adaptation challenges that influence immigrant mental health outcomes. For example, traditional cultural values such as familismo (strong family loyalty), collectivistic orientations, and spiritual beliefs often serve as significant sources of resilience during the immigration process. Bekteshi (2024), emphasizes that family commitment (familismo) and faith provide Mexican immigrant women with emotional support that buffers stress, helping them overcome discrimination or hardship22. When immigrant cultures retain strong social support and culturally competent care, health outcomes improve; their review found that social support was a key mitigating factor against health problems caused by cultural stressors23. In other words, positive cultural assets (family solidarity, community identity, etc.) can protect immigrant wellbeing even as they navigate a new society.
These positive cultural assets – including family solidarity, community identity, and traditional coping mechanisms – can protect immigrant wellbeing even while navigating significant societal challenges. Cultural practices such as communal gatherings, religious traditions, and collective decision-making often provide structure and meaning that support psychological adaptation. However, immigrants themselves acknowledge that cultural factors significantly influence their healthcare decisions and help-seeking behaviors, suggesting that effective interventions must account for these cultural frameworks rather than imposing external models of care24.
At the same time, certain cultural factors create barriers. Language barriers represent the most immediate obstacle, with immigrants reporting limited English proficiency as a primary reason for avoiding healthcare services25. Misunderstanding medical instructions, inability to communicate symptoms effectively, and difficulty navigating complex healthcare systems often lead to underutilization of preventive care precisely when it would be most beneficial.
Cultural differences in conceptualizing mental health and help-seeking behavior may also create additional adaptation challenges. Traditional healing practices, different understandings of psychological distress, and varying levels of trust in medical authorities can conflict with Western biomedical approaches to mental healthcare. Choi & Kang (2025) likewise identify language barriers and ethnic discrimination as “significant obstacles” that increase acculturative stress23. In this view, the very cultural differences that enrich immigrant life can, without support, become hurdles to health and integration.
Integration with Economic Stress and Healthcare Access
The relationship between cultural factors, social support, and the economic stressors examined in this study operates through complex pathways. Strong cultural networks may buffer against some effects of economic hardship by providing practical assistance, emotional support, and alternative resources. However, when entire immigrant communities face similar economic challenges, the capacity of these networks to provide meaningful assistance becomes limited. Cultural barriers to healthcare access may compound the effects of financial barriers, creating multiple pathways through which economic stress undermines mental health outcomes.
Understanding these cultural and social dynamics is essential for interpreting patterns of healthcare utilization and mental health outcomes among economically stressed immigrant populations. The protective potential of cultural assets may be undermined when structural barriers prevent access to services, while cultural barriers may exacerbate the effects of economic constraints on healthcare access.
The Current Study
Building on previous research examining immigrant mental health, this study investigates the relationships between economic hardship, healthcare access barriers, and mental health outcomes among immigrant populations in the United States. Guided by Pearlin’s Stress Process Model, the study examines how economic strain operates as a primary stressor that directly affects mental health while simultaneously creating secondary stressors in the form of healthcare access barriers5.
According to this theoretical framework, primary stressors can proliferate into secondary stressors that become additional pathways through which the original stressor influences wellbeing. In the context of immigrant experiences, this study conceptualizes healthcare access barriers, including financial, structural, and cognitive obstacles, as secondary stressors that mediate the relationship between economic hardship and psychological outcomes. The study also examines the potential protective role of social support in buffering these relationships.
The study addresses two primary research questions:H1:Greater economic hardship will be associated with poorer outcomes in both domains; H2: healthcare access barriers will mediate the relationship between economic hardship and mental health outcomes, such that increased economic hardship leads to greater healthcare barriers, which in turn predict higher levels of depression and anxiety
Method
This study employed a cross-sectional, correlational design using self-report survey methodology. Data was collected from April 2025 to June 2025 through online questionnaires in English and Spanish distributed via Google Forms. The main survey through which responses were received were in English, while an alternate survey was offered in Spanish through Google Translate.
Participants
Participants were recruited through convenience and snowball sampling between April 8th, 2025 and June 28th, 2025. Recruitment strategies included: (1) posting flyers in local parishes and at school, (2) emails to former families of classmates, and (3) word of mouth. Eligible participants included individuals aged 18 or older who self-identified as first-generation immigrants (defined as foreign-born individuals who moved to the United States). Of 58 individuals who accessed the survey link, 57 completed sufficient data for inclusion (response rate = 98.3%). Participants received no compensation for participation.
The final sample consisted of 58 participants, with 57 providing complete data for the primary analyses (1 participant excluded due to missing data). As shown in Table 1, participant ages ranged from 17 to 55 years (M = 33.19, SD = 12.26). The sample was diverse across multiple demographic characteristics. The majority of participants identified as female (n = 38, 67.9%), with 19 participants identifying as male (33.9%). One participant had missing gender data. Regarding sexual orientation, the vast majority identified as heterosexual (n = 47, 82.5%), followed by bisexual (n = 7, 12.3%). Gay and queer participants each comprised 1.8% of the sample (n = 1 each), with one participant providing missing data. The sample was predominantly Asian (n = 34, 59.6%), followed by White participants (n = 17, 29.8%). Black participants comprised 3.5% of the sample (n = 2), and Hispanic participants comprised 7.0% (n = 4). The detailed ethnicity breakdown revealed substantial diversity, with Korean participants being the largest single ethnic group (n = 12, 20.7%), followed by Asian (general) (n = 9, 15.5%), White (n = 6, 10.3%), and German (n = 4, 6.9%). The remaining participants represented 18 different ethnic backgrounds, reflecting the multicultural nature of the sample.
Participants demonstrated high levels of educational achievement. The largest group held Bachelor’s degrees (n = 25, 43.1%), followed by Master’s degrees (n = 14, 24.1%) and doctoral degrees (n = 8, 13.8%). High school education was reported by 6 participants (10.3%), while 2 participants (3.4%) had secondary education, 2 had Associate’s degrees (3.4%), and 1 participant (1.7%) reported middle school education as their highest level. Regarding nativity status, US citizens comprised the largest group (n = 23, 39.7%), followed by equal proportions of permanent residents and participants who preferred not to disclose their status (n = 12 each, 20.7%). Non-immigrants represented 19.0% of the sample (n = 11). Notably, no participants identified as undocumented immigrants. English proficiency was generally high, with the majority reporting fluent English skills (n = 35, 61.4%). Advanced proficiency was reported by 11 participants (19.3%), intermediate by 8 participants (14.0%), and beginner level by 3 participants (5.3%). One participant had missing English proficiency data.
Procedure
Participants were recruited through family members, community outreach, and reaching out to other professors working with immigrant populations. Eligible participants included: 1) To be the age of 18 or over and 2) To be part of an immigrant population. Each survey took approximately 15 minutes to complete. Informed consent was obtained electronically from all participants prior to the surveys.
