
Abstract
Due to differences in healthcare quality and access, cross-border healthcare is expanding quickly. This study analyzes demographic patterns, regional preferences, and symptom trends among 1,007 users of MedSeek, a digital health platform for international patients. Only cross-border seekers who specifically chose their target nation were included in the data after it was filtered. Analysis methods included Fisher’s Exact Test, Chi-square tests, descriptive statistics, and linear regression. This logistic regression analysis reveals that higher income classes and medium geographic distance significantly predict the likelihood of selecting the United States for medical treatment, underscoring the role of economic resources and travel feasibility in cross-border decisions, with the model exhibiting excellent discriminatory ability (AUC=0.879) and good calibration (Brier score=0.115). Results show that 64.6% of users sought treatment in the United States, with significant preferences among elderly (p=0.013) users, and individuals from countries with limited healthcare infrastructure such as Montenegro, Cameroon, and Sierra Leone. Middle-aged users prioritized cardiac arrhythmia, heart failure and multi organ failure, older users concentrated on diseases of liver and chronic kidney disease, and younger users were more impacted by systemic lupus erythematosus and leukemia. According to temporal trends, users were more likely to seek treatment in the United States allergic or hypersensitivity conditions of unspecified type and cardiac arrhythmia, heart failure issues. The results emphasize the necessity of more specialized service capacity and focused healthcare strategies.
Keywords: Cross-border healthcare; medical tourism; healthcare accessibility; international patients; specialized treatment; healthcare policy
Introduction
In a globalized society, health care has become a more international issue. This phenomenon of seeking care outside of the country of residence has been labeled as cross-border healthcare or medical tourism, with patients commonly seeking care abroad to gain access to specialist services and advanced technology and for affordable care1. This worldwide phenomenon has grown tremendously in the last 20 years, as the United States, along with other high-income countries, has become a leading destination for foreign patients seeking cancer, cardiac, orthopedic, and elective surgeries2. At the same time, developing economies like India, Thailand, and Mexico vigorously market themselves as low-cost destinations for global health care, only adding to this complex situation. As the number of healthcare purchasers and patients who can choose their healthcare continues to grow, the question of how these patients make decisions in those settings becomes more and more relevant for policymakers, healthcare providers, and technology developers.
While the popularity of medical tourism has undoubtedly been increasing, the research on cross-border healthcare decision-making itself is still fragmented and underdeveloped. Much of the existing literature takes a narrow focus on economic or structural factors such as affordability, availability of advanced technology, and quality of facilities3. Important as these are, they cannot fully explain the behavioral processes underlying patients’ decision-making. Patients exercising choice in new healthcare markets are confronted with a myriad of complexities – cultural and linguistic barriers, issues of trust and reputation, logistical obstacles, and ethical dilemmas of privacy and safety, to name a few. Classical models of medical decision making do not commonly account for such cross-border dilemmas. According to Shabani and Borry4, the increasing use of digital health platforms adds other factors such as patient engagement with technology, interpretation of digital advice, and negotiation of privacy issues under regulations such as the General Data Protection Regulation (GDPR) in Europe.
In addition, decision-making theories, such as bounded rationality5, prospect theory6, and discrete-choice experiments7, have rarely been applied to international healthcare in particular. While these frameworks have been used widely in domestic healthcare studies, there is little research investigating how they apply when patients are required to consider costs and risks and benefits across borders, and frequently under conditions of uncertainty. In addition, new approaches to capture real-time behavioral and demographic data by using the emerging discipline of digital phenotyping open up novel methods to explore cross-border healthcare decision-making, but to date, its use has been limited8,9. This calls to mind the urgent need to connect the dots between digital health data-driven innovations and theories of behavioral science.
This work fills these gaps through the analysis of anonymized user data from MedSeek. This custom-built mobile application assists international patients in finding and accessing health care providers across the countries. MedSeek has a unique data set that captures user behavior, preferences, and demographic profiles in real time. By correlating behavioral analytics with frameworks for decision-making, this research makes three important contributions. For one, it extends knowledge of international patients’ experiences of digital health products for high-stakes medical decisions. Second, it brings behavioral and economic decision-making models together with empirical evidence gathered through app-based research in order to derive new perspectives. Thirdly, it addresses policy and ethical concerns, especially concerning privacy, transparency, and fair access to healthcare for international patients. In doing so, this study provides a unique contribution to the academic literature as well as the practical implementation of patient-centric and intelligent digital health solutions for making informed healthcare choices across borders.
Literature Review
Cross-Border Healthcare and Medical Tourism
Cross-border healthcare has gained recognition and developed from a niche activity to a formal, structured multi-stakeholder market which connects patients with intermediaries and destination providers. Health economics has identified the following drivers of international patient travel: differences in prices; perceived quality and safety; waiting times in their home economy; availability of procedures; and cultural or linguistic connections10,2,11. Initially, medical tourism was conceptualized as non-homogeneous: parts of the business sector cover from elective low-risk procedures combined with tourism packages, to highly specialized tertiary care12,13. For the United States in particular, inbound travel tends to be centered in quaternary centers (e.g., oncologic, transplantation, advanced cardiovascular care), in which brand, results, and subspecialty reputation are the most influential of these price decision criteria10,2. These trends act as a background for information aggregation on digital platforms as well as lower search costs for globally mobile consumers.
Patient Decision Making and Preference Elicitation
Specifically, patients facing cross-border decisions are responsible for difficult trade-offs under uncertainty–the very type of decision that features of bounded rationality, heuristics, and framing effects influence preferences14,15,6. In health economics, the discrete choice experiment (DCE) has been the de facto stated preference method to quantify the value that people place on attributes such as outcomes, safety, waiting time, cost, travel time, and provider reputation16,17,18,19. DCE guidance emphasizes stringent attribute design, experimental design, and transparent reporting in evidence use to support policy and product decisions16,18,19, and evidence from hospital-choice and provider-choice settings indicates that clinical quality measures, mortality/readmission proxies, and waiting time are important20,21,22. Collectively, this literature offers a strong basis for modeling the choice of destination for medical travel as utility maximisation over a bundle of clinical and non-clinical features and for testing how digital signals (rates, sensitivity, transparency) are incorporated into those utility functions.Digital Health Platforms, Digital Phenotyping, And Online Decision Environments
Digital Health Platforms, Digital Phenotyping, And Online Decision Environments
The internet has become a central point of reference for people to seek health information, and increasingly influences the pre-treatment pathways for cross-border care. Population surveys report the mainstreaming of the use of online health information and services23. Platform affordances (search, filtering, reviews, messaging, teleconsults, price/quality transparency, etc) help lower transaction costs but also create new informational frictions and risks24,25. An emerging trend in the domain of digital health is digital phenotyping – continuous in situ measurement of behaviour using smartphones and sensors – for personalised engagement and triage26,9,27. While these techniques have been developed primarily in the context of mental and behavioral health, they apply to pre-diagnostic journeys. They may help imply intent, personalize content (e.g., destination shortlists), and get in front of the user over time. However, governance needs to keep pace with new measurement tools: structured assessments show significant shortcomings in privacy disclosures, data sharing practices, and security of consumer health apps8,28. The effectiveness of this platform (efficient, accessible) has been cautioned by the necessity for trustworthy data stewardship and integration with high-quality clinical pathways29,30,31.
