
Smaritha Tadiboyina1, Makaila Furderer1
1 Lumiere Premium Research and Publication Program
Abstract
Progressive supranuclear Palsy (PSP) is a neurodegenerative disease that is caused by abnormal tau accumulation mainly in the frontal lobe and the midbrain. Patients with PSP experience symptoms such as loss of muscle function, cognitive, and behavioral problems. Parkinson’s disease (PD) is a neurodegenerative disease that leads to loss of motor movements, tremors, bradykinesia, and changes in posture and gait. The pathological hallmark of PD is the formation of Lewy Bodies. Using a literature review approach, this paper investigates the differences between PSP and Parkinson’s disease, and how Parkinson’s treatments might be used as interventions for PSP. The results show that PSP and Parkinson’s both have similar symptoms, such as loss of motor movements and cell loss in the substantia nigra. A key difference is that Parkinson’s disease is characterized by the formation of Lewy bodies, while PSP is characterized by the accumulation of tau in the frontal lobe. Current/previously tested treatments for PSP include deep-brain stimulation and tau vaccines. The most promising treatments seem to be vaccines that prevent tau buildup and immunotherapies.
Keywords: PD, PSP, Therapeutic approaches, neurodegenerative disease, motor movements, tauopathy
Introduction
Background for PSP
Progressive Supranuclear Palsy (PSP) is a neurodegenerative disease, often referred to as atypical Parkinsonian syndrome, also known as Parkinson-plus disorder.1 PSP was first described in 1964 by three scientists: John Steele, J Clifford Richardson, and Jerzy Olzewski.2 PSP is characterized by the loss of muscle function.3,4 PSP features abnormal tau accumulation, predominantly in the frontal lobe and midbrain. The disease is usually diagnosed through performing physical and neurological tests on the patient. A definite diagnosis requires a neuropathological examination.5Currently, there is a strong predominance of males over females, with a ratio of 1.6:1.6. The average age of diagnosis is 65, and patients are usually expected to live 6 to 9 years after the disease emerges.7 Patients with PSP-Richardson’s Syndrome (PSP-RS) were found to have shorter lifespans than patients with non-PSP-RS in a small sample study of 32 patients.7 Patients with PSP experience symptoms such as loss of muscle function, and cognitive and behavioral problems. PSP is also associated with a dopamine energy system impairment in the nigrostriatal, mesolimbic, and mesocortical pathways.8
Currently, there are no definitive treatment options for PSP that lead to recovery, but there are treatment options to manage symptoms, such as physical therapy. Early signs of the disease include difficulty walking and running, and frequent falls. As the disease progresses, supranuclear ophthalmoplegia, slurring of speech, difficulty swallowing, and frontal cognitive difficulties become present.9 Dopaminergic cell loss in the substantia nigra is also present.8 There is not a single definitive test to definitively diagnose PSP at this time. Physicians will usually conduct physical and neurological exams to rule out other disorders. While there is no cure for PSP, there are some treatment options available to help patients combat symptoms, but these treatments don’t eliminate them. For example, physical therapy and Levodopa are common treatments. Physical therapy enables significant improvement in clinical rating scales, and Levodopa often shows transient benefits.10 The main gap present in medical treatment is the lack of long-term treatments and treatments that prevent the progression of the disease.