Measures
Economic Strain. The Economic Strain Questionnaire26 assesses financial hardship through nine items rated on a 5-point Likert scale (1 = never, 2 = rarely, 3 = sometimes, 4 = often, 5 = always). Sample items include: “How often do you cut back on social activities or entertainment?” and “How often do you postpone major household purchases?” Items measure behavioral adaptations to economic difficulties, including reduced spending on necessities and social activities. Total scores are calculated by summing all items (range: 9-45), with higher scores indicating greater economic strain. Scores of 9-18 indicate low strain, 19-27 moderate strain, and 28-45 high strain. While originally developed with U.S. samples, the ESQ has been successfully used with immigrant populations27. The internal consistency was excellent (α = .90).
Mental Health. Depression symptoms were measured using the Patient Health Questionnaire28, a nine-item scale assessing symptoms over the past two weeks on a 4-point scale (0=not at all to 3=nearly every day). Scores range from 0-27, with established cutoffs for minimal (0-4), mild (5-9), moderate (10-14), moderately severe (15-19), and severe (20-27) depression.
Anxiety was assessed using the Generalized Anxiety Disorder scale, a seven-item measure rated on the same 4-point scale as the PHQ-929. Total scores range from 0-21, with established cutoffs for minimal (0-4), mild (5-9), moderate (10-14), and severe (15-21) anxiety. The PHQ-9 has demonstrated adequate reliability and validity across diverse immigrant populations30. The PHQ-9 and GAD-7 have demonstrated validity across diverse immigrant populations31,32,33. The Cronbach’s alphas for the scale demonstrated a good internal consistency (α= .88).
Healthcare Access Barriers. Healthcare access barriers were assessed using items developed based on the three domains of the Health Care Access Barriers Model34: financial, structural, and cognitive barriers. While the HCAB was originally proposed as a conceptual framework rather than a validated instrument, its domains have been widely used to guide data collection in healthcare access research. For example, researchers have successfully used the HCAB framework to develop interview guides and survey items, organize thematic analysis of qualitative data, and structure quantitative analyses of healthcare barriers (see recent application in latent class analysis of prenatal care barriers, 2025)35,36,37. Following this established approach, we developed 15 items (5 per domain) using a 5-point Likert scale.
The HCAB framework identifies three domains: financial barriers (e.g., “I cannot afford to pay for healthcare services”), structural barriers (e.g., “I have difficulty getting appointments when I need them”), and cognitive barriers (e.g., “I do not know where to go for healthcare services”). The 15-item scale uses a 5-point Likert format (1=Strongly Disagree to 5=Strongly Agree). Domain scores are calculated as means, with higher scores indicating greater barriers. The total score ranges from 15-75. Internal consistency in the current sample was excellent for the total scale (α = .95) and adequate for subscales: financial (α = .90), structural (α = .89), and cognitive (α = .92).
Multidimensional Scale of Perceived Social Support.
Perceived social support was assessed using the Multidimensional Scale of Perceived Social Support38. The MSPSS is a 12-item self-report measure designed to assess perceptions of social support adequacy from three specific sources: family (4 items; e.g., “My family really tries to help me”), friends (4 items; e.g., “I can count on my friends when things go wrong”), and significant others (4 items; e.g., “There is a special person who is around when I am in need”). Participants rated their agreement with each statement on a 7-point Likert-type scale ranging from 1 (very strongly disagree) to 7 (very strongly agree). The MSPSS has shown measurement invariance across cultural groups, supporting its use with immigrant populations39. The Cronbach’s alphas demonstrated excellent internal consistency in the study α= .97.
Data Analysis
All analyses were conducted using R statistical software40. Prior to hypothesis testing, data were examined for missing values, outliers, and assumptions of normality and linearity. Of the 58 participants who participated in the study, one participant was excluded from all analyses due to incomplete responses on the PHQ-9 depression measure, resulting in an analytic sample of N = 57. Among these 57 participants, sporadic missing data occurred on demographic variables: gender (n = 1, 1.7%), sexual orientation (n = 1, 1.7%), race/ethnicity (n = 1, 1.7%), and English proficiency (n = 1, 1.7%). All 57 participants provided complete data on primary study variables (economic stress, depression, anxiety, healthcare access barriers, and social support). Visual inspection revealed no systematic patterns of missingness. Given that missing data represented < 2% of the total dataset and was limited to demographic covariates rather than primary variables, listwise deletion was deemed appropriate. For regression analyses including demographic covariates, this resulted in sample sizes ranging from N = 56-57 depending on the specific model.
Descriptive statistics and bivariate correlations were computed for all study variables to examine patterns of association and identify potential multicollinearity issues. To test whether economic hardship predicts mental health outcomes, we conducted two hierarchical multiple regression analyses (one for depression, one for anxiety). In Step 1, demographic covariates were entered: age, gender (dummy coded: 0 = male, 1 = female), race/ethnicity (three dummy codes with Asian as reference: White, Black, Hispanic), education, and nativity status (dummy coded: 0 = non-citizen, 1 = US citizen). Based on theoretical considerations and previous research on immigrant mental health, the following covariates were included in all models: age, gender (dummy coded with male as reference), race/ethnicity (dummy coded with Asian as reference), education level (treated as ordinal), and nativity status (dummy coded with US citizen as reference)41. Missing data were handled using listwise deletion for the primary analyses. To test mediation effects, a mediation package in R was used. Mediation was tested separately for each barrier type (financial, structural, cognitive) predicting each outcome (depression, anxiety).
Results
Preliminary Analyses
Descriptive statistics and correlations among study variables are presented in Table 1. The final analytic sample consisted of 57 participants. One participant from the initial sample of 58 was excluded due to incomplete responses on the PHQ-9 depression measure, which was required for primary analyses. Examination of the correlation matrix revealed expected patterns, with economic stress significantly correlated with both depression (r = .46, p < .001) and anxiety (r = .30, p < .05). Healthcare barriers showed strong positive correlations with economic stress (r = .55, p < .001) and moderate correlations with mental health outcomes (depression r = .51, p < .001; anxiety r = .48, p < .001). Social support demonstrated expected negative correlations with economic stress (r = -.42, p < .01) and mental health symptoms (see Table 2).
