
Abstract
This paper reviews literature surrounding sex differences in depression, anxiety, and post-traumatic stress disorder (PTSD). Women are two to three times more likely to develop psychiatric disorders such as these, but more sex difference research is needed to further understand how these disorders appear differently in women and men. Biological factors, such as brain activation, can contribute to the development of psychiatric disorders, along with other factors, such as pregnancy and postpartum. Sex differences can be studied in those aspects, along with animal and human models, which provide insight into behavioral patterns and common symptoms. The pharmacological and non-pharmacological treatment of these disorders can also shed light on sex differences, as reactions to treatment can best indicate future directions. With the introduction of the policy that designates sex as a biological variable (SABV), research into sex differences has grown, and it is important for that field to continue expanding for future diagnoses and treatments to better represent both sexes.
Introduction
This review primarily discusses sex differences in three psychiatric disorders, while also including discussions regarding biological sex differences. Depression, anxiety, and posttraumatic stress disorder (PTSD) are the three psychiatric disorders that are focused on in this review. Animal and human models of these psychiatric disorders are discussed in order to present sex differences in diagnosis and treatment. Additionally, the biological sex differences discussed include neuroanatomical and hormonal differences. This review focuses on sex differences within the context of the historical lack of research using females to study psychiatric disorders.
Historically, the inclusion of female animals in preclinical research has been lacking. Due to this, much of the foundation for current therapeutics is based solely on male physiology and neurobiology. Almost 80% of articles from the early 20th century did not include a specific sex for animal trials, and after 1969, there was a substantial increase in trials that were specified as being only male1. In 1993, the NIH passed the Revitalization Act, which mandated that female participants should be included in clinical trials, but the mandate did not state that female animals had to be included and tested in preclinical trials or earlier research stages2. Therefore, a policy requiring sex as a biological variable (SABV) in NIH-funded research on vertebrate animals and humans went into effect in 20163, a pivotal moment in history for more gender inclusive research. Measures such as these have allowed for greater inclusion within research and enabled a greater opportunity for understanding sex differences.
Methods
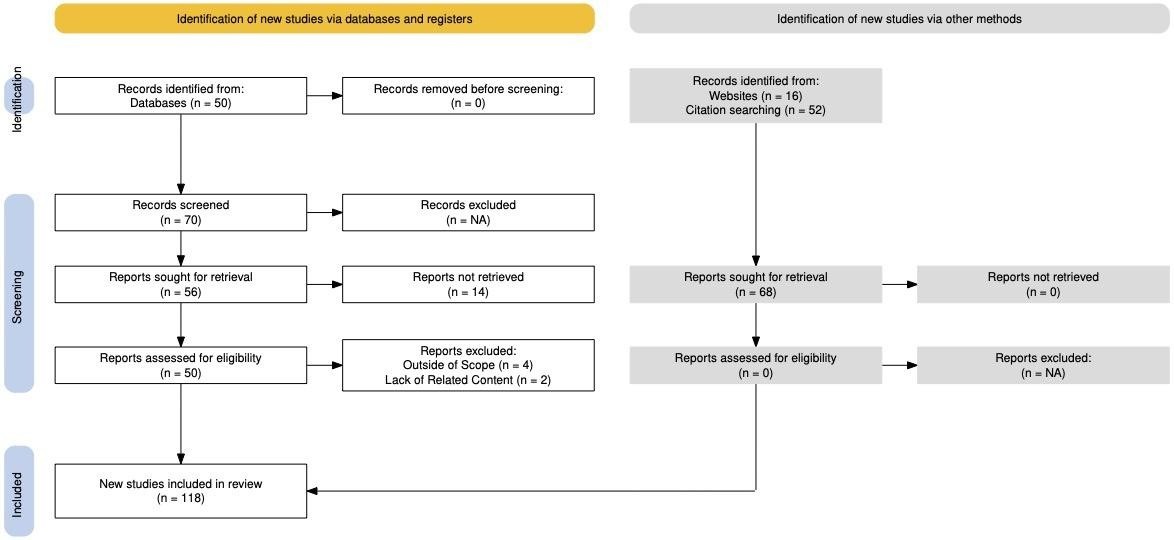
The scientific papers in this literature review were found using PubMed and Google Scholar. Research papers were included if they discussed sex differences in depression, anxiety, and/or PTSD and had a section on sex differences in a topic associated with these disorders. Papers were excluded if they discussed disorders that were not relevant to this review or did not discuss sex differences in findings. Limitations of this review include the inability to reference papers that I could not access, such as those not on the PubMed Central database, or ones without full access on another database’s website. The main keywords included sex differences, psychiatric disorders, depression, anxiety, PTSD, animal models, treatment. Papers from 2010-2025 were searched due to specificity of the criteria. Older papers were cited due to their contributions to the understanding of the topics presented in the review.
Biological Sex Differences
Neuroanatomical Sex Differences: The Biology Behind Psychiatric Disorders
There are many differences in the neuroanatomy of women and men, which originate before birth and continue to change through puberty. During prenatal and postnatal development, the hypothalamic-pituitary-gonadal axis produces high levels of gonadal steroids, such as testosterone and estradiol. This promotes the organization of the central nervous system for sexual differentiation, otherwise known as the “masculinization” or “feminization” of the brain4 (Table 1).Testosterone for males and estrogen and progesterone for females then begin to circulate during puberty and continue to impact brain development. This can be supported by a positive correlation between testosterone and white matter5 and a positive correlation between estradiol, parahippocampus, and uncus gray matter6(Table 1). These observations demonstrate how hormones enable the neuroanatomy of women and men to develop and mature in distinct ways.
| Female Features | Male Features |
| Feminization of the brain due to production of high levels of gonadal steroids in prenatal and postnatal development4 | Masculization of the brain due to production of high levels of gonadal steroids in prenatal and postnatal development4 |
| Positive correlation between estradiol, parahippocampus, and uncus gray matter6 | Positive correlation between testosterone and white matter5 |
| Greater between-hemispheric connectivity7 | Greater within-hemispheric connectivity7 |
| Greater activation in the left amygdala during the exhibition of negative emotions8 | Greater activation in the left amygdala during the exhibition of positive emotions8 |
This table summarizes the neuroanatomical differences that are discussed in the Biological Sex Differences section. As such, the following differing features that distinguish female and male brains are represented: feminization and masculinization of the brain, gray and white matter in the brain quantity, hemispheric connectivity, and amygdala activation.
In the brain, the cerebrum can be divided into the frontal, parietal, temporal and occipital lobes. It is also split into two hemispheres, the right and the left hemispheres, which each contain portions of these lobes. Neurons form the connections between regions of the brain, since these lobes are divided and need to be able to communicate in close and far distances. However, research has discovered that this may occur differently in women and men.
A study found that men tend to have greater within-hemispheric connectivity, while women tend to have greater between-hemispheric connectivity, showing how communication pathways differ in the brains of women and men7(Table 1). Consequently, the left and right hemispheres in the male brain tend to have improved communications within each individual hemisphere, while the left and right hemispheres in the female brain tend to have improved communications between the two hemispheres. The same study concluded that greater-within hemisphere connectivity creates an efficient system for coordinated action, and enhanced motor abilities have allowed more aggressive tendencies to develop in men. The study then determined that greater between-hemispheric connectivity creates improved integration of analytical and sequential reasoning with spatial and intuitive information processing in women; this has allowed for women to have enhanced memory and social cognition skills.