Policy and Ethics: GDPR, Consent, and Algorithmic Transparency
Because digital platforms can profile sensitive states of an individual’s health, cross-border patients are subject to overlapping regulatory regimes. Within the context of the EU General Data Protection Regulation (GDPR), health and genetic data constitute special categories for which processing, transfer of data outside the EU, and secondary use for research purposes are provided with stringent conditions4. Dynamic consent represents a recently proposed ethical framework that attempts to give individuals controlled, revocable granularity of control over their data sharing and re-use. At the same time, the existence and scope of a “right to explanation” in automated decision making has become a popular topic of discussion in light of the need for algorithmic transparency and contestability32,33, in particular in cases where profiling might lead to clinical routing or pricing. I also argue that for platforms linking patients to providers in the US, the practical compliance obstacles of lawful bases for processing, data minimisation and purpose limitation, and protections for international transfers all impact user trust and, by extension, signals of engagement that platforms depend upon.
Destination Choice for Medical Travel to the United States
The destination-choice literature identifies clinical quality and experience cues (outcomes, accreditation, specialist volume), access cues (waiting time, visa/logistics, language support), and financials (price transparency, bundling, financing) as influential factors for choice10,2,13. For the US, the density of centres of excellence yields robust brand prior multiplier effects which are amplified – or mitigated – by platform features like outcomes reporting, surgeon-level volume disclosure, and live inquiry responsiveness. While the provider-choice literature in the domestic setting points to low quality and responsiveness in a population being enough to alter demand, even relatively small increases in perceived quality and responsiveness can shift demand, especially among more activated and digitally literate patients24,34. By contrast, frictions such as opaqueness in price, complexity of eligibility screening, or poor post-discharge coordination detract from destination utility. These trade-offs will be changed by digital platforms (i) by making presentations of information more uniform and thus reducing choice overload14,15, (ii) by providing trusted third-party signals (accreditation, outcomes), and (iii) by reducing time in deciding rapid tele-triage.
Synthesis and Evidence Base for the Study Hypotheses
Findings for the reviewed literature provide tentative support for four empirically testable pathways related to the study’s hypotheses. First, platform-level transparency and responsiveness should improve the likelihood that a U.S. facility makes (and stays in) a patient’s consideration set (H1) as shown by DCE evidence that information salience and other waiting time/communication attributes have a significant impact on choice16,17, 20,18,22. Second, implicit data on behaviour from digital phenotyping and engagement logs can be used to enhance match quality, but this is only possible under explicit consent and strong privacy protections that maintain trust26,35,28,9,27. Third, platform nudge options (defaults, rank-ordering, highlighted badges) will interact with cognitive biases and measurably reframe choices14,6 – prospect theory, choice architecture in a health context32,4,33 – clear GDPR-compliant governance/transparency of algorithmic logic (when applicable) This synthesis drives the design of DCE-style attribute estimations from platform interaction data for destination choice modeling while maintaining the scope of privacy-preserving analytics to balance the tradeoff between personalization and compliance.
Method
Platform design
The MedSeek platform includes a cross-platform mobile application developed for both iOS and Android using the .NET MAUI framework, allowing a unified codebase to support multiple operating systems. The app offers key functionalities such as user authentication (including login and sign-up), symptom-based searches for medical resources, and presentation of matched results with concise summaries and recommended healthcare providers. Each result includes detailed information such as the name of the hospital or physician, contact details, and geographic location to support informed decision-making. Figure 1 displays screenshots of the application interface.

Software architecture
The diagram (Figure. 8) illustrates the architecture of the MedSeek application platform, emphasizing its modular, scalable, and secure design. At the core is the main application, which adopts the MVVM (Model-View-ViewModel) pattern. The View layer comprises XAML-based user interface pages bound to the ViewModel, which manages application logic and state. The ViewModel communicates with the Model layer, which incorporates several essential services, including the Firebase Service, which responsible for user authentication and Firestore data operations; and the OpenAI Service, which provides intelligent, symptom-based medical provider recommendations. To support global accessibility, a dedicated Localization Service enables multilingual user experiences tailored to different regions.
In terms of security, the architecture includes a Credential Management module, ensuring that sensitive assets such as API keys are never exposed on the client side. These credentials are securely managed through server-side mechanisms, such as Firebase Cloud Functions, and are further protected using certification-based strategies to guarantee data integrity and trust.
The MedSeek app determines the target country for medical resource retrieval dynamically. When a user enters symptoms, the system’s AI module infers the most relevant country based on available contextual cues, including the input language, user profile data, and prior interactions. If insufficient information is available, the AI applies heuristic rules to select a likely country, with no fixed default applied. Users can override the AI-selected country prior to search execution.
This inference module was implemented using OpenAI GPT-4o Search Preview model API calls combined with heuristic rules. The approach was designed as a pragmatic aid for country suggestion rather than a validated predictive model. No supervised training was performed, and no fixed model was deployed beyond the API calls and heuristics. Validation was limited to retrospective checks against a subset of explicit user choices, which showed approximate concordance but were not sufficient to support scientific analysis. For this reason, AI-assigned cases were excluded from the analytic cohort to ensure the results reflected explicit user-driven decisions.
This layered, service-oriented architecture enhances the security, maintainability, and extensibility of the MedSeek platform.
User data structure and collection
Users access the MedSeek application by downloading it from the Google Play Store or Apple App Store. During the sign-up process, the app collects basic user information, including name, email address (used for login verification), age, country of residence, and gender. As users interact with the app by entering symptoms or health-related questions and receiving personalized medical resource recommendations, their inputs are securely stored in Firebase Cloud, which also manages user authentication. The system allows the application administrator to manage and monitor both authentication records and database access for research purposes, while maintaining strict privacy controls.
For data collection, a Python script is used to automate the extraction of user symptom search histories from Firestore. This script processes user metadata along with nested search history subcollections. Non-English symptom entries were automatically translated into English using Google Translate prior to analysis. While this ensured broad inclusivity across diverse users, author recognize that automatic translation can occasionally misinterpret technical medical terms or idiomatic expressions. The output is compiled into a structured Excel spreadsheet, enabling detailed behavioral analysis across demographic segments.
The dataset covers the full period from May 2025 to July 2025. This three-month window defines the analytic cohort and is reported to provide clarity on the temporal scope of the study.
Data Process
Data filter
To prepare the dataset for analysis, each entry was manually reviewed and filtered. Symptom records irrelevant to medical issues were removed, such as empty, meaningless, or duplicate queries. The data included only searches from cross-border seekers which defined as a user whose self-reported country of residence differed from their explicitly selected target country for medical resource retrieval. Users selecting their own country were classified as domestic seekers. The study excluded records where the target country was automatically assigned by the MedSeek AI module, retaining only explicit user selections. This decision ensured that analyses reflected user-driven decision-making rather than system inferences, which may be influenced by language detection or prior interactions.
For the gender variable, users who chose the ‘other’ category (n=87) were not included in the subsequent statistical analysis due to their insufficient scale for meaningful inter-group comparisons. Therefore, the analysis of this study was limited to users who identified themselves as “male” or “female”.
After all filtering steps, the final dataset comprised 1,007 valid user records, forming the basis for subsequent analyses of global healthcare-seeking behavior via the MedSeek platform. Figure 2 shows the flow diagram for analytic sample selection.

