
Abstract
Although public opinion on CRISPR-Cas9 gene editing technology has been extensively studied, the existing literature overwhelmingly represents older populations and underrepresents younger demographics despite age being a significant predictor of opinion found in previous studies. We explored how high school students, a previously unstudied age demographic, perceived CRISPR-Cas9 gene editing in various medical contexts. A survey-based method was used to evaluate high school students’ (N=102) attitudes in a co-educational private Catholic school. We hypothesized that high school students would share similar views with the public on specific uses of CRISPR-Cas9 but would support the technology across a broader range of uses. The students had a positive attitude towards using CRISPR-Cas9 for preventing life-threatening and debilitating diseases, infertility treatment, and genome research. However, few supported its use for physical, cognitive, or personality enhancements. The students recognized that CRISPR-Cas9 usage for medical purposes and enhancement-related purposes posed different ethical challenges. When compared to other studies that studied older demographics, the students supported similar uses of CRISPR-Cas9 and expressed comparable ethical concerns. However, we also found that, on average, private high school students showed greater support for all uses of CRISPR-Cas9 compared to participants representing the public in previous studies. Given the limitations of this study and the limited knowledge of the opinions on CRISPR-Cas9 of this demographic, further research must be conducted to qualify the findings of this study.
Keywords: CRISPR-Cas9, genome editing, survey, high schoolers, public opinion
Introduction
CRISPR-Cas9 (Clustered Regularly Interspaced Short Palindromic Repeats and CRISPR-associated protein 9) is a revolutionary gene-editing technology that allows scientists to precisely modify DNA in living organisms. Its ability to target, cut, and edit specific DNA sequences with high accuracy has transformed biomedical research, agriculture, and potential therapeutic applications. In 2023, the FDA approved its first gene-editing-based therapy for sickle cell disease1. This marked a significant development in genetic medicine, demonstrating the potential of CRISPR-Cas9 to treat hereditary diseases. However, CRISPR-Cas9 has also sparked ethical debates surrounding the implications of altering human genetics. In 2015, a group of researchers attempted to edit human tripronuclear zygotes to understand the efficiency of CRISPR-Cas9 in human zygotes2. Following this study, human zygote editing was denounced by many academic journals3.
However, the public attention surrounding Liang’s study was overshadowed by the global controversy sparked by Dr. Jiankui He’s experimentation on twin girls in 2018. Dr. He used CRISPR-Cas9 gene editing to modify the embryos of the twins to make them resistant to HIV4. This research violated numerous laws surrounding research and experimentation and rapidly publicized CRISPR-Cas9 in the media4. One issue with Dr. He’s research is that there was a lack of peer and public review, showing the need for a clearer society-science dialogue. Thus, many studies attempted to grow this society-science dialogue by conducting public opinion surveys on CRISPR-Cas9.
Current research on global public opinion regarding CRISPR-Cas9 shows a general trend of support for medical applications but opposition to non-medical uses. A worldwide survey conducted on this topic showed strong approval of health-related applications of gene editing but moral opposition to enhancement applications, though their study had sampling biases, including an overrepresentation of young adults and an underrepresentation of other age groups5. Another study focusing on Western countries found higher support for medical uses but similar levels of opposition to non-medical uses of CRISPR-Cas9, suggesting that cultural differences influence perspectives6,7. While both studies agree that support for CRISPR-Cas9 is context-dependent, their broad sampling limits demographic-specific conclusions and inferences about any populations outside of the global scale. A study surveying Australians’ opinions on the topic found similar results as the two studies above along with various predictors of opinion, including age, literacy, and religiosity8. However, despite the study finding that age influences opinion, the study did not include any participants below the age of 18, hindering a full understanding of age-related opinion trends.
The culmination of these studies shows that there is a lack of research on public opinion of CRISPR-Cas9 targeting specific demographics of the population, especially high schoolers. Due to CRISPR-Cas9’s relevance in both modern and future policy making, it is vital to evaluate the opinions of a generation that is soon going to be handling the ethical and scientific implications of this technology. Therefore, the central research question of this paper is: How do high school students perceive CRISPR-Cas9 gene editing technology across various medical applications, and how do their views compare to those of the public as reported in previous studies? We will also analyze how demographic factors influence participants’ responses. After analyzing the literature surrounding this topic, we hypothesized that high schoolers would view genetic editing positively for most forms of disease treatment but not human enhancement. Additionally, we proposed that they would express greater approval of technology compared to the general public.
Due to time and logistical constraints, the sample size of 102 represents the high school population of approximately 800 at the p < 0.05 level with a margin of error of approximately ±9.1%, limiting the precision of the study. Additionally, since religion influences the participants’ ethical standpoints, the results of this study cannot be generalized to non-Catholic private schools9. Because most of the participants of this study were white, this study should also not be generalized to private schools with a more diverse student body (see Appendix A for race/ethnicity data). Moreover, most of these students are from higher income brackets, causing generalizability to be limited to this socioeconomic status (see Appendix B). Biases from the school environment may have also been introduced to the study because of our positions as student researchers.
Materials and Methods
A survey was conducted to assess support levels of various medical usages of CRISPR-Cas9 among secondary schoolers between the ages of 14-18. The objective of the survey was to evaluate how high schoolers reacted to various usages of CRISPR-Cas9 and how various background factors influenced their views. The survey collected data relating to public opinion using a 5-point Likert scale (1=Strongly disagree, 7=Strongly agree) to evaluate levels of support for each of the usages of CRISPR-Cas9.
Participants
This study collected data from students from a private Catholic school in Maryland with a student population of approximately 800 in grades 9-12. A total of 102 students were surveyed anonymously between January 27 and February 24, 2025. Student personal information was kept confidential throughout the data collection process.
Materials
The survey was provided to participants via Microsoft Forms. The first section of the survey asked participants to identify their age, grade level, gender, religiosity, ethnicity, if they have a family member with a serious illness, if they have family in the medical field, household income, and support level for science and technological advancements (see Appendices A-C to find data on all of the demographic factors). Following the collection of basic demographic information, participants were asked an open-ended question regarding their level of knowledge of CRISPR-Cas9. The responses were then coded based on whether the participant made an incorrect statement on CRISPR-Cas9, made a partially correct statement on CRISPR-Cas9, or made a correct statement on CRISPR-Cas9.