This difference in brain connectivity could provide an explanation for the greater prevalence of psychiatric disorders in women. The effect of an enhanced memory on women is reflected in higher rates of lifetime prevalence of PTSD and the effect of enhanced social cognition on women is reflected in a type of anxiety disorder, Social Anxiety Disorder. This lack of memory enhancement in men could potentially explain the difference in symptoms of depression, anxiety, and PTSD, which will be discussed in greater detail later in this review. However, these differences can be influenced by brain size, as another study found a lack of sex differences in connectivity with brains of a similar size9. If this is the case, then differences in connectivity could occur regardless of sex and may necessitate research on how brain volume relates to functionality.
There are also sex differences in brain activation. In a study by Stevens & Hamann, it was found there to be greater activation in the left amygdala for women who exhibited negative emotions, compared to men8(Table 1). Women tend to respond more strongly to negative emotional stimuli, which can be connected to a greater risk for the development of depression and anxiety10. Additionally, the same study found that men who exhibited positive emotions had greater activation in the left amygdala compared to women(Table 1). The amygdala is a part of the neural network that controls emotional regulation and can also be activated during exposure to stressors for women11. While sex differences in the activation of the amygdala have not been fully explored, they may be linked to the prevalence of psychiatric disorders in women. In general, sex differences in connectivity and activation of the brain are significant in understanding the differing neurobiology of women and men.
Testosterone & Estrogen: The Hormones That Could Affect Psychiatric Disorders
In the research of psychiatric disorders, the hormone testosterone has been found to have a variety of effects in women and men. Testosterone is a hormone that can exist in concentrations ten times higher in men than women, and starts circulating in young boys during puberty, but can affect men throughout the rest of their lives12. It was found that men with decreased levels of testosterone due to the condition hypogonadism more often developed an anxiety disorder or major depressive disorder than those with normal levels of testosterone13. Additionally, men with prostate cancer who were treated with a drug that lowers testosterone levels had an increased chance of developing an anxiety disorder or major depressive disorder14. As such, it is evident that decreased levels of testosterone may be connected to adverse psychiatric effects. Therefore, testosterone treatment has been administered to hypogonadal men to combat these effects, and in the majority of situations, it has improved symptoms of depression and anxiety12.
Although testosterone exists in lower concentrations in women, a study found that women with a depressive or anxiety disorder contained less salivary testosterone than women without a psychiatric disorder15. When testosterone treatment, which increases testosterone levels, was given to depressed women, it lessened feelings of depression16. As such, testosterone levels may factor into the prevalence of psychiatric disorders in women. Another study found that testosterone levels may affect amygdala reactivity in women17, which would be significant since the amygdala controls emotional regulation. The same study found that lower levels of testosterone were associated with decreased amygdala reactivity, and when testosterone was administered to increase levels, amygdala reactivity also increased. While this study increased testosterone in middle-aged women, whose testosterone levels were lower simply due to aging, it is worthy to note the impact that the hormone had on the brain. However, it has been found that the administration of testosterone in women may instead increase feelings of depression and therefore, consideration of all potential effects, wanted or unwanted, must be taken into account18. While more research is needed to investigate the potential relationship between testosterone levels and psychiatric disorders, individuals should not overlook that the hormone may affect research studies in human models.
The hormone estrogen has also been found to affect systems in the brain in both women and men. Men have higher and more stable estrogen levels in the brain than women, due to androgens being aromatized to estradiol19. Aromatization is a process where the enzyme aromatase converts androgens into estradiol, a form of estrogen. Since androgens, hormones that are readily available in males, are continuously being converted to estradiol, it allows for levels to remain at a more constant rate in men. However in women, levels of estrogen can fluctuate, impacting mood and emotion, particularly in a way that may increase symptoms of anxiety and depression20. Therefore, this may contribute to the varying development of psychiatric disorders in women versus men.
Estrogen receptors can be found in a variety of places in the brain, such as the hippocampus, hypothalamus, and amygdala21. In a study of Major Depressive Disorder (MDD), it was found that G protein-coupled estrogen receptor 1 (GPER1) levels were higher in those with MDD than those without22. Additionally, the same study found there was a positive correlation with high GPER1 levels and depression scores. This study looked at GPER1 levels in women and men, showing how estrogen receptors can affect psychiatric disorders regardless of sex. The influence of estrogen and estrogen receptors is certainly significant, and further research will need to be conducted to fully understand their role in psychiatric disorders.
Research Concerns Regarding Testosterone and Estrogen
There are a variety of concerns in research about the effect of hormones, especially estrogen, on research in animal and human models. Hormone fluctuations during the menstrual cycle in women (estrous cycle in rodents), such as estrogen, have been known to discourage the use of human and rodent females in research23. Female rodents have a four-day ovarian cycle, which could necessitate researchers to take vaginal swabs in studies that may have hormonal effects24. However, the effect of testosterone could be just as consequential as the hormones typically avoided in females. It was found that male rats housed together tend to establish a dominance hierarchy, which has the potential to activate circulating testosterone in both the dominant males and non-dominant males23. The circulation of testosterone could skew data results just as much as a hormone like estrogen would, therefore, causing the favor of male animals to be unwarranted.
The need for more studies including female animals was recognized with the implementation of the sex as a biological variable (SABV) policy in 201625. The policy necessitates the use of both female and male animals, and if researchers choose not to include both sexes, an acknowledgement of the reason why is required. The policy has certainly made an impact, with Gereau et al. finding sex differences in neurotransmitter release that modulate alcohol consumption26. The policy’s future life and success remain a mystery, though, with current legislation terminating activities aimed at advancing diversity, equity, and inclusion27. As the potential for a future without this policy approaches, it is important for sex differences to be acknowledged when necessary, as the current research has made a significant impact.
A Unique Biological Difference: The Effect of Pregnancy on Psychiatric Disorders
Pregnancy and postpartum are instances unique to women where there is an increased risk for a psychiatric disorder, such as depression or anxiety. Approximately 10-14% of pregnant women in the general obstetric population meet the criteria for major depressive disorder28. Additionally, approximately 1 in 5 women will develop an anxiety disorder during pregnancy29. It has also been found that women who have a previous psychiatric disorder and then become pregnant tend to have a higher allostatic load and higher rates of depression and anxiety than pregnant women who were not previously diagnosed with a psychiatric disorder30. Pregnancy is difficult to study in human and animal models, but it is evident that pregnancy can affect the mental state of a significant portion of women. Treatment to help relieve women of symptoms of depression and anxiety during pregnancy is even more difficult to study, and there have been a variety of findings on the effects.
Several researchers have studied the effects of pharmaceuticals for psychiatric disorders on pregnant women. For example, the use of benzodiazepines and selective serotonin reuptake inhibitors (SSRIs) has been found to have adverse behavioral effects in infants one month postpartum31. Benzodiazepines are commonly used to treat anxiety disorders, and SSRIs are commonly used to treat depressive disorders. However, there is a risk for development of preeclampsia with pharmaceutical interventions during pregnancy. Preeclampsia is a condition that includes hypertension that develops at less than 20 weeks of gestation and either proteinuria, adverse conditions, or severe complications32. Bernard et al. found that women who used antidepressant and anxiolytic medications during the 16 weeks of pregnancy increased their risk of developing preeclampsia by 3 times, compared to women who did not use those medications33. Additionally, women increased their risk of preeclampsia if they continued to use the medications after 16 weeks. Most pharmacological treatments for anxiety and depression come with complications. However, non-pharmacological treatments, such as mindfulness-based programs, can be beneficial to pregnant and postpartum women34. These programs should be accessible and recommended, especially due to the risks with medications, until further research can be done to create safer drugs for pregnant and postpartum women with psychiatric disorders.
