
Abstract
Parkinson’s Disease (PD) is one of the most complex diseases known to humans. PD affects about two percent of the population and is often diagnosed in people above the age of sixty-five. Due to the progressive loss of dopamine cells in the substantia nigra (SN), patients experience involuntary tremors, slowed movement, impaired posture and balance, and rigid muscles. Because there is no known cure for PD, many patients turn to stem cell therapy to slow the disease’s progression and severity. This paper reviews recent studies applying stem cell therapy in the treatment of PD and then summarizes the benefits and challenges associated with this approach while considering potential future treatments. While current stem cell treatments cannot cure PD, stem cell placement in the brain may delay the development of the disease’s most debilitating symptoms by increasing dopamine levels. Stem cell therapy can also be complemented with various medications simultaneously. While scientists have made significant progress in alleviating the most severe symptoms in earlier stages of PD, there is a long road ahead to develop effective treatments to not only slow the disease’s progression but, hopefully, halt the continual deterioration and potentially restore individuals affected by PD to their prior physical health.
Introduction
Parkinson’s Disease (PD) currently affects over 1 million people in the United States alone and it is anticipated that it will affect over 1.2 million individuals by 2030, with about 90,000 newly diagnosed patients each year1. As more research is conducted on PD, scientists have observed the significant impacts the disease has on families and society overall. Results from previous studies indicate that the annual incremental cost of PD ranges from $8,000 to $10,000 per patient2.
The most prominent PD symptoms appear as neurons die in the basal ganglia, a group of structures in the central brain controlling movement. When these neurons die, the brain produces less dopamine, ultimately resulting in motor dysfunctions. These motor dysfunctions can lead to various issues such as stuttering, affecting the individual’s ability to speak3. In addition, other non-motor dysfunctions can occur as well. These include fatigue, depression, anxiety, sleep disturbances, constipation, and sensory issues. Sensory symptoms include pain, numbness, tingling, and burning in the affected limbs. Patients can experience changes in mood, decreased motivation, apathy, bradyphrenia or slowness in thinking, and declining cognition. These non-motor dysfunctions occur in about 40% of patients4.
To diagnose PD, a doctor would review a table like the one shown in Table 1. Because PD is traditionally considered a type of movement disorder, Table 1 depicts the assessments associated with movement discrepancies. To make a conclusive diagnosis, the doctor would expect to observe a patient exhibiting bradykinesia with either tremor or rigidity symptoms combined with none of the exclusion criteria exhibited and at least two supportive criteria observed5.
| 1. Diagnosis of parkinsonism a) Bradykinesia Plus, one of b) Tremor c) Rigidity 2. Exclusion criteria a) Cerebellar abnormalities b) Supranuclear gaze palsy c) Diagnosis of behavioral variant of frontotemporal dementia or primary progressive aphasia within 5 years of disease onset d) Parkinsonian features restricted to the lower limbs for more than 3 years. e) Treatment with a dopamine receptor blocker or dopamine depleting agent consistent with drug-induced parkinsonism f) Absence of a response to high-dose levodopa despite at least moderate disease severity g) Cortical sensory loss, clear limb ideomotor apraxia, or progressive aphasia h) Normal functional imaging of the dopaminergic system (“DAT scan”) i) Diagnosis of alternative condition causing parkinsonism which could be causing the symptoms. 3. Supportive criteria a) Clear beneficial response to dopaminergic therapy b) Presence of levodopa-induced dyskinesia c) Rest tremor of a limb d) The presence of either olfactory loss or cardiac sympathetic denervation on MIBG scintigraphy (although the latter is rarely done in current practice) 4. Red flags a) Rapid progression of gait impairment leading to wheelchair use within 5 years. b) Absence of progression of motor symptoms over 5 years, unless related to treatment. c) Early bulbar dysfunction d) Inspiratory respiratory dysfunction e) Severe autonomic failure within the first 5 years of disease f) Recurrent falls because of impaired balance within 3 years of onset g) Disproportionate anterocollis or contractures within 10 years of disease onset h) Absence of any of the common non-motor features despite 5 years of disease i) Unexplained pyramidal signs j) Bilateral symmetrical parkinsonism | |
| For the diagnosis of clinically established PD | For the diagnosis of clinically probable PD |
| ParkinsonismAbsence of exclusion criteriaAt least 2 supportive criteria | ParkinsonismAbsence of exclusion criteriaBalanced numbers of supportive criteria and red flags |
Many individuals are only diagnosed with PD after motor functions begin to degrade. Other common symptoms include tremors throughout the body, muscle stiffness, movement slowness, and impaired balance. There are many risk factors for PD including age, gender, genetics, and environmental causes, which become increasingly prominent in people over 60 years of age. Men are about one and a half times more likely to develop this disease than women1. Genetic factors also impact PD susceptibility, as people with relatives who have had this disease are two times more likely to develop PD than others6. Approximately 10 to 15% percent of patients with PD exhibit a genetic link. Ashkenazi Jews and North African Arab Imazighens most commonly exhibit at least one of the seven genes linked to PD7. According to the Parkinson’s Foundation, the seven genes include GBA, LRRK2, PRKN, SNCA, PINK1, PARK7 and VPS35, with GBA being the most common PD-related gene, but it is also one of the most difficult to test. GBA mutations are found in approximately five to ten percent of PD patients. The GBA gene produces a protein responsible for removing the protein alpha-synuclein and mutations in GBA cause an accumulation of this protein in the brain of people with PD8. Much research has been done, but the cause of PD remains ambiguous, making it difficult to identify a potential cure6.