Hypothesis 1: Economic Stress and Mental Health Outcomes
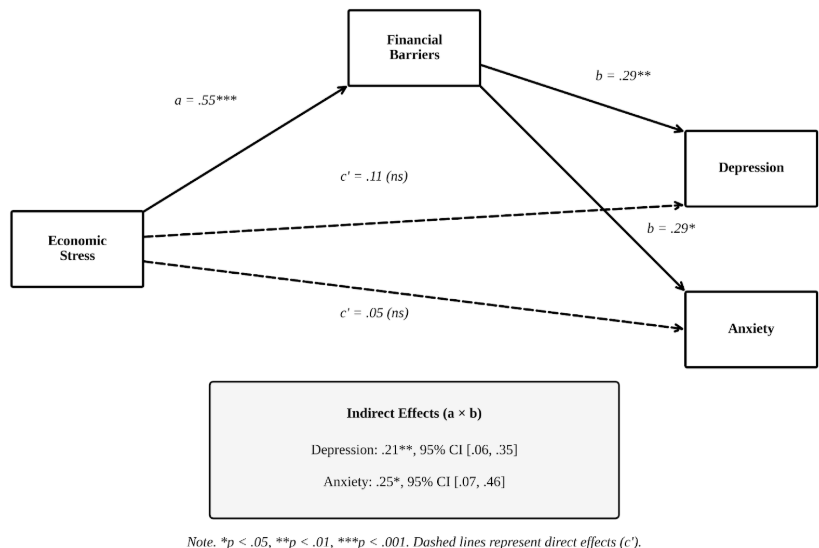
Hierarchical regression analyses controlling for age, gender, race, education, and nativity status revealed differential effects of economic stress on mental health outcomes. Economic stress significantly predicted depression symptoms (β = .23, SE = .10, p = .02), supporting our first hypothesis for depressive outcomes (See Figure 1). The model explained 50.3% of the variance in depression (R² = .50, F(9,47) = 5.29, p < .001).
However, economic stress did not significantly predict anxiety symptoms when covariates were included (β = .17, SE = .123, p = .17). The anxiety model explained 34.4% of the variance (R² = .34, F(9,47) = 2.73, p = .01), with significant effects primarily attributable to demographic factors rather than economic stress.
Hypothesis 2: Healthcare Access Barriers as Mediators
Mediation analyses using bootstrap procedures (1,000 simulations) provided strong support for healthcare barriers as mediators of the economic stress-mental health relationship, with important distinctions across barrier types. As shown in Figure 1, financial barriers emerged as the strongest mediator. For depression, the indirect effect was significant (mediated effect = .21, 95% CI [.06, .35], p = .01), with financial barriers accounting for approximately 89% of the total effect of economic stress on depression. Similarly, financial barriers significantly mediated the economic stress-anxiety relationship (mediated effect = .25, 95% CI [.07, .46], p = .02). Structural barriers showed mixed mediation effects. While the mediation was marginally significant for depression (mediated effect = .15, 95% CI [-.01, .31], p = .07), it reached significance for anxiety (mediated effect = .21, 95% CI [.01, .39], p = .04). Cognitive barriers did not demonstrate significant mediation effects for either depression (mediated effect = .06, 95% CI [-.05, .26], p = .29) or anxiety (mediated effect = .11, 95% CI [-.03, .34], p = .13).
Healthcare Barrier Types: Differential Effects
When examining specific barrier types simultaneously, financial barriers consistently emerged as the strongest predictor across models. In the comprehensive model including all barrier types, only financial barriers remained a significant predictor of both depression (β = .29, p = .01) and anxiety (β = .29, p = .04) while controlling for economic stress and demographic covariates.
Social Support Effects
Contrary to expectations, social support did not demonstrate significant protective effects in controlled analyses. Neither total social support nor specific support types (family, friend, significant other) showed significant associations with mental health outcomes when economic stress and demographic factors were controlled (all p > .05).
Covariate Effects
Several demographic factors emerged as significant predictors. Age demonstrated a protective effect against depression (β = -.02, p = .01), with older participants reporting fewer depressive symptoms. Race showed significant effects, with Black (β = 1.14, p = .01) and Hispanic (β = .78, p = .01) participants reporting significantly higher depression levels compared to Asian participants. For anxiety, Hispanic participants showed elevated symptoms (β = .82, p = .03), and White participants also demonstrated higher anxiety levels (β = .55, p = .02) relative to Asian participants.
The racial/ethnic differences found here warrant cautious interpretation, particularly considering the small size of the Black (n = 2) and Hispanic (n = 4) subgroups represented in the study, estimates of effects for these two subgroups may be less stable or more likely to reflect random fluctuations caused by individual differences. Therefore, the results presented here can be viewed as an initial trend and that further studies involving larger and more representative samples are needed to confirm the results presented here.
Model Comparisons. Comparison of controlled versus uncontrolled models revealed that demographic covariates substantially improved model fit and provided more conservative estimates of economic stress effects. The inclusion of covariates increased explained variance for depression from R² = .21 (uncontrolled) to R² = .50 (controlled), demonstrating the importance of accounting for demographic factors in immigrant mental health research.
Discussion
This study examined the relationships between economic hardship, healthcare access barriers, and mental health outcomes among immigrants in the United States. The findings provide partial support for our first hypothesis and strong support for second hypothesis, while also raising unexpected questions about the protective role of social support and demographic influences on mental health outcomes
Economic Hardship and Mental Health Outcomes
Economic stress emerged as a significant predictor of depression symptoms but not anxiety symptoms when demographic covariates were controlled. The differential effects across mental health domains suggest that economic hardship operates through distinct pathways for depression versus anxiety. For depression, the significant relationship is consistent with Pearlin’s Stress Process Model5, which posits that economic strain generates cascading effects on psychological wellbeing through resource depletion and chronic worry about basic needs. The findings are consistent with prior literature that support ,immigrant families often experience compounding stressors that heighten vulnerability to depressive outcomes6. The persistence of this relationship after controlling for demographic factors indicates that economic stress exerts an independent influence on depressive symptoms among immigrant populations. However, this interpretation should be treated cautiously, as the study design cannot determine whether economic strain precedes changes in depressive symptoms or whether individuals experiencing greater depression perceive their economic circumstances more negatively.
The absence of a significant association between economic stress and anxiety challenges assumptions about uniform effects of financial strain across mental health domains. This pattern is consistent with research finding heterogeneity in how immigrant groups manifest psychological distress15, suggesting that anxiety may be more strongly influenced by factors not captured in our economic stress measure, such as discrimination experience, uncertainty about legal status, or other stressors not directly related to financial strain42. The null finding for anxiety may reflect several possibilities: anxiety symptoms might be more strongly influenced by factors not captured in our economic stress measure, such as discrimination experiences, uncertainty about legal status, or acculturative stressors.