Sex Differences in Common Psychiatric Disorders
Depression
Depression is a common psychiatric disorder that has a variety of symptoms and subtypes under its general categorization. Symptoms can include depressed mood, loss of interest in activities, weight changes, fatigue, and suicidal ideation35. The most common subtype of depression is major depressive disorder (MDD), with other subtypes including seasonal depression, bipolar disorder, and persistent depressive disorder36. Depression is an example of a psychiatric disorder more common in females than in males, with data from a recent survey showing that the overall depression prevalence was 16% for females and 10.1% for males37. Additionally, the survey showed that depression prevalence for every age group was higher in females than males. With these data, it is important to discuss observed sex differences in animal models and human studies to improve the diagnosis and treatment of depression.
In the study of depression, animal models have revealed differences in the behaviors of females and males, with certain tests being used on rodents to investigate this. The forced swim test (FST) had been commonly used to measure depressive behaviors, such as learned helplessness and despair, by placing a rodent in a container of water where it cannot escape. In a study that researched literature that conducted the FST, whether female or male rodents tended to exhibit more depressive behaviors varied, with some stating that females exhibited more depressive behaviors, others stating that males exhibited more depressive behaviors, and some with no differences between the behaviors of males and females38 (Table 2). The inconclusiveness of these findings represents the range of sex-based research in the study of depression. A study has hypothesized many reasons for this, including the use of genetically different strains of mice, the inability to replicate certain symptoms in animals, slight differences in lab protocol during behavioral tests, and the effect of the estrous cycle39. Additionally, the validity of the FST has been questioned, and ethical concerns have been raised about its methods40. Therefore, as the study of depression with animal models continues, it is important to acknowledge the factors which may be contributing to sex differences or a lack of sex differences, especially when making comparisons with humans.
| Behavioral Test(s) | Female Behavior | Male Behavior | Interpretation |
| Depression: Forced Swim | ↑ floating and immobility | ↑ floating and immobility | Both female and male rodents have shown depressive behaviors38 |
| Anxiety: Elevated Plus-Maze (EPM) Open Field (OF) | ↑ time in open arms (EPM) ↑ time in center (OF) | ↓ time in open arms (EPM) ↓ time in center (OF) | Male rodents tend to show more anxiety-like behavior41 |
| PTSD: Cat Predator Stress | ↑ vulnerability to cat odor | ↓ vulnerability to cat odor | Female rodents tend to show more vulnerability to predatory cues42 |
This table summarizes the sex differences in animal models that are discussed in the Sex Differences in Common Psychiatric Disorders section. Female and male rodents both express depressive behaviors. Male rodents tend to show more anxiety-like behavior while female rodents tend to be more vulnerable to PTSD tests.
Sex differences in the study of depression have also been investigated via human models. It has been reported that women experience depressive symptoms, such as depressed mood, weight change, and sleep disturbance, at a higher frequency and intensity than men43.This is supported by the fact that women are more likely to develop an eating disorder and have an increased risk for depression, while men are more likely to abuse anabolic steroids and have an increased risk for depression44 (Table 3). In another example, those who have experienced childhood sexual abuse (before 18 years of age) can be linked to depression in adolescence and adulthood45. In a survey from the United States, this occurs in as many as 14.5% of women and 7.2% of men46, showing the sex discrepancy for those who are most likely to experience this social situation and potentially develop depression. These examples have allowed researchers to further understand the sex differences in depression and how certain situations may have led to the existence of these differences. Additionally, these situations give an insight into how depression should be diagnosed, with consideration of environments that have impacted women and men in various ways.
| Psychiatric Disorder | Female Tendencies | Male Tendencies | Interpretation |
| Depression | ↑ Comorbid with eating disorder | ↓ Comorbid with eating disorder | Women are more likely than men to be comorbid with an eating disorder47 |
| Anxiety | ↓ Comorbid with drug or alcohol use disorder | ↑ Comorbid with drug or alcohol use disorder | Men are more likely than women to be comorbid with a drug or alcohol use disorder48 |
| PTSD | ↑ Comorbid with depression | ↓ Comorbid with depression | Women are more likely to be comorbid with depression49 |
This table summarizes the sex differences in comorbidity that are discussed in the Sex Differences in Common Psychiatric Disorders section. Women with depression tend to have comorbidity with eating disorders, men with anxiety tend to have comorbidity with drug or alcohol use disorders, and women with PTSD tend to have comorbidity with depression.
A variety of sex differences in the pharmacological treatment of depression have been researched. Some medications for depression include selective serotonin reuptake inhibitors (SSRIs) and tricyclic antidepressants (TCAs)50. Kornstein et al. found that women were more likely to respond favorably to sertraline, an SSRI, while men were more likely to respond favorably to imipramine, a TCA51. Another study found that women with nonmelancholic major depression, a form of depression less severe than melancholic major depression, or dysthymia, a long-lasting form of depression, found sertraline more effective and tolerable than imipramine, while men with the same disorders had a similar response to both drugs52. Additionally, a study found no sex differences in response to SSRIs and TCAs by women and men with melancholic and non-melancholic depression53. However, the same study noted that younger age was associated with a better response to SSRIs, and older age was associated with a better response to TCAs.
Due to the various study designs, length of the studies, and location of the studies, these findings contradict one another. Additionally, there are several biological factors that can contribute to these conflicting results and explain the sex differences that exist in the response to antidepressants. Some of these factors are pharmacokinetic, meaning they influence how the drug is broken down, like absorption in the stomach, distribution through the bloodstream, and rate of metabolism by enzymes54. Another study has found that genes may play a role in the efficacy of antidepressants, when gene expression impacts neural structures and neurotransmitters, especially in those who have MDD55. Therefore, due to the number of biological factors and studies with varying findings of responses to antidepressant pharmaceuticals, it is important to consider these sex differences in future treatment of depression.
There have also been observed sex differences in responsiveness to non-pharmacological methods of treatment. This includes cognitive behavioral therapy, counseling, psychoeducation, and other therapies. Women were more likely to rate cognitive behavioral therapy or counseling as more effective than men56 (Table 4). Another study found that women with depression more often lacked psychoeducation than men, and showed less comprehension of their depression than men57. The researchers believe that this is not linked with remission of depression in females, but possibly linked with the remission of depression in males. Additionally, not all subtypes of depression can be treated with just one type of treatment, with Miklowitz et. al confirming that medication in combination with a non-pharmacological treatment, such as cognitive behavioral therapy, is more effective at reducing recurring episodes in those with bipolar disorder58. Observations such as these allow for a further understanding of the effectiveness of these treatments in both women and men.
| Psychiatric Disorder | Female Tendencies | Male Tendencies | Interpretation |
| Depression | ↑ Likeliness to rate cognitive behavioral therapy or counseling as effective | ↓ Likeliness to rate cognitive behavioral therapy or counseling as effective | Women were more likely than men to rate non-pharmacological treatment as effective56 |
| Anxiety | ↑ Likeliness to seek a mental health professional | ↓ Likeliness to seek a mental health professional | “Feminization” of non-pharmacological treatment can impact its appeal for men59 |
| PTSD | ↑ Likeliness to seek pharmacological treatment | ↓ Likeliness to seek pharmacological treatment | Pharmacological treatments may be more popular due to comorbidity with anxiety and depression60 |
This table summarizes the sex differences in preferred treatments that are discussed in the Sex Differences in Common Psychiatric Disorders section. Women are more likely than men to seek a non-pharmacological treatment for depression and anxiety, but more likely to seek a pharmacological treatment for PTSD.