As of now, researchers know that PSP is caused by the aggregation of the tau protein in the brain, but the cause of this abnormal protein accumulation is unknown. Scientists speculate that environmental factors such as exposure to toxins, unknown chemicals in food, or genetic mutations are possible sources. Tau is normally used to stabilize microtubules, structures that support the cell’s morphology. PSP features hyperphosphorylation of tau, thus promoting the clumping in neurons, astrocytes, and oligodendrocytes, leading to neurofibrillary tangles. These tangles disrupt neuronal function and eventually lead to neuronal death in key areas of the brain – such as the midbrain, subthalamic nucleus, and pons – that affect vision, balance, and motor movements.10
Pathology
PSP is a tauopathy, a specific type of neurodegenerative disease that involves the tau protein. Specifically, PSP affects 4R-tau, a type of tau with 4 microtubule-binding repeats. In PSP, the 4R-tau becomes abnormally folded and sticky, clumping together in brain cells. This leads to neurofibrillary tangles and tufted astrocytes, leading to a loss of motor functions3. This affects the regions of the brain called the subthalamic nucleus, pallidum, striatum, red nucleus, substantia nigra, pontine tegmentum, oculomotor nucleus, medulla, and dentate nucleus, many of which are part of a region called the basal ganglia, which is primarily involved in motor control and movement-related functions.11 Currently, MRIs showcase atrophy and a signal increase in the midbrain, degeneration of the red nucleus, atrophy of the quadrigeminal plate, and enlargement of the aqueduct and third ventricles. A key indicator is the “hummingbird sign,” where the midbrain atrophy is in the shape of a hummingbird.12
Early signs of PSP consist of difficulty walking and moving, as well as sudden falls. Using data drawn from the Adelphi PSP Disease Specific Programme (large multinational surveys) conducted in 2018 in the USA and EU5, researchers found that most patients usually wait 5.2 months before visiting a healthcare professional, and wait around 9.2 months until they are definitively diagnosed with PSP.10 Supranuclear ophthalmoplegia is usually a distinctive sign of PSP, and bradykinesia and the slurring of speech are common symptoms later on in the disease.3 Frontal lobe dysfunction is also a common sign of PSP.
Introduction to Parkinson’s Disease
Parkinson’s disease (PD) is a neurodegenerative disorder that leads to difficulty with motor movements, characterised by bradykinesia, resting tremor, and changes in posture and gait. The pathological hallmark of PD is the formation of Lewy bodies (abnormal clumps of protein in the brain) and Lewy neurites, with cell loss in the substantia nigra. Due to PD’s overlap with other neurodegenerative diseases, such as PSP, early diagnosis is difficult. Age is the most common risk factor associated with PD, and men are more likely to get PD than women, with a ratio of 3:2. There is also a genetic component associated with PD, with 90 genetic risk loci currently identified.13 PD and PSP have many similar symptoms, such as slowness in gait movement, with PSP also being referred to as atypical Parkinsonian syndrome.
Similar to PSP, PD is another disorder in which dopaminergic signaling is altered due to degeneration of the substantia nigra.14 The symptoms include difficulty with motor movements, characterised by bradykinesia, rest tremor, and changes in posture and gait. Due to Parkinson’s overlap with other neurodegenerative diseases such as PSP, early diagnosis is difficult.15 New studies have shown that MRPI and MRPI 2.0 have become more reliable sources for differentiating PSP and PD, fulfilling “level 2” biomarker criteria, meaning that they can support clinical diagnosis.16
Researchers compared Advanced Parkinson’s Disease (APD), a stage in PD that affects patients’ daily lives to the point that they start needing additional care, and PSP. They found that PSP patients were older at the age of diagnosis, typically around 69, while APD patients were 61 on average. The researchers also found that PSP progressed faster, with patients having PSP for around 2.3 years at the time of the study, while APD patients had the disease for 11.8 years, while experiencing similar symptoms. PSP patients need day/nighttime care around 200-300 days of the year, while APD patients need it only around 6-7 days a year.17 This study suggests that PSP is a much more severe disorder compared to PD, suggesting that Parkinson’s treatments may not be as beneficial to PSP patients.
Additionally, in another study that compared non-motor symptoms in PSP and Parkinson’s disease, patients underwent a series of neurological assessments. These tests showed that patients with PSP had greater cognitive impairment than patients with PD. Patients with PSP were also shown to have a worse quality of life, higher apathy levels, and higher levels of depression and anxiety.18 In this literature review, the differences and similarities between PSP and PD will be investigated to evaluate whether PD treatments may be effective for PSP. PD treatments have the potential to benefit PSP patients due to the similar causes and symptomology of the disorders, such as the degeneration of dopamine signaling and loss of motor movements.
