
Abstract
The role of mental illness in criminal psychology raises complex questions about accountability, fairness, and justice. Disorders such as schizophrenia, bipolar disorder, PTSD, and antisocial personality disorder can distort judgment, raising difficult questions about responsibility and fairness in the justice system. This review examines the ethical and legal challenges of excusing crime on the basis of mental illness, with a particular focus on how emerging neurotechnologies such as fMRI may shape sentencing outcomes. I discuss how courts determine legal insanity through psychological evaluations, the distinction between Not Guilty by Reason of Insanity (NGRI) and Guilty but Mentally Ill (GBMI), through the potential role of neurotechnology — especially functional magnetic resonance imaging (fMRI) — as supplementary evidence in evaluating criminal responsibility. While fMRI and related tools have potential applications for supporting expert testimony, they cannot yet replace psychological evaluation. A balanced approach is needed, integrating neuroscience with ethical considerations, to ensure that mental illness is neither unjustly punished nor misused as a defense in criminal cases.
Keywords: Criminal Psychology, mental health, ethics, fMRI, drug abuse, justice system
Introduction
Can neurotechnology replace psychological expertise in criminology? This question motivates the present review. Mental illness plays a significant role in Criminal Psychology, influencing a defendant’s behavior and legal outcomes. Multiple mental disorders — such as schizophrenia, bipolar disorder, brain tumors, obsessive compulsive disorder (OCD), drug abuse, Post Traumatic Stress Disorder (PTSD), and antisocial personality disorder — can be seen in criminal behavior. This review focuses on three main areas: 1) Ethical considerations surrounding criminal sentencing for individuals with mental illness, 2) Neurotechnologies, such as fMRI and brain-machine interfaces, that may shape future evidence in criminal cases, and 3) Clinical examples of mental disorders as they appear in criminal psychology, highlighting how neuroscience and legal practice intersect.
Nature vs. Nurture
Is it ethical to excuse someone of a crime based on their mental illness?
One of the oldest debates in criminal psychology is whether it is ethical to dismiss or diminish a punishment for a defendant with mental illness. When discussed, the topic of nature vs nurture is often raised. Does criminal behavior arise more from genetics or environment? Research shows complicated interactions between the two. For example, one could be genetically predisposed to bipolar disorder, but only develop the symptoms of the illness following trauma or stress1. Gene editing technologies (e.g., CRISPR) could be used to modify genes that play a role in predicting criminal behavior. It raises the possibility of eliminating genes affiliated with violence and impulse control. Scholars debate whether it is ethical to excuse criminal responsibility based on mental illness. These technologies are risky, as they can carry the risk of misuse, bias, and other unintended consequences.
The Insanity Plea
The insanity plea is a defense that allowed defendants to claim that their criminal actions are not a reflection of who they are, due to their mental illness. In some cases, the insanity plea may result in a reduced sentence. “Insanity” is often determined by the court of law by evaluating whether the defendant understood their actions or were aware of what they were doing. An expert testimony from psychiatrists and psychologists is conducted to examine the defendant’s mental state for better understanding. The legal standard typically involves the M’Naghten rule, which is the most common form of testing. It focuses on the defendant’s intentions and awareness of their act. Alongside the M’Naghten, the irresistible impulse test could be used to assess if the defendant was in control of their own actions while committing the crime. The model penal code (MPC), is another form of testing commonly involved with the insanity plea, sometimes used in jurisdictions, where they consider whether the defendant had the ability to be aware of their crime when committing it. In U.S law, the plea comes with two main outcomes.
- Not Guilty by the reason of insanity (NGRI)— the defendant avoids imprisonment, instead they are sent to a psychiatric facility.
- Guilty but mentally ill (GBMI)— The individual is still imprisoned but still receives treatment during incarceration.