A variety of tests can be used to diagnose PD while at the same time eliminating other potential sources of symptoms, such as brain tumors. The most common tests to verify PD are neurological exams and brain scans. Neurological exams test how one’s nervous system works, revealing the source of different symptoms9. One of the most common brain scans done for PD patients is magnetic resonance imaging (MRI) which examines the structure of the brain using a tunnel-shaped piece of equipment that contains magnets and radio waves, generating two or three-dimensional pictures of the brain tissue. Importantly for PD, MRIs can identify dopamine function in the brain and lead to a PD diagnosis if the dopamine levels are extremely low10.
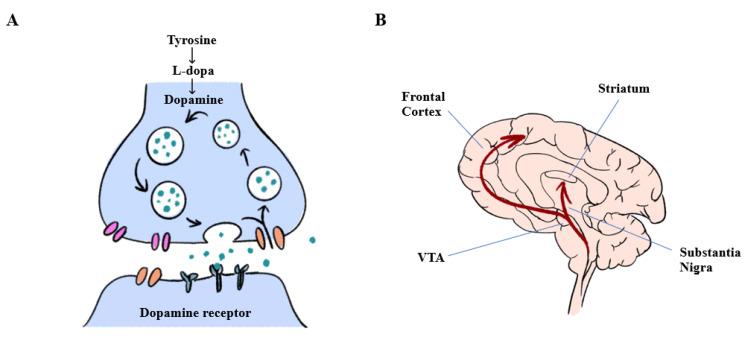
Different treatments can be prescribed to slow the biological progression of PD with the same desired outcome at a molecular level. These treatments target the dopamine-producing cells, to ensure that they continue to synthesize neurotransmitters, passing an electrical signal chemically between one neuron and the next, passing signals to and from the central nervous system11. Figure 1 Image A depicts the dopaminergic neurons with enzymes that biosynthesize dopamine and release it into the mid-brain. Specifically, tyrosine is converted to L-dopa which is then converted to dopamine. Image B of Figure 1 demonstrates the central nervous system pathways of dopamine flow, including VTA or the ventral tegmental area, the frontal cortex, the striatum and the substania nigra12.
According to the American Parkinson Disease Association, deep brain stimulation (DBS) is a further treatment option available to patients suffering from PD which involves implanting electrodes within certain areas of the brain. Specifically, the targeted brain regions are the subthalamic nucleus (STN) or the globus pallidus interna (GPI). Leads are attached to a battery in the chest, like a pacemaker battery. The electrical stimulation provided by the device treats the movement disorders associated with PD13.
Lifestyle changes can drastically reduce the negative impact of PD, particularly aerobic exercise. As Daalen et al. report, higher intensity of exercise (80%–85% of maximum heart rate) is associated with better motor outcomes than a slower pace (60%–65% of maximum heart rate). Exercise may also have various beneficial effects on non-motor functions such as improved cognitive function, sleep, fatigue reduction, and reducing depression. Regular exercise is associated with a reduced risk of developing PD, suggesting that it might even prevent the disease rather than only slowing its progression14. Additionally, physical, occupational, and speech therapy are commonly used to mitigate the effects of PD15.
PD has both rapidly and slowly progressive forms10. Alborghetti and Nicoletti point out that the treatment of either form often involves pharmaceutical options including levodopa preparations and monoamine oxidase-B (MAO-B) inhibitors. Levodopa is used as a direct replacement for the lost dopamine in the brain and MAO-B inhibitors block enzymes that degrade dopamine, thus prolonging the effects of levodopa. A significant downside of PD pharmaceutical treatments is that individuals eventually lose both the long- and short-term response to these types of medications due to ongoing disease-related changes in the brain16.