The respondent was then asked to read information regarding CRISPR-Cas9 (see Appendix D). This was done to inform the respondent of CRISPR-Cas9 if they had not heard of it or made an incorrect statement about it. While giving the participants a description of CRISPR-Cas9 would prime them and influence their responses, it was necessary to establish a baseline of understanding. This would ensure that respondents weren’t using uninformed guesses in their responses. The following questions had participants state their level of support for various usages of CRISPR-Cas9 on a Likert scale. Lastly, the participants were asked if they were willing to use CRISPR-Cas9 on their children if they had children and asked to elaborate further in a free-response question (see Appendix D for actual wording of all questions).
Statistical Analyses
Multi-ordinal regression analysis was used to evaluate the significance between the predicting factors and the opinions on CRISPR-Cas9 measured using a Likert scale. However, due to the large amount of predicting factors for a relatively small sample, there is an increased risk of type II errors. 9 predicting factors were selected for the multi-ordinal regression: Age, participants’ experience with serious illnesses, family in healthcare, religious affiliation, levels of CRISPR-Cas9 knowledge, income level, support of science, concerns over scientists’ power, and trust in science (see Appendices A-C for the data used for the predicting factors). Religiosity was coded numerically (scale 1-10) with 1 being self-described low religiosity and 10 being self-described high religiosity. Given that missing data were minimal (<1%) for religiosity, median imputation was employed to preserve the complete sample size while providing a robust and conservative central value unaffected by outliers.
The free-response question was coded according to Appendix F, and a thematic analysis was performed to find patterns in respondents’ answers.
To assess demographic differences between this study and 2 other studies, significance was tested using Welch’s t-test, and effect sizes were calculated using Hedges’ g. We selected literature that used similar Likert scales and posed questions in a style closely aligned with our own. The studies selected were Scheufele et al.’s study on American adults and Armsby et al.’s study on genetics professionals10,11. Because most literature surrounding this topic focused on CRISPR-Cas9 for disease uses and CRISPR-Cas9 for enhancement purposes, the data for questions of those specific types were combined and averaged for comparative analysis. For example, the data for the first two questions (life-threatening and debilitating diseases) were averaged and used as one dataset in the statistical comparison. The 3 enhancement questions (physical, cognitive, and personality enhancement) similarly averaged. For Scheufele et al.’s study, it was necessary to transform 7-point Likert scales to 5-point Likert scales to gain usable data. A linear scaling formula to convert these values was used:
𝑿5 = (𝑿7 – 1)(4/6) + 1
Derived from this formula, the mean and standard deviation formulas are as follows:
𝝻5 = (𝝁7 – 1)(4/6) + 1
𝛔5 = (𝛔7)(4/6)
This transformation introduces measurement error as a limitation, given the ordinal nature of Likert scales and the non-uniform psychological distance between points12. However, omitting this relevant study would introduce selection bias. Thus, they were included for the sake of statistical comparisons.
Results
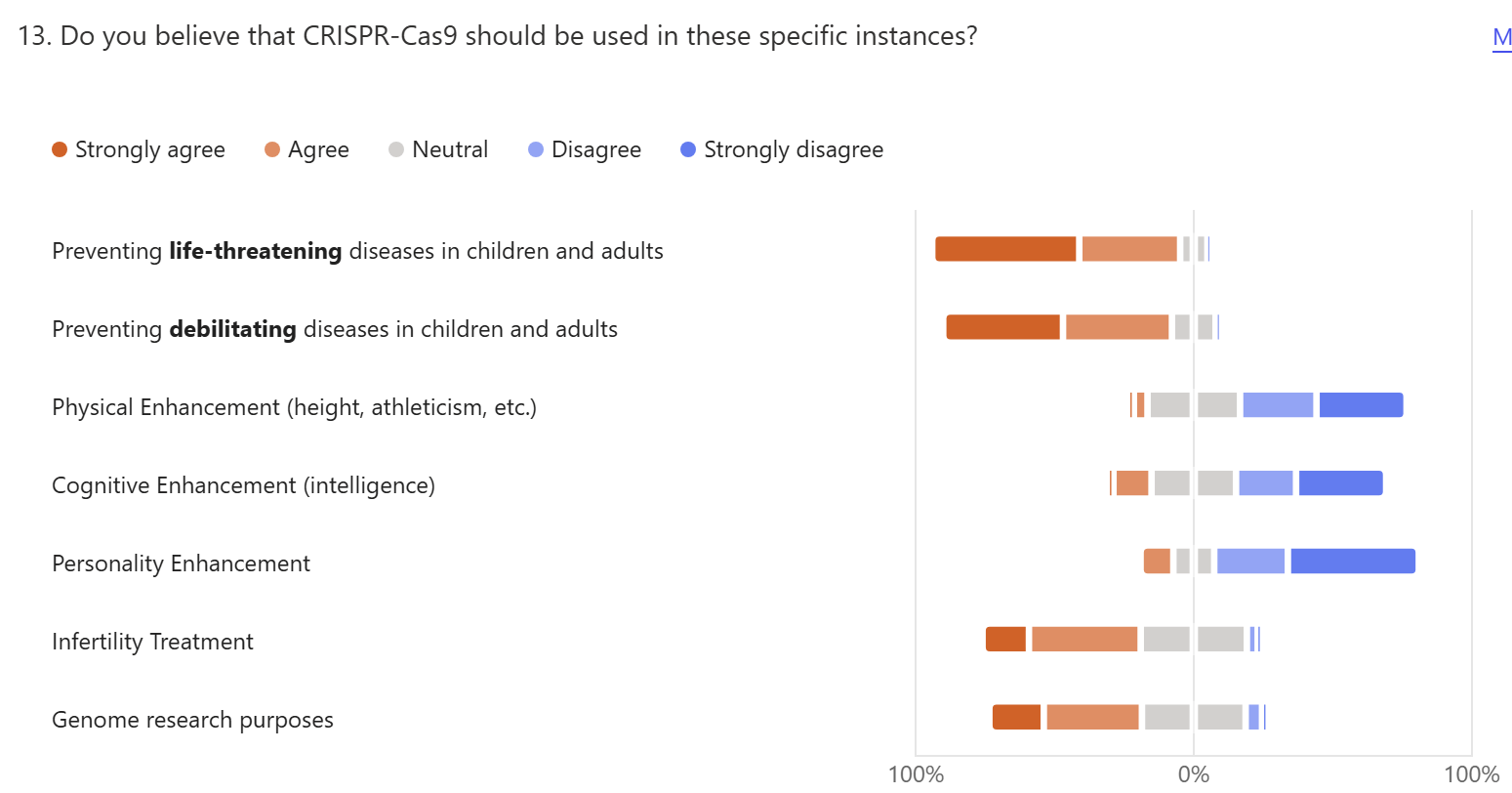
The students had a positive opinion towards medical-related usages of CRISPR-Cas9, including using it to prevent life-threatening diseases (52.9% Strongly agreeing; 36.3% Agreeing) and debilitating diseases (43.1% Strongly agreeing; 39.2% Agreeing), infertility treatment (16.7% Strongly Agreeing; 40.2% Agreeing) and genome researching purposes (19.6% Strongly Agreeing; 35.3% Agreeing), but they opposed its usage for any physical (2% Strongly Agreeing; 4.9% Agreeing), cognitive (2% Strongly Agreeing; 13.7% Agreeing), or personality (11.8% Agreeing) enhancements (Figure 1).