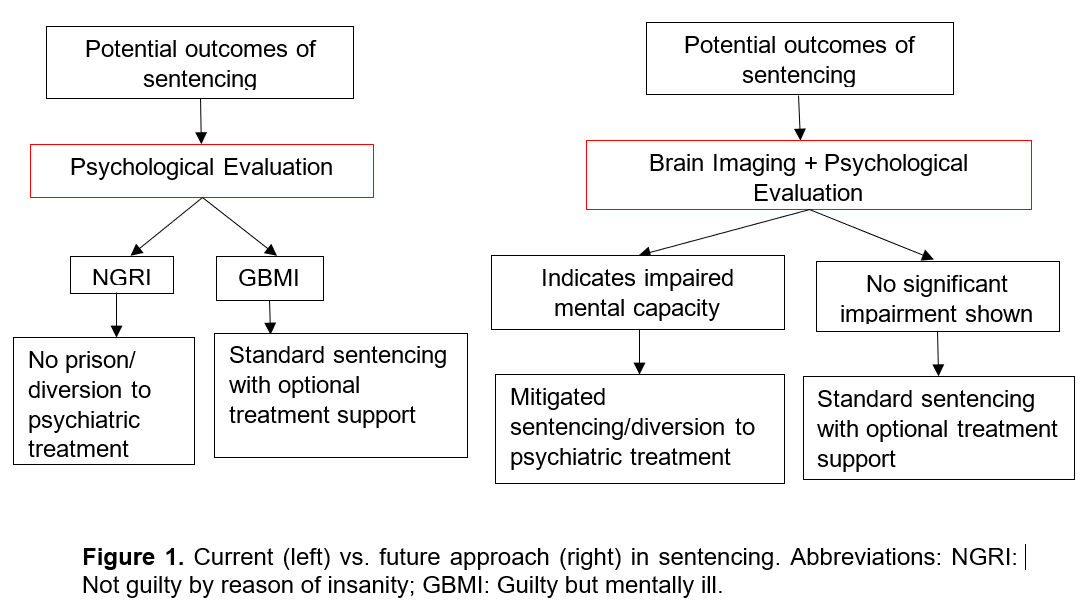
A key question in the field is how to add quantitative evidence to determine the extent to which a criminal falls under the category of NGRI or GMBI. In this review article I explore the potential for neurotechnology to be a useful tool for supporting a psychologist expert opinion. Figure 1 shows the current approach in a legal system when evaluating a defendant with a mental disorder vs. the predicted future approach that could be realized through technological developments.
Neurotechnology in Criminal Psychology
Functional Brain Imaging (fMRI)
FMRI (function magnetic resonance imaging) technology is a brain imaging technology used in criminal psychology, measuring blood flow in the brain, indicating which regions are active during specific tasks2. FMRI is used to study psychopathy, impulse control, and emotional regulation. When examining a fMRI, reduced activities in the prefrontal cortex and amygdala have shown up in violent offenders, as the prefrontal cortex is linked to judgment and the amygdala is linked to fear and empathy. This suggests biological effects in different kinds of criminal behavior. Brain-Machine Interfaces (BMIs) have also been emerging tools that connect neural activity with external devices. One commercial example is Neurable, which has developed consumer-oriented EEG devices.
State-of-the-Art in Lie Detection
Traditional lie detection methods, like the polygraph, galvanic skin response, and electrodermal activity all have been criticized due to unreliability. These methods are not very reliable, since they rely on peripheral physiological changes—such as heart rate, sweating, and even skin conductance—that can be influenced by several factors unrelated to lying, such as anxiety, fear, or even just practicing for control. Lie detection is vulnerable to false negatives and positives, and is rarely admissible in court due to limited reliability.
In contrast, fMRI is often seen as more objective by directly measuring brain activity patterns that are often correlated with deception. Studies found that regions of the brain like the prefrontal cortex are responsible for executive control, which lights up when a defendant lies, implying that fMRI is probably more reliable compared to other lie detection methods3. FMRI can potentially be a factor in determining whether a defendant is Not guilty by reason of insanity (NGRI) or Guilty but mentally ill (GBMI) with identification in brain activity, including abnormal functioning in vulnerable areas in the brain such as the amygdala or anterior cingulate cortex, both being involved with emotion regulation and impulse control. These markers can help determine if someone is truly incapable of recognizing what they were doing while committing the crime, or if they are exaggerating symptoms to avoid accountability.
Still, neuroimaging alone is not reliable. Brain patterns are extremely complex, being a lot more complicated than just black and white. To assure accuracy, neurological evidence should be interpreted with psychological assessments instead of replacing expert testimonies. The goal is to complement it to help psychologists, judges, and juries get more details about a case before making decisions involving the insanity plea, but should not be relied on alone.
In addition to brain-based markers, research from drug abuse studies has seen to also be informative. Chronic substance abuse is often linked to criminal behavior and often results in neurological impairments such as dysfunction in the dopaminergic reward system or damage to the orbitofrontal cortex, which can affect and reduce impulse control, increasing the chances of partaking in risky behavior. By recognizing these parallels found in mental illnesses, researchers might reveal neurological pathways, helping to explain antisocial and criminal tendencies and offer another perspective for assessment and rehabilitation4.