Due to the limited effectiveness of pharmaceutical and surgical treatments used for PD to date and because a cure remains elusive, researchers have started to consider the potential use of stem cells as a promising treatment option. This paper reviews the current understanding of PD and considers recent studies that have applied developments in stem cell therapy to delay the progression of PD symptoms. Based on the current state of this research, the paper considers what next steps could be taken to further progress the treatment options.
Methodology
This research investigates the current understanding of PD and the use of stem cell therapy through a systemic review of over thirty articles. This qualitative approach using respected databases, such as Google Scholar and the National Institute of Health (NIH) clinical trial database, is intended to provide a general understanding of PD combined with the basics of stem cell therapy. The search words chosen include “Stem Cell Therapy” and “Parkinson’s Disease.” The cited references in each collected study are also gathered and reviewed for deeper understanding. There are limited stem cell human studies conducted to date associated with PD treatments, but all searches were conducted in medical databases to minimize the likelihood of bias or referencing unscientific data. Additionally, due to the limited number of identified stem cell therapy studies associated with PD, all work that was collected is discussed, including one currently underway.
Stem Cell Research Basics
Stem cell therapies have received interest due to their broad potential to treat many conditions. Amongst the many experiments underway for various diseases, some researchers are determining whether stem cells might also mitigate the effects of PD17.
Stem cells are unique from all other human cell types, as they have the potential to turn into specialized tissue types, like bones18. Under the right conditions in a lab or human body, stem cells can divide to form daughter cells. These daughter cells can differentiate into new cell types with specific functions such as blood cells, brain cells, or heart muscle19. Stem cell differentiation involves the changing of a cell to a more specialized cell type, involving a switch from proliferation (increase in cell numbers due to cell division) to specialization. This occurs through the activation of some genes and the repression of others, changing the cell’s function, size, shape, and metabolic activity20. Scientists can utilize stem cells to observe how diseases progress, which may ultimately result in a PD cure.
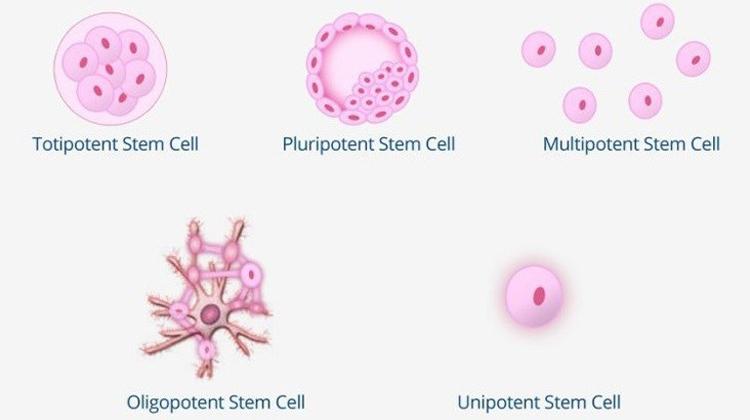
The three main types of stem cells used in scientific research are multipotent, pluripotent, and totipotent (or omnipotent) stem cells. Multipotent stem cells can only grow and specialize into a few specific cell types and are used to create different tissues like fat, bone, and muscle21. Unlike multipotent stem cells, pluripotent cells can grow into all adult cell types. Third, the totipotent stem cell is the most diverse and can differentiate into all types of embryonic and adult cells. With this diversity, totipotent stem cells are applied to many biological research efforts, including regenerative medicine, breeding, and conservation22. There are two other types of stem cells: oligopotent and unipotent. However, they are not used for PD stem cell therapy as they can only differentiate into a closely related cell type (oligopotent) or single cell type (unipotent)23. The five stem cell types are summarized in Figure 2.
Specific to PD research, Omole and Fakoya explain that the two main stem cells used are pluripotent (embryonic) stem cells and induced pluripotent stem cells (IPSCs). These cells are used to replace or repair damaged cells in the brain that can affect motor function. Embryonic stem cells can differentiate into any cell type, which is why they are commonly used in studies to treat diseases like PD25.