Alternatively, anxiety may manifest differently across cultural groups, with some immigrant populations expressing distress through somatic complaints or other symptoms not captured by the GAD-7. Cultural adjustment processes and mental health stigma may also contribute to these disparities, given that norms surrounding emotional expression and resilience differ widely across immigrant communities. For example, collectivist cultures may emphasize endurance and self-reliance, which discourages open acknowledgement of anxiety systems. On the other hand, other groups may also rely on religious or familial coping strategies that buffer psychological distress but also delay clinical intervention. These culturally shaped patterns of expressing and managing distress may influence how individuals perceive formal treatment, which creates a natural link between cultural stressors and the health care system. As a result, cultural norms surrounding help-seeking may interact with structural factors, shaping the extent to which individuals ultimately engage with or avoid health services. Furthermore, intergroup disparities in access to culturally competent care further reinforce these patterns, as groups who face higher stigma or lower familiarity with Western mental health ideals are generally less likely to report or seek treatment for anxiety.
The divergent findings for depression versus anxiety highlight the importance of domain-specific approaches to understanding immigrant mental health rather than assuming homogeneous effects across all psychological outcomes. The divergent findings for depression versus anxiety potentially highlight the importance of domain-specific approaches to understanding immigrant mental health rather than assuming homogeneous effects across all psychological outcomes.
Connecting this work to existing theories of immigrant well-being, particularly the Stress Process Model5, may enhance understanding of the results reported in this study. According to the Stress Process Model, primary stressors (e.g., economic hardship) lead to the emergence of secondary stressors like family conflict or lack of access to healthcare, which then affect psychological health. As such, the current study’s results support Pearlin’s model in that economic hardship is the initial stressor and leads to a chain reaction of psychosocial and structural problems that together greatly increase an immigrant’s risk for developing depressive disorders; in addition, healthcare access barriers were found to be mediators of the relationship between economic hardship and depression; thus, they demonstrate the second form of stress proliferation described by Pearlin.
Furthermore, without acknowledging the role of acculturation-related stressors, it would be difficult to fully comprehend how immigrants adapt to their new society. According to Berry’s Acculturation Theory43, there are many different types of variables that affect how an individual experiences acculturation. These include language barriers, differences in cultural values, removal of supportive relationships, and changes to family dynamics and responsibilities. The combination of these stressors may indeed interact with the effects of economic stressors and may result in more intense psychological impact. For example, having limited English proficiency increases financial stress due to fewer job opportunities; whereas, being unfamiliar with a culture reduces cognitive access to, or structural barriers in understanding, available medical resources. Some cultural orientations (e.g., familismo or collectivism) can protect from such stressors but may also be weakened due to the sharing of these socio-economic strains throughout the entire community.
By using both sets of theories together, we have created a better way to understand what our study found. Economic hardship could be considered a structural primary stressor whereas acculturative stressors would be the cultural and interpersonal stressors that would affect how people view, cope or deal with financial strain. All three processes would assist us in understanding the relationship between economic hardship and depression through healthcare barriers and also would provide insight into the greater dependence on cultural/contextual stressors we did not account for in this model to help define the nature of anxiety. Using this combined framework gives support to developing culturally appropriate interventions that would encompass both structural inequalities as well as acculturative stressors.
It is important to note that the cross-sectional nature of this study precludes understanding how these relationships unfold dynamically across settlement stages. The observed associations may vary considerably depending on immigrants’ length of residence and position in the acculturation process, limitations discussed in detail below.
The inclusion of demographic covariates substantially altered the observed relationships between economic stress and mental health outcomes, underscoring the importance of considering these factors when examining immigrant mental health. The model comparison revealed that accounting for age, gender, race/ethnicity, education, and nativity status increased explained variance in depression from R² = .21 to R² = .50, suggesting that these demographic characteristics play a crucial role in shaping how economic hardship translates into psychological distress. Age demonstrated a protective effect, suggesting that older immigrants may have developed more effective coping strategies or accumulated resources that buffer against depression despite economic challenges. Education level also showed a positive association with depression, which may reflect a different phenomenon- highly educated immigrants may experience greater status incongruence when their credentials are not recognized in the U.S. labor market, leading to frustration and depressive symptoms independent of absolute economic hardship.
The pronounced racial/ethnic differences observed (with Black and Hispanic participants reporting higher depression than Asian participants) may suggest that economic stress operates within broader contexts of systemic discrimination and differential access to resources. These demographic factors do not merely confound the economic stress-mental health relationship; rather, they may moderate these effects such that economic hardship has differential impacts depending on immigrants’ social positioning.
Notably, while social support was tested as a potential protective factor, it did not demonstrate significant buffering effects in controlled analyses. This may suggest that social resources alone may be insufficient to mitigate the mental health consequences of economic hardship when structural barriers (particularly healthcare access barriers) remain in place. Length of residence in the United States was not assessed in this study but represents an important consideration for future research, as it may influence both the severity of economic strain, through employment stability and wage progression, and access to healthcare resources through acquisition of insurance and knowledge of available services. Future studies should examine whether the mediating role of healthcare barriers varies by duration of U.S. residence.
It should however be noted that the racial or ethnic observations contained in this analysis should only be viewed as indicators of potential future research outcomes due to the small sample size of Black and of Hispanic participants; thus any comparisons made between these two groups are likely to be highly variable and not reliably representative of the overall population. Therefore, these results should be understood as early indicators of potential differences rather than definitive proof of disparities at the population level.
Healthcare Access as Mediating Pathways
The mediation analyses provided robust evidence for healthcare access barriers as key mechanisms linking economic hardship to mental health outcomes, offering support for the stress process model’s emphasis on how primary stressors create secondary stressors that become independent pathways to poor outcomes5. Financial barriers accounted for nearly 89% of the total effect of economic stress on depression and demonstrated significant mediation for both depression and anxiety. These mediational patterns should not be interpreted as evidence of causal pathways, since cross-sectional mediation can reflect statistical associations rather than directional processes. This finding supports the stress process model’s emphasis on how primary stressors create secondary stressors that become independent pathways to poor outcomes. The prominence of financial barriers specifically aligns with extensive literature demonstrating that healthcare affordability represents the most significant obstacle to immigrant healthcare access16,11.
The differential mediation effects across barrier types reveal important nuances in how healthcare access influences immigrant mental health. While financial barriers consistently mediated relationships with both mental health outcomes, structural barriers showed mixed effects, reaching significance only for anxiety. This pattern suggests that different types of secondary stressors may have varying impacts across mental health domains. Structural obstacles such as transportation difficulties, appointment availability, and system navigation challenges may create particular uncertainty and unpredictability that manifests as anxiety-related concerns rather than depressive symptoms.
Notably, cognitive barriers such as lack of knowledge about available services did not demonstrate significant mediation effects. This finding diverges from research highlighting information deficits as critical barriers, but may reflect characteristics of our highly educated sample, which likely possessed greater healthcare literacy than typical immigrant populations11. This suggests that the relative importance of different secondary stressors may vary across immigrant populations with different resources and characteristics.