When asked to further elaborate on their answers, participants frequently stated that they were hopeful for the technology’s potential to treat various health conditions. One participant responded that “CRISPR-Cas9’s potential to treat health conditions is promising, especially for those that are not easily treated with current technology.”
However, many participants also brought up concerns about designer babies, intervention in nature, and “playing God.” Almost all respondents considered using CRISPR-Cas9 for any form of enhancements to be “immoral” and feared the use of it in this way: “Using a technology to alter lives can be argued to be inhumane, and for some aspects, solving problems that can also be worked toward manually can be considered as a way for parents to disregard their kid.” The normalization of genetically enhanced children was also feared: “I don’t think using it for aesthetic or unfair advantages would be good because it then makes the extraordinary ordinary.” Another respondent described this normalization as making a sort of “superhuman.”
The free-response question gave a general consensus that while medical treatment for preventable diseases is supported, enhancement of traits is not. Themes from the free-response question are summarized in Table 1.
| Theme | # | Example |
| Support mentioning saving lives | 54 | “It is best that my child gets the medicine that he needs for a life-threatening illness and it should be treated.” |
| Support mentioning therapy, improving quality of life | 47 | “I think it would be good to use in scenarios of bettering the condition of someone’s life (preventing disease).” |
| Only use for diseases | 40 | “If it was life-threatening or prevent them from getting diseases I would, but I don’t find any need in changing physical appearance, intelligence, or personality.” |
| Risks, unknown consequences, safety | 17 | “The idea of changing my child sounds scary for me and the child. I wouldn’t want to risk both of our lives.” |
| Parents can’t impose on child | 14 | “I think each person needs to be themselves and not personalized by their parents.” |
| Not needed, average/normal is OK | 12 | “I personally would never use it on my children. Everyone is beautiful the way they are.” |
| Undermines character, loss of humanity | 11 | “I believe some of the options could further help individuals for the better but others take away from natural humanity.” |
| Obtaining an unfair advantage | 9 | “I don’t think using it for aesthetic or unfair advantages would be good because it then makes the extraordinary ordinary.“ |
| Unethical, immoral | 8 | “Using this technology to enhance humans is too unethical.” |
| Support mentioning parents wanting the best | 8 | “I can edit my kids to be the best they can be physically, and to prevent diseases.” |
| Playing God, unnatural | 8 | “I would like to benefit my child in health, not in their personality or looks, it feels unnatural.” |
| Uncertain, can’t decide | 4 | “I am not sure, I don’t know enough about this topic.” |
The results of the multi-ordinal regression analysis are summarized in Table 2. The 5-point likert scale was coded numerically on a scale from 1 to 5 (1 = Strongly disagree, 5 = Strongly agree). The multi-ordinal regression analysis yielded 4 instances of significance (p<0.05) across the 7 different models. Those with family in health care were 3.36 times as likely to support physical enhancement uses of CRISPR-Cas9 compared to those without (OR = 3.36, 95% CI [1.08, 10.48], p < 0.05). For each one-year increase in age, participants were 1.57 times as likely to be supportive of infertility treatment using CRISPR-Cas9 (OR = 1.57, 95% CI [1.01, 2.45], p < 0.05). Additionally, respondents who were more supportive of science were 4.41 times as likely to support this use of CRISPR-Cas9 (OR = 4.41, 95% CI [1.62, 12.02], p < 0.05). Lastly, for each one-point increase in self-identified religiosity, respondents were 0.76 times as likely to support CRISPR-Cas9 for genome research purposes (OR = 0.76, 95% CI [0.61, 0.95], p < 0.05).
| Model 1 OR(95% CI) | Model 2 OR(95% CI) | Model 3 OR(95% CI) | Model 4 OR(95% CI) | Model 5 OR(95% CI) | Model 6 OR(95% CI) | Model 7 OR(95% CI) | |
| Age | 1.68 (0.80,3.55) | 1.02 (0.64,1.64) | 0.76 (0.46,1.26) | 0.91 (0.58,1.43) | 0.68 (0.42,1.10) | 1.57 (1.01,2.45)* | 0.92 (0.61,1.37) |
| Serious illness | 0.61 (0.09,4.08) | 0.38 (0.08,1.67) | 0.68(0.20,2.35) | 0.67 (0.23,2.00) | 0.70 (0.19,2.51) | 0.67 (0.24,1.89) | 0.92 (0.29,2.91) |
| Family in health services | 4.56 (0.65,31.61) | 2.55 (0.68,9.61) | 3.36 (1.08,10.48)* | 1.14 (0.42,3.12) | 2.23 (0.64,7.76) | 1.62 (0.63,4.19) | 0.55 (0.21,1.39) |
| Religious affiliation | 1.29 (0.86,1.93) | 0.79 (0.57,1.10) | 0.80 (0.63,1.03) | 0.94 (0.76,1.17) | 0.89 (0.69,1.15) | 0.87 (0.70,1.10) | 0.76 (0.61,0.95)* |
| CRISPR expertise | 0.51 (0.11,2.29) | 1.68 (0.42,6.80) | 0.60 (0.20,1.76) | 1.34 (0.52,3.44) | 0.41 (0.11,1.54) | 0.96 (0.42,2.18) | 0.96 (0.41,2.24) |
| Income level | 1.19 (0.55,2.61) | 1.06 (0.62,1.81) | 1.55 (0.92 2.61) | 1.13 (0.72,1.77) | 1.27 (0.73,2.19) | 1.06 (0.70,1.60) | 1.08 (0.73,1.59) |
| Support of science | 4.11 (0.89,19.01) | 1.15 (0.34,3.94) | 0.67 (0.23,1.86) | 2.48 (0.95,6.48) | 1.24 (0.45,3.42) | 4.41 (1.62,12.02)* | 1.15 (0.43,3.04) |
| Concern over scientist’s power | 1.60 (0.41,6.28) | 1.61 (0.64,4.06) | 2.38 (1.07,5.25) | 1.49 (0.71,3.13) | 1.98 (0.78,5.00) | 0.84 (0.44,1.60) | 1.48 (0.76,2.87) |
| Trust in science | 2.02(0.51,8.01) | 1.71 (0.62,4.74) | 1.15 (0.48,2.72) | 0.75 (0.35,1.59) | 0.92 (0.37,2.32) | 1.11 (0.53,2.34) | 1.54 (0.75,3.16) |
The comparative analysis between this study and 2 other studies is summarized in Table 3 and Table 4. For the comparisons between the studies’ support levels of medical purposes for CRISPR-Cas9, we found that there was a large difference between our study and another study on American adults (g = 0.74, p < 0.001). This implies the high school students in our study supported CRISPR-Cas9 for this use significantly more frequently than the population studied in Scheufele et al.’s study13. There was no significant difference between the opinions of private high schoolers and genetic professionals (p > 0.05).