Anxiety
Anxiety is a common psychiatric disorder with a variety of subtypes and symptoms. Some of these include generalized anxiety disorder (GAD), social anxiety disorder (SAD), and panic disorder (PD). Symptoms of these subtypes can range, but they generally include feelings of worry, restlessness, or fear35. Anxiety is a psychiatric disorder that tends to be more prevalent in women than men. In a recent survey, approximately 23.8% of women had ever been diagnosed with anxiety, compared to 12.8% of men61. A review found that differences in gender socialization could contribute to the development of anxious behaviors, in addition to biological factors and having other psychiatric disorders62. This might provide an explanation for the sex differences that exist amongst anxiety disorders, and further research is encouraged to explore this pattern and others.
In order to study anxious behavior in animals, several models have been developed with various purposes in mind. A review focused on existing models describes unconditioned, conditioned, drug, and genetic animal models, the behavioral tests that are used, and the biological factors that contribute to anxiety63. The researchers of the review suggest the use of multiple models since one model may only elicit certain aspects of anxiety. In this review, the studies that used behavioral tests will be compared, but it is important to note the existence and the impact that other models may have. Behavioral tests of anxiety include the elevated plus maze (EPM) test, where rodents are monitored in an elevated plus-shaped maze with open and closed arms, and the large open field (LOF) test, where rodents are monitored in an open enclosed area64. Anxiety is measured in the EPM test by comparing how much time is spent on closed and open arms, since rodents tend to prefer closed arms that are darker where they cannot see the elevation. In the LOF test, researchers will measure anxiety by comparing the amount of time that is spent in the corners or the center of the area, with less exploratory rodents showing more anxiety and vice versa.
Knight et al. observed that females entered and spent more time on open arms during the EPM test and entered the center zone more than males during the LOF test65(Table 2). The researchers in this study note that the rodents were not exposed to any stressors beforehand, which could have affected the sex differences in the prevalence of anxiety-related behaviors. In another study, no sex differences were observed in the EPM test66. While these studies found female rodents to display less anxiety-like behavior and were more active than male rodents, this does not necessarily reflect the prevalence of anxiety-related behaviors in humans. Recent work has called for the development of new models that are validated with female animals, especially with the effect of the menstrual cycle in humans and estrous cycle in rodents on anxious behaviors67. It highlights the need for further research on sex differences, as animal models and the tests conducted on them are limited in mimicking the same disorders in humans.
There have been various observed sex differences in human studies of anxiety as well. Vesga-López et al. reported that women with lifetime generalized anxiety disorder (GAD) were more likely to have more autonomic, cardiovascular, respiratory, and gastrointestinal symptoms than men68. Additionally, the study also found that men were more often reported to use alcohol, medication, and drugs to help relieve their symptoms of GAD than women (Table 3). A sex difference is evident in the presentation of symptoms, along with reaction to symptoms, showing a similarity in humans and animal models. In another study, women who met criteria for social anxiety disorder (SAD) were more likely to report a greater number of social fears, while men who met criteria for SAD were more likely to report a greater number of dating fears69. Sex differences being exhibited in a range of fears in SAD represent the extent to which differences can occur. Additional observations in human studies of anxiety can provide further insight into the prevalence of these sex differences and their effect on diagnosis and treatment.
There are a variety of pharmacological treatments that have been developed for anxiety, along with sex differences that have been observed in some of those treatments of anxiety. Some common pharmacological treatments include benzodiazepines, buspirone, and antidepressants70. However, the female hormone progesterone is associated with reduced gastric acid production, which could affect dosage and ability to absorb certain medications, such as the anxiety medications mentioned above71. As such, it is clear that biological sex differences can impact the efficacy of treatment for anxiety disorders. Additionally, it has been observed that an equal number of women and men were using pharmacological methods to treat their anxiety, even though more women reported having an anxiety disorder72. However, the researchers also found a higher frequency of antidepressant use in women. This is in accordance with another study that found women to use medications for treatment significantly more often than men across all mental disorders73. However, the researchers mention that women were also more likely to be diagnosed with a mental disorder, which could affect prescription rates . They also say that stigmas around mental illness often vary from country to country, which would discourage reporting by men, impacting these frequencies. It is important that researchers continue to seek the best methods for the treatments of anxiety for women and men, even if they are not the same.
There are also a variety of non-pharmacological treatments for anxiety, in which sex differences have been observed. Examples of non-pharmacological treatments include psychoeducation, psychotherapy, and mindfulness programs, with each one dedicated to lessening symptoms in ways such as honing in on emotions, changing behavior, and becoming adaptable to anxious situations74. All of these non-pharmacological methods approach treating anxiety in different ways, but can have different effects on women and men.
This is reflected in the fact that men are less likely to seek a mental health professional, potentially due to ideas that it contradicts masculinity, and that non-pharmacological treatments tend to be “feminized”59 (Table 4). Many ideals of masculinity do not include the emotional vulnerability that these therapies require, and the “feminization” of these treatments may be due to a decent majority of mental health professionals being female. Sex differences in treatments can be affected by cultural and environmental issues such as these. Therefore, additional research is needed to further understand sex differences in anxiety to improve non-pharmacological treatments for women and men.
Post-traumatic Stress Disorder (PTSD)
Post-traumatic stress disorder (PTSD) is a trauma and stress-related disorder that used to be classified as a subtype of anxiety. The trauma response can turn pathological when an individual re-experiences symptoms such as flashbacks, nightmares, or memories. Encountering a reminder of trauma may also lead to emotional distress, such as thoughts of negativity, isolation, and self-blame75. The amalgamation of these symptoms may lead to irritability, concentration difficulties, and destructive behaviors75. It has been reported that women have a 2 to 3 times higher risk of developing PTSD, with the lifetime prevalence of PTSD being approximately 10-12% in women and 5-6% in men76. Hypotheses for this sex difference include exposure to trauma at a younger age, differences in emotional reactions to traumatic situations, and differences in brain activity in traumatic situations77. With the help of animal and human studies, these sex differences can be further explored to impact future diagnosis and treatment.
There are a variety of ways that PTSD can be modeled in animals. These include exposure to physical stressors, which may involve fear conditioning, and predator or predator odor exposure78. In fear conditioning, animals are exposed to unconditioned stimulus, such as an electric footshock, which cause natural or reflexive reactions, such as freezing, and are trained to associate it with a conditioned stimulus, such as a sound79. Fear extinction is the process of the conditioned stimulus occurring without the unconditioned stimulus, which results in the rodent creating a new memory in which the shock and sound are no longer associated. This review will highlight the findings of animal models with these tests that may provide insight to PTSD in humans.
In a study that used a stress-enhanced fear learning (SEFL) model, a version of fear conditioning, no sex differences were found in stress susceptibility, but the researchers note that sex differences existed in factors that predicted stress susceptibility, which can be genetic, biological, or environmental80. In the cat predator stress test, the vulnerability of the rodents is assessed after exposure to a cat or its odor. Adamec et al. found no sex differences in the behavior of mice after exposure to a cat, but that females were more likely to be vulnerable to the odors of a cat after exposure42 (Table 2). Another study found no sex differences in fear conditioning or fear extinction in rats81. However, the researchers suggested that a lack of a sex difference could be explained by a difference in fear expression by female rodents.
Most of these studies suggest that female rodents exhibit the same response to fear compared to male rodents. This lack of a sex difference in vulnerability may indicate a need for further research into the manifestation of PTSD specifically in female animal models However, the effect of the estrous cycle on animal models has been researched, with one study finding that the estrous cycle in adolescent rats may cause the fluctuation of fear inhibition, suppressing instincts of fear, and estradiol may protect against impairment in fear conditioning82. This is significant because multiple studies have found hormone levels during the menstrual cycle in human females to affect fear extinction83,84,85, which may bring into question the ability to use female animals as a comparable model. Therefore, further research is needed to understand the expression and extinction of PTSD in female rats, especially with the impact of biological factors.