Beyond the substantive findings, our study extends previous applications of the HCAB framework by demonstrating strong internal consistency when operationalized as survey items. While previous research has primarily used the HCAB as a conceptual framework for organizing qualitative findings or developing interview guides44,37, our study provides initial psychometric evidence that the three domains can function reliably as quantitative measures. This contribution addresses a gap in the literature by moving toward a standardized assessment tool for healthcare access barriers among immigrant populations.
Reconsidering Social Support in Immigrant Mental Health
Contrary to extensive literature documenting the protective effects of social support among immigrant populations, neither total social support nor domain-specific support from family, friends, or significant others showed significant associations with mental health outcomes when economic and demographic factors were controlled45,46. This finding challenges theoretical models that position social support as a primary protective factor for immigrant mental health and diverges from research highlighting strong family and faith-based networks as critical buffers for immigrant mental health.
Several explanations may account for this unexpected result. When economic hardship affects entire immigrant communities, the capacity of network members to provide meaningful assistance becomes limited, as suggested by research on strained immigrant support systems20. Social support may lose its protective value when potential providers face similar financial constraints, creating what could be termed “stressed networks” where traditional reciprocity patterns break down. As noted by Jacquez and colleagues (2024), immigrants often report less emotional support compared to U.S.-born adults, with many “rarely” or “never” having someone to confide in18.
The null findings may also reflect measurement limitations of the MSPSS in capturing culturally specific forms of support particularly relevant to immigrant populations. Traditional scales may not adequately assess collective obligations (familismo), religious community assistance, or transnational support networks that have been identified as critical resources in Latino immigrant communities22. Future research should consider culturally adapted measures that capture these distinctive support patterns.
Demographic Disparities and Cultural Considerations
Demographic differences emerged as robust predictors of mental health outcomes, with age demonstrating protective effects against depression and significant racial/ethnic disparities evident across both outcomes. Older participants reported fewer depressive symptoms, consistent with findings that age can serve as a protective factor against mental illness6. However, this finding should be interpreted cautiously given that older immigrants in our sample may represent a particularly resilient subset who successfully navigated immigration challenges.
The racial and ethnic disparities were also pronounced: Black and Hispanic immigrants reported higher depression, while Hispanic and White participants reported higher anxiety compared to Asian immigrants. These findings are consistent with research documenting persistent racial disparities in mental health outcomes and service utilization12. The patterns observed support research finding that mental health outcomes differ considerably by race and ethnicity among immigrant populations, with some groups showing resilience while others face heightened risk42.
These disparities likely reflect complex interactions among discrimination experiences, cultural factors, migration circumstances, and access to resources that vary significantly across immigrant groups. For instance, Asian immigrants in our sample may have benefited from different migration pathways (e.g., educational or employment-based immigration) that provide greater economic stability and social resources compared to refugees or asylum seekers who may be overrepresented among other ethnic groups.
Implications
These findings have direct implications for clinical practice and policy development. Given that financial barriers mediated approximately 89% of the economic stress-depression relationship, healthcare providers should prioritize screening immigrant patients for economic stressors and financial access challenges when assessing depression risk11. The domain-specific effects observed suggest that depression may be more responsive to economic interventions than anxiety, which appears more influenced by demographic and potentially cultural factors not measured in this study. The strong mediation effects of healthcare access barriers suggest that interventions targeting healthcare affordability could contribute to significant mental health benefits for immigrant populations.
Policy initiatives should also prioritize reducing financial barriers through expanded insurance coverage, sliding-fee scales, and enhanced funding for community health centers serving immigrant populations17. The prominence of structural barriers as mediators of anxiety symptoms also suggests that improvements in healthcare system navigation, transportation assistance, and appointment flexibility may be particularly beneficial for reducing anxiety-related distress for this population.
Immigration policy itself may play a crucial role in mental health outcomes. Policies that create fear of deportation or limit access to public benefits may exacerbate both economic stress and healthcare access barriers. Mental health advocacy should include immigration policy reform that recognizes the health implications of legal uncertainty and exclusion from social services.
The racial/ethnic disparities observed in mental health outcomes suggest a need for culturally responsive approaches that address the unique stressors and resources of different immigrant groups12. The finding that Black and Hispanic participants reported higher depression levels while Hispanic and White participants showed elevated anxiety compared to Asian participants suggests that one-size-fits-all interventions are unlikely to be effective. Mental health services should be tailored to address the specific risk and protective factors operating within different ethnic communities.
The unexpected absence of protective effects for social support, despite controlling for other factors, suggests that traditional social support interventions may be less effective than structural approaches targeting healthcare access. Rather than focusing primarily on building social connections, clinical interventions might be more effective when they directly address financial barriers to care and help families navigate healthcare systems. Community-based programs should consider how economic stressors may strain support networks and develop approaches that strengthen communities’ collective capacity to address financial healthcare barriers20.
Limitations
Several critical statistical limitations constrain the interpretation and generalizability of these findings. Most fundamentally, the mediation analyses conducted in this study suffer from the inherent limitations of cross-sectional data. While bootstrap procedures were employed to generate confidence intervals for indirect effects, these statistical techniques cannot address the core methodological issue that temporal precedence among variables cannot be established from concurrent measurements47. The mediation models assume that economic stress precedes healthcare barriers, which in turn precede mental health outcomes, but this temporal ordering cannot be verified with the current data.
It remains equally plausible that mental health problems contribute to economic difficulties, that healthcare barriers lead to economic stress, or that unmeasured third variables influence all relationships simultaneously. The significant indirect effects observed may therefore reflect statistical associations rather than true mediational processes, limiting the causal inferences that can be drawn from these analyses. Yet, the relationships observed in this study may differ substantially depending on length of residence, acculturation stage, and position in the settlement process. For instance, newly arrived immigrants may face acute economic hardship but maintain protective cultural resources, while long-term residents may have achieved economic stability but experience eroded social support networks or cumulative discrimination effects.
Healthcare access barriers may also shift over time as immigrants gain familiarity with the system, acquire insurance, or conversely, become disillusioned with discriminatory experiences. Future research should employ longitudinal designs that track immigrants across multiple time points.
The relatively small sample size of 58 participants presents additional statistical constraints that may have influenced the pattern of results obtained. Power analyses conducted post hoc suggest that the study had adequate power ( > .80) to detect large effect sizes but insufficient power to detect small to moderate effects that may nonetheless be theoretically and practically meaningful. This limitation is particularly relevant for interpreting the non-significant relationship between economic stress and anxiety symptoms. The observed effect size, while not statistically significant, approaches conventional thresholds for small effects and may represent a meaningful association that was not detected due to insufficient statistical power.
Similarly, the marginal significance of structural barriers as mediators of the economic stress-depression relationship may reflect power limitations rather than absence of effect. Future studies with larger samples would be better positioned to detect these potentially important but modest associations.