However, ethical concerns have arisen regarding embryonic stem cell use. Lo and Parham summarize these issues in Table 2. The public and potential embryonic donors to research hold strong and varied opinions regarding stem cells. For many people, the ethical debate around stem cell research centers on the fact that these cells could have produced a viable human baby. Some people believe that an embryo is a person and therefore has interests and rights that must be respected. From this perspective, some believe all embryonic research is unacceptable, while others only support limited research. Obtaining informed consent for potential future uses of the donated embryo attempts to respect this diversity of personal views26.
| Research Phase | Potential Ethical Concern |
| Donation of biological materials | Informed and voluntary consent |
| Research with hESCs | Destruction of embryos |
| Creation of embryos specifically for research purposes | |
| 1. Payment to oocyte donors | |
| 2. Medical risks of oocyte retrieval | |
| 3. Protecting reproductive interests of women in infertility treatment | |
| Use of stem cell lines derived at another institution | Conflicting legal and ethical standards |
| Stem cell clinical trials | Risks and benefits of experimental intervention |
| Informed consent |
IPSCs are like embryonic stem cells but without any ethical concerns and were first discovered by Professor Shinya Yamanaka in 2006. IPSCs are produced by ectopic expression of a combination of embryonic transcription factors. This new technology is a breakthrough as it allowed for the creation of patient-specific stem cells25.
With the use of IPSCs rather than embryonic cells, many of the ethical debates are eliminated. However, scientists continue to face technical challenges. The main difficulty with using pluripotent or IPSCs is that there is a risk of genetic abnormalities and tumor formations. These stem cells can grow irregularly or specialize in different cell types spontaneously. They may also trigger an immune response in which the recipient’s body attacks the stem cells as foreign invaders, or the stem cells might simply fail to function as expected, with unknown consequences. Researchers continue to study how to avoid these possible complications19.
Potential Use of Mesencephalic fetal cell transplantation
Mesencephalic fetal cell transplantation is a surgical procedure that removes mesencephalic tissue within the midbrain to place it in the patient’s putamen, a brain region correlated to a variety of movement disorders, the most well-known of which is PD27. The procedure’s goal is to implant dopamine-producing cells from the mesencephalic region into the PD-affected putamen areas of the brain to alleviate the severe physical symptoms of this condition. Another common way to treat PD is using human embryonic stem cells derived from dopamine cells for allogenic grafting. Allogenic grafting is a technique where tissue is transferred between two genetically nonidentical members of the same species. This PD transplant process uses stem cells from human embryos to create nerve cells that are then used to treat different conditions including PD28.
As demonstrated by Lui and Cheung, the success of these new techniques is still being evaluated, but there have been early indications they could provide effective long-term treatments. Clinical trials have revealed that the transplantation of fetal midbrain tissues relieved neurological symptoms and restored motor functions in patients with PD. However, several important challenges remain regarding the use of stem cells. Difficult ethical issues exist surrounding the use of human embryonic stem cells, added to the fact this approach produces intense immune responses within the subject’s body. The use of stem cells derived from skin or blood cells does not have the same ethical hurdle, but the risks of tumor development are greater than other stem cell sources. In short, stem cell therapy remains at the early stages of development12. Ultimately, PD is a life-threatening disease affecting millions of people and the risks and benefits of conducting research using stem cell therapy must be weighed against the life-changing and costly social impacts of PD29.
Potential Use of Human Induced Pluripotent Stem Cells (HIPSC) Derived Dopamine Cells for Grafting
As previously mentioned, individuals with PD face numerous physical difficulties resulting from reduced levels of dopamine cells in the brain. Within the brain, the substantia nigra (SN) plays a critical role associated with motor movement and reward functions. Located in the midbrain, the SN can be categorized by regions: the pars compacta (SNpc) containing dopaminergic neurons and the pars reticulata (SNpr) with inhibitor gamma-aminobutyric acid-containing (or GABAergic) neurons30.
Projections that extend from the SN to the putamen have been shown to cause the observed motor deficits in PD. These projections leave the SN via the medial forebrain bundle and form synapses, particularly within the putamen. The SN is believed to provide the primary input into the basal ganglia, which are interconnected subcortical nuclei that are critical in functions including emotions, reward functions, voluntary movement, and cognitive planning and learning. When these subcortical nuclei are damaged, a multitude of neurological conditions can result, including PD30.
Creating specific dopamine-producing brain cells from pluripotent cells is important in treating PD. One specific neuron type strongly linked to PD is called the rA9 SNpc dopamine neuron found in the midbrain. This neuron subtype controls motor function and is one current research focus in stem cell research. Finding ways to generate these neurons in the brains of PD patients might lead to better treatment options31.