| Study and Population | Application | n | x̄ | SD | Hedges’ g | p |
| Our Study: Private high schoolers | Life-threatening and debilitating disease prevention | 102 | 4.32 | 0.75 | – | – |
| Scheufele et al. American adults | Treating medical conditions | 1600 | 3.53* | 1.08* | 0.74 | < 0.001 |
| Armsby et al. Genetics professionals Ages 20-39 | Therapeutic applications | 262 | 4.22 | 0.91 | 0.12 | > 0.05 |
Note: Values marked with an asterisk have been transformed according to the formulas outlined earlier in the Statistical Analyses subsection under Methods.
For the comparisons between the studies’ support levels of enhancement purposes for CRISPR-Cas9, we found there was a medium-sized difference between our population and a population of American adults. The negative value indicates that our own population rated this use of CRISPR-Cas9 less favorably than American adults13. When compared to a population of genetics professionals, we found that there was a minor difference between the populations (g = 0.33, p < 0.05). Our population tended to support CRISPR-Cas9 uses slightly more frequently than genetics professionals.
| Study and Population | Application | n | x̄ | SD | Hedges’ g | p |
| Our Study: Private high schoolers | Human trait enhancements | 102 | 2.12 | 1.06 | – | – |
| Scheufele et al. American adults | Enhancing or selecting human abilities | 1600 | 2.87* | 1.15* | -0.66 | < 0.001 |
| Armsby et al. Genetics professionalsAges 20-39 | Enhancement applications | 262 | 1.80 | 0.93 | 0.33 | < 0.05 |
Note: Values marked with an asterisk have been transformed according to the earlier Statistical Analyses subsection under Methods.
Discussion
We found that high school students supported the usage of CRISPR-Cas9 for the majority of medical uses except physical and mental enhancements. This is in line with other studies that have analyzed public opinion (including university students) on CRISPR-Cas95,14,15. The reasoning behind the opinions of students aligned with many of the reasons found in other studies. There were ethical and moral arguments against CRISPR-Cas9 for non-medical uses. Common arguments against such applications include the idea that humans would be “playing God” or “imposing parental beliefs on children.” The majority of these arguments fall under the ethical principles of autonomy and non-maleficence because of the fundamental belief of respecting an individual’s right to self-determination and protecting them from potential harm16. Similar objections have been identified in other studies, with the most prevalent concern of individuals losing human diversity17,18. This implies that high schoolers and the public hold similar reasons for their lack of support for enhancement uses of CRISPR-Cas9. Additionally, this study confirms that high schoolers, like participants in other research, express optimism about CRISPR-Cas9’s potential for medical applications17,18. This aligns with the principle of beneficence, showing that they view CRISPR-Cas9 in some contexts as a way to promote human welfare16.
Our multi-ordinal regression analysis was only significant for four demographic factors, with none of them influencing any more than one use of CRISPR-Cas9. Other studies have also noted that age, prior knowledge of CRISPR-Cas9, and religious affiliation have a more significant effect on opinions in comparison to this study5,8. This study only saw age be a significant predictor variable in the “infertility treatment” variable (see Appendix A for data on age distributions). However, other studies saw age predicting factors such as CRISPR-Cas9 usage for cosmetic purposes and non-disease characteristics5,13. This suggests that while there is a distinction between the general public and students in school, there is minimal difference among the age groups of 14 to 18. In both this paper and other research papers, family involvement in healthcare was not significant (see Appendix C for data on responses for family involvement in healthcare)14. Additionally, in this study, religious affiliation was only found to be a significant predictor for how participants viewed CRISPR-Cas9 for “genome research purposes” (see Appendix B for data on religiosity). In other studies, those with higher religiosity opposed more applications for CRISPR-Cas9 than was seen in this study5,8. However, this is likely because the private Catholic school setting of this study would influence participants’ responses regardless if they self-reported high religiosity or not.
Our results from the comparative analysis show our population’s strong support for medical applications when compared to other populations. The large, significant difference from the American public (Table 3) suggests a generational shift in viewing CRISPR-Cas9 as a tool for treatment. Moreover, we also found no significant difference to genetics professionals’ views on this use, indicating that these two groups share a consensus that CRISPR-Cas9 is highly promising for future health treatment purposes (Table 3). For enhancement applications, the students demonstrated significant caution when compared to the American public, rejecting imposing traits or “playing God” (Table 4). However, they were shown to be slightly more supportive of this application of CRISPR-Cas9 when compared to genetics professionals (Table 4). This indicates a more open stance on enhancement applications of CRISPR-Cas9 compared to the conservative views of experts.
This study has found that high schoolers support the usage of CRISPR-Cas9 for severe ailments; however, they do not support its usage for superficial purposes. Moreover, this aligns with broader public sentiment, where the potential for CRISPR-Cas9 to be used for genetic modifications perceived as unnecessary or cosmetic is met with resistance. The underlying concerns are largely centered around the fear of creating inequalities, as genetically modified traits could lead to a divide between those who have access to such technologies and those who do not. Additionally, the idea of “designer babies” and the ethical implications of altering traits like intelligence or personality were seen as disrupting societal norms.