The sample size also prevented more sophisticated analytical approaches that may have provided additional insights into the relationships of key variables. Additionally, the small sample precluded examination of potential moderating effects of demographic characteristics such as length of residence, legal status, or cultural background variables that may influence the strength or direction of the observed relationships. These analytical limitations restrict understanding of the boundary conditions under which the identified associations hold and limit the ability to develop more nuanced theoretical models of immigrant mental health processes.
Furthermore, while the measures demonstrated strong internal consistency, potential cultural limitations should be acknowledged. For example, the MSPSS may not fully capture culturally-specific support forms such as familismo or faith-based community support. Also, 38.6% of participants reported less than fluent English proficiency, which may have affected their interpretation of items. Cultural variations in expressing psychological distress (e.g., somatization) may not be fully captured by Western-developed measures.
Moreover, the exclusive reliance on self-report measures introduces the possibility of shared method variance inflating the observed correlations among study variables. This concern is particularly important given that economic stress, healthcare barriers, and mental health symptoms were all assessed through participant self-report, potentially leading to artificially inflated associations due to common response biases, social desirability effects, or individual differences in response styles. Future research would benefit from incorporating objective measures of economic status (e.g., income verification, employment records) and healthcare utilization patterns to complement self-report assessments and provide convergent validity for the observed relationships.
There is also a limitation relating to the demographic characteristics of the sample being studied. It contained a very small number of different racial/ethnic subgroups, particularly Black immigrants (N = 2) and Hispanic immigrants (N = 4). Therefore, the results for these groups must be taken with great caution. The numbers for these subgroups do not provide enough statistical power to draw firm conclusions about differences; therefore, it is important for future studies to actively recruit larger and more diverse samples in order to determine the level of racial/ethnic variability with greater statistical confidence.
Conclusion
The present study demonstrates that economic hardship among immigrants operates through healthcare access barriers to influence mental health outcomes, with financial barriers serving as the primary mechanism linking economic stress to psychological distress. This phrasing reflects observed associations, and the results should not be interpreted as demonstrating that economic hardship or healthcare barriers directly cause changes in mental health. The domain-specific effects observed for depression versus anxiety highlight the complexity of immigrant mental health processes and the need for nuanced theoretical and intervention approaches. The prominence of demographic factors in predicting mental health outcomes underscores persistent inequalities that require targeted attention in both research and practice.
These findings ultimately support the development of structural interventions targeting healthcare accessibility as a means of promoting mental health equity among immigrant populations. While limitations in study design prevent definitive causal conclusions, the patterns observed provide valuable insights for developing more effective approaches to supporting immigrant mental health in the context of economic adversity. Based on these conclusions, future policy initiatives should prioritize measures that promote inclusivity such as job training programs, subsidized employment, expanded access to affordable and culturally competent mental health services, and language support programs. Such interventions would directly address the economic and systemic barriers identified in the study, advancing both mental health outcomes and social inclusion among immigrant communities
| Characteristic | n | % |
| Total Sample | 58 | 100.0 |
| Age | ||
| M (SD) | 33.19 (13.74) | |
| Range | 17-55 years | |
| Gender | ||
| Male | 19 | 33.9 |
| Female | 38 | 67.9 |
| Missing | 1 | 1.8 |
| Sexual Orientation | ||
| Heterosexual | 47 | 82.5 |
| Bisexual | 7 | 12.3 |
| Gay | 1 | 1.8 |
| Queer | 1 | 1.8 |
| Missing | 1 | 1.8 |
| Race | ||
| Asian | 34 | 59.6 |
| White | 17 | 29.8 |
| Black | 2 | 3.5 |
| Hispanic | 4 | 7.0 |
| Missing | 1 | 1.8 |
| Education Level | ||
| Secondary Education | 2 | 3.4 |
| Middle School | 1 | 1.7 |
| High School | 6 | 10.3 |
| Bachelor’s Degree | 25 | 43.1 |
| Associate’s Degree | 2 | 3.4 |
| Master’s Degree | 14 | 24.1 |
| Doctoral Degree | 8 | 13.8 |
| Nativity Status | ||
| US Citizen | 23 | 39.7 |
| Permanent Resident | 12 | 20.7 |
| Non-immigrant | 11 | 19.0 |
| Prefer not to say | 12 | 20.7 |
| English Proficiency | ||
| Beginner | 3 | 5.3 |
| Intermediate | 8 | 14.0 |
| Advanced | 11 | 19.3 |
| Fluent | 35 | 61.4 |
| Missing | 1 | 1.8 |
| Geographic Region | ||
| North Jersey | 13 | 22.4 |
| New York | 9 | 15.5 |
| Europe | 9 | 15.5 |
| California | 6 | 10.3 |
| Other locations | 21 | 36.2 |
| Variable | M | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 |
| 1. Age | 33.19 | 12.26 | |||||||||||
| 2. Female | 0.67 | 0.48 | -.04 | ||||||||||
| 3. White | .40 | 0.46 | -.31* | -.03 | |||||||||
| 4. Black | .04 | 0.19 | .20 | .07 | -.12 | ||||||||
| 5. Hispanic | 0.09 | 0.11 | .06 | -.05 | -.18 | -.52 | |||||||
| 6. Education attainment | 4.69 | 1.51 | .33* | .10 | .19 | -.21 | |||||||
| 7.Nativity | 0.21 | 0.41 | -.03 | .09 | .04 | .14 | – .18 | ||||||
| 8. Economic stress | 2.86 | 0.85 | -.23 | .25 | .13 | .16 | .03 | .06 | -.09 | ||||
| 9. Depression | 11.28 | 05.69 | -.33* | .25 | .09 | .26 | .32* | -.20 | .04 | .46** | |||
| 10. Anxiety | 9.37 | 04.79 | -.15 | .22 | .23 | .17 | .28* | -.12 | .11 | .30* | .84*** | ||
| 11. Healthcare barrier | 2.69 | 1.01 | -.04 | .04 | .05 | .18 | .13 | -.08 | -.02 | .55** | .51** | .48** | |
| 12. Social support | 5.27 | 1.49 | .20 | .14 | -.11 | -.25 | .06 | .13 | .01 | – .42** | -.22 | – .13 | -.51 |
Note. M and SD are used to represent mean and standard deviation, respectively. Values in square brackets indicate the 95% confidence interval for each correlation. The confidence interval is a plausible range of population correlations that could have caused the sample correlation (Cumming, 2014). * indicates p < .05. ** indicates p < .01. Depression and anxiety scores are presented as mean item scores. Depression (PHQ-9): Cutoffs for total scores are 0-4 (minimal), 5-9 (mild), 10-14 (moderate), 15-19 (moderately severe), 20-27 (severe). The sample mean of 1.28 per item corresponds to a total score of 11.5, indicating moderate depression. Anxiety (GAD-7): Cutoffs for total scores are 0-4 (minimal), 5-9 (mild), 10-14 (moderate), 15-21 (severe). The sample mean of 1.37 per item corresponds to a total score of 9.6, indicating mild anxiety.