Pre-sentencing phase
For a criminal, there is the pre-sentencing phase and there is the post-sentencing phase. The focus of this review article is on the pre-sentencing phase rather than on the post-sentencing phase. Although questions about remediation are important, they fall outside the scope of this review. Instead, this paper focuses on how mental illness is evaluated before sentencing and its impact on the outcome of a trial.
During the pre-sentencing phase, mental illness may be used as a mitigating factor that can reduce a defendant’s sentence or affect the type of sentence originally imposed onto them. For instance, if the defendant is diagnosed with a severe psychiatric disorder such as schizophrenia, and acts out of character during the crime, it can be shown that the disorder impaired their judgment and control, which can influence the outcome in court. In some cases, this can lead to a lessened charge, such as reduced prison time, or even entirely avoiding incarceration and instead being brought to psychiatric treatment. The legal system considers mental capacity and intent when judging a defendant with expert testimonies from psychologists to psychiatrists. Understanding mental illness in the pre-sentencing phase is crucial, not only to determine outcomes but to ensure a fair sentencing, by considering the nuance in each case. This pre-sentencing phase naturally leads into ethical debates, which I discuss in Section 5.
Commonly referenced mental disorders in criminal psychology
In this section, I discuss several mental illnesses associated with criminal behavior including common symptoms and treatments (Table 1).
Schizophrenia
Schizophrenia is a chronic brain disorder that distorts how an individual thinks, feels, and behaves, described as a disorder of having a distorted reality5. Hallucinations, delusions, paranoia, and disorganized speech are all symptoms shown in schizophrenia characterized by psychosis, suspected to be triggered from genetics, brain chemistry, and/or environmental stressors. Estimates suggest schizophrenia is present in 5–10% of forensic psychiatric populations, compared to 1% in the general population6. Due to its ability to completely alter the way one thinks, acts, and interacts with others, antipsychotic medications such as risperidone, olanzapine, and clozapine are all recommended to reduce hallucinations and stabilize mood, with side effects possibly being sleepiness and weight gain. In addition to medication, cognitive behavior therapy (CBT) is recommended to allow individuals to manage their symptoms and improve how they function7. In criminal psychology, schizophrenia is not an uncommonly seen disorder in individuals when they commit crimes while in a psychotic state, especially when their hallucinations and/or delusions distort their perception of reality. An example of this is the case of John Hinckley Jr, who attempted to assassinate President Ronald Reagan in 1981. Due to his delusions, he was convinced that this would impress a woman named Jodie Foster, who he was obsessively infatuated with. Hinckley was found Not Guilty by Reason of Insanity (NGRI), going under institutional psychiatric care instead8. The public, however, had mixed opinions about this verdict, as many found this unfair. Later, this led to reforms on how insanity defense was used in U.S cases. His case is one example of the ongoing ethical debate between accountability and mental illness, becoming a commonly referenced legal case involving psychology in criminal law.
Bipolar Disorder
Bipolar disorder, once known as manic-depressive illness, is a mood disorder typically characterized by mood swings from depressive to manic/hypomanic9. During a depressive episode, one can experience major sadness, difficulty concentrating, hopelessness, and burnout. On the other hand, in a manic episode, one normally would face irritable moods, inflated sense of self-esteem, decreased sleep, and think/act on impulse, e.g., drug abuse. These mood swings can take a major toll on one’s personal relationships, work performance, and daily functioning, which is why medication is highly recommended for relief. Medications typically include lithium, valproate, or lamotrigine, all of which are proven to stabilize brain chemicals involved in mood regulation10. In addition to medication, cognitive behavioral therapy (CBT) and psychoeducation are important for long-term support. Due to the cognitive distortion and impulsivity caused by manic episodes, it can lead to harmful behaviors such as stealing or endangering others. Still, it is important to note that these crimes are not normally with the intention of causing harm, but rather due to the lack of self-control and distortion that the disorder has on the individual, and that the vast majority of those struggling do not engage in criminal behavior. Due to the weight bipolar disorder has in making decisions, it creates discussions on the fairness of punishments when working with a defendant of the disorder.
Brain Tumor
Brain tumors are clusters of abnormal cells in the brain, typically growing in the frontal lobe or amygdala, caused by cells changing from their original DNA11. This can result in extreme changes in personality, impulsive behavior, poor decision making, and even criminal activity. An example of this is a man named Charles Whitman, who committed an act of mass murder in the University of Texas after killing his own mother. Later, an autopsy revealed there was a tumor pressing on his amygdala, an area in the brain responsible for aggressive behavior and emotional regulation12.