Methods
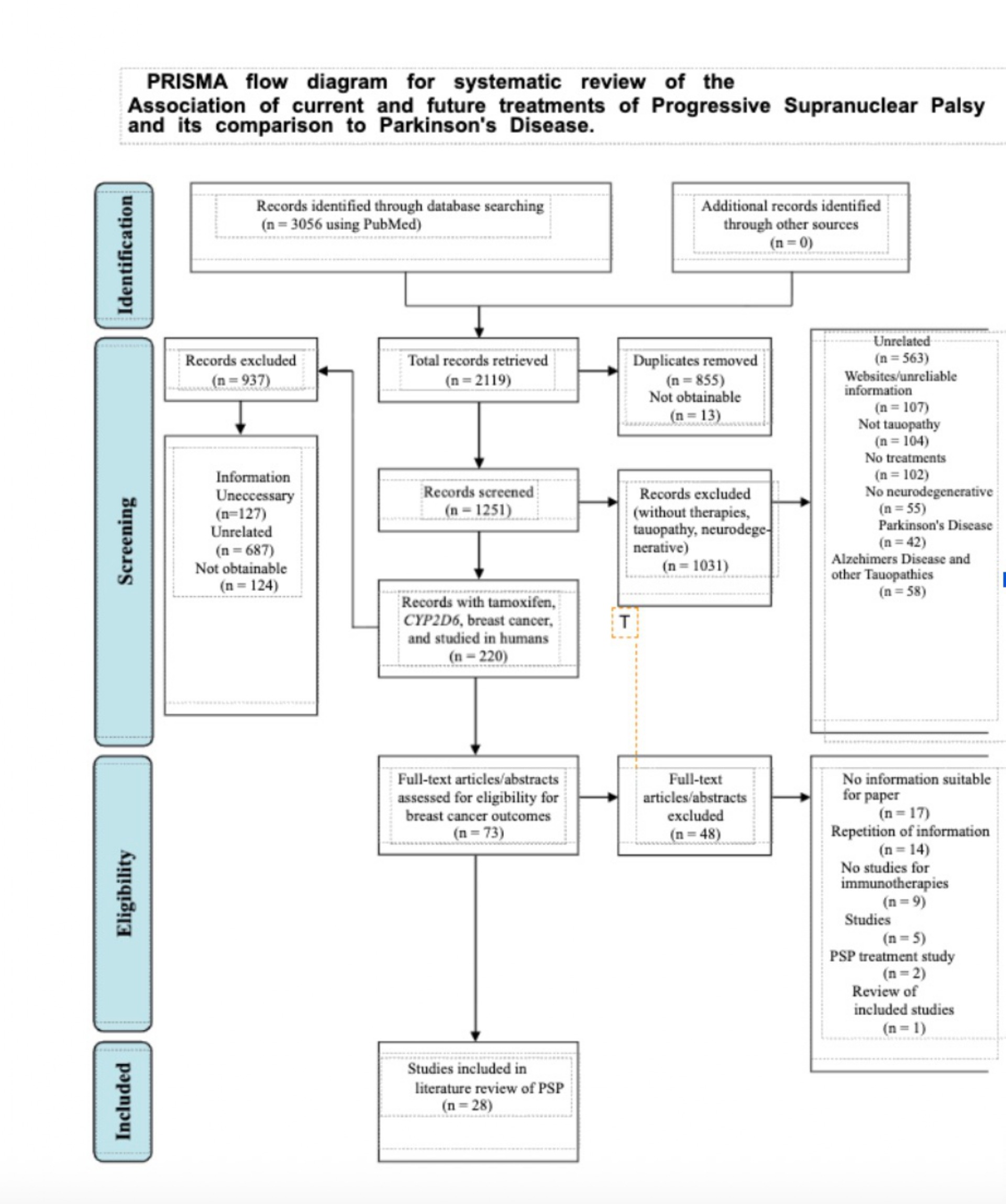
Peer-reviewed publications were searched for using PubMed (https://pubmed.ncbi.nlm.nih.gov/) and Google Scholar (https://scholar.google.com/). Searches were conducted between the years 2015 and 2025 to ensure the incorporated literature was current. Searches were conducted using the keywords “Progressive Supranuclear Palsy,” “Parkinson’s Disease Treatments,” “PSP therapies,” and “PSP treatments.” Inclusion criteria were peer-reviewed research articles, experiments testing different treatment methods, English-language articles, and articles published between 2000 and 2025. After an initial search was conducted, 638 articles were found and screened. For each included study, data were extracted about experimental procedures, experimental data, discussion about implications of findings, and discussion about potential future treatments.