A study done by Ni and Ernst demonstrated that SNpc cells have higher metabolic activity than other cells. As a result, SNpc cells go through many more biochemical reactions and energy exposure, leading to genetic or metabolic challenges. This study concluded that many factors contribute to the vulnerability of the changing stem cells. The SNpc cell may require more energy to sustain its functions, resulting in this vulnerability. While the SNpc cell is in a heightened energy state, specific factors like metabolic regulation and insulin maintenance are affected. The metabolic function programming may be the cause for the heightened state31.
Scientists are investigating whether the use of HIPSCs might address these challenges. HIPSCs have been used to treat a variety of diseases. This cell type is commonly used to treat PD as it provides accurate modeling, unlike other types of stem cells. In a study published by Stoddard-Bennett and Pera, the loss of dopamine cells due to PD resulted in patient weakness as current therapies cannot reverse the significant cell loss. However, HIPSCs offer a solution, as patient-specific HIPSCs can be transplanted into everyone. This is a promising answer to the quest to find a PD cure and mitigate PD’s detrimental effects32.
A study by Schweitzer et al. was conducted using stem cell therapy on a 69-year-old PD patient. This patient suffered from a loss of dopamine cells in the brain which led the researchers to create stem cells that were implanted into the PD-affected SN area of the brain. A few months after this surgery, the patient’s dopamine levels were higher, and dopamine was being generated by these stem cells. This research showed the significant positive impact stem cell therapy can have on PD and the overall importance of understanding this disease33.
Further evidence is emerging that suggests HIPSCs for clinical use are increasingly viable. Sundberg et al conducted an animal study to demonstrate that the use of improved surface protein-based cell sorting techniques to differentiate and identify specialized dopamine-producing neurons from pluripotent stem cells improves the outcomes of cell transplantation. Their results from a non-human primate (macaque monkey) induced pluripotent stem cells (iPSC)-derived neural cell graft 1 year after the procedure did not detect any abnormal overgrowth of the graft in the monkey’s striatum34. Similarly, a study by Tao et al. also reported that transplanting iPSCs into the brains of rhesus monkeys exhibiting PD improved neuron growth and motor function over two years. Behavioral improvement in mood was also noted35.
In a study conducted by Thanaskody et al., the importance of HIPSCs was demonstrated by exhibiting the positive and negative consequences of this stem cell. The primary advantage of using HIPSCs is associated with fewer ethical issues prohibiting researchers from acquiring and using stem cells36. A continuing technical issue faced by researchers is the concern with immune rejection from a patient’s body. This can be countered by using mesenchymal stem cells to suppress the likelihood of immune rejection. Mesenchymal stem cells control HIPSC rejection by mediating immune tolerance through activated lymphocytes37. A further challenge with using this type of stem cell is that there is a chance of initiating tumorigenesis. Prior studies, such as the one described by Tao et al., have shown that pluripotent stem cell-derived neural cells entail risks of tumor formation upon transplantation if the cell population contains undifferentiated cells or non-neural cells35.
This promising preliminary clinical research appears to have encouraged further efforts to assess iPSC transplantation results in human PD subjects. As recently reported by the NIH; a study has been initiated in China to use laboratory-grade HIPSCs for Parkinson’s disease treatment. The study plans to recruit three eligible PD subjects and prepare dopaminergic neural precursor cells from autologous iPSCs in advance. After surgery, the patients will be observed for six months, during which the safety of this treatment will be assessed. If the test results within the first six months post-surgery indicate both safety and some level of efficacy, the trial will continue for an additional six months. The study is expected to conclude sometime in 202538. As of the writing this paper, no similar studies have been reported on the NIH clinical trial tracking website nor in other literature search reviews. What remains clear is that the use of HIPSCs as a PD treatment option has benefits and disadvantages.
Although promising, the limited number of human clinical trials creates unanswered questions and highlights some challenges. Harary et al. state that the long-term efficacy and side effects of this type of stem cell therapy are not yet fully understood and it is unclear which surgical delivery technique is optimal. Finally, the approach’s scalability to iPSC-derived cell production at a commercial level might be challenging39. Although clinical research has shown that stem cell therapy is beneficial in mitigating the effects of PD by using HIPSCs in a few studies36, more systematic studies are needed to make reliable inferences.