Recent neuropsychological work shows that the impact of brain tumors on criminal behavior depends less on lesion size than on network location. Lesion network mapping was used to demonstrate that tumors affecting networks linked to the orbitofrontal cortex and amygdala are disproportionately associated with aggression, impulsivity, and criminal acts. This underscores the need for nuanced, network-based interpretations rather than automatically associating a tumor to violence13. Treatment for brain tumors often involve surgery, radiation, and chemotherapy. In a legal system, brain tumors raise questions for whether this kind of impairment can lessen the punishment for criminal actions.
Obsessive Compulsive Disorder (OCD)
Obsessive compulsive disorder (OCD) is often defined as having recurring, obsessive and repetitive behaviors. Although OCD is typically not associated with violent crimes, some individuals may commit illegal acts as a response to obsessive fears. OCD can be a very challenging disorder to manage on its own, which is why a form of behavioral therapy combined with medication such as selective serotonin reuptake inhibitors (SSRIs) like fluoxetine is often recommended for those struggling. There have been reported cases of individuals that have committed a crime in attempt to relieve their anxiety, such as compulsively stealing objects. Although these incidents are rare, these suggest that intended harm and compulsive behaviors can be blurred for individuals suffering from severe OCD14.
Substance Abuse
Substance abuse is often defined as harmful use of psychoactive substances such as alcohol and illicit drugs. These substances include cocaine, alcohol, and methamphetamine, which can distort judgement and increase aggression. Addiction can start from several different situations, such as experimental use in social situations, coping with mental illness such as depression, or even after being prescribed to take medicine from a doctor. This abuse of substances is heavily seen in criminal behavior because of the effect drugs and alcohol have on self-control. Treatments often include detox, rehabilitation, and medications such as methadone for opioid addiction. Studies have estimated that over 50% of incarcerated individuals have been diagnosed with a form of substance use disorder15. This alarming statistic suggests a strong connection between addiction and criminal behavior, highlighting the importance of treatment in a justice system. Research consistently shows that comorbid substance use is the primary cause of increased criminal behavior among individuals with mental illness16. A meta-analysis found that once substance use disorders were controlled for, the risk of violence associated with schizophrenia or bipolar disorder was substantially reduced. This highlights the importance of addressing substance abuse in forensic assessments. However, it is important to remember that while substance abuse has been linked to neurological impairments that affect impulse control, it is important to emphasize that this relationship is complex and not deterministic. Many individuals with substance use disorders never engage in criminal behavior, and factors such as environment, prior trauma, and social circumstances play equally significant roles. While substance-induced violence may reduce sympathy for the defendant, some cases recognize comorbidity with mental illness as mitigating. This dual approach reflects a balance of punishment and treatment. Courts therefore must be cautious not to treat this as a direct cause and effect pathway.
Autism Spectrum Disorder (ASD)
Autism spectrum disorder (ASD) is a developmental condition characterized by a spectrum of social interaction difficulties, obsessive behaviors, restricted and repetitive behaviors, and differences in interpretation. ASD can make it difficult to communicate and interact with others, which is why it often makes one find it hard to understand how people feel or think, and changes how one interacts with others. Treatments include applied behavior analysis (ABA) and social skills training. While autism itself does not cause criminal behavior, due to the impact it has on misinterpreting social cues and obsessive interests, it can lead to unintentional violations. The individual may feel as though what they are doing is harmless, which is why the debate of how punishment should be applied in a justice system is brought up when working with a defendant with autism. It is important to understand their intent when assessing an individual with ASD in a legal context17.
Post-Traumatic Stress Disorder (PTSD)
Post-traumatic stress disorder (PTSD) is a mental health condition often shown through exposure to traumas, flashbacks, hyper vigilance, and emotional outbursts. It is often seen among veterans and abuse survivors, due to the nature of those environments. Studies indicate that 15–30% of incarcerated veterans meet criteria for PTSD 18 PTSD can trigger violent and unpredictable behaviors, especially when substance abuse also becomes involved. Treatments such as trauma-focused CBT (Cognitive behavioral therapy), EMDR (Eye movement desensitization and reprocessing), and SSRIs are all recommended for recovery. Studies show that veterans coming from combat zones are at a greater risk of committing a violent crime due to PTSD symptoms 19, which is why it is a disorder considered in the justice system due to the weight it can have on an individual.
Antisocial Personality Disorder (ASPD)
ASPD (Anti-social personality disorder) is defined as a long-term patten of having a lack of empathy, manipulative and aggressive behavior, and the lack of awareness for others. Due to its characteristics, it is strongly linked to criminal behavior, as individuals with ASPD often lack empathy and awareness for others, violating social norms. Treatments are unfortunately normally ineffective, but typically include psychotherapy, mood stabilizers, and antipsychotics. Many infamous criminals have been suspected to have ASPD, such as Ted Bundy. In court, ASPD is not a condition the justice system believes can dismiss a punishment, as the defendant is seen as responsible for their actions despite a lack of remorse20. However, the disorder does spark conversation on rehabilitation.