For transparency, Comparison of user characteristics before and after AI-assigned target country exclusion is provided in Table 1.
| Characteristic | Excluded non-medical or duplicate entries (N = 1945) |
Excluded AI-assigned target countries (N = 1098) |
|---|---|---|
| Gender | ||
| – Male (%) | 58% | 66% |
| – Female (%) | 38% | 30% |
| – Other (%) | 4% | 4% |
| Age (years) | ||
| Mean age | 40 | 43 |
| – 0–9 | 11% | 11% |
| – 10–19 | 15% | 11% |
| – 20–29 | 10% | 9% |
| – 30–39 | 10% | 10% |
| – 40–49 | 10% | 10% |
| – 50–59 | 18% | 23% |
| – 60–69 | 9% | 11% |
| – 70–79 | 11% | 10% |
| – 80–89 | 6% | 5% |
| Language of Input | ||
| – English (%) | 70% | 80% |
| – Non-English (%) | 30% | 20% |
The filtered cohort was slightly older on average (mean age 40 vs. 43 years), with a lower proportion of users at age 80-89 (6% vs. 5%) and a higher proportion at 50-59 (18% vs. 23%). Gender distribution also shifted modestly, the share of male users increasing from 58% to 66%. In addition, English input was more prevalent among explicit-choice users (70% vs. 80%), while non-English inputs were less common (30% vs. 20%). These differences suggest that the analytic cohort may overrepresent mid-aged and English-speaking users compared with the overall base, which is acknowledged in the limitations.
Data grouping
For age-based analysis, two age classifications were used: “Broad Age Groups” – a three-category scheme (young, middle-aged, elderly) for high-level comparisons, and “Detailed Age Groups” – a nine-interval scheme (0–9 to 80–89 years) for fine-grained trend analysis.
For analysis, individual symptom entries were grouped into broader symptom categories to enable clearer comparison across demographic groups and countries. Similar or related terms were standardized under a single category, reducing redundancy caused by variations in terminology, spelling, or translation. The classification scheme was informed by the International Statistical Classification of Diseases and Related Health Problems (ICD-11) to ensure clinical interpretability. The complete set of categories is presented in Figure 6 and detailed in Table 5. To assess the reliability of symptom classification, we calculated the inter-rater consistency of 150 randomly selected symptom descriptions. Two independent coders used the established classification method and obtained Cohen’s Kappa coefficient of 0.78, indicating good classification consistency.
Data analysis methods
A binary variable called “ifus” (short for “if U.S.”) was introduced to this study that gave 1 to people who wanted to go to the United States for treatment and 0 to everyone else. This preprocessing made a strong dataset for demographic and regional studies, especially for looking at what kinds of medical treatment people in the U.S. prefer.
Chi-square tests were used to see if there was a link between age group and U.S. treatment preference (ifus=1). Fisher’s Exact Test examined the association between a person’s country of origin and their choice of treatment in the United States. Intent-based segmentation analyzed health issues by age and gender and determined the relative frequency of symptom categories among individuals seeking care in the United States. A p-value of 0.05 was used as the threshold for statistical significance, with values below this indicating a significant association.
Descriptive statistics summarized the user base, including gender distribution, age group distribution, and the proportion seeking treatment in the United States. The analysis was conducted on above filtered and grouped records to identify patterns in cross-border healthcare behavior.
The chi-square test of independence examines whether there is a significant association between the month (May, June, and July 2025) and the proportion of users choosing the United States for medical treatment (ifus). It tests the null hypothesis that the ifus proportions are consistent across the three months, with a p-value greater than 0.05 indicating no significant difference.
Multivariate logistic regression analysis was used to select the situation of the United States versus non-United States. The model includes age group (0-29 as reference, coded 0; 30-59 as 1; 60-89 as 2), income tier (Low-Income as reference, coded 0; Lower-Middle-Income as 1; Upper-Middle-Income as 2; High-Income as 3), distance group (0 as nearest to 3 as farthest), gender (female = 0, male = 1), and language (Non-English = 0, English = 1).
Ethics and Regulatory Compliance
This study was reviewed and determined exempt from full Institutional Review Board (IRB) review under 45 CFR 46.104(d)(4) of the U.S. Common Rule. This exemption applies to research involving the secondary use of identifiable private information, provided that data are recorded in a manner that prevents investigators from readily ascertaining the identity of the subjects, that there is no direct contact with subjects, and that investigators do not attempt re-identification. In our case, all analyses were conducted using retrospective, de-identified MedSeek app usage data, with personal identifiers (e.g., names and email addresses) removed prior to data extraction. The investigator accessed and analyzed only anonymized data, which were stored on secure, access-restricted servers and processed at the aggregate level. Because no identifiable information was retained, and no attempts at re-identification were made, the research met the criteria for exemption from full IRB review. Consequently, no additional informed consent was required for secondary analysis.
Results
User base
Table 2 summarizes the demographic characteristics of the final analytic cohort (N = 1,007), including gender, age group, World Bank income tier, platform (iOS vs. Android), and language of symptom input.
Regarding the handling of gender variables, as mentioned earlier, users who chose the ‘other’ category (n=87) were excluded from the main analysis because their sample size was too small to be reliably estimated as an independent category in the model. This move was based on considerations of statistical robustness rather than due to data deficiency.
| Characteristic | Number | Ratio (%) |
|---|---|---|
| Gender | ||
| Male | 680 | 67.5% |
| Female | 327 | 32.5% |
| Age Group (years) | ||
| 0–9 | 108 | 10.7% |
| 10–19 | 118 | 11.7% |
| 20–29 | 92 | 9.1% |
| 30–39 | 98 | 9.7% |
| 40–49 | 99 | 9.8% |
| 50–59 | 230 | 22.8% |
| 60–69 | 108 | 10.7% |
| 70–79 | 99 | 9.8% |
| 80–89 | 55 | 5.5% |
| Platform | ||
| iOS | 152 | 15.1% |
| Android | 853 | 84.9% |
| World Bank Income tier | ||
| High-Income | 442 | 43.9% |
| Upper-Middle-Income | 198 | 19.7% |
| Lower-Middle-Income | 128 | 12.7% |
| Low-Income | 239 | 23.7% |
| Language | ||
| English | 807 | 80.1% |
| Non-English | 200 | 19.9% |
Findings are based solely on MedSeek users, who may not be representative of all cross-border healthcare seekers. App users are typically digitally literate, own smartphones, and may differ from populations who access cross-border care through offline or intermediary channels. This limits generalizability to the broader patient population.

Figure 3 illustrates the monthly distribution of users in the final analytic cohort across the three-month study period (May–July 2025). User counts were relatively stable over time, with 320 users in May, 365 in June, and 322 in July. The modest peak observed in June suggests a temporary increase in platform activity but does not indicate a strong secular trend. These results support the use of month fixed effects in regression models to account for potential seasonal or temporal confounding. The chi-square test of independence yields a p-value greater than 0.05, suggesting no significant difference in ifus proportions across the months of May, June, and July 2025. This result supports the stability of the user preference for choosing the United States for medical treatment across the study period and validates the use of month fixed effects as a sufficient adjustment for potential seasonal variation, indicating that month does not confound the demographic associations.
The dataset tracks the number of individuals from different countries seeking medical care across borders. The findings indicate that smaller or developing nations, such as Hungary, Cameroon, Montenegro, etc., account for a high share of cross-border medical seekers, likely due to limited local healthcare capacity or the need for specialized treatment. Figure 4 presents the distribution for the top 30 countries.

Figure 4. Top 30 Countries by Per App-User-Base Rate of U.S.-Bound Healthcare Seekers
Turkey and Colombia are tied for first place, with a ratio of 1.000 each. This indicates that all (or almost all) application users in these countries have the need to switch to American healthcare.
Montenegro (0.90, N = 9), Albania (0.89, N = 8), Brazil (0.88, N = 7), and Uzbekistan (0.88, N = 7) show high rates, indicating that a large proportion of their app users seek U.S. care. These findings align with the paper’s note that countries with limited healthcare infrastructure (e.g., Montenegro) drive cross-border care36,11.