There are a variety of sex differences that have been observed in human studies of PTSD. Men are more prone to developing PTSD after witnessing or experiencing combat, while women are more prone to developing PTSD after sexual assault or sexual molestation86. However, there are exceptions to these sex differences, and female veterans are an example of that. A study found that women and men who are exposed to similar levels of combat stress are equally likely to develop PTSD symptoms87. Despite these findings, the same study also found that men were still more likely to be diagnosed with PTSD. However, this may be due to a presentation of differing symptoms, and future research is necessary to understand how PTSD in female veterans may need to be diagnosed differently from PTSD in male veterans. Additionally, PTSD in all women and men may need to be diagnosed differently, since the trauma that is experienced is distinct, and therefore, may cause varying symptoms.
Comorbidity, the co-occurrence of two or more psychiatric disorders, is another aspect of analyzing sex differences in psychiatric disorders, such as PTSD. The findings from a study conducted in war veterans suggested that one can develop anxiety and depression because of PTSD but not vice versa88. However, another study argues that there could be instances where the disorders may just share common risk factors, causing their cooccurrence89. The researchers found that the main risk factors, regardless of gender, were childhood sexual assault and physical abuse. It has been found though, that women with childhood abuse, which could include sexual abuse, are more likely to have increased depressive symptoms in adulthood49 (Table 3). Therefore, it is important to acknowledge the common risk factors that may cause greater comorbidity in women. Additionally, when multiple disorders are involved, certain symptoms may not be as informative, which is why efforts are being made to identify if certain features of PTSD, depression, and anxiety can be used to differentiate from a symptom overlap90. Further research is still needed though, to understand all of these aspects of comorbidity.
The successful pharmacological treatment of PTSD is also impacted by sex differences, with one reason being due to disorder comorbidity. Some pharmacological treatments of PTSD include the SSRIs, sertraline and paroxetine91. In terms of sex differences in pharmacological treatments of PTSD, Bernardy et al. found that from 1999 to 2009, usage of SSRIs and SNRIs (serotonin-norepinephrine reuptake inhibitors) for treatment of veterans went from 56.4% to 65.7% in women, and 49.2% to 58.3% in men60 (Table 4). Benzodiazepines are commonly used for anxiety disorders, but are not recommended for PTSD treatment due to conflicting effects with non-pharmacological treatments. However, it was found that from 1999 to 2009, prescriptions went from 36.7% to 29.8% for men, and 33.4% to 38.3% for women60.
These sex differences may be due to comorbidity with anxiety and depression, since SSRIs, SNRIs, and benzodiazepines can be used to treat those disorders as well. There may be other reasons for these differing prescription rates, such as side effects of these medications that impact women and men in different ways. Additionally, sex differences in prescription rates could be due to increased exposure to off-label medications and television advertising, which are reflections of how prescription standards have developed over time92,93. Further research may be necessary to understand if this is the case, or if differing symptoms in women and men may need to be reevaluated before treatment.
Additionally, there are a variety of non-pharmacological treatments of PTSD in which sex differences have been observed. Some of these include trauma-focused therapies, such as prolonged exposure, eye movement desensitization and reprocessing, or cognitive processing therapy, all which have been shown to be especially beneficial, due to their individuality and non-group nature94. In terms of sex differences for non-pharmacological treatment, Galovski et al. found similar rates of it improving symptoms for women and men, and similar rates of drop-out for women and men95. Additionally, the same study found that several studies stated that women are more likely to gain benefits from treatment, and men have a higher risk of dropping out of treatment prematurely. By further understanding these sex differences, the necessities for better treatment can be tailored to women and men accordingly.
Discussion
Through the introduction of the Sex as a Biological Variable (SABV) policy in 2016, there has been an increase in the study of sex differences in the past decade. A review found that there has been a significant increase in studies that have included both sexes, but most of these studies lacked data analysis by sex96. Additionally, some researchers have found the inclusion of both sexes more costly, but acknowledge that identifying sex differences earlier on may save more time and money for human trials97. However, schools such as UCLA have participated in the NIH Office of Research on Women’s Health SCORE (Specialized Centers of Research Excellence) program to educate researchers on the undergraduate, graduate, postgraduate, and faculty levels about SABV with a Career Enhancement Core98. This research may add to the study of sex differences in psychiatric disorders, and shows how policy is impacting findings in neuroscience and other disciplines.
The sex differences that exist in depression, anxiety, and PTSD have been observed in animal and human models. Some models were inconclusive due to a lack of sex differences observed or not enough evidence to distinguish a sex difference. However, others have determined sex differences in research, and this disparity further encourages the need for future research, to add support or refutation to previous findings. Animal models may need to be created with different methods for simulating depression, anxiety, or PTSD. The study of human models may also need to be modified to better understand sex differences in symptoms and the effects of medication. Also, further research that identifies environmental, genetic, and other factors that can contribute to the development of psychiatric disorders may be helpful to reference for diagnosis and treatment. The research on these sex differences is critical to improving the lives of those with psychiatric disorders.
Additional Sex Differences in Psychiatric Research and Future Directions
Attention-deficit hyperactivity disorder (ADHD) is a psychiatric disorder that was not discussed in this review, but it contains prevalent sex differences. The core symptoms of ADHD include inattention and hyperactivity-impulsivity35. The majority of diagnoses occur in childhood, and the ratio of diagnoses is 3:1 for boys to girls99. However, research has determined that a significant number of girls go undiagnosed and untreated for ADHD, due to a presentation of more internalizing symptoms than externalizing symptoms100. Some of these internalizing symptoms include social difficulties, anxiety, and depression101.
Since presentations of symptoms of the disorder are typically reported by parents, teachers, and other persons close to the young boys and girls potentially with ADHD, a lack of detection of internalized symptoms has likely occurred, because they are harder to detect than externalizing symptoms102. An eight-year longitudinal study found that hormonal fluctuations and developmental changes during puberty may be one reason as to why girls may tend to present more internalizing symptoms103. However, another study found an equal need to monitor boys and girls for both externalizing and internalizing symptoms, claiming that both can be under-recognized104. This review previously mentioned how comorbidity is difficult to determine with depression, anxiety, and PTSD, and similarly, it can be difficult to distinguish for depression, anxiety, and ADHD. This may be an instance where symptoms are overlapping, but generally there is obscurity in pinpointing the origin of symptoms, and as a result, diagnosing comorbidity or ADHD. While certainly more research is needed, awareness of this potential comorbidity should also be spread, to further prevent diagnoses and treatment from not happening.
ADHD is also studied in a preclinical setting; however, researchers find difficulty replicating some features of ADHD in rodents. ADHD is the product of genetic, epigenetic, and environmental factors; however, rodent researchers are limited to studying a few key behavioral traits, such as inattentiveness and hyperactivity105. In terms of treatment of ADHD, a review found that stimulants, such as methylphenidate, may require further research to investigate their effect on symptoms in girls, while non-stimulants, such as atomoxetine, have been found to treat symptoms between sexes effectively106. Further research of sex differences in diagnosis and treatments of ADHD allows for the understanding of the disorder to increase, so those who have gone undiagnosed and untreated, specifically girls, may be positively impacted.
Substance use disorders (SUDs) are another type of psychiatric disorder that was not discussed in this review but has also been observed to have sex differences. A substance use disorder is described as a condition where a substance that often has harmful consequences is abused and limits one’s ability to perform daily functions107. Additionally, SUDs are often commonly diagnosed in people with psychiatric disorders such as depression, anxiety, ADHD, and PTSD, which may influence the treatment of these disorders108,109. This review will only highlight sex differences in alcohol misuse, but there are various other SUDs involving substances such as cannabis, opioids, and nicotine110.