It is also important to note that large-scale epidemiological studies suggest mental illness alone is a weak predictor of criminal behavior. Population studies show mental illness alone is a poor predictor of criminality. Most crimes committed by individuals with psychiatric diagnoses are unrelated to their symptoms and are instead mediated by factors such as socioeconomic disadvantage, trauma history, and most prominently substance use comorbidity. Reconciling these findings with case law requires careful attention to context. While mental illness may play a role in some cases, generalizations can risk exaggerating its causal impact.21
| Mental Illness | Common Symptoms | Common Treatments/Drugs |
| Schizophrenia | Hallucinations, delusions, disorganized thinking | Risperidone, Clozapine, Cognitive Behavioral Therapy (CBT) |
| Bipolar Disorder | Mood swings (mania and depression), impulsivity | Lithium, Valproate, Lamotrigine, CBT |
| Brain Tumor | Cognitive deficits, mood changes, behavioral issues | Surgery, Radiation, Anticonvulsants, Steroids |
| Obsessive-Compulsive Disorder (OCD) | Obsessions, compulsive behaviors, anxiety | SSRIs (e.g., Fluoxetine), CBT, Exposure Therapy |
| Substance Use Disorder (Drug Abuse) | Cravings, loss of control, compulsive drug seeking | Methadone, Buprenorphine, Naltrexone, Behavioral Therapy |
| Autism Spectrum Disorder | Social difficulties, repetitive behaviors, sensory issues | Behavioral therapy, Educational interventions |
| Post-Traumatic Stress Disorder (PTSD) | Flashbacks, hypervigilance, emotional numbness | SSRIs (e.g., Sertraline), Trauma-focused CBT, EMDR |
| Antisocial Personality Disorder | Disregard for others, deceitfulness, aggression | Psychotherapy, Mood stabilizers, Antipsychotics (limited efficacy) |
Taken together, these disorders reveal important overlaps that challenge legal decision-making. For example, while schizophrenia and PTSD may both impair judgment through delusions or hyperarousal, juries often respond differently depending on expert testimony and the type of evidence presented. Neuroscientific tools such as fMRI are increasingly used to illustrate these impairments, but their influence depends on how courts weigh scientific credibility against traditional legal standards of responsibility. This interaction between clinical diagnosis, expert interpretation, and neurotechnology underscores the complexity of applying psychiatric evidence in real-world trials.
Population-level studies demonstrate that individuals with serious mental illness (SMI) are only slightly more likely to engage in criminal behavior compared to the general population, and that much of the excess risk is attributable to substance use comorbidity. For example, there has been reported a 2–3 fold increase in violent crime among people with schizophrenia compared to controls, though absolute rates remained low20.
Methods
To gather relevant academic sources for this review, a literature search was conducted through Google Scholar, ranging from 1980-2025, a widely known search engine for peer-reviewed journals. The search’s purpose was to identify research related to mental illness in criminal behavior. In addition to Google Scholar, PubMed and SciFinder were used to broaden the scope of the search and ensure inclusion of biomedical and clinical studies relevant to psychiatry, neuroscience, and forensic psychology.
The following keywords were used both individually and in combination to narrow the search: “Criminal Psychology”, “mental health”, “ethics”, “drug abuse”, and “fMRI”. These keywords helped scope out the main themes of the review, including ethical questions on the insanity plea, the impact of disorders on criminal accountability, and the role neuroimaging technologies have in a legal context.
Where possible, this review draws on meta-analytic studies. For example, Fazel & Seewald (2012) provide pooled estimates of violence among patients with schizophrenia, bipolar disorder, and substance use disorders, offering a systematic basis for comparison.
Inclusion criteria required that articles be peer-reviewed and directly address the relationship between mental illness and criminal behavior, the insanity plea, or neurotechnology in forensic contexts. Exclusion criteria included non-English sources, non-peer-reviewed reports, and studies that focused solely on treatment outcomes without legal relevance. A total of 47 sources were initially identified, of which 30 were included in this review after evaluation for relevance and quality.
Discussion
Ethics of Excusing Crime Based on Mental Illness
Building on the clinical and legal frameworks outlined earlier, this section examines the ethical implications.