The list includes high-income (e.g., Denmark, Canada), upper-middle-income (e.g., Brazil, Malaysia), and low-income countries (e.g., Guinea-Bissau, Uganda), suggesting that U.S. healthcare appeals across economic contexts, possibly driven by specialized treatments like oncology and cardiology37),34.
651 individuals (64.6%) identified the United States as their target country for medical resources, showing that the United States is a common destination for cross-border healthcare. In the table 3, mark those results that remain significant after FDR correction with an asterisk (*). Chi-square test results indicated that individuals that grouped as elderly (60–89) were significantly more likely to choose the United States, whereas young group (0–29) and middle-aged (30–59) showed no statistically significant preference, as shown in Table 3. The stronger association observed in the elderly group may reflect greater disease severity or higher financial capacity to seek care abroad.
| Age group | P_value | Significant |
|---|---|---|
| Young (0–29) | 0.781 | FALSE |
| Middle-aged (30–59) | 0.045 | FALSE |
| Elderly (60–89) | 0.013* | TRUE |
Fisher’s Exact Test was applied to countries with more than 10 users in the dataset, ensuring sufficient sample size for meaningful comparison. The analysis indicated strong associations between country of origin and preference for U.S. cross-border medical care (ifus = 1) for Montenegro (p <0.001), Vatican City (p = 0.002), Cameroon (p = 0.003), Malaysia (p = 0.003), and Sierra Leone (p = 0.004). No significant association was observed for Hungary (p = 0.781), Bhutan (p = 0.950), or Uganda (p = 0.950), as shown in Table 4. The strong preferences seen in Montenegro, Cameroon, and Sierra Leone may be due to limited local healthcare options, while Malaysia’s result could reflect specific demand for U.S. medical expertise. In Vatican City, the pattern may be influenced by its small population and limited medical facilities. Countries with no clear preference may be affected by financial constraints or easier access to other destinations. For countries with fewer records, the results were even less significant, making it difficult to determine whether differences in U.S. preference truly reflect variations in population characteristics.
| Most Significant | P-value | Significant | Least Significant | P-value | Significant |
|---|---|---|---|---|---|
| Montenegro | <0.001* | TRUE | Bhutan | 0.950 | FALSE |
| Vatican City | 0.002* | TRUE | Uganda | 0.950 | FALSE |
| Cameroon | 0.003* | TRUE | Hungary | 0.781 | FALSE |
| Malaysia | 0.003* | TRUE | |||
| Sierra Leone | 0.004* | TRUE |
The logit regression results for the MedSeek app users (N = 1,007) highlight the significant predictors influencing the likelihood of choosing the United States (ifus = 1) for medical treatment. As shown in table 5, the AUC is 0.879, indicating that the model has an excellent discriminatory ability in differentiating between American and non-American selectors. The Brier score is 0.115, reflecting good calibration. A lower value indicates better prediction accuracy.
The model shows a strong correlation between income class and the possibility of choosing the United States. Users in Upper-Middle-Income and High-Income countries show a significantly higher probability compared to Low-Income users. This indicates that economic resources play a key role in cross-border medical decisions and may make the use of medical facilities in the United States possible. The significant effect of medium distance (Group 2) indicates that users in areas where the distance is neither too close nor too far may consider the United States a feasible option, possibly due to travel feasibility and perceived medical quality.
| Variable | OR | 95% CI [Low, High] |
|---|---|---|
| Intercept | 0.085 | [0.044, 0.167] |
| Age group (T1) | 0.932 | [0.603, 1.442] |
| Age group (T2) | 0.672 | [0.415, 1.088] |
| Income tier (T1) | 4.650 | [2.667, 8.107] |
| Income tier (T2) | 53.05 | [29.662, 94.878] |
| Income tier (T3) | 71.965 | [43.210, 119.857] |
| Distance group (T1) | 1.589 | [0.909, 2.779] |
| Distance group (T2) | 1.778 | [1.043, 3.031] |
| Distance group (T3) | 1.560 | [0.931, 2.615] |
| Gender code | 1.319 | [0.894, 1.945] |
| Language code | 1.185 | [0.725, 1.936] |
The mixed-effects logistic regression model analyzes the likelihood of MedSeek app users (N = 1,007) choosing the United States (ifus = 1) for medical treatment, with users nested within 189 countries.
The low group variance (0.010) indicates that country-level differences explain a small portion of the variability, with random effects highlighting specific countries (e.g., Sierra Leone, Solomon Islands) where U.S. preference is notably higher, possibly due to healthcare infrastructure gap, as shows in the table 6.
| Variable | Coef. | Std. Err. | z | p | 95% CI [Low, High] |
|---|---|---|---|---|---|
| Intercept | 0.054 | 0.042 | 1.290 | 0.197 | [−0.028, 0.136] |
| Age group (T1) | −0.0009 | 0.025 | −0.336 | 0.721 | [−0.058, 0.040] |
| Age group (T2) | −0.0046 | 0.028 | −0.16 | 0.106 | [−0.101, 0.010] |
| Income tier (T1) | 0.769 | 0.035 | 22.137 | <0.001 | [0.701, 0.837] |
| Income tier (T2) | 0.800 | 0.028 | 28.275 | <0.001 | [0.744, 0.857] |
| Distance group (T1) | 0.049 | 0.039 | 1.259 | 0.208 | [−0.027, 0.125] |
| Distance group (T2) | 0.072 | 0.038 | 1.903 | 0.057 | [−0.002, 0.146] |
| Distance group (T3) | 0.054 | 0.037 | 1.462 | 0.144 | [−0.019, 0.127] |
| Gender code | 0.033 | 0.023 | 1.432 | 0.152 | [−0.012, 0.077] |
| Language code | 0.024 | 0.035 | 0.691 | 0.490 | [−0.044, 0.092] |
| Group variance | 0.010 | 0.012 | — | — | — |
Intent-based segmentation
Age
The data indicate that health concerns vary across age groups. The following heat map (see Figure 5) summary presents the most common symptom categories among individuals seeking treatment in the United States. These differences reflect both age-related physiological factors and varying motivations for seeking care in the U.S.

Figure 5. Symptom category distribution by age group
In the young cohort (0–29 years), Primary neoplasms of brainoncology (9.13%, n=19) and Systemic lupus erythematosusautoimmune disorders (8.17%, n=17) were the major concern categories, followed by Leukemiahematologic cancer (8.17%, n=17) and Multi organ failureorgan failure (7.69%, n=16). Complex Osteomyelitis or osteitisorthopedic problems (7.21%, n=15), Complete trisomies of the autosomesrare genetic disorders (6.73%, n=14), and Dissociative neurological symptom disorderrare neurologic disorders (6.73%, n=14) were also frequent. In contrast, common conditions, such as allergies, the common cold, and routine checkups, were infrequent in this cohort. This suggests that cross-border care among young users is concentrated on serious, specialist conditions.
Middle-aged individuals (30–59 years) have a wide range of health issues, with Cardiac arrhythmia, Heart failurecardiovascular problems (7.37%, n=21), Leukemiahematologic cancer (7.02%, n=20), Multi organ failureorgan failure (7.02%, n=20), and Primary neoplasms of brainoncology (6.67%, n=19) being the most common. Presence of transplanted organ or tissueTransplant evaluation (6.67%, n=19) and Chronic kidney disease, stage unspecifiedchronic renal disease (6.32%, n=18) are also high on the list. Similar to the young group, typical problems such as minor injuries or simple fractures are not well represented, suggesting that the focus is on more serious, life-threatening disorders that require advanced medical knowledge.