There are a few biological sex differences that may impact the prevalence of an alcohol use disorder (AUD) in men versus women. Women have been observed to exhibit lower levels of activity for the enzyme that metabolizes ethanol, alcohol dehydrogenase, and lower total body water111. This causes women to have a higher blood alcohol concentration, even if they consume the same amount of alcohol as men112, which may create a need for distinct diagnostic criteria for women and men. A study found that significant alcohol usage may have a greater effect on women in the regulation of negative emotions in the brain113. While more research is needed to confirm this, it is worth noting the intersection of alcohol misuse and mood, as it was previously mentioned that alcohol misuse is often diagnosed with other psychiatric disorders.
Biological impacts are likely one of the contributors to the varying patterns of alcohol usage in women and men. Historically, men have been found to consume more alcohol than women and have been more likely to be diagnosed with an AUD, but evidence suggests that this difference is becoming smaller114. However, a gender gap in the prevalence of SUDs may also be dictated by access to substances and gender roles that can vary from country to country115. In terms of the treatment of alcohol usage, Alvanzo et al. found that women are less likely than men to receive treatment, but women tend to have a shorter period between the onset of a dependency and the usage of a treatment such as therapy116. Sex differences in substance use disorders require further research to understand the several factors that can contribute to them.
Comorbidity is another topic that requires more research, especially pertaining to the disorders that were discussed in this review. Comorbidity for depression and anxiety with PTSD or ADHD was discussed, but it can commonly develop in a variety of other ways. For example, MDD and SAD are highly comorbid with one another, with Kim & Duval finding that the relationship between social interaction anxiety and individual depression symptoms can vary by gender117. Additionally, the comorbidity of psychiatric disorders in women can make it difficult to treat women who develop an SUD, too118. This may be an explanation for sex differences in the lack of diagnosis and treatment of SUDs. Therefore, it is important for further research to be conducted surrounding comorbidity, to determine how disorders should be treated in tandem, where an ideal mixture of the treatments from each individual disorder is created, tailored to an individual’s specific symptoms. The sex differences that exist in these psychiatric disorders individually are significant enough to necessitate their own research, but comorbidity is an important factor to consider when studying these differences.
With the study of sex differences rapidly expanding, measures can be taken to publicize key findings. Currently, there is an international standard called the Sex and Gender Equity in Research (SAGER) guidelines, which promote systematic reporting of sex and gender across biomedical research and help authors and editors determine appropriate consideration of these variables119. Many science and clinical journals have adopted the SAGER guidelines and other policies, but are still not consistently utilized120. Therefore, it is important that the publication of sex difference research in journals continues to be encouraged. Additionally, journals could also dedicate specific issues to publishing sex difference research, allowing for these findings to have their own spotlight. As more sex difference findings occur, it will be important to highlight them and emphasize them, and that can start with greater journal recognition.
In addition to the expansion of publicizing sex differences, the study of sex differences in psychiatric disorders can also be grown. In this review, studies regarding depression, anxiety, PTSD, were discussed, conducted under various circumstances within the past 20 years. Findings from a review of multiple psychiatric disorders including anxiety, suggested that female mice presented with lower levels of anxiety than male mice121, which is comparable to another study that found that female mice displayed lower levels of anxiety than male mice, particularly in the EPM and LOF tests65. While these studies share similar findings, this representation of anxiety in mice is not comparable to anxiety in humans, which tends to be greater in females than in males. Within this review, this has been attributed to environmental circumstances for the animals and comorbidity potentials for humans. However, this still necessitates further research to be conducted surrounding psychiatric disorders, in order to explain disparities and determine their impact on the study of sex differences.
Conclusion
Sex differences in psychiatric disorders are numerous and have been researched in various contexts. The continuation of this research ensures the improvement of diagnosis and treatment standards that do not fully reflect sex differences. Additionally, further research will ensure that a greater understanding of these disorders has been achieved. Even outside of psychiatry and neuroscience, the study of sex differences should continue to expand. It is important for this research to advance current knowledge and further developments in the treatment of disorders that afflict people all over the world.
Acknowledgements
The author would like to thank Dr. Amanda G Iglesias and Dr. Elizabeth Tawa for their endless support in the writing of this paper. Additionally, thanks are given to Kiana Manian, Srishti Bansal, and the Lumiere team for their support.
Reference
- A. K. Beery & I. Zucker. Sex Bias in Neuroscience and Biomedical Research. Neuroscience and Biobehavioral Reviews. 35(3), 565–572 (2011). [↩]
- Institute of Medicine (US) Committee on Ethical and Legal Issues Relating to the Inclusion of Women in Clinical Studies. Mastroianni AC, Faden R, Federman D, editors. Women and Health Research: Ethical and Legal Issues of Including Women in Clinical Studies: Volume I. Washington (DC): National Academies Press (US); 1994. B, NIH Revitalization Act of 1993 Public Law 103-43 [↩]
- M. E. Arnegard, L. A. Whitten, C. Hunter, & J. A. Clayton. Sex as a Biological Variable: A 5-Year Progress Report and Call to Action. Journal of Women’s Health. 29(6), 858–864 (2020). [↩]
- M. M. Herting & E. R. Sowell. Puberty and structural brain development in humans. Frontiers in Neuroendocrinology. 44, 122–137 (2017). [↩] [↩] [↩]
- J. S. Perrin, G. Leonard, M. Perron, G. B. Pike, A. Pitiot, L. Richer, S. Veillette, Z. Pausova, & T. Paus. Sex differences in the growth of white matter during adolescence. NeuroImage, 45(4), 1055–1066 (2009). [↩] [↩]
- S. Neufang, K. Specht, M. Hausmann, O. Güntürkün, B. Herpertz-Dahlmann, G. R. Fink, & K. Konrad. Sex differences and the impact of steroid hormones on the developing human brain. Cerebral Cortex. 19(2), 464–473 (2009). [↩] [↩]