Since scientific literacy in schools, especially in biotechnology, has decreased relative to the amount of developments in biotechnology in the last 3 decades, further education in this field is needed for students to make informed decisions in the future19,20,21,22. This literacy gap underscores a failure of science curricula to keep pace with innovation, leaving students unprepared for new genetic technologies23 24 25. This study confirms the importance of science communication in biotechnology, and we believe that, in the long term, science education and clarity will help society understand the relevance of biotechnologies in the future23,24.
Given the limitations of this study in sample size and generalizability, future studies should select a sample from multiple schools, representing a broader range of students. This would alleviate the limitations in sample size this study had and give future studies more generalizability.
Appendices
Appendix A: Demographic characteristics of respondents. A) Bar graph showing self-reported race or ethnicity; participants could select multiple options. B) Pie chart displaying participant age distribution. C) Donut chart representing participant grade levels. D) Donut chart showing participant gender self-identification.

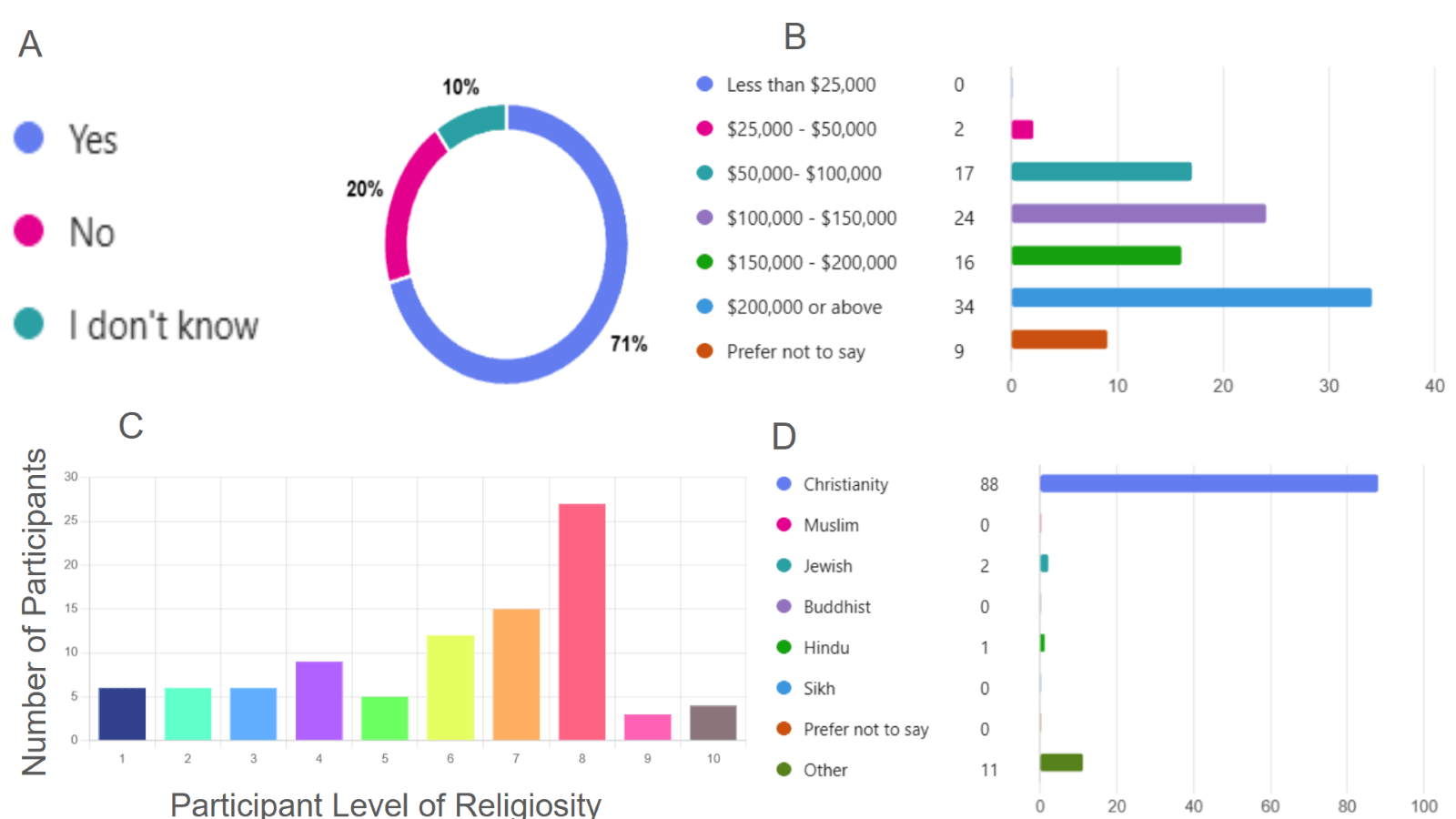
Appendix B: Background characteristics of survey respondents. A) Donut chart showing responses to whether participants or their family members have experienced a serious illness. B) Bar graph of self-reported incomes. C) Bar graph showing participant self-ratings on religiosity (scale of 1-10). D) Bar graph indication religious affiliation of respondents
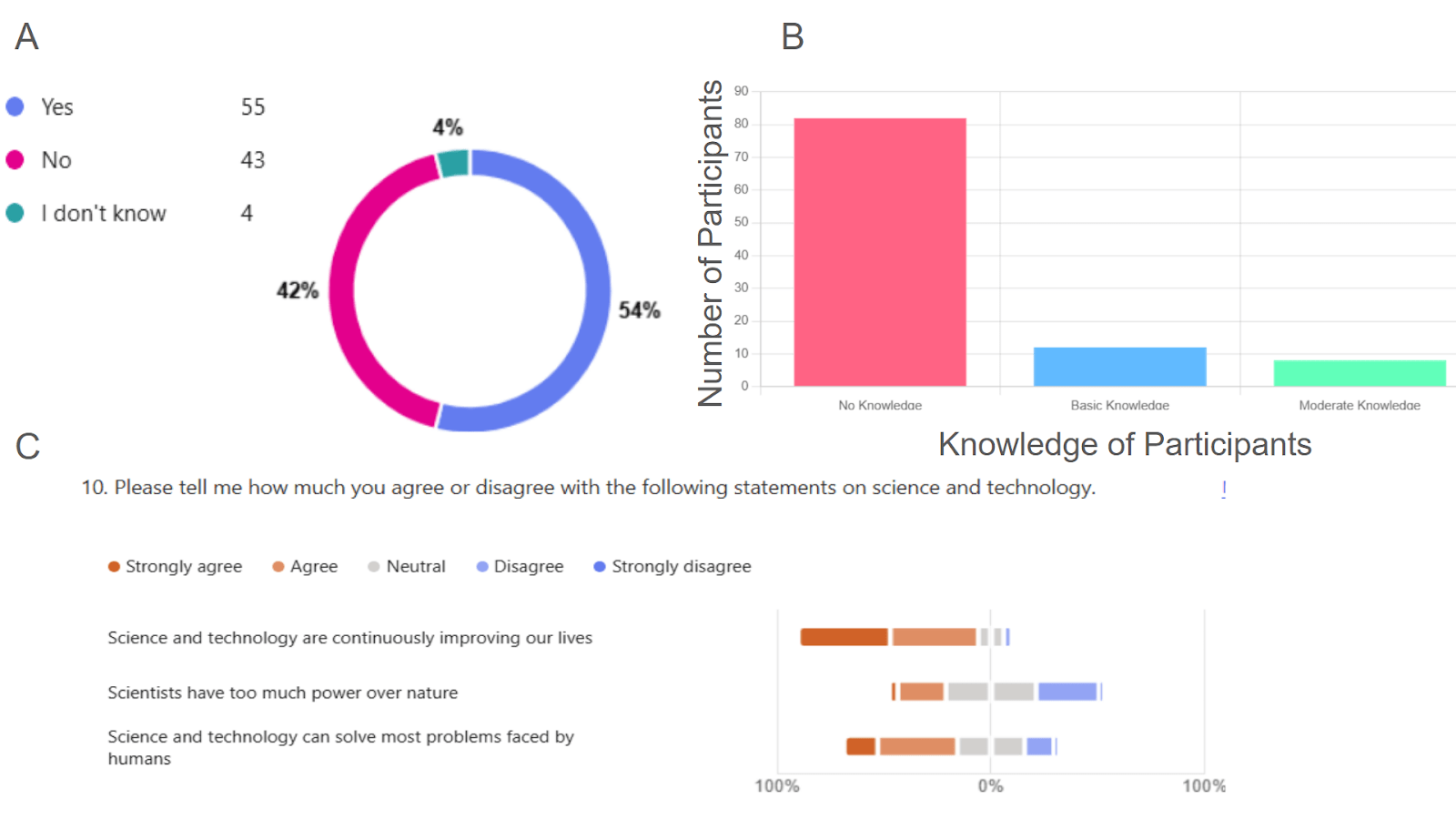
Appendix C: Participant connections to healthcare, support for science and technology, and knowledge of CRISPR-Cas9. A) Donut chart showing the percentage of respondents who have family members involved in medical fields. B) Bar graph indicating participants’ level of knowledge on CRISPR-Cas9. C) Diverging bar chart showing the percentage of participants who supported various aspects of science and technology development (scale from “Strongly Disagree” and “Strongly Agree” ).
Appendix D
My name is Dylan Vo, and I am a junior in an AP Research class. For my AP Research project, I am collecting data on how high schoolers’ view CRISPR-Cas9 in different medical contexts. Thank you for taking the time to fill out my survey. Please only fill out this survey once.
This section will collect some basic demographic information.
- Gender:
a. Female