Results
Current Treatments for PSP
Basic Treatments
Currently, PSP patients are usually treated with LEDD (levodopa combined with dopa decarboxylase) to release dopamine into the brain.3 This treatment is often considered transient and doesn’t provide long-term effectiveness for patients. Patients have started to utilize physical therapy to learn how to fall safely and improve balance to minimize the risks of potential injury. Patients can also take antidepressants to help with the depression associated with PSP. Additionally, they can utilize a speech and language therapist to help with vocal muscles and with dysphasia in the earlier stages. As the dysphasia continues to worsen as the disease progresses, patients may be referred to a dietitian to ensure that they still have a balanced diet that accommodates their swallowing problems. A feeding tube is also a common tool to ensure that patients are getting proper nutrients. Hospice is also a commonly used tool near the end of a patient’s life.3
How Basic Treatments are Deficient
Most treatments are utilized to ease the patient’s pain but don’t truly cure, reverse, or halt the progression of the disease. To make treatments more effective, they would have to eliminate the underlying source of PSP – the abnormal tau protein. While clinical trials are ongoing, there hasn’t been an effective drug that can eliminate the tau that has accumulated in the brain. In addition, there is no confirmed diagnosis for PSP either. Being able to detect PSP/pinpoint its cause could make finding treatment easier and maximize a patient’s chance of survival. Analyzing causes that make a patient more susceptible to the disease could help develop a vaccine, preventing people from getting it. For example, the spreading of neurofibrillary tangles from one brain region to the next is thought to be due to extracellular transsynaptic transmission of misfolded tau protein. This led researchers to speculate that antibodies against tau could potentially prevent the transfer of misfolded tau.19
Standard of Care
The standard of care for PSP patients is complicated, as there aren’t many treatments that have proven to be effective. The standard of care focuses on improving the quality of life for patients rather than treating the disease itself. Currently, drugs like levodopa are used at doses around 900-1200 mg for a month to help with bradykinesia. To manage gait dysfunction, drugs such as Amantadine are recommended to help with dyskinesia.20 It’s given at around 50-100mg daily and titrated at intervals of at least 2 weeks. Coenzyme Q-10 is another drug that is prescribed to patients but has a moderate benefit on average. It’s given in doses of 100mg and supplements cell protection. In addition to pharmacological therapy, physical therapy and aerobic exercise are recommended.
PSP-Parkinonsian (PSP-P): A cross between PSP and PD
PSP-P is a subtype of PSP and is associated with a less severe course of the disease. The clinical manifestation of PSP-P presents significant overlap with PD, but requires different neuropathic examinations.16 PSP-P also presents a symptom called Freezing of Swallowing (FOS). In a study, three patients diagnosed with PSP-P presented symptoms of freezing episodes of the tongue and palate during chewing and swallowing. All three patients showed symptoms of irregular trembling of the tongue base and soft palate. Levodopa was offered at doses up to 850 mg and did not help or worsen the symptoms.21 New biomarkers have emerged to distinguish PSP-P from PD. Patients with PSP-P often have lower levels of cerebrospinal fluid (CSF) phosphorylated tau (p-tau) and higher CSF and plasma Nfl levels compared to patients with Parkinson’s. Patients also exhibit higher concentrations of CSF noradrenaline (NE).22 In a study comparing Multiple System Atrophy – Parkinsonian (MSA-P) and PSP-P, it was found that Magnetic Resonance Parkinsonian Index 2.0 (MRPI 2.0) seems to be feasible in differentiating PSP-P from PD.18 In a study that compared clinical and MRI presentations among 150 PSP patients, it was found that midbrain-based MRI parameters showed a significant decrease in midbrain size in PSP-P compared to PD.23 Another method of differentiating occurs in the ratio of the midbrain area and pontine area (m_a/p_a) ratio. This ratio is found to be smaller in PSP patients compared to non-PSP patients. In a study examining white matter content in PSP-P patients, ten native Serbian-speaking PSP patients underwent a series of clinical, neuropsychological, and MRI scans. Healthy controls were also evaluated to provide a baseline. The results showed that PSP-P patients did not have a significant difference in cerebellum white matter.23