One of the most debated questions in criminal psychology is the ethics of excusing crime: Is it ethical to excuse someone of a crime based on their mental illness? While mental disorders can impair an individual’s judgment, perception of reality, and ability to control their actions, whether that impairment should affect a defendant’s outcome in a legal system remains a highly complex and controversial topic. The legal use of the Not Guilty by Reason of Insanity (NGRI) plea raises questions about fairness: to what extent should mental illness protect individuals who have committed serious crimes from legal punishment?
Two highly controversial cases that highlight this ethical dilemma involve John Hinckley Jr. and Andrea Yates. Hinckley, who attempted to assassinate President Ronald Reagan in 1981, was found Not Guilty by Reason of Insanity, a verdict that shocked and upset the public. This verdict was made under a version of the American Law Institute (ALI) Standard (1962), which allowed more defendants with mental illness qualify for NGRI, better allowing defendants to be considered insane if they lacked substantial impairment of capacity. The ALI Standard was made as a broader standard to include loss of control after the M’Naghten Rule (1843), a strict insanity standard that focused on cognition, without considering a person’s ability to control their actions when evaluating a defendant22. Although mental health experts testified that Hinckley was suffering from severe psychosis, a poll from ABC news found that 83% of people polled believed justice had not been served, as someone who nearly killed a president was sent to a psychiatric hospital rather than prison23. The Hinckley verdict led to reforms for insanity defenses in several U.S. states, reflecting on the public backlash against leniency. Congress later passed the Insanity Defense Reform Act (1984), making it harder to plead insanity by requiring defendants to prove their insanity with clear evidence and narrowing the definition of insanity24. The ALI Standard was restricted, and the new U.S law was moved closer to the previous M’Naghten approach.
Similarly, Andrea Yates, who drowned her five children while experiencing severe postpartum psychosis, has also been a commonly referenced case in the field. Though she was initially convicted, her verdict was later overturned to NGRI25. While some agreed that the final decision reflected a compassionate understanding of her mental state, others felt that it failed to deliver justice for the victims25. Comparing the two cases, the public reaction was divided, with surveys at the time showing that a majority of Americans opposed the Hinckley decision, while the Yates case similarly sparked national debate25. These reactions highlight the tension between psychiatric expertise and public expectations of justice.
Together, these cases challenge traditional ideas of guilt and punishment. In both, the individuals committed horrific and violent acts, yet were ultimately found not criminally responsible due to mental illness. This raises broader ethical questions: If someone is found legally insane, can society still hold them morally accountable? How should the justice system balance compassion for mental illness with the public’s expectation for punishment and justice?
Still, it Is important to remember that the relationship between psychotic symptoms and criminal behavior is highly complex. While persecutory delusions and command hallucinations have been associated with violent acts, most individuals with psychosis are not violent. Comorbid conditions such as PTSD, OCD, and ASD further complicate this relationship. For instance, PTSD has been linked with impulsive aggression in incarcerated populations, while ASD and OCD are rarely predictive of violence but may influence criminal responsibility through impaired social cognition26.
One goal of this review article was to explore the potential for neurotechnology, especially functional magnetic resonance imaging (fMRI), to provide additional evidence for diagnosing mental illness that might be used in court. These technologies have already been studied in the context of lie detection27, where brain activity is observed in connection with deception. The idea that brain patterns might reliably reveal truth or mental illness raises further questions: Could fMRI be used to distinguish genuine psychiatric conditions from malingering? Could such evidence influence legal outcomes—potentially excusing serious criminal behavior?
While these technologies seem promising, they bring ethical concerns of their own. The prospect of relying on brain scans as admissible legal evidence remains controversial. Should neuroimaging replace clinical judgment? And if so, what would that mean for justice?
Ultimately, excusing criminal behavior due to mental illness should not be resolved by science alone. There must be a balance between compassion for those who are mentally suffering, safety for the public, and respect for the rule of law. As neuroscience and psychology play a growing role in legal decisions, the justice system must continue to evaluate these factors carefully, ensuring that mental illness is neither unjustly punished nor misused as a legal loophole. (As seen in Figure 1.)
The Promise and Limitations of Neurotechnology
Scholars argue that neurotechnology will never replace the expertise of a psychologist, but can provide valuable evidence to be taken into consideration though may not be the most reliable source. One recurring concern in the legal use of neuroimaging is the problem of validity and reproducibility. This is exemplified in the debate over ‘no-lie fMRI,’ a proposed method of lie detection. As brain imaging techniques such as fMRI continue to advance, they also hold the potential to support expert testimonies by offering quantitative measures of brain activity that could affect sentencing outcomes. For example, abnormal functioning in brain regions is related to impulse control and emotional regulation, which might support a claim of reduced culpability from mental illness. By making use of more quantitative measures of brain activity, justice can be upheld28. Experimental studies show that jurors can be influenced by neuroimaging evidence, sometimes assigning it disproportionate weight. However, actual cases of fMRI influencing sentencing remain extremely rare, and courts have generally been reluctant to admit its evidence29.