b. Male
c. Prefer not to say
- Age:
a. Grade Level:
b. Freshman
c. Sophomore
d. Junior
e. Senior
- Race or Ethnicity (check all that apply):
a. Black or African American
b. Asian or Pacific Islander
c. Hispanic or Latino
d. White
e. American Indian or Alaskan Native
f. Prefer not to say
g. Other
- Have you or a family member had a serious illness (e.g. cancer, diabetes, heart disease, etc.)
a. Yes
b. No
c. I don’t know
- Do you have any family members who work in any fields related to biological sciences or healthcare?
a. Yes
b. No
c. I don’t know
- Household Income (estimate if you don’t know)
a. Less than $25,000
b. $25,000 – $50,000
c. $50,000 – $100,000
d. $100,000 – $150,000
e. $150,000 – $200,000
f. $200,000 or above
g. Prefer not to say
- Religious Affiliation:
a. Christianity
b. Muslim
c. Jewish
d. Buddhist
e. Hindu
f. Sikh
g. Prefer not to say - If you list a religion on the previous question, how involved are you in your faith from a scale of 1-10? With 1 being not involved and 10 being very involved.
- Please tell me how much you agree or disagree with the following statements on science and technology. Note: This question was asked on a 5 point Likert scale from “Strongly Disagree” to “Strongly Agree.”
a. Science and technology are continuously improving our lives
b. Scientists have too much power over nature
c. Science and technology can solve most problems faced by humans
- Describe in one or two sentences the level of knowledge you have on the history and usages of CRISPR-Cas9 gene editing. You can put ‘none’ if you have no background knowledge on CRISPR-Cas9.
Background and Questions on CRISPR-Cas9 Gene Editing
Without changing your answer for the previous question, please read the following description of CRISPR-Cas9 gene editing.
CRISPR-Cas9 is a technology that scientists use to perform genome editing and precisely change the DNA of living cells. While CRISPR-Cas9 has mostly been used for research purposes, it has various other applications. In 2023, the Food and Drug Administration (FDA) approved of the first CRISPR-Cas9 gene therapy to treat patients with Sickle Cell Disease, a serious genetic disorder. Although future possibilities, like altering physical traits such as height, have been imagined, such uses remain speculative and raise ethical questions.
In the following question you will be asked about different scenarios where CRISPR-Cas9 could be used, and you will state your level of agreement for each. The responses options will be strongly agree, agree, neutral, disagree, and strongly disagree.