Conclusions
PD is a deadly disease affecting millions of people in the United States alone. Although significant time and money have been dedicated to researching this disease, a cure has not been identified. Stem cell therapy does have some ethical considerations and potential disadvantages, particularly when stem cells are gathered from embryonic sources that otherwise may have resulted in a human life. Fortunately, the use of HIPSCs might bypass many of these concerns if it can be demonstrated that these cells can consistently and predictably be grown into desired cell types, such as dopamine-producing neurons without the risk of patient rejection or uncontrolled cell growth. This therapy should continue to be explored with ethical considerations in mind and used in combination with other pharmaceutical and physical therapy options. Current research and clinical methodologies suggest significant treatment benefits are possible and with time may offer the promise of a long-term cure for this deadly disease. The first human stem cell clinical trials are just underway to evaluate the potential treatment for PD, with results expected in 2025. This will provide scientists with additional data to assess true potential and viability of stem cells as a long-term treatment.
Acknowledgments
Thank you for the guidance of my mentor Mr. Cyrus Ayubcha from Harvard Medical School, and Empowerly coaches Ms. Rose Wang and Mr. Ayush Dhall in this research paper’s development.
- “Statistics: Get Informed about Parkinson’s Disease with These Key Numbers.” Parkinson’s Foundation, www.parkinson.org/understanding-parkinsons/statistics. Accessed 6 Sept. 2023. [↩] [↩]
- Albarmawi, Husam Ph.D., et al. “The Economic Burden of Parkinson Disease among Medicare Beneficiaries.” Journal of Managed Care & Specialty Pharmacy, 28 Apr. 2022, www.jmcp.org/doi/full/10.18553/jmcp.2022.28.4.405. Accessed 6 Sept. 2023. [↩]
- Alm, Per A. “The Dopamine System and Automatization of Movement Sequences: A Review with Relevance for Speech and Stuttering.” Frontiers in Human Neuroscience, 2 Dec. 2021, www.frontiersin.org/articles/10.3389/fnhum.2021.661880/full. Accessed 6 Sept. 2023. [↩]
- Fahn, Stanley. “Description of Parkinson’s Disease as a Clinical Syndrome.” Annals of the New York Academy of Sciences, vol. 991, no. June 2003, 2003, p. 7, https://apps.dtic.mil/sti/pdfs/ADA419154.pdf#page=27. Accessed 6 Sept. 2023. [↩]
- Greenland, Julia C., and Roger A. Barker. “The Differential Diagnosis of Parkinson’s Disease.” National Library of Medicine: National Center for Biotechnology Information, 21 Dec. 2018, www.ncbi.nlm.nih.gov/books/NBK536715/table/. Accessed 7 Sept. 2023. [↩] [↩]
- “Parkinson’s Disease Risk Factors and Causes.” John’s Hopkins Medicine, www.hopkinsmedicine.org/health/conditions-and-diseases/parkinsons-disease/parkinsons-disease-risk-factors-and-causes. Accessed 6 Sept. 2023. [↩] [↩]
- “Genetics & Parkinson’s.” Parkinson’s Foundation, www.parkinson.org/understanding-parkinsons/causes/genetics. Accessed 6 Sept. 2023. [↩]
- “Genetics Behind Parkinson’s.” Parkinson’s Foundation, www.parkinson.org/advancing-research/our-research/pdgeneration/genetics-behind-pd. Accessed 10 Sept 2023. [↩]
- “About Brain Tumors: Diagnosis.” American Brain Tumor Association, www.abta.org/about-brain-tumors/brain-tumor-diagnosis/. Accessed 6 Sept. 2023. [↩]
- “How Parkinson’s Disease Is Diagnosed.” American Parkinson Disease Association, www.apdaparkinson.org/what-is-parkinsons/diagnosing/#:~:text=Imaging%20studies%20to%20evaluate%20Parkinson%E2%80%99s%20disease%20and%20Parkinsonian,to%20detect%20the%20dopamine%20function%20in%20the%20brain. Accessed 6 Sept. 2023. [↩] [↩]