- M. Ingalhalikar, A. Smith, D. Parker, T. D. Satterthwaite, M. A. Elliott, K. Ruparel, H. Hakonarson, R. E. Gur, R. C. Gur, & R. Verma. Sex differences in the structural connectome of the human brain. Proceedings of the National Academy of Sciences of the United States of America. 111(2), 823–828 (2014). [↩] [↩] [↩]
- J. S. Stevens & S. Hamann. Sex differences in brain activation to emotional stimuli: a meta-analysis of neuroimaging studies. Neuropsychologia. 50(7), 1578–1593 (2012). [↩] [↩] [↩]
- J. Hänggi, L. Fövenyi, F. Liem, M. Meyer, & L. Jäncke. The hypothesis of neuronal interconnectivity as a function of brain size-a general organization principle of the human connectome. Frontiers in Human Neuroscience. 8, 915 (2014). [↩]
- L. Jäncke. Sex/gender differences in cognition, neurophysiology, and neuroanatomy. F1000Research. 7 F1000 Faculty Rev, 805 (2018). [↩]
- L. Kogler, R. C. Gur, & B. Derntl. Sex differences in cognitive regulation of psychosocial achievement stress: brain and behavior. Human Brain Mapping. 36(3), 1028–1042 (2015). [↩]
- J. McHenry, N. Carrier, E. Hull, & M. Kabbaj. Sex differences in anxiety and depression: role of testosterone. Frontiers in Neuroendocrinology. 35(1), 42–57 (2014). [↩] [↩]
- M. M. Shores, K. L. Sloan, A. M. Matsumoto, V. M. Moceri, B. Felker, & D. R. Kivlahan. Increased incidence of diagnosed depressive illness in hypogonadal older men. Archives of General Psychiatry. 61(2), 162–167 (2004). [↩]
- C. J. DiBlasio, J. Hammett, J. B. Malcolm, B. A. Judge, J. H. Womack, M. C. Kincade, M. L. Ogles, J. G. Mancini, A. L. Patterson, R. W. Wake, & I. H.Derweesh. Prevalence and predictive factors for the development of de novo psychiatric illness in patients receiving androgen deprivation therapy for prostate cancer. The Canadian Journal of Urology. 15(5), 4249–4256 (2008). [↩]
- E. J. Giltay, D. Enter, F.G. Zitman, B. Penninx, J. Van Pelt, P. Spinhoven, K. Roelofs. Salivary testosterone: Associations with depression, anxiety disorders, and antidepressant use in a large cohort study. Journal of Psychosomatic Research. 72(3), 205-213 (2012). [↩]
- K. K. Miller, R. H. Perlis, G. I. Papakostas, D. Mischoulon, D. V. Losifescu, D. J. Brick, & M. Fava. Low-dose transdermal testosterone augmentation therapy improves depression severity in women. CNS Spectrums. 14(12), 688–694 (2009). [↩]
- G. A. van Wingen, S. A. Zylicz, S. Pieters, C. Mattern, R. J. Verkes, J. K. Buitelaar, & G. Fernández. Testosterone increases amygdala reactivity in middle-aged women to a young adulthood level. Neuropsychopharmacology: official publication of the American College of Neuropsychopharmacology. 34(3), 539–547 (2009). [↩]
- U. D. Rohr. The impact of testosterone imbalance on depression and women’s health. Maturitas. 41 Suppl 1, S25–S46 (2002). [↩]
- K. M. Albert, & P. A. Newhouse. Estrogen, Stress, and Depression: Cognitive and Biological Interactions. Annual Review of Clinical Psychology. 15, 399–423 (2019). [↩]
- M. Kundakovic & D. Rocks. Sex hormone fluctuation and increased female risk for depression and anxiety disorders: From clinical evidence to molecular mechanisms. Frontiers in Neuroendocrinology. 66, 101010 (2022). [↩]
- W. J. Hwang, T. Y. Lee, N. S. Kim, & J. S. Kwon. The Role of Estrogen Receptors and Their Signaling across Psychiatric Disorders. International Journal of Molecular Sciences. 22(1), 373 (2020). [↩]
- E. Findikli, E. B. Kurutas, M. A. Camkurt, M. F. Karaaslan, F. Izci, H. A. Fındıklı, S. Kardaş, B. Dag, & H. Altun. Increased Serum G Protein-coupled Estrogen Receptor 1 Levels and Its Diagnostic Value in Drug Naïve Patients with Major Depressive Disorder. Clinical Psychopharmacology and Neuroscience : The Official Scientific Journal of the Korean College of Neuropsychopharmacology. 15(4), 337–342 (2017). [↩]
- R. M. Shansky. Are hormones a “female problem” for animal research?. Science. 364, 825-826 (2019). [↩] [↩]
- C. Wald & C. Wu. Biomedical research. of mice and women: The bias in animal models. Science. 327, 1571-1572 (2010). [↩]
- National Institute of Health: Office of Research on Women’s Health. Sex as a Biological Variable. https://orwh.od.nih.gov/sex-as-biological-variable (2025). [↩]
- G.B. Gereau, M.L. Torruella-Suárez, S.E. Sizer, M. Xia, D. Zhou, L.A. Wykoff, A.T. Teklezghi, A. Alvarez-Pamir, K.M. Boyt, T. L. Kash, & Z. A. McElligott. GABA release from central amygdala neurotensin neurons differentially modulates ethanol consumption in male and female mice. Neuropsychopharmacol. 49, 1151–1161 (2024). [↩]
- C. L. Lloreda. NIH appears to archive policy requiring female animals in studies. https://www.thetransmitter.org/policy/exclusive-nih-appears-to-archive-policy-requiring-female-animals-in-studies/ (2025). [↩]
- N. I. Gavin, B. N. Gaynes, K. N. Lohr, S. Meltzer-Brody, G. Gartlehner, & T. Swinson. Perinatal depression: a systematic review of prevalence and incidence. Obstetrics and Gynecology. 106(5 Pt 1), 1071–1083 (2005). [↩]
- E. J. Fawcett, N. Fairbrother, M. L. Cox, I. R. White, & J. M. Fawcett. The Prevalence of Anxiety Disorders During Pregnancy and the Postpartum Period: A Multivariate Bayesian Meta-Analysis. The Journal of Clinical Psychiatry. 80(4), 18r12527 (2019). [↩]
- A. Biaggi, S. Conroy, S. Pawlby, & C. M. Pariante. Identifying the women at risk of antenatal anxiety and depression: A systematic review. Journal of Affective Disorders. 191, 62–77 (2016). [↩]
- A. L. Salisbury, K. E. O’Grady, C. L. Battle, K. L. Wisner, G. M. Anderson, L. R. Stroud, C. L. Miller-Loncar, M. E. Young, & B. M. Lester. The Roles of Maternal Depression, Serotonin Reuptake Inhibitor Treatment, and Concomitant Benzodiazepine Use on Infant Neurobehavioral Functioning Over the First Postnatal Month. The American Journal of Psychiatry. 173(2), 147–157 (2016). [↩]
- L. A. Magee, A. Pels, M. Helewa, E. Rey, P. von Dadelszen, & Canadian Hypertensive Disorders of Pregnancy (HDP) Working Group. Diagnosis, evaluation, and management of the hypertensive disorders of pregnancy. Pregnancy Hypertension. 4(2), 105–145 (2014). [↩]
- N. Bernard, J. C. Forest, G. M. Tarabulsy, E. Bujold, D. Bouvier, & Y. Giguère. Use of antidepressants and anxiolytics in early pregnancy and the risk of preeclampsia and gestational hypertension: a prospective study. BMC Pregnancy and Childbirth. 19(1), 146 (2019). [↩]
- W. L. Pan, C. W. Chang, S. M. Chen, & M. L. Gau. Assessing the effectiveness of mindfulness-based programs on mental health during pregnancy and early motherhood – a randomized control trial. BMC Pregnancy and Childbirth. 19(1), 346 (2019). [↩]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. (5th ed., text rev.) (2022). [↩] [↩] [↩]
- What is Depression? https://www.psychiatry.org/patients-families/depression/what-is-depression#section_6 (2024). [↩]
- D.J. Brody, J.P. Hughes. Depression Prevalence in Adolescents and Adults: United States, August 2021–August 2023. National Center for Health Statistics. (527), 1–11 (2025). [↩]
- N. Kokras, & C. Dalla. Sex differences in animal models of psychiatric disorders. British Journal of Pharmacology. 171(20), 4595-4619 (2014). [↩] [↩]