However, challenges remain, as many are shown through research on “no-lie fMRI”, a method with the purpose of detecting deception based on brain activity. The scientific validity of ‘no-lie fMRI’ remains heavily debated. Scholars highlight issues of replicability, ecological validity, and susceptibility to countermeasures. From a legal standpoint, courts have generally excluded this evidence, citing lack of reliability under Daubert and Frye admissibility standards, the rule that scientific evidence is admissible only if the method or principle is accepted by the science community30. These concerns show that fMRI cannot be considered a scientifically valid lie detection tool at present. Discussed in a Frontier in Human Neuroscience article, “no-lie fMRI” faces limitations in terms of accuracy, as it highlights the difficulty in replicating results in a real-world situation31. These challenges also apply in fMRI in criminal psychology: in the same way it is difficult to confirm whether someone is lying based on a scan, it is equally difficult to confirm whether a defendant was lacking mental compacity while committing a crime. They both attempt to offer insight on invisible mental states from brain data, which means the reliability concerns of “no-lie fMRI” parallel the fMRI-based assessments in legal settings.
In addition to fMRI, there are exciting developments in Brain-Machine Interfaces (BMIs) building on research advances in neuroscience, artificial intelligence, and engineering. In particular, non-invasive neural recording technologies that collect brain data and analyze “brain state” are commercialized. Companies such as Neurable have developed a wearable headphone technology that provides a user with feedback on their level of focus . Still, the emergence of Brain-Machine Interfaces raises new ethical concerns, such as data privacy, predictive use of brain states, and whether these tools could erode the primacy of human judgment in court decisions32. While it is still too early to be used in a legal setting, one day these tools may assist in evaluating mental health, predicting recidivism, and even design personalized rehabilitation methods.
Conclusion
In this review article, I examined the role of mental illness in criminal behavior and the ethical considerations involved in adjusting sentencing based on assessments of mental responsibility. Prior work in lie detection suggests that functional brain imaging may serve as a useful supplement to psychological expertise, potentially contributing to more informed and just verdicts. While neurotechnology — particularly fMRI — provides quantitative insights into brain activity and mental capacity, its limitations must be carefully acknowledged.
The integration of neuroscience in criminal psychology may represent a step towards fairness, though its impact remains debated. These tools can support or challenge expert testimony, but should not replace traditional psychological evaluations.
Ultimately, this review advocates for a balanced approach that respects both the elements of psychological expertise and the potential of emerging neurotechnologies. Mental illness plays a significant role in many criminal cases, and the legal system must recognize the complexity of human behavior. By combining ethical considerations with neuroscientific evidence, courts can strive towards justice that is both legally sound and humane.
Acknowledgements
I would like to thank Professor George McConnell at the Stevens Institute of Technology for the helpful discussions on how to write a review article.
References
- T.E. Moffitt. Genetic and environmental influences on antisocial behaviors: evidence from behavioral–genetic research. Advances in Genetics. 55, 41-104 (2005). [↩]
- R. Bonnie. The moral basis of the insanity defense. American bar association Journal. 69, 194-197 (1983). [↩]
- N. Feigenson. Brain imaging and courtroom evidence: on the admissibility and persuasiveness of fMRI. International Journal of Law in Context. 2, 233-255 (2006). [↩]
- D. P. McCabe, A. D. Castel, M. G. Rhodes. The Influence of fMRI Lie Detection Evidence on Juror Decision-Making. Behavioral Sciences & the Law. 29, 566-577 (2011). [↩]
- K.S. Kendler. The genetics of schizophrenia: A current, genetic-epidemiologic perspective. Schizophrenia Bulletin. 19, 261-285 (1993). [↩]