Parkinson’s Treatments and How They Can Be Applied to PSP
Currently, many scientists are testing the benefits of physical therapy in Parkinson’s patients. A study investigated the benefits of physiotherapy and the use of treadmills in improving gait quality. The study found that both interventions increased gait velocity and gait parameters such as stride length, swing time, etc. This study excluded patients with atypical/secondary Parkinsonian syndrome (such as PSP), but could potentially benefit PSP patients in gait movement. Utilizing physical therapy in the early stages of PSP could benefit patients’ gait movements in the long run and reduce the loss of muscle function.24 Herbal products have also shown potential benefits for Parkinson’s patients. Peganum harmala has reduced oxidative stress in rats with induced PD and has been shown to improve muscle stiffness and prevent degeneration of dopaminergic neurons. Chunghyuldan (CHD) is a Chinese herbal medicine that has also showcased potential benefits for Parkinson’s. In mice testing, CHD reduced symptoms such as bradykinesia and lowered dopaminergic neuronal damage. CHD also prevents Reactive Oxygen Species (ROS) -mediated mitochondrial dysfunction, which is thought to be one of the major pathological indicators for Parkinson’s Disease, preventing energy production in the body. CHD and Peganum harmala both could potentially benefit PSP patients as well by helping with motor movements and dopamine. Although ROS is not a major cause/reason for PSP, CHD could potentially benefit energy production in PSP patients as well, if the disorder is diagnosed early on.19 No studies have been done with herbal products on humans with PD, which is a possible limitation of this study. A potential treatment for targeting Lewy Bodies is NLPR3 inhibitors, which have been shown to block inflammasome activity in preclinical PD models, and daily dosing of MCC950 was shown to protect nigrostriatal dopaminergic degeneration.23 These treatments have potential benefits in treating PSP patients, as PSP also has inflammasome activity and dopaminergic degeneration.23 Additionally, there are minimal studies that examine PD treatments on PSP, and the literature that exists often tests the same treatments (LEDD and physical therapy). An additional treatment that has been tested on tauopathies is mitochondrial bioenergetics. Gln supplementation has been shown to increase oxidative phosphorylation (OXPHOS) , thereby promoting autophagosome biogenesis in tauopathy neurons.25 In vitro and in vivo findings have also demonstrated autophagy enhancement upon stimulation of OXPHOS in normal neurons, showing potential for tauopathy neurons as well.25 This study was conducted on Alzheimer’s patients, but the study talked about Gln supplementation in relation to tauopathies as a whole.
Discussion
In conclusion, PSP is a neurodegenerative disease that is characterized by the aggregation of tau in the frontal lobe and the midbrain. PSP causes the loss of gait movement and voluntary eye movement. Currently, there are no effective treatments for PSP. Physical and speech therapy have proven to show some benefit in helping patients with their gait and slurring of speech. Additionally, patients are usually also given levodopa, which releases dopamine into the brain. This treatment is usually common among Parkinson’s disease patients, but is given to PSP patients as well, and has shown little to no effect in most patients. Currently, the most promising future treatments look like preventing an anti-tau vaccine, to prevent the tau from aggregating, or a treatment that targets the aggregated tau and gets rid of them. Additionally, autophagy also seems to be a promising way to prevent clumping of tau.
Currently tested methods
Currently, there haven’t been any effective treatments for managing/treating PSP. Neurologists have tried unilateral/bilateral pedunculopontine nucleus deep brain stimulation, but have shown little to no effect.3 Deep-brain stimulation is a procedure where electrodes are implanted into the brain to deliver electrical impulses to regulate brain activities. Another treatment that has been tested was microtubule stabilizers, to compensate for the dysfunction that is caused by the loss of tau protein. Davenuntine is a microtubule stabilizer that showcased potential benefits in animals with tauopathy diseases, but showed no efficacy on humans when tested.