Elderly individuals (60–89 years) most commonly present with Diseases of liveradvanced liver disease (9.49%, n=15) and Systemic lupus erythematosusautoimmune illnesses (8.86%, n=14), followed by Chronic kidney disease, stage unspecifiedchronic renal disease (8.23%, n=13) and Cardiac arrhythmia, Heart failureheart problems (6.96%, n=11). Primary neoplasms of brainOncology, advanced lung disease, severe psychiatric problems, and transplant evaluation each account for approximately 6.33% (n=10). Common conditions such as stomach issues or ear infections are absent in this group, reinforcing the trend that cross-border treatment is sought primarily for serious, long-term health problems.
Gender
Primary neoplasms of brain (8.17%, n=17) is the most common health problem among female users seeking medical care in the United States. This is closely followed by Presence of transplanted organ or tissue (7.69%, n=16) and Complete trisomies of the autosomes (7.21%, n=15). Pneumonia and Dissociative neurological symptom disorder each account for 6.73% (n=14) of cases. Systemic lupus erythematosus, Chronic kidney disease, stage unspecified, Osteomyelitis or osteitis, Leukemia, and Multi organ failure each represent 6.25% (n=13). Metabolic disorders (5.29%, n=11) and Cardiac arrhythmia, Heart failure (4.81%, n=10) are less common but still important. Minor conditions, such as Influenza due to identified seasonal influenza virus (1.92%, n=4), Diseases of external ear; Diseases of middle ear or mastoid; Diseases of inner ear (1.44%, n=3), Spinal pain (1.44%, n=3), Dental examination (1.44%, n=3), and Skin disorders involving certain specific body regions (1.44%, n=3), are infrequent, suggesting that female users primarily seek U.S. care for complex, specialized conditions requiring advanced diagnostic or therapeutic interventions (see Figure 5).
For male users, Cardiac arrhythmia, Heart failure (7.45%, n=33) and Leukemia (7.22%, n=32) are the most common, followed closely by Systemic lupus erythematosus (7.00%, n=31) and Primary neoplasms of brain (7.00%, n=31). Diseases of liver and Multi organ failure each account for 6.77% (n=30), while Chronic kidney disease, stage unspecified and Osteomyelitis or osteitis each represent 6.09% (n=27). Autism spectrum disorder (5.42%, n=24), Dissociative neurological symptom disorder (5.64%, n=25), and Complete trisomies of the autosomes (5.42%, n=24) are also frequent. Similar to female users, male users rarely report minor conditions, including Impairment of visual functions; Disorders of the eyeball (1.58%, n=7), Spinal pain (1.35%, n=6), and Influenza due to identified seasonal influenza virus (1.13%, n=5), indicating that U.S. treatment is sought mainly for serious, long-term, or highly specialized problems (see Figure 6).
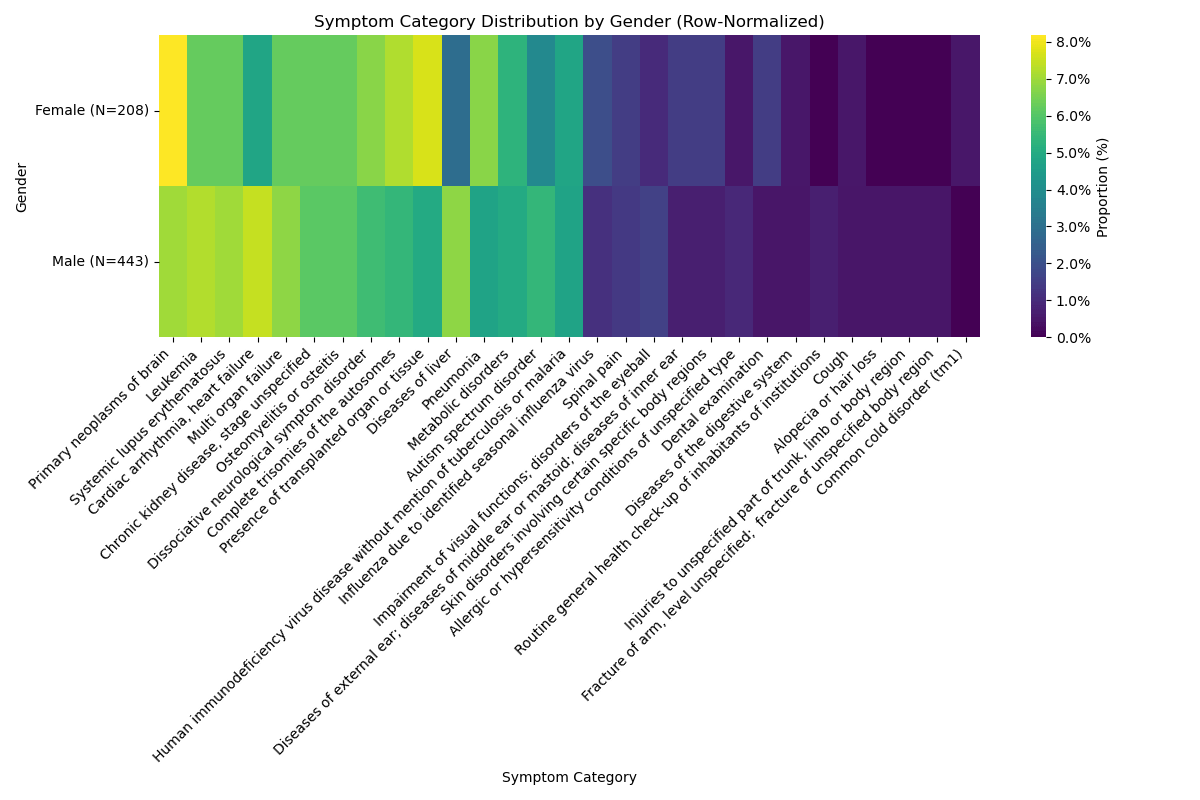
Figure 6. Symptom category distribution by gender
Symptom
The frequency of each symptom in each country and age group was calculated using only records in which the user selected the United States as the target country, followed by linear regression analysis of symptom frequency against age patterns. Figure 7 presents the results. Regression findings indicate that the following symptoms have a p-value of less than 0.05, indicating statistically significant trends.
Cardiac arrhythmia, Heart failure (p = 0.0334) shows more cases in later age groups, particularly those between 50–59 and 80–89 years, suggesting that older individuals are more likely to seek treatment for heart problems in the United States, potentially due to increased complexity of conditions with age or greater availability of advanced treatments such as heart surgeries.
Diseases of external ear; Diseases of middle ear or mastoid; Diseases of inner ear (p = 0.0171) is more common in younger groups (0–9, 10–19), likely because it is more prevalent in children, while the prevalence in older groups is very low, implying that cross-border treatment for ear infections is primarily a pediatric concern.
Dental examination (p = 0.0238) is more frequent in younger individuals and declines sharply with age, indicating that younger individuals or their parents are more likely to seek dental care across borders, potentially for cosmetic or specialized pediatric dental services.
Injuries to unspecified part of trunk, limb or body region (p = 0.0267) is notable only in the youngest groups, likely due to minor injuries such as sports-related incidents in children, with a sharp decline suggesting that older individuals seldom seek cross-border treatment for minor injuries.
Allergic or hypersensitivity conditions of unspecified type (p = 0.0121) is relatively uncommon in younger groups but increases in older groups, particularly among those aged 60–69 and 80–89 years, suggesting that elderly individuals may seek treatment for severe or complex allergies in the United States, possibly due to limited local expertise.