- Olguín, Hugo J., et al. “The Role of Dopamine and Its Dysfunction as a Consequence of Oxidative Stress.” Oxidative Medicine and Cellular Longevity, vol. 2016, 2016, pp. 1-13, https://doi.org/10.1155/2016/9730467. Accessed 6 Sept. 2023. [↩]
- Lui, Zhaohui, and Hoi-Hung Cheung. “Stem Cell-Based Therapies for Parkinson Disease.” National Library of Medicine: National Center for Biotechnology Information, 21 Nov. 2020, www.ncbi.nlm.nih.gov/pmc/articles/PMC7663462/. Accessed 6 Sept. 2023. [↩] [↩] [↩]
- Armstrong, Melissa J. MD, MSc, and Michael S. Okun MD. “Diagnosis and Treatment of Parkinson Disease A Review.” JAMA, vol. 323, no. 6, 2020, p. 548, https://doi.org/10.1001/jama.2019.22360. Accessed 6 Sept. 2023. [↩]
- Daalen, Jules M. J. MD, et al. “Lifestyle Interventions for the Prevention of Parkinson Disease.” Neurology, vol. 99, 2022, p. S46, https://doi.org/10.1212/WNL.0000000000200787. Accessed 6 Sept. 2023. [↩]
- “What Is Parkinson’s Disease?” American Parkinson Disease Association, www.apdaparkinson.org/what-is-parkinsons/. Accessed 6 Sept. 2023. [↩]
- Alborghetti, Marika, and Ferdinando Nicoletti. “Different Generations of Type-B Monoamine Oxidase Inhibitors in Parkinson’s Disease: From Bench to Bedside.” PubMed Central, 17 Sept. 2019, www.ncbi.nlm.nih.gov/pmc/articles/PMC7052841/#:~:text=Three%20 inhibitors%20of%20type%2DB,%2Dterm%20L%2DDOPA%20treatment. Accessed 6 Sept. 2023. [↩]
- Hoang, Duc M., et. al. “Stem Cell-Based Therapy for Human Diseases.” Signal Transduction and Targeted Therapy, 6 Aug 2022, https://doi.org/10.1038/s41392-022-01134-4. Accessed 12 Feb 2024. [↩]
- “Stem Cells.” MedlinePlus Trusted Health Information for You, 29 Mar. 2016, medlineplus.gov/stemcells.html. Accessed 6 Sept. 2023. [↩]
- “Stem Cells: What They Are and What They Do.” Mayo Clinic, 19 Mar. 2022, www.mayoclinic.org/tests-procedures/bone-marrow-transplant/in-depth/stem-cells/art-20048117. Accessed 6 Sept. 2023. [↩] [↩]
- Clause, Kelly C., et al. “Directed Stem Cell Differentiation: The Role of Physical Forces.” National Library of Medicine: National Center for Biotechnology Information, 23 Feb. 2012, www.ncbi.nlm.nih.gov/pmc/articles/PMC3285265/. Accessed 6 Sept. 2023. [↩]
- Abinaya, Ravichandran V., and Pragasam Viswanathan. “Biotechnology-based Therapeutics.” ScienceDirect, 29 Jan. 2021, www.sciencedirect.com/science/article/abs/pii/ B9780128219720000198. Accessed 6 Sept. 2023. [↩]
- Tabansky, Inna, and Joel N. H. Stern. “Basics of Stem Cell Biology as Applied to the Brain.” National Library of Medicine, National Center for Biotechnology Information, 27 Jul. 2016, www.ncbi.nlm.nih.gov/books/NBK435799/. Accessed 6 Sept. 2023. [↩]
- Hildreth, Cade. “Do You Know The 5 Types of Stem Cells?” Bioinformant, 14 Feb. 2023, bioinformant.com/types-of-stem-cells/. Accessed 7 Sept. 2023. [↩]
- ((Hildreth, Cade. “Do You Know The 5 Types of Stem Cells?” Bioinformant, 14 Feb. 2023, bioinformant.com/types-of-stem-cells/. Accessed 7 Sept. 2023. [↩]
- Omole, Adekunle E., and Adegbenro O. J. Fakoya. “Ten Years of Progress and Promise of Induced Pluripotent Stem Cells: Historical Origins, Characteristics, Mechanisms, Limitations, and Potential Applications.” National Library of Medicine: National Center for Biotechnology Information, 11 May 2018, pubmed.ncbi.nlm.nih.gov/29770269/. Accessed 6 Sept. 2023. [↩] [↩]
- Lo, Bernard, and Lindsay Parham. “Ethical Issues in Stem Cell Research.” Endocrine Reviews, 1 May 2009, https://doi.org/10.1210/er.2008-0031. Accessed 12 Feb 2024 [↩] [↩]