Tau-Therapy and mAB trials
Immunotherapeutic approaches have been tried as well, with passive immunization of anti-tau antibodies showcasing some potential. One study injected mice with full-length human-tau protein and injected them with three anti-tau antibodies. One antibody (HJ8.5) showed a reduction in phosphorylated tau and an improvement in associative learning, highlighting potential in humans as well.26 Two tau-therapy vaccines entered human clinical trials, but neither has proven any efficacy, and were thus discontinued. Lastly, another tau-therapy tried to assemble and disassemble aggregated tau proteins. Methylene blue derivatives entered Phase III clinical trials but ended up being negative.27 Researchers also tried to prevent phosphate groups from being added to tau, utilizing a drug called GSK-3, but that also proved to be negative.28 A humanized tau antibody (ABBV-8E12) was developed in a phase 1 clinical trial and was found to have an acceptable safety profile. AbbVie enrolled patients in phase 2 clinical trials in 2017, and no update was found on the efficacy of the vaccine.19
Challenges
Challenges in finding treatments for PSP occur due to a lack of understanding of the disease. The cause of the disease is unknown, and misdiagnosis is common due to the disease’s similarities with Parkinson’s. Additionally, most treatments focus on managing symptoms, rather than disease-modifying treatments. Most drugs that prove to be effective on animals with tauopathic conditions fail when they are tested on humans. In addition, PSP is presented in numerous different ways, with PSP having numerous different subtypes, making it difficult to develop a treatment. There is not much research on PSP yet, but one avenue of research could be to delve into Parkinson’s disease treatments and assess whether they would be applicable to PSP. While this could be a good starting point, there would need to be further research done to ensure the treatment’s effectiveness on PSP. Vaccines may be unable to reach the brain due to the blood-brain barrier. If a vaccine were to be developed, it would need to be developed in a way that the antibodies would be able to pass through the blood-brain barrier. Treatments are also costly, and not many people can afford them, leading to affordable care being an issue as well.
Limitations
PSP is an extremely rare disease, limiting the amount of research that has been done on it. This led to the majority of the research reviewing similar treatments. Many peer-reviewed studies repeat the same information due to the lack of knowledge about the disease. Additionally, many of the clinical studies were blocked by paywalls, making them inaccessible. Clinical studies have often been done on mice, with many clinical studies progressing to being tested on humans. None of the studies used in this review tested on cells. There were also no current vaccine trials found, only ones that were done in the past.
References
- Agarwal, Shashank, and Rebecca Gilbert. “Progressive Supranuclear Palsy.” PubMed, StatPearls Publishing, 2020, www.ncbi.nlf5cm.nih.gov/books/NBK526098/. [↩]
- Dickson, D.W., Rademakers, R. and Hutton, M.L. (2007), Progressive Supranuclear Palsy: Pathology and Genetics. Brain Pathology, 17: 74-82. https://doi.org/10.1111/j.1750-3639.2007.00054.x [↩]
- Agarwal, Shashank, and Rebecca Gilbert. “Progressive Supranuclear Palsy.” PubMed, StatPearls Publishing, 2020, www.ncbi.nlf5cm.nih.gov/books/NBK526098/. [↩] [↩] [↩] [↩] [↩] [↩]