Figure 7. Age-Based Distribution of Symptom Categories
Discussion
The study highlights key demographic and health-related factors driving cross-border medical care, with the United States as the leading destination. Most users were male (67.5% vs. 32.5% female), possibly reflecting gender differences in healthcare-seeking behavior or access to resources for foreign treatment. The largest proportion was in the 50–59 age group (22.8%), indicating that middle-aged individuals who often with complex or long-term conditions are constitute a substantial share of medical tourism.
Overall, 64.6% of users selected the United States, reflecting its reputation for advanced healthcare systems and specialized expertise. Chi-square tests showed significant U.S. treatment preferences among middle-aged (30–59 years, p=0.045) and elderly (60–89 years, p=0.013) groups, with stronger preference in the elderly, likely due to severe conditions such as cardiovascular anomalies or chronic kidney disease requiring specialized care. In contrast, the young group (0–29 years, p=0.781) showed no significant preference, possibly because they face fewer complex conditions or have adequate local treatment options.
Fisher’s Exact Test revealed strong associations between country of origin and U.S. preference for Montenegro (p<0.001), Vatican City (p=0.002), Cameroon (p=0.003), Malaysia (p=0.003), and Sierra Leone (p=0.004). For Montenegro, Cameroon, and Sierra Leone, this may reflect limited healthcare infrastructure. Malaysia’s result may be driven by demand for specialized expertise, while Vatican City’s pattern is likely influenced by its small population and limited local medical facilities. Hungary, Bhutan, and Uganda showed no significant association, possibly due to economic constraints or access to alternative destinations.
Health issues varied across age and gender. Young individuals (0–29 years) were most affected by oncology, autoimmune illnesses, and hematologic cancer, indicating a need for advanced diagnostics and treatments. Middle-aged individuals (30–59 years) most often sought care for cardiovascular problems, hematologic cancer, and organ failure, suggesting demand for complex procedures such as transplants. Elderly individuals (60–89 years) focused on advanced liver disease, autoimmune illnesses, and chronic renal disease, aligning with the higher prevalence of these conditions in older populations. Female users most frequently sought care for oncology, transplant evaluation, and uncommon genetic illnesses, while male users prioritized hematologic cancer and cardiovascular problems. Across all groups, minor issues such as allergies or mild injuries were rare, reinforcing that cross-border care is sought primarily for serious, specialized conditions.
Linear regression identified significant symptom trends by age group. Cardiovascular anomalies (p=0.0334) were more common in older groups (50–59 and 80–89 years), indicating greater need for advanced cardiac care. Ear infections (p=0.0171), mild dental issues (p=0.0238), and mild injuries (p=0.0267) were more prevalent among younger groups, suggesting these are predominantly pediatric concerns. Allergies (p=0.0121) increased in older groups, pointing to potential demand for specialized allergy care in the U.S.
Our findings indicate significant patient outflows from countries with limited healthcare infrastructure, such as Montenegro, Cameroon, and Sierra Leone, seeking specialized care in the U.S. This trend may exacerbate healthcare inequities in source countries, as resources are diverted to wealthier patients traveling abroad. For these nations, investing in local capacity for oncology and cardiology could reduce reliance on cross-border care. Digital platforms like MedSeek can provide data to guide resource allocation and policy development, helping source countries strengthen their healthcare systems.
The exclusion of AI-assigned records narrowed the analytic cohort to explicit-choice users, which introduced modest demographic differences compared with the broader user base. As shown in Table 1, explicit-choice users tended to be slightly older, more often male, and more likely to use English input. This suggests that the analytic sample may overrepresent digitally literate and linguistically advantaged users, limiting the generalizability of findings to the entire MedSeek population.
The use of Google Translate for non-English entries is a limitation of this study. Although translation facilitated the integration of a linguistically diverse dataset, automated tools may misclassify specialized clinical terminology, introducing potential bias in symptom categorization. To partially mitigate this, we grouped symptoms into broad categories and validated classification on a stratified subset. Nonetheless, some residual misclassification is possible, and future research should employ back-translation protocols or professional medical translation to improve accuracy.
A key limitation of this study is the exclusion of search items whose target country was assigned by the MedSeek AI module. This filtering step was necessary to ensure that the analytic dataset reflected user-driven decisions rather than algorithmic inference. Including AI-assigned records could have introduced additional bias because the AI model applies proprietary heuristic rules whose internal logic is not fully transparent. However, this decision also narrows the generalizability of our findings, since excluded users may differ systematically from explicit choosers, for example, they may rely more heavily on automated guidance or possess lower digital literacy. As such, the final cohort may overrepresent individuals who actively specify their healthcare preferences, and future work should aim to incorporate both explicit and AI-assisted decisions in a more controlled fashion.
Another limitation of this study is the restricted three-month collection window (May–July 2025). Although it included month fixed effects in all models to account for short-term seasonal variation, the absence of a full year of data precludes evaluation of broader seasonal cycles or long-term secular trends. As such, the generalizability of findings across different times of year is constrained.
This study presents a behavioral analysis of user decision-making patterns captured through the MedSeek platform. The focus is on how demographics, country of residence, and symptom categories shape cross-border healthcare preferences. The MedSeek platform is described only to provide context; the analyses do not evaluate its clinical effectiveness or usability. Although the app was originally designed to assist users in finding international healthcare resources, in this study it is used as a data source for observing patient behavior. The insights generated may serve as evidence to inform and enhance the platform’s features in future development.
Conclusion
According to MedSeek data, the United States is the leading destination for cross-border medical care, with 64.6% of the 1,007 users selecting U.S. healthcare facilities. Clear preferences were observed among individuals aged 30–59 and 60–89, as well as among those from countries with limited healthcare infrastructure, such as Montenegro, Cameroon, and Sierra Leone. Health concerns varied by age and gender: younger individuals were more often affected by cancer and autoimmune illnesses, middle-aged individuals prioritized cardiovascular problems and organ failure, and older individuals focused on advanced liver disease and chronic kidney disease. Women most frequently sought care for oncology and transplant evaluation, while men more often pursued treatment for hematologic cancer and cardiovascular anomalies. Temporal trends indicated that older individuals were more likely to require treatment in the U.S. for cardiovascular problems and allergies, whereas younger individuals more commonly presented with ear infections.
These findings underscore the importance of developing healthcare strategies tailored to the diverse medical needs of cross-border patients. U.S. policymakers and healthcare providers should ensure adequate capacity for specialist services, particularly in oncology and cardiovascular care. Future research should examine the social and economic drivers of cross-border healthcare and explore ways to strengthen healthcare systems in developing countries, reducing reliance on overseas treatment.
Acknowledgments
The author gratefully acknowledges Peng Yin for his guidance on the app design and for the insightful discussions, informed by his prior work in medical related software development.