References
- U.S. Census Bureau. (2023). Current Population Survey, Annual Social and Economic Supplements [↩]
- Geiger, Abigail. “What the Data Says about Immigrants in the U.S.” Pew Research Center, 21 Aug. 2025, www.pewresearch.org/short-reads/2025/08/21/key-findings-about-us-immigrants/ . [↩]
- Department of Homeland Security. (2023). Yearbook of Immigration Statistics: 2022. [↩]
- Koczan, Zsoka, et al. “The Impact of International Migration on Inclusive Growth: A Review.” IMF Working Papers, vol. 2021, no. 088, 19 Mar. 2021, https://doi.org/10.5089/9781513571966.001.A001. [↩] [↩]
- Pearlin, L. I., Lieberman, M. A., Menaghan, E. G., & Mullan, J. T. (1981) – The Stress Process. Journal of Health and Social Behavior, 22(4), 337-356. [↩] [↩] [↩] [↩] [↩]
- Zhang, Liwei, et al. “To Unfold the Immigrant Paradox: Maltreatment Risk and Mental Health of Racial-Ethnic Minority Children.” Frontiers in Public Health, vol. 9, 17 Feb. 2021, https://doi.org/10.3389/fpubh.2021.619164. [↩] [↩] [↩] [↩]
- Massey, Douglas S, and Emilio A Parrado. “International Migration and Business Formation in Mexico.” Social Science Quarterly, vol. 79, no. 1, 1998, pp. 1–20. JSTOR, www.jstor.org/stable/42863761,. [↩]
- Fernandez, Isabella. “Radicalization and Exodus: Analyzing the Impact of Governmental Extremism on Migration Patterns in Venezuela.” Silicon Valley Sociological Review, vol. 23, no. 5, 27 Aug. 2025. Scholar Commons. [↩]
- Robinson, William I. Saskia Sassen and the Sociology of Globalization: A Critical Appraisal. 1 Mar. 2009. [↩]
- Cespedes-Reynaga, Nikita. “A Quantitative General Equilibrium Approach to Migration, Remittances, and Brain Drain.” Macroeconomic Dynamics, vol. 29, 18 Sept. 2024, https://doi.org/10.1017/s1365100524000269. [↩]
- Hacker, Karen, et al. “Barriers to Health Care for Undocumented Immigrants: A Literature Review.” Risk Management and Healthcare Policy, vol. 8, no. PMC4634824, 30 Oct. 2015, p. 175, https://doi.org/10.2147/rmhp.s70173. [↩] [↩] [↩] [↩] [↩]
- Derr, Amelia Seraphia. “Mental Health Service Use among Immigrants in the United States: A Systematic Review.” Psychiatric Services, vol. 67, no. 3, 15 Dec. 2015, pp. 265–274, https://doi.org/10.1176/appi.ps.201500004. [↩] [↩] [↩]
- Teruya, Stacey A, and Shahrzad Bazargan-Hejazi. “The Immigrant and Hispanic Paradoxes: A Systematic Review of Their Predictions and Effects.” Hispanic journal of behavioral sciences vol. 35,4 (2013): 486-509. doi:10.1177/0739986313499004 [↩]
- Williams, D. R., Haile, R., González, H. M., Neighbors, H., Baser, R., & Jackson, J. S. (2007). The Mental Health of Black Caribbean Immigrants: Results from the National Survey of American Life. American Journal of Public Health, 97(1), 52–59. https://doi.org/10.2105/ajph.2006.088211 [↩]
- Takeuchi, David T., et al. “Immigration and Mental Health: Diverse Findings in Asian, Black, and Latino Populations.” American Journal of Public Health, vol. 97, no. 1, 1 Jan. 2007, pp. 11–12, https://doi.org/10.2105/AJPH.2006.103911. [↩] [↩]
- Chandler, Juliet T., et al. ““No Me Ponían Mucha Importancia.”” Advances in Nursing Science, vol. 35, no. 2, Apr. 2012, pp. E24–E36, https://doi.org/10.1097/ans.0b013e31825373fe. [↩] [↩]
- Rivers, Patrick A., and Fausto G. Patino. “Barriers to Health Care Access for Latino Immigrants in the USA.” International Journal of Social Economics, vol. 33, no. 3, Mar. 2006, pp. 207–220, https://doi.org/10.1108/03068290610646234. [↩] [↩]
- Jacquez, Farrah, Lisa M Vaughn, and Jamie Hardy-Besaw. “Immigrant Perspectives of Social Connection in a Nontraditional Migration Area.” Healthcare 12, no. 6 (March 19, 2024): 686–86. https://doi.org/10.3390/healthcare12060686. [↩] [↩] [↩]
- Parra-Cardona, Rubén, Ofelia Zapata, María Emerson, Reverend Jairo Sandoval-Pliego, and Deliana García. “Faith-Based Organizations as Leaders of Implementation.” Stanford Social Innovation Review 19, no. 3 (2021): 21–24. https://doi.org/10.48558/rre8-dt78. [↩]
- Kerker, Bonnie D, R. Gabriela Barajas-Gonzalez, Natalia M Rojas, Jennifer M Norton, and Laurie M Brotman. “Enhancing Immigrant Families’ Mental Health through the Promotion of Structural and Community-Based Support.” Frontiers in Public Health 12 (May 1, 2024). https://doi.org/10.3389/fpubh.2024.1382600. [↩] [↩] [↩]
- Nayak, Sameera S., Christine A. Mair, and Suliyat O. Adewuyi. “Immigrant Status and Social Ties: An Intersectional Analysis of Older Adults in the United States.” Journal of Immigrant and Minority Health, November 21, 2024. https://doi.org/10.1007/s10903-024-01644-z. [↩]
- Bekteshi, Venera. “Decoding Acculturative Stress and Psychological Distress in Mexican Immigrant Women: Insights from a Path Mediation Analysis.” BMC Women’s Health 24, no. 1 (December 27, 2024). https://doi.org/10.1186/s12905-024-03494-1. [↩] [↩]
- Choi, Sujin, and Eunjeong Kang. “Cultural Factors Related to Immigrants’ Health: A Scoping Review.” Frontiers in Public Health 13 (June 18, 2025). https://doi.org/10.3389/fpubh.2025.1606772. [↩] [↩]
- Solveig Vederhus, Eirik Myhre, Esperanza Diaz, and Liv Grimstvedt Kvalvik. “Cultural Factors Influencing COVID-19-Related Perceptions and Behavior, Seen from Immigrants’ Own Perspective – a Qualitative Study in Norway.” Archives of Public Health 82, no. 1 (July 19, 2024). https://doi.org/10.1186/s13690-024-01327-z. [↩]
- Pandey, Mamata, R. Geoffrey Maina, Jonathan Amoyaw, Yiyan Li, Rejina Kamrul, C. Rocha Michaels, and Razawa Maroof. “Impacts of English Language Proficiency on Healthcare Access, Use, and Outcomes among Immigrants: A Qualitative Study.” BMC Health Services Research 21, no. 1 (July 26, 2021): 1–13. https://doi.org/10.1186/s12913-021-06750-4. [↩]