12. Did you understand the explanation of CRISPR-Cas9 above?
a. I understood it completely
b. I understood it for the most part
c. I did not understand it very well
d. I did not understand it at all
13. Do you believe that CRISPR-Cas9 should be used in these specific instances? Note: This question was asked on a 5 point Likert scale from “Strongly Disagree” to “Strongly Agree.”
a. Preventing life-threatening diseases in children and adults
b. Preventing debilitating diseases in children and adults
c. Physical Enhancement (height, athleticism, etc.)
d. Cognitive Enhancement (intelligence)
e. Personality Enhancement
f. Infertility Treatment
g. Genome research purposes
14. If you had children, would you consider using CRISPR-Cas9 technology on them for any of the purposes mentioned above before their birth?
- Yes
- No
15. Please provide an explanation for your answers to question 13 and 14.
Appendix E
import pandas as pd
import statsmodels.api as sm
from statsmodels.miscmodels.ordinal_model import OrderedModel
from IPython.display import display, HTML
display(HTML(“<style>.container { width:100% !important; }</style>”))
# Load the CSV file
df = pd.read_csv(“Opinions_CRISPR(Sheet1).csv”, encoding=”ISO-8859-1″)
### Convert Grade Level to Numeric
df.columns = df.columns.str.strip()
### Convert Serious Illness Experience to Binary (1 = Yes, 0 = No)
df[“Serious Illness”] = df[“Have you or a family member had a serious illness (e.g. cancer, diabetes, heart disease, etc.)”].apply(
lambda x: 1 if str(x).lower() == “yes” else 0
)
df[“Age”] = pd.to_numeric(df[“Age:”], errors=’coerce’)
### Convert Family in Healthcare to Binary (1 = Yes, 0 = No)
df[“Family in Healthcare”] = df[“Do you have any family members who work in any fields related to biological sciences or healthcare?”].apply(
lambda x: 1 if str(x).lower() == “yes” else 0
)
# Function to process religiosity responses
def process_religiosity(involvement, religion):
try:
# Convert valid numeric responses (1-10)
num_response = float(involvement)
return num_response if 1 <= num_response <= 10 else None
except ValueError:
# If they provided a religion but no response, return None for now
return None if pd.notna(religion) and religion.strip() else 0 # Non-religious get 0
# Apply the function to create Religiosity Level
df[“Religiosity Level”] = df.apply(
lambda row: process_religiosity(row[“If you listed a religion on the previous question, how involved are you in your faith from a scale of 1-10? With 1 being not involved and 10 being very involved.”],
row[“Religious Affiliation:”]),
axis=1
)
# Fill missing religiosity levels with median of those who listed a religion
median_religiosity = df.loc[df[“Religious Affiliation:”].notna(), “Religiosity Level”].median()
df[“Religiosity Level”] = df[“Religiosity Level”].fillna(median_religiosity)
# Define a function to categorize household income
def categorize_income(income):
if pd.isna(income):
return None # Keep NaN values for now
income = str(income).strip().lower()
if “less than” in income or “<$25,000” in income:
return 1
elif “$25,000” in income or “25,000 – $50,000” in income:
return 2
elif “$50,000” in income or “50,000 – $100,000” in income:
return 3
elif “$100,000” in income or “100,000 – $150,000” in income:
return 4
elif “$150,000” in income or “150,000 – $200,000” in income:
return 5
elif “$200,000” in income or “200,000 or above” in income:
return 6
else:
return None # “Prefer not to say” or unclear values
df[“Household Income Level”] = df[“Household Income (do your best to estimate if you don’t know):”].apply(categorize_income)likert_mapping = {
“Strongly Disagree”: 1,
“Disagree”: 2,
“Neutral”: 3,
“Agree”: 4,
“Strongly Agree”: 5
}
science_tech_questions = [
“Please tell me how much you agree or disagree with the following statements on science and technology..Science and technology are continuously improving our lives”,
“Please tell me how much you agree or disagree with the following statements on science and technology..Scientists have too much power over nature”,
“Please tell me how much you agree or disagree with the following statements on science and technology..Science and technology can solve most problems faced by humans”
]
for col in science_tech_questions:
if col in df.columns:
df[col] = df[col].map(likert_mapping)
def categorize_knowledge(value):
try:
num_value = int(float(value))
return num_value if num_value in [0, 1, 2] else 1
except (ValueError, TypeError):
return 1
df[“CRISPR Knowledge Level”] = df[“Describe in one or two sentences the level of knowledge you have on the history and usages of CRISPR-Cas9 gene editing. You can put ‘none’ if you have no background knowledge on CRISPR-Cas9.”].apply(categorize_knowledge)
independent_vars = [
“Age”, # Age as a numeric value (14-18)
“Serious Illness”, # Binary (1 = Yes, 0 = No)
“Family in Healthcare”, # Binary (1 = Yes, 0 = No)
“Religiosity Level”, # Categorical codes
“CRISPR Knowledge Level”, # 0 = No knowledge, 1 = Basic, 2 = Moderate
“Household Income Level”,
# Science & Technology Attitudes (Likert Scale 1-5)
“Please tell me how much you agree or disagree with the following statements on science and technology..Science and technology are continuously improving our lives”,
“Please tell me how much you agree or disagree with the following statements on science and technology..Scientists have too much power over nature”,
“Please tell me how much you agree or disagree with the following statements on science and technology..Science and technology can solve most problems faced by humans”
]
dependent_vars = [
“Do you believe that CRISPR-Cas9 should be used in these specific instances?.Preventing life-threatening diseases in children and adults”,
“Do you believe that CRISPR-Cas9 should be used in these specific instances?.Preventing debilitating diseases in children and adults”,
“Do you believe that CRISPR-Cas9 should be used in these specific instances?.Physical Enhancement (height, athleticism, etc.)”,
“Do you believe that CRISPR-Cas9 should be used in these specific instances?.Cognitive Enhancement (intelligence)”,
“Do you believe that CRISPR-Cas9 should be used in these specific instances?.Personality Enhancement”,
“Do you believe that CRISPR-Cas9 should be used in these specific instances?.Infertility Treatment”,
“Do you believe that CRISPR-Cas9 should be used in these specific instances?.Genome research purposes”
]
for var in dependent_vars:
if var in df.columns:
df[var] = df[var].map(likert_mapping)
# W = dependent_vars position in array
dependent_var = dependent_vars[W]
df = df.dropna(subset=[dependent_var])
df[independent_vars] = df[independent_vars].fillna(df[independent_vars].median())
# Define X (independent) and y (dependent)
X = df[independent_vars]
y = df[dependent_vars[W]]
# Fit the Ordinal Logistic Regression Model
model = OrderedModel(y, X, distr=’logit’)
result = model.fit(method=’bfgs’)
# Print Model Summary
print(result.summary())
Appendix F
Coding frame of open ended question “Please provide an explanation for your answers to questions 13 and 14.”