- S. Fazel, N. Långström, A. Hjern, M. Grann, P. Lichtenstein. Schizophrenia, Substance Abuse, and Violent Crime. JAMA. 301, 2016-2023 (2009). [↩]
- T. Rahman, J. Lauriello. Schizophrenia: An Overview. FOCUS. 14, 300-307 (2016). [↩]
- D. Capps. John W. Hinckley, Jr.: A case of narcissistic personality disorder. Pastoral Psychol. 62, 247-269 (2013). [↩]
- L. Tondo, G.H. Vazquez, R. J. Baldessarini. Depression and mania in bipolar disorder. Current Neuropharmacology. 15, 353-358 (2017). [↩]
- N. Brunello. Mood stabilizers: protecting the mood…protecting the brain. Journal of Affective Disorders. 79, 15-20 (2004). [↩]
- R. Wechsler-Reya, M. P. Scott. The developmental biology of brain tumors. Annual Review of Neuroscience. 24, 385-428 (2001). [↩]
- G. Sajeev. The Texas tower shooter: An analysis of Charles Whitman. Scholarly review. 5, 76-81 (2023). [↩]
- R. Darby, A. Horn, F. Cushman, M. Fox. Esion network localization of criminal behavior. Proc Natl Acad Sci USA. 115, 601-606 (2017). [↩]
- D.J. Stein, D. L. C. Costa, C. Lochner, E.C. Miguel, Y.C. Janardhan Reddy, R. G. Shavitt, O.A. van den Heuvel, H. Blair Simpson. Obsessive–compulsive disorder. Nature Reviews Disease Primers. 5, 52-60 (2019). [↩]
- S. Fazel, I. A. Yoon, A. J. Hayes. Substance use disorders in prisoners: an updated systematic review and meta-regression analysis in recently incarcerated men and women. Addiction. 112, 1701-1724 (2017). [↩]
- J.Volavka, J.Swanson. Violent Behavior in Mental Illness: The Role of Substance Abuse. JAMA. 304, 563–564 (2010). [↩]
- O. P. O’Sullivan. Autism spectrum disorder and criminal responsibility: historical perspectives, clinical challenges and broader considerations within the criminal justice system. Irish Journal of Psychological Medicine. 35 333-339 (2018). [↩]
- U. Orak. From Service to Sentencing: Unraveling Risk Factors for Criminal Justice Involvement Among U.S. Veterans. Council on criminal justice. October (2023). [↩]
- J. J. Collins, S. L. Bailey. Traumatic stress disorder and violent behavior. Traumatic Stress. 3, 203-220 (1990). [↩]
- D. W. Black. Bad Boys Bad Men. third Edition, (2022). [↩] [↩]
- R. Andrew. J. Piel, M.Makey Jr. Competency to Stand Trial and Defendants Who Lack Insight into Their Mental Illness. American Academy Psychiatry Law Journal. 41, 85-91 (2013). [↩]
- R. Andrew. J. Piel, M.Makey Jr. Competency to Stand Trial and Defendants Who Lack Insight into Their Mental Illness. American Academy Psychiatry Law Journal. 41, 85-91 (2013). [↩]
- D.Whiting, P.Lichtenstein, S.Fazel. Violence and mental disorders: a structured review of associations by individual diagnoses, risk factors, and risk assessment. The Lancet Psychiatry. 8,150-161 (2021). [↩]
- D.Whiting, P.Lichtenstein, S.Fazel. Violence and mental disorders: a structured review of associations by individual diagnoses, risk factors, and risk assessment. The Lancet Psychiatry. 8,150-161 (2021). [↩]
- A. Banerji. Infanticide: Who is to blame? A look into Andrea Yates. Women Leading Change: Case Studies on Women, Gender, and Feminism. 8, 73-94 (2024). [↩] [↩] [↩]
- O. P. O’Sullivan. Autism spectrum disorder and criminal responsibility: historical perspectives, clinical challenges and broader considerations within the criminal justice system. Irish Journal of Psychological Medicine. 35 333-339 (2018. [↩]
- M. J. Farah, J. Benjamin Hutchinson, E. A. Phelps , A. D. Wagner. Functional MRI-based lie detection: scientific and societal challenges. Nature Reviews Neuroscience. 15, 123-131 (2014). [↩]
- A.Fel. The Pros and Cons of Neuroscience in the Legal System. Biofocal. 44, 1-21 (2023). [↩]
- G. Stevens. ‘My Brain Made Me Do It?’ Reflections on the Role of Neuroscience in Assessing Criminal Responsibility – A South African Medico-legal Perspective. Psychiatry, Psychology and Law. 27, 202–213, (2020). [↩]
- A. Roskies, N. Schweitzer, M. Saks. Neuroimages in court: less biasing than feared. Forum: Science & Society. 17, 99-101, (2013). [↩]
- E. Rusconi, T. Mitchener-Nissen. Prospects of functional magnetic resonance imaging as lie detector. Frontier Human Neuroscience. 7, 1-12 (2013). [↩]
- H. Yang, L. Jiang. Regulating neural data processing in the age of BCIs: Ethical concerns and legal approaches. Digital Health. 11, 1-19 (2025). [↩]



{kind=link}