- Lempers, Jacques D, et al. “Economic Hardship, Parenting, and Distress in Adolescence.” Child Development, vol. 60, no. 1, 1989, pp. 25–39, https://doi.org/10.2307/1131068. [↩]
- Ishii-Kuntz, M., Gomel, J. N., Tinsley, B. J., & Parke, R. D. (2010). Economic hardship and adaptation among Asian American families. Journal of Family Issues, 31(3), 407-420. [↩]
- Kroenke, Kurt, et al. “The PHQ-9: Validity of a Brief Depression Severity Measure.” Journal of General Internal Medicine, vol. 16, no. 9, 2001, pp. 606–613, https://doi.org/10.1046/j.1525-1497.2001.016009606.x. [↩]
- Spitzer, R. L., Kroenke, K., & Williams, J. B. W. (2006). APA PsycNet. Psycnet.apa.org. https://psycnet.apa.org/doiLanding?doi=10.1037%2Ft02591-000 [↩]
- Klein, E. M., Kruse, J., Löwe, B., Brähler, E., Lahmann, C., Witthöft, M., & Krakau, L. (2025). Somatic symptom severity and psychological distress among immigrants: findings from a population-based study. Annals of Medicine, 57(1), 2578726., Rodriguez, M. O., Gudino, J., Valencia, J., Rhew, I., & Ornelas, I. J. (2025). Patterns of mental health help seeking among Latina immigrant women. BMC Public Health, 25(1), 1-8. [↩]
- Familiar, I., Borges, G., Orozco, R., & Medina-Mora, M. E. (2011). Mexican migration experiences to the US and risk for anxiety and depressive symptoms. Journal of affective disorders, 130(1-2), 83–91. https://doi.org/10.1016/j.jad.2010.09.025. [↩]
- Huang, F. Y., Chung, H., Kroenke, K., Delucchi, K. L., & Spitzer, R. L. (2006). Using the Patient Health Questionnaire-9 to measure depression among racially and ethnically diverse primary care patients. Journal of general internal medicine, 21(6), 547–552. https://doi.org/10.1111/j.1525-1497.2006.00409.x. [↩]
- Yeung, A., Fung, F., Yu, S. C., Vorono, S., Ly, M., Wu, S., & Fava, M. (2008). Validation of the Patient Health Questionnaire-9 for depression screening among Chinese Americans. Comprehensive psychiatry, 49(2), 211–217. https://doi.org/10.1016/j.comppsych.2006.06.002. [↩]
- Carrillo, J. Emilio, et al. “Defining and Targeting Health Care Access Barriers.” Journal of Health Care for the Poor and Underserved, vol. 22, no. 2, 2011, pp. 562–575, https://doi.org/10.1353/hpu.2011.0037. [↩]
- Colton, Z. A., Liles, S. M., Griffith, M. M., Stanek, C. J., Walden, J., King, A., Barnard-Kirk, T., Creary, S., & Nahata, L. (2025). Using the consolidated framework for implementation research to identify challenges and opportunities for implementing a reproductive health education program into sickle cell disease care. Journal of Pediatric Psychology, 50(1), 30–39. https://doi.org/10.1093/jpepsy/jsae031., [↩]
- Duah, J. K. (2025). Beyond Intentionality: A Latent Class Analysis of Barriers to Prenatal Care in an Explanatory Mixed Methods Study. Healthcare, 13(13), 1546. https://doi.org/10.3390/healthcare13131546. [↩]
- Santalahti, M., Sumit, K., & Perkiö, M. (2020). Barriers to accessing health care services: a qualitative study of migrant construction workers in a southwestern Indian city. BMC Health Services Research, 20(1). https://doi.org/10.1186/s12913-020-05482-1. [↩] [↩]
- Zimet, G. D., Dahlem, N. W., Zimet, S. G., & Farley, G. K. (1988). The multidimensional scale of perceived social support. Journal of Personality Assessment, 52(1), 30–41. https://doi.org/10.1207/s15327752jpa5201_2. [↩]
- Chou, K.-L. (2000). Assessing Chinese adolescents’ social support: The multidimensional scale of perceived social support. Personality and Individual Differences, 28(2), 299-307. https://doi.org/10.1016/S0191-8869(99)00098-7. [↩]
- R Core Team (2023) R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna. https://www.R-project.org/. [↩]
- Villatoro, A. P., Mays, V. M., Ponce, N. A., & Aneshensel, C. S. (2017). Perceived Need for Mental Health Care: The Intersection of Race, Ethnicity, Gender, and Socioeconomic Status. Society and Mental Health, 8(1), 1–24. https://doi.org/10.1177/2156869317718889. [↩]
- Williams, D. R., Haile, R., González, H. M., Neighbors, H., Baser, R., & Jackson, J. S. (2007). The Mental Health of Black Caribbean Immigrants: Results from the National Survey of American Life. American Journal of Public Health, 97(1), 52–59. https://doi.org/10.2105/ajph.2006.088211. [↩] [↩]
- Berry, J. W. (1997) – Immigration, Acculturation, and Adaptation. Applied Psychology: An International Review, 46(1), 5-34. [↩]
- George, S., Daniels, K., & Fioratou, E. (2018). A qualitative study into the perceived barriers of accessing healthcare among a vulnerable population involved with a community centre in Romania. International Journal for Equity in Health , 17(41). https://doi.org/10.1186/s12939-018-0753-9. [↩]
- Jacquez, Farrah, Lisa M Vaughn, and Jamie Hardy-Besaw. “Immigrant Perspectives of Social Connection in a Nontraditional Migration Area.” Healthcare 12, no. 6 (March 19, 2024): 686–86. https://doi.org/10.3390/healthcare12060686. [↩]
- Parra-Cardona, Rubén, Ofelia Zapata, María Emerson, Reverend Jairo Sandoval-Pliego, and Deliana García. “Faith-Based Organizations as Leaders of Implementation.” Stanford Social Innovation Review 19, no. 3 (2021): 21–24. https://doi.org/10.48558/rre8-dt78. [↩]
- Maxwell, S. E., & Cole, D. A. (2007). Bias in cross-sectional analyses of longitudinal mediation. Psychological methods, 12(1), 23–44. 10.1037/1082-989X.12.1.23. [↩]



{kind=link}