- Ghandili, Mehrnoosh, and Sunil Munakomi. “Neuroanatomy, Putamen.” National Library of Medicine: National Center for Biotechnology Information, 30 Jan. 2023, www.ncbi.nlm.nih.gov/books/NBK542170/. Accessed 6 Sept. 2023. [↩]
- “Cell Transplantation (Mesencephalic, Adrenal-Brain and Fetal Xenograft) – CAM 075.” Medical Policies, 12 Mar. 2014, www.southcarolinablues.com/web/public/brands/medicalpolicy/ external-policies/cell-transplantation-mesencephalic-adrenal-brain-and-fetal-xenograft/. Accessed 6 Sept. 2023. [↩]
- Cona, Louis A. MD. “Stem Cells: Parkinson’s Treatment Breakthrough (2023).” DVCSTEM, 12 May 2023, www.dvcstem.com/post/stem-cell-therapy-for-parkinsons. Accessed 6 Sept. 2023. [↩]
- Sonne, James, et al. “Neuroanatomy, Substantia Nigra.” National Library of Medicine: National Center for Biotechnology Information, 24 Oct. 2022, www.ncbi.nlm.nih.gov/books/NBK536995/. Accessed 7 Sept. 2023. [↩] [↩]
- Ni, Anjie, and Carl Ernst. “Evidence That Substantia Nigra Pars Compacta Dopaminergic Neurons Are Selectively Vulnerable to Oxidative Stress Because They Are Highly Metabolically Active.” National Library of Medicine: National Center for Biotechnology Information, 4 Mar. 2022, www.ncbi.nlm.nih.gov/pmc/articles/PMC8931026/. Accessed 6 Sept. 2023. [↩] [↩]
- Stoddard-Bennett, Theo, and Renee R. Pera. “Treatment of Parkinson’s Disease through Personalized Medicine and Induced Pluripotent Stem Cells.” National Library of Medicine: National Center for Biotechnology Information, 7 Jan. 2019, www.ncbi.nlm.nih.gov/pmc/articles/PMC6357081/. Accessed 6 Sept. 2023. [↩]
- Schweitzer, Jeffrey S. M.D., Ph.D., et al. “Personalized IPSC-Derived Dopamine Progenitor Cells for Parkinson’s Disease.” National Library of Medicine: National Center for Biotechnology Information, 14 May 2020, www.ncbi.nlm.nih.gov/pmc/articles/PMC7288982/. Accessed 6 Sept. 2023. [↩]
- Sundberg, Maria, et al. “Improved Cell Therapy Protocols for Parkinson’s Disease Based on Differentiation Efficiency and Safety of HESC-, HiPSC-, and Non-Human Primate IPSC-Derived Dopaminergic Neurons.” StemCells, 10 May 2013, stemcellsjournals.onlinelibrary.wiley.com/doi/pdf/10.1002/stem.1415. Accessed 6 Sept. 2023. [↩]
- Tao, Yunlong, et al. “Autologous Transplant Therapy Alleviates Motor and Depressive Behaviors in Parkinsonian Monkeys.” Nature Medicine, Apr. 2021, www.nature.com/articles/s41591-021-01257-1.epdf?sharing_token=R1_Sqghus1bnQ-7uI1amUdRgN0jAjWel9jnR3ZoTv0O8Oqzek3iJNvWeLxN5-aruw3YwylBBf98qUX-xszFcV3HVzhe2p8QaSDRwWyyumNGaG0OHqtHfkR5EgCcdo0ADAH_H6mLTpZA1GpMNo5pR82xOObXBs6VHXdo6DbBNBv-tcgw8xGVsa5u5g3LwQQ5JG24w 2eCuNdHZ2OSQZY_OoI0C3TJXPByRjrTvJIJEAx8%3D&tracking_referrer=www.the-scientist.com. Accessed 5 Sept. 2023. [↩] [↩]
- Thanaskody, Kalaiselvaan, et al. “MSCs Vs. IPSCs: Potential in Therapeutic Applications.” National Library of Medicine: National Center for Biotechnology Information, 2 Nov. 2022, www.ncbi.nlm.nih.gov/pmc/articles/PMC9666898/. Accessed 6 Sept. 2023. [↩] [↩]
- Yoshida, Shohei, et al. 12 Mar. 2020, pubmed.ncbi.nlm.nih.gov/32165680/. Accessed 7 Sept. 2023. [↩]
- “A Clinical Trial of Parkinson’s Disease Treatment by hiPSCs Derived Dopaminergic Neural Precursor Cells (hiPSC-DAP).” Shanghai East Hospital, 24 Nov. 2023, www.clinicaltrials.gov/study/NCT06145711?cond=NCT06145711&rank=1. Accessed 12 Feb 2024. [↩]
- Harary, Paul M., et al. “Cell Replacement Therapy for Brain Repair: Recent Progress and Remaining Challenges for Treating Parkinson’s Disease and Cortical Injury.” Brain Sci. 29 Nov. 2023. https://doi.org/10.3390/brainsci13121654. Accessed 12 Feb 2024. [↩]



{kind=link}