1 Support mentioning therapy, improving quality of life
2 Support mentioning saving lives
3 Support mentioning parents wanting the best
4 Uncertain, can’t decide
5 Playing God, unnatural
6 Unethical, immoral
7 Only use for diseases
8 Risks, unknown consequences, safety
9 Obtaining an unfair advantage
10 Undermines character, loss of humanity
11 Parents can’t impose on child
12 Not needed, average/normal is OK
References
- A. Philippidis. Casgevy makes history as FDA approves first CRISPR/Cas9 genome edited therapy. Human Gene Therapy 35, 1-4 (2024). [↩]
- P. Liang, Y. Xu, X. Zhang, C. Ding, R. Huang, Z. Zhang, J. Lv, X. Xie, Y. Chen, Y. Li, Y. Sun, Y. Bai, Z. Songyang, W. Ma, C. Zhou, J. Huang. CRISPR/Cas9-mediated gene editing in human tripronuclear zygotes. Protein Cell 6, 363-372 (2015). [↩]
- D. Cyranoski, S. Reardon. Chinese scientists genetically modify human embryos. Nature 22, (2015). [↩]
- I. Karunarathna, T. J. Smith, R. Patel, L. Chen. The ethics of genetic editing: Navigating the future of science. Proc Uva Clinical Research (2024). [↩] [↩]
- T. McCaughey, P. G. Sanfilippo, G. E. C. Gooden, D. M. Budden, L. Fan, E. Fenwick, G. Rees, C. MacGregor, J. E. Craig, T. L. Edwards, K. P. Burdon. A global social media survey of attitudes to human genome editing. Cell Stem Cell 18, 569-572 (2016). [↩] [↩] [↩] [↩] [↩]
- G. Gaskell, I. Bard, A. Allansdottir, R. Vieira da Cunha, P. Eduard, J. Hampel, E. Hildt, C. Hofmaier, N. Kronberger, S. Laursen, A. Meijknecht, S. Nordal, A. Quintanilha, G. Revuelta, N. Saladié, J. Sándor, J. Borlido Santos, S. Seyringer, I. Singh, H. Somsen, W. Toonders, H. Torgersen, V. Torre, M. Varju, H. Zwart. Public views on gene editing and its uses. Nature Biotechnology 35, 1021-1023 (2017). [↩]
- D. R. Forsyth, E. H. O’Boyle, M. A. McDaniel. East meets west: A meta-analytic investigation of cultural variations in idealism and relativism. Journal of Business Ethics 83, 813-833 (2008). [↩]
- C. Critchley, D. Nicol, G. Bruce, J. Walshe, T. Treleaven, B. Tuch. Predicting public attitudes toward gene editing of germlines: The impact of moral and hereditary concern in human and animal applications. Frontiers in Genetics 9, 704 (2019). [↩] [↩] [↩]
- F. Bird. How Do Religions Affect Moralities? A Comparative Analysis. Social Compass 37, 291-314 (1990). [↩]
- D. Scheufele, M. Xenos, E. Howell, K. Rose, D. Brossard, B. Hardy. U.S. attitudes on human genome editing. Science 357, 553-554 (2017). [↩]
- A. Armsby, Y. Bombard, N. Garrison, B. Halpern-Felsher, K. Ormond. Attitudes of Members of Genetics Professional Societies Toward Human Gene Editing. CRISPR J. 2, 331-339 (2019). [↩]
- T. Knapp. Treating Ordinal Scales as Interval Scales: An Attempt To Resolve the Controversy. Nursing Research. 39, 121-123 (1990). [↩]
- J. Durlak. How to Select, Calculate, and Interpret Effect Sizes. Journal of Pediatric Psychology 34, 917-928 (2009). [↩] [↩] [↩]
- T. Sawai, M. Okamura, T. Yaguchi, R. Nakagawa, M. Koike, K. Sakashita, A. Koike, Y. Fujioka, K. Suzuki Human. Human genome editing in clinical applications: Japanese lay and expert attitudes. Frontiers in Genetics 14, 1205092 (2023). [↩] [↩]
- B. Vajen, B. Möller, K. Papsdorf, J. Stenzig, A. Biermann, J. Löhler, H. Scherthan, U. Rüther. Students’ attitudes towards somatic genome editing versus genome editing of the germline using an example of familial leukemia. Journal of Community Genetics 12, 397-406 (2021). [↩]
- B. Varkey. Principles of Clinical Ethics and Their Application to Practice. Medical principles and practice : international journal of the Kuwait University, Health Science Centre 30, 17-28 (2020). [↩] [↩]
- S. Hendriks, N. A. A. Giesbertz, A. L. Bredenoord, S. Repping. Reasons for being in favour of or against genome modification: A survey of the Dutch general public. Human Reproduction Open 2018, hoy008 (2018). [↩] [↩]
- D. So, R. Sladek, Y. Joly. Assessing public opinions on the likelihood and permissibility of gene editing through construal level theory. New Genetics and Society 40, 473-497 (2021). [↩] [↩]
- C. Gormally, A. Heil. A Vision for University Biology Education for Non-science Majors. CBE—Life Sciences Education 21 (2022). [↩]
- N. Allum, P. Sturgis, D. Tabourazi, I. Brunton-Smith. Science knowledge and attitudes across cultures: a meta-analysis. Public Understanding of Science 17, 35-54 (2008). [↩]
- S. Chen, Y. Chu, C. Lin, T. Chiang. Students’ knowledge of, and attitudes towards biotechnology revisited, 1995–2014: Changes in agriculture biotechnology but not in medical biotechnology. Biochemistry and Molecular Biology Education 44, 475-491 (2016). [↩]
- V. Dragoş, V. Mih. Scientific Literacy in School. Procedia – Social and Behavioral Sciences 209, 167-172 (2015). [↩]
- H. Field, P. Powell. Public understanding of science versus public understanding of research. Public Understanding of Science 10, 421-426 (2001). [↩]
- A. Altun, Ö. Kalkan. Cross-national study on students and school factors affecting science literacy. Educational Studies 47, 403-421 (2019). [↩]



{kind=link}