- C. Pitzer, B. Kurpiers, & A. Eltokhi. Sex Differences in Depression-Like Behaviors in Adult Mice Depend on Endophenotype and Strain. Frontiers in Behavioral Neuroscience. 16, 838122 (2022). [↩]
- P. Barai, V. Pogakula, J. S. Sandhu, A. Parida, N. Krishnadas & G. L. Viswanatha. Re‐evaluating the forced swim test: ethical, scientific, and regulatory drivers for validated alternatives. Frontiers in Animal Science. 7, 1692092 (2026). [↩]
- P. Knight, R. Chellian, R. Wilson, A. Behnood-Rod, S. Panunzio, & A. W. Bruijnzeel. Sex differences in the elevated plus-maze test and large open field test in adult Wistar rats. Pharmacology, Biochemistry, and Behavior. 204, 173168 (2021). [↩]
- R. Adamec, P. Burton, J. Blundell, D. L. Murphy, & A. Holmes. Vulnerability to mild predator stress in serotonin transporter knockout mice. Behavioral Brain Research. 170 (1), 126–140 (2006). [↩] [↩]
- A. Cavanagh, C. J. Wilson, D. J. Kavanagh, & P. Caputi. Differences in the Expression of Symptoms in Men Versus Women with Depression: A Systematic Review and Meta-analysis. Harvard Review of Psychiatry. 25(1), 29–38 (2017). [↩]
- M. Altemus, N. Sarvaiya, & C. Neill Epperson. Sex differences in anxiety and depression clinical perspectives. Frontiers in Neuroendocrinology. 35(3), 320–330 (2014). [↩]
- M. D. De Bellis, E. G. Spratt, & S. R. Hooper. Neurodevelopmental biology associated with childhood sexual abuse. Journal of Child Sexual Abuse. 20(5), 548–587 (2011). [↩]
- K. M. Gorey & D. R. Leslie. The prevalence of child sexual abuse: Integrative review adjustment for potential response and measurement biases. Child Abuse & Neglect. 21(4), 391-398 (1997). [↩]
- M. Altemus, N. Sarvaiya, & C. Neill Epperson. Sex differences in anxiety and depression clinical perspectives. Frontiers in Neuroendocrinology. 35(3), 320–330 (2014). [↩]
- O. Vesga-López, F. R. Schneier, S. Wang, R. G. Heimberg, S. M. Liu, D. S. Hasin, & C. Blanco. Gender differences in generalized anxiety disorder: results from the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC). The Journal of Clinical Psychiatry. 69(10), 1606–1616 (2008). [↩]
- S. Assari, B. Najand, & A. Donovan. Sex/Gender Differences in the Effects of Childhood Abuse on Future Risk of Depression: Longitudinal Evidence from the Global Flourishing Study. Children (Basel, Switzerland). 12(6), 754 (2025). [↩] [↩]
- J. J. Sramek, M. F. Murphy, & N. R. Cutler. Sex differences in the psychopharmacological treatment of depression. Dialogues in Clinical Neuroscience. 18(4), 447–457 (2016). [↩]
- S. G. Kornstein, A. F. Schatzberg, M. E. Thase, K. A. Yonkers, J. P. McCullough, G. I. Keitner, A. J. Gelenberg, S. M. Davis, W. M. Harrison, & M. B. Keller. Gender differences in treatment response to sertraline versus imipramine in chronic depression. The American Journal of Psychiatry. 157(9), 1445–1452 (2000). [↩]
- E. Baca, M. Garcia-Garcia, & A. Porras-Chavarino. Gender differences in treatment response to sertraline versus imipramine in patients with nonmelancholic depressive disorders. Progress in Neuro-psychopharmacology & Biological Psychiatry. 28(1), 57–65 (2004). [↩]
- G. Parker, K. Parker, M. P. Austin, P. Mitchell, & H. Brotchie. Gender differences in response to differing antidepressant drug classes: two negative studies. Psychological Medicine. 33(8), 1473–1477 (2003). [↩]
- J. Seifert. Do sex and gender matter in the pharmacological treatment of depression?. Naunyn-Schmiedeberg’s Archives of Pharmacology. 399(3), 3353–3368 (2026). [↩]
- A. G. Bertollo, R. Mocelin, & Z. M. Ignácio. Pharmacogenetics and the Response to Antidepressants in Major Depressive Disorder. Pharmaceuticals (Basel, Switzerland). 18(9), 1360 (2025). [↩]
- G. Parker & J. Crawford. Personality and self-reported treatment effectiveness in depression. The Australian and New Zealand Journal of Psychiatry. 43(6), 518–525 (2009). [↩] [↩]
- T. Tomita, S. Kudo, N. Sugawara, A. Fujii, K. Tsuruga, Y. Sato, M. Ishioka, K. Nakamura, & N. Yasui-Furukori. Sex Differences In Psychoeducation For Patients With Depression: A Comparison Of Frequency And Efficacy Of Psychoeducation. Neuropsychiatric Disease and Treatment. 15, 3069–3078 (2019). [↩]
- D. J. Miklowitz, O. Efthimiou, T. A. Furukawa, J. Scott, R. McLaren, J. R. Geddes, & A. Cipriani. Adjunctive Psychotherapy for Bipolar Disorder: A Systematic Review and Component Network Meta-analysis. JAMA Psychiatry. 78(2), 141–150 (2021). [↩]
- W. Affleck, V. Carmichael, & R. Whitley. Men’s Mental Health: Social Determinants and Implications for Services. Canadian Journal of Psychiatry. 63(9), 581–589 (2018). [↩] [↩]
- N. C. Bernardy, B. C. Lund, B. Alexander, A. B. Jenkyn, P. P. Schnurr, & M. J. Friedman. Gender differences in prescribing among veterans diagnosed with posttraumatic stress disorder. Journal of General Internal Medicine. 28 Suppl 2(Suppl 2), S542–S548 (2013). [↩] [↩] [↩]
- Mental Health Conditions & Care https://www.cdc.gov/mental-health/about-data/conditions-care.html?cove-tab=2 (2025). [↩]
- N. Z. Farhane-Medina, B. Luque, C. Tabernero, & R. Castillo-Mayén. Factors associated with gender and sex differences in anxiety prevalence and comorbidity: A systematic review. Science Progress. 105(4), 368504221135469 (2022). [↩]
- H. Zhao, M. Zhou, Y. Liu, J. Jiang, & Y. Wang. Recent advances in anxiety disorders: Focus on animal models and pathological mechanisms. Animal Models and Experimental Medicine. 6(6), 559–572 (2023). [↩]
- Himanshu, Dharmila, D. Sarkar, & Nutan. A Review of Behavioral Tests to Evaluate Different Types of Anxiety and Anti-anxiety Effects. Clinical Psychopharmacology and Neuroscience : The Official Scientific Journal of the Korean College of Neuropsychopharmacology. 18(3), 341–351 (2020). [↩]
- P. Knight, R. Chellian, R. Wilson, A. Behnood-Rod, S. Panunzio, & A. W. Bruijnzeel. Sex differences in the elevated plus-maze test and large open field test in adult Wistar rats. Pharmacology, Biochemistry, and Behavior. 204, 173168 (2021). [↩] [↩]
- I.V. Pavlova, N.D. Broshevitskaya, M.V. Onufriev, Y.W. Moiseeva. Sex-Related Differences in Anxious-Depressive and Defensive Behavior in Wistar Rats. Neuroscience and Behavioral Physiology. 50(9), 1163–1175 (2020). [↩]
- T. A. Lovick & H. Zangrossi Jr. Effect of Estrous Cycle on Behavior of Females in Rodent Tests of Anxiety. Frontiers in Psychiatry. 12, 711065 (2021). [↩]
- O. Vesga-López, F. R. Schneier, S. Wang, R. G. Heimberg, S. M. Liu, D. S. Hasin, & C. Blanco. Gender differences in generalized anxiety disorder: results from the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC). The Journal of Clinical Psychiatry. 69(10), 1606–1616 (2008). [↩]
- Y. Xu, F. Schneier, R. G. Heimberg, K. Princisvalle, M. R. Liebowitz, S. Wang, & C. Blanco. Gender differences in social anxiety disorder: results from the national epidemiologic sample on alcohol and related conditions. Journal of Anxiety Disorders. 26(1), 12–19 (2012). [↩]
- M. P. Fankhauser. Psychiatric disorders in women: psychopharmacologic treatments. Journal of the American Pharmaceutical Association. NS37(6), 667–678 (1997). [↩]
- I. Jalnapurkar, M. Allen, & T. Pigott. Sex Differences