Supplementary Materials
| ICD-11 Chapter (Highest Level) | ICD-11 Subcategory (Nearest Match) | User Query Keywords |
|---|---|---|
| 02 Neoplasms | 2B33.4 Leukemia, unspecified | leukemia diagnosis, blood cancer treatment, acute myeloid leukemia, chronic lymphocytic leukemia, stem cell transplant, bone marrow biopsy, hematology specialist, leukemia remission, pediatric leukemia care |
| 04 Diseases of the immune system | 4A40.0 Systemic lupus erythematosus | lupus flare, lupus nephritis care, lupus rash, lupus arthritis, lupus fatigue, lupus treatment, lupus medication, lupus diet |
| 01 Certain infectious or parasitic diseases | 1C62 Human immunodeficiency virus disease without mention of tuberculosis or malaria | HIV infection, HIV positive, AIDS, HIV treatment, HIV medication, HIV testing, HIV prevention, HIV care, HIV viral load |
| 06 Mental, behavioural or neurodevelopmental disorders | 6B60 Dissociative neurological symptom disorder | dissociative disorder, functional neurological disorder, conversion disorder, psychogenic seizure, non-epileptic seizure, functional paralysis, functional tremor, functional blindness, psychogenic speech loss, psychogenic movement disorder |
| 21 Symptoms, signs or clinical findings, not elsewhere classified | MG4A Multi organ failure | multi organ failure, multiple organ dysfunction, kidney liver failure, heart lung kidney failure, brain organ dysfunction syndrome, systemic organ failure |
| 12 Diseases of the respiratory system | CA40 Pneumonia | lung infection, lung inflammation, lung disease pneumonia, fluid in lungs, lung consolidation, lung crackles, lung infiltrate, lung bacterial infection, lung viral infection, lung chest infection |
| 11 Diseases of the circulatory system | Cardiac arrhythmia, Heart failure | cardiac failure, cardiac arrhythmia, cardiac murmur, cardiac valve disease, cardiac hypertrophy, cardiac anomaly, cardiac ischemia, heart attack, heart blockage, heart palpitations, heart disease |
| 16 Diseases of the genitourinary system | GB61.Z Chronic kidney disease, stage unspecified | chronic kidney disease, kidney damage, kidney function decline, kidney insufficiency, renal disease, chronic renal failure, kidney problems, impaired kidney function |
| 20 Developmental anomalies | LD40 Complete trisomies of the autosomes | down syndrome, trisomy 21, trisomy 13, chromosomal trisomy, genetic trisomy disorder, autosomal trisomy, chromosome abnormality trisomy |
| 13 Diseases of the digestive system | DB9Z Diseases of liver, unspecified | liver disease, chronic liver disease, liver disorder, liver inflammation, liver condition, liver damage, hepatic disease, hepatic disorder, abnormal liver function, liver problem drainage |
| 15 Diseases of the musculoskeletal system or connective tissue | FB84 Osteomyelitis or osteitis | arm bone pain, leg bone pain, chest bone pain, knee bone lesion, ankle bone lump |
| 02 Neoplasms | 2A00 Primary neoplasms of brain | brain tumor, brain cancer, primary brain tumor, glioma, astrocytoma, glioblastoma, meningioma, oligodendroglioma, medulloblastoma, malignant brain neoplasm |
| 06 Mental, behavioural or neurodevelopmental disorders | 6A02 Autism spectrum disorder | autism, autism spectrum disorder, ASD, autistic disorder, childhood autism, pervasive developmental disorder, social communication disorder, high functioning autism, Asperger syndrome, autistic traits |
| 10 Diseases of the ear or mastoid process | Diseases of external ear; Diseases of middle ear or mastoid; Diseases of inner ear | ear infection, otitis media, mastoiditis, fluid in middle ear, eustachian tube dysfunction, chronic otitis media, ear drum perforation, ear effusion, ear pain |
| 24 Factors influencing health status or contact with health services | QB63 Presence of transplanted organ or tissue | transplant evaluation, organ donor matching, pre-transplant workup, transplant eligibility test, transplant waiting list registration, living donor consult, cross-match testing, transplant center referral, immunosuppressant planning, post-transplant care |
| 13 Diseases of the digestive system | DE2Z Diseases of the digestive system, unspecified | stomach pain, belly pain, stomach cramps, gut pain, upset stomach, bad digestion, bloated belly, stomach ache, tummy pain, stomach problem |
| 05 Endocrine, nutritional or metabolic diseases | 5D2Z Metabolic disorders, unspecified | diabetes specialist, insulin therapy adjustment, HbA1c monitoring, diabetic complications screening, oral hypoglycemic initiation, endocrinologist referral, glucose monitoring devices |
| 21 Symptoms, signs or clinical findings, not elsewhere classified | ME84 Spinal pain | back pain therapy, spinal manipulation, lumbar strain treatment, disc herniation care, ergonomic advice, pain clinic referral, MRI for back pain, conservative spine management |
| 24 Factors influencing health status or contact with health services | QA00.8 Dental examination | dentist visit, dental cosmetic, routine dental care, cavity filling, gum treatment, teeth cleaning, oral exam, preventive dentistry, dental x-ray, pediatric dentist, tooth extraction consult |
| 22 Injury, poisoning or certain other consequences of external causes | Injuries to unspecified part of trunk, limb or body region | wound cleaning, tetanus shot, first aid center, scratch dressing, sports injury care, outpatient dressing change, abrasion management, laceration glue |
| 22 Injury, poisoning or certain other consequences of external causes | ND52 Fracture of arm, level unspecified; ND56.2 Fracture of unspecified body region | broken arm treatment, orthopedic casting, fracture reduction, x-ray imaging, bone setting, plaster cast care, orthopedic surgeon visit, fracture healing timeline, physical therapy for fracture |
| 14 Diseases of the skin | Skin disorders involving certain specific body regions | skin rash clinic, eczema treatment, dermatology referral, atopic dermatitis management, allergy patch test, moisturizer therapy, chronic eczema plan, dermatology telehealth |
| 04 Diseases of the immune system | 4A8Z Allergic or hypersensitivity conditions of unspecified type | pollen allergy care, food allergy test, allergy immunotherapy, rhinitis management, asthma trigger avoidance, allergen testing panel, desensitization program, allergist visit, epinephrine prescription, environmental allergy counseling |
| 26 Supplementary Chapter Traditional Medicine Conditions | SA60 Common cold disorder (TM1) | common cold medicine, cough clinic, viral URI treatment, rest and hydration advice, fever management, throat swab test, nasal congestion relief, sore throat care, over-the-counter cold remedy, telemedicine consult for URI |
| 09 Diseases of the visual system | Impairment of visual functions; Disorders of the eyeball | red eye doctor, eye infection treatment, conjunctivitis care, allergic eye drop prescription, bacterial eye infection, viral conjunctivitis, eye discharge cleaning, optometrist consult, eye redness diagnosis, pediatric eye care |
| 14 Diseases of the skin | ED70 Alopecia or hair loss | hair loss treatment, alopecia areata care, scalp biopsy, hair regrowth therapy, wig consultation, hormonal hair loss treatment, trichology clinic |
| 24 Factors influencing health status or contact with health services | QA03.1 Routine general health check-up of inhabitants of institutions | annual checkup, preventive screening, health risk assessment, blood work panel, wellness visit, routine physical exam, occupational health clearance, lifestyle counseling, general practitioner visit |