- Höglinger, G. U., Respondek, G., Stamelou, M., Kurz, C., Josephs, K. A., Lang, A. E., Mollenhauer, B., Müller, U., Nilsson, C., Whitwell, J. L., Arzberger, T., Englund, E., Gelpi, E., Giese, A., Irwin, D. J., Meissner, W. G., Pantelyat, A., Rajput, A., van Swieten, J. C., Troakes, C., … Movement Disorder Society-endorsed PSP Study Group (2017). Clinical diagnosis of progressive supranuclear palsy: The movement disorder society criteria. Movement disorders : official journal of the Movement Disorder Society, 32(6), 853–864. https://doi.org/10.1002/mds.26987 [↩]
- Testa, D., Monza, D., Ferrarini, M., Soliveri, P., Girotti, F., & Filippini, G. (2001). Comparison of natural histories of progressive supranuclear palsy and multiple system atrophy. Neurological sciences : official journal of the Italian Neurological Society and of the Italian Society of Clinical Neurophysiology, 22(3), 247–251. https://doi.org/10.1007/s100720100021 [↩]
- Mahale, R. R., Krishnan, S., Divya, K. P., Jisha, V. T., & Kishore, A. (2022). Gender differences in progressive supranuclear palsy. Acta neurologica Belgica, 122(2), 357–362. https://doi.org/10.1007/s13760-021-01599-0 [↩]
- Marchand, F., Blaise, A. S., Defebvre, L., Cailliau, E., Bombois, S., Devos, D., & Moreau, C. (2024). Clinical prognostic factors in progressive supranuclear palsy: Implications for clinical trials. Journal of Parkinson’s disease, 14(8), 1652–1658. https://doi.org/10.1177/1877718X241291996a [↩] [↩]
- Gómez-Virgilio, L., Gutiérrez-Malacara, A. I., Rivera-Osorio,are difficulty J., Del, M., Padilla-Mendoza, J. R., Gómez-Ramírez, D. E., & Del, M. (2024). Progressive supranuclear palsy: an updated approach on diagnosis, treatment, risk factors and outlook in Mexico. Gaceta Médica de México, 160(4). https://doi.org/10.24875/gmm.m24000930 [↩] [↩]
- Boxer, A. L., Yu, J.-T., Golbe, L. I., Litvan, I., Lang, A. E., & Höglinger, G. U. (2017). Advances in progressive supranuclear palsy: new diagnostic criteria, biomarkers, and therapeutic approaches. The Lancet Neurology, 16(7), 552–563. https://doi.org/10.1016/s1474-4422(17)30157-6 [↩]
- Vaswani, P. A., & Olsen, A. L. (2020). Immunotherapy in progressive supranuclear palsy. Current Opinion in Neurology, 33(4), 527–533. https://doi.org/10.1097/wco.0000000000000836 [↩] [↩] [↩]
- Morgan, John C., et al. “Disease Course and Treatment Patterns in Progressive Supranuclear Palsy: A Real-World Study.” Journal of the Neurological Sciences, vol. 421, Feb. 2021, p. 117293, https://doi.org/10.1016/j.jns.2020.117293. Accessed 10 Nov. 2022. [↩]
- Dickson, D. W., Ahmed, Z., Algom, A. A., Tsuboi, Y., & Josephs, K. A. (2010). Neuropathology of variants of progressive supranuclear palsy. Current opinion in neurology, 23(4), 394–400. https://doi.org/10.1097/WCO.0b013e32833be924 [↩]
- Coughlin, D. G., & Litvan, I. (2020). Progressive supranuclear palsy: Advances in diagnosis and management. Parkinsonism & related disorders, 73, 105–116. https://doi.org/10.1016/j.parkreldis.2020.04.014 [↩]
- Tolosa, Eduardo, et al. “Challenges in the Diagnosis of Parkinson’s Disease.” The Lancet Neurology, vol. 20, no. 5, 1 May 2021, pp. 385–397. [↩]
- Radhakrishnan, Divya M; Goyal, Vinay. Parkinson’s disease: A review. Neurology India 66(Suppl 1):p S26-S35, Mar–Apr 2018. | DOI: 10.4103/0028-3886.226451 [↩]
- Quattrone, A., Morelli, M., Bianco, M. G., Buonocore, J., Sarica, A., Caligiuri, M. E., Aracri, F., Calomino, C., De Maria, M., Vaccaro, M. G., Gramigna, V., Augimeri, A., Vescio, B., & Quattrone, A. (2022). Magnetic Resonance Planimetry in the Differential Diagnosis between Parkinson’s Disease and Progressive Supranuclear Palsy. Brain sciences, 12(7), 949. https://doi.org/10.3390/brainsci12070949 [↩] [↩]
- Chen, Ying, et al. “Comparative Study of Nonmotor Symptoms in Progressive Supranuclear Palsy and Parkinson’s Disease.” BMC Neurology, vol. 25, no. 1, 19 May 2025, https://doi.org/10.1186/s12883-025-04225-1. Accessed 28 Aug. 2025. [↩]
- Alster, P., Madetko-Alster, N., Migda, B., Nieciecki, M., Koziorowski, D., & Królicki, L. (2022). The Assessment of Subregions in the Frontal Lobe May Be Feasible in the Differential Diagnosis of Progressive Supranuclear Palsy-Parkinsonism Predominant (PSP-P) and Multiple System Atrophy (MSA). Diagnostics (Basel, Switzerland), 12(10), 2421. https://doi.org/10.3390/diagnostics12102421 [↩] [↩]
- Amro, M. S., et al. “The Potential Role of Herbal Products in the Treatment of Parkinson’s Disease.” La Clinica Terapeutica, vol. 169, no. 1, 2018, pp. e23–e33, pubmed.ncbi.nlm.nih.gov/29446788/, https://doi.org/10.7417/T.2018.2050. [↩] [↩] [↩]
- West, T., Hu, Y., Verghese, P. B., Bateman, R. J., Braunstein, J. B., Fogelman, I., Budur, K., Florian, H., Mendonca, N., & Holtzman, D. M. (2017). Preclinical and Clinical Development of ABBV-8E12, a Humanized Anti-Tau Antibody, for Treatment of Alzheimer’s Disease and Other Tauopathies. The Journal of Prevention of Alzheimer’s Disease, 4(4), 236–241. https://doi.org/10.14283/jpad.2017.36 [↩]
- Maetzler, W., Rattay, T. W., Hobert, M. A., Synofzik, M., Bader, A., Berg, D., Schaeffer, E., Rommel, N., Devos, D., Bloem, B. R., & Bender, B. (2016). Freezing of Swallowing. Movement disorders clinical practice, 3(5), 490–493. https://doi.org/10.1002/mdc3.12314 [↩]
- Cerroni R, Liguori C, Stefani A, Conti M, Garasto E, Pierantozzi M, Mercuri NB, Bernardini S, Fucci G and Massoud R (2020) Increased Noradrenaline as an Additional Cerebrospinal Fluid Biomarker in PSP-Like Parkinsonism. Front. Aging Neurosci. 12:126. doi: 10.3389/fnagi.2020.00126 [↩]
- Wen, Y., Yang, Q., Jiao, B., Zhang, W., Lin, J., Zhu, Y., Xu, Q., Zhou, H., Weng, L., Liao, X., Zhou, Y., Wang, J., Guo, J., Yan, X., Jiang, H., Tang, B., & Shen, L. (2023). Clinical features of progressive supranuclear palsy. Frontiers in aging neuroscience, 15, 1229491. https://doi.org/10.3389/fnagi.2023.1229491 [↩] [↩] [↩] [↩]
- Gaßner, Heiko, et al. “Treadmill Training and Physiotherapy Similarly Improve Dual Task Gait Performance: A Randomized-Controlled Trial in Parkinson’s Disease.” Journal of Neural Transmission, vol. 129, no. 9, 13 June 2022, pp. 1189–1200, www.ncbi.nlm.nih.gov/pmc/articles/PMC9463305/, https://doi.org/10.1007/s00702-022-02514-4. Accessed 6 Jan. 2023. [↩]
- Jia, N., Ganesan, D., Guan, H., Jeong, Y. Y., Han, S., Rajapaksha, G., Nissenbaum, M., Kusnecov, A. W., & Cai, Q. (2025). Mitochondrial bioenergetics stimulates autophagy for pathological MAPT/Tau clearance in tauopathy neurons. Autophagy, 21(1), 54–79. https://doi.org/10.1080/15548627.2024.2392408 [↩] [↩]
- Fabbri, Margherita, et al. “Multidisciplinary Care Use in Neurodegenerative Complex Diseases: The Example of Progressive Supranuclear Palsy and Advanced Parkinson’s Disease in Real-Life.” Parkinsonism & Related Disorders, vol. 125, 28 June 2024, pp. 107047–107047, https://doi.org/10.1016/j.parkreldis.2024.107047. Accessed 17 Oct. 2024. [↩]
- Boxer, Adam, et al. “New Diagnostics and Therapeutics for Progressive Supranuclear Palsy HHS Public Access.” Lancet Neurol, vol. 16, no. 7, 2017, pp. 552–563, https://doi.org/10.1016/S1474-4422(17)30157-6. Accessed 9 Sept. 2025. [↩]
- Alster P, Madetko N, Koziorowski D and Friedman A (2020) Progressive Supranuclear Palsy—Parkinsonism Predominant (PSP-P)—A Clinical Challenge at the Boundaries of PSP and Parkinson’s Disease (PD). Front. Neurol. 11:180. doi: 10.3389/fneur.2020.00180 [↩]



{kind=link}