| 21 Symptoms, signs or clinical findings, not elsewhere classified | MD12 Cough | seasonal cough treatment, persistent cough doctor, chest x-ray for cough, post-viral cough clinic, chronic cough workup, cough syrup prescription, respiratory infection clinic, cough specialist |
| 01 Certain infectious or parasitic diseases | 1E30 Influenza due to identified seasonal influenza virus | flu vaccine clinic, influenza treatment abroad, antiviral medication, seasonal flu outbreak map, fever reduction therapy, flu shot appointment, influenza hospitalization, rapid flu test, flu prevention |

Figure 8. Architecture of the MedSeek application
References
- D. Bell, R. Holliday, M. Ormond, & T. Mainil. Transnational healthcare, cross-border perspectives. Social Science & Medicine, 124, 284–289 (2015). [↩]
- J. Hanefeld, N. Lunt, R. Smith, & D. Horsfall. Why do medical tourists travel to where they do? The role of networks in determining medical travel. Social Science & Medicine, 124, 356-363 (2015). [↩] [↩] [↩] [↩]
- A. de la Hoz-Correa, F. Muñoz-Leiva, & M. Bakucz. Past themes and future trends in medical tourism research: A co-word analysis. Tourism Management, 65, 200–211 (2018). [↩]
- M. Shabani, & P. Borry. Rules for processing genetic data for research purposes in view of the new EU general data protection regulation. European Journal of Human Genetics, 26(2), 149–156 (2018). [↩] [↩] [↩]
- H. A. Simon. Invariants of human behavior. Annual Review of Psychology, 41, 1–20 (1990). [↩]
- D. Kahneman, & A. Tversky. Prospect theory: An analysis of decision under risk. Econometrica, 47(2), 263–291 (1979). [↩] [↩] [↩]
- M. Ryan, & K. Gerard. Using discrete choice experiments to value health care programmes: Current practice and future research reflections. Applied Health Economics and Health Policy, 2(1), 55–64 (2003). [↩]
- K. Huckvale, J. T. Prieto, M. Tilney, P.-J. Benghozi, & J. Car. Unaddressed privacy risks in accredited health and wellness apps: A cross-sectional systematic assessment. BMC Medicine, 13, 214 (2015). [↩] [↩]
- J.-P. Onnela, & S. L. Rauch. Harnessing smartphone-based digital phenotyping to enhance behavioral and mental health. Neuropsychopharmacology, 41(7), 1691–1696 (2016). [↩] [↩] [↩]
- J. Connell. Contemporary medical tourism: Conceptualisation, culture and commodification. Tourism Management, 34, 1–13 (2013). [↩] [↩] [↩]
- R. Johnston, V. A. Crooks, J. Snyder, & P. Kingsbury. What is known about the effects of medical tourism in destination and departure countries? A scoping review. International Journal for Equity in Health, 24 (2010). [↩] [↩]
- P. M. Carrera, & J. F. Bridges. Globalization and healthcare: Understanding health and medical tourism. Expert Review of Pharmacoeconomics & Outcomes Research, 6(4), 447–454 (2006). [↩]
- V. C. S. Heung, D. Kucukusta, & H. Song. Medical tourism development in Hong Kong: An assessment of the barriers. Tourism Management, 32(5), 995–1005 (2011). [↩] [↩]
- J. H. Hibbard, & E. Peters. Supporting informed consumer health care decisions: Data presentation approaches that facilitate the use of information in choice. Health Affairs, 24, 413-433 (2003). [↩] [↩] [↩]
- S. S. Iyengar, & M. R. Lepper. When choice is demotivating: Can one desire too much of a good thing? Journal of Personality and Social Psychology, 79(6), 995–1006 (2000). [↩] [↩]
- M. D. Clark, D. Determann, S. Petrou, D. Moro, & E. W. de Bekker-Grob. Discrete choice experiments in health economics: A review of the literature. Pharmacoeconomics, 32, 883–902 (2014). [↩] [↩] [↩]
- E. W. de Bekker-Grob, M. Ryan, & K. Gerard. Discrete choice experiments in health economics: A review of the literature. Health Economics, 21(2), 145–172 (2012). [↩] [↩]
- E. Lancsar, & J. Louviere. Conducting discrete choice experiments to inform healthcare decision making: A user’s guide. Pharmacoeconomics, 26(8), 661–677 (2008). [↩] [↩] [↩]
- V. Soekhai, E. W. de Bekker-Grob, A. R. Ellis, & C. Vass. Discrete choice experiments in health economics: Past, present and future. Pharmacoeconomics, 37(2), 201–226 (2019). [↩] [↩]
- N. Gutacker, L. Siciliani, G. Moscelli, & H. Gravelle. Choice of hospital: Which type of quality matters? Journal of Health Economics, 50, 230–246 (2016). [↩] [↩]
- G. Moscelli, H. Gravelle, L. Siciliani, & R. Santos. Heterogeneous effects of patient choice and hospital competition on mortality. Social Science & Medicine, 216, 50–58 (2018). [↩]
- P. Sivey. The effect of waiting time and distance on hospital choice for English cataract patients. Health Economics, 21(4), 444–456 (2012). [↩] [↩]
- P. E. Kummervold, C. E. Chronaki, B. Lausen, H.-U. Prokosch, J. Rasmussen, S. Santana, A. Staniszewski, & S. C. Wangberg. eHealth trends in Europe 2005–2007: A population-based survey. Journal of Medical Internet Research, 10(4), e42 (2008). [↩]
- J. H. Hibbard, & J. Greene. What the evidence shows about patient activation: Better health outcomes and care experiences; fewer data on costs. Health Affairs, 32(2), 207–214 (2013). [↩] [↩]
- A. C. Powell, A. B. Landman, & D. W. Bates. In search of a few good apps. JAMA, 311(18), 1851–1852 (2014). [↩]
- T. R. Insel. Digital phenotyping: Technology for a new science of behavior. JAMA, 318(13), 1215–1216 (2017). [↩] [↩]
- J. Torous, M. V. Kiang, J. Lorme, & J.-P. Onnela. New tools for new research in psychiatry: A scalable and customizable platform to empower data-driven smartphone research. JMIR Mental Health, 3(2), e16 (2016). [↩] [↩]
- M. E. Larsen, K. Huckvale, J. Nicholas, J. Torous, L. Birrell, E. Li, & B. Reda. Using science to sell apps: Evaluation of mental health app store quality claims. npj Digital Medicine, 2(1), 18 (2019). [↩] [↩]
- T. S. Bergmo. How to measure costs and benefits of eHealth interventions: An overview of methods and frameworks. Journal of Medical Internet Research, 17(11), e254 (2015). [↩]
- M. J. Bietz, C. S. Bloss, S. Calvert, J. G. Godino, J. Gregory, M. P. Claffey, J. Sheehan, & K. Patrick. Opportunities and challenges in the use of personal health data for health research. Journal of the American Medical Informatics Association, 23(e1), e42–e48 (2016). [↩]
- J. Zhao, B. Freeman, & M. Li. Can mobile phone apps influence people’s health behavior change? An evidence review. Journal of Medical Internet Research, 18(11), e287 (2016). [↩]
- J. M. M. Rumbold, & B. Pierscionek. The effect of the general data protection regulation on medical research. Journal of Medical Internet Research, 19(2), e47 (2017). [↩] [↩]
- S. Wachter, B. Mittelstadt, & L. Floridi. Why a right to explanation of automated decision-making does not exist in the general data protection regulation. International Data Privacy Law, 7(2), 76–99 (2017). [↩] [↩]
- R. Santos, H. Gravelle, & C. Propper. Does quality affect patients’ choice of doctor? Evidence from England. The Economic Journal, 127(600), 445–494 (2017). [↩] [↩]
- J. Kaye, E. A. Whitley, D. Lund, M. Morrison, H. Teare, & K. Melham. Dynamic consent: A patient interface for twenty-first century research networks. European Journal of Human Genetics, 23, 141–146 (2015). [↩]
- S. H. Jain, B. W. Powers, J. B. Hawkins, & J. S. Brownstein. The digital phenotype. Nature Biotechnology, 33(5), 462–463 (2015). [↩]
- V. A. Crooks, P. Kingsbury, J. Snyder, & R. Johnston. What is known about the patient’s experience of medical tourism? A scoping review. BMC Health Services Research, 266(2010 [↩]



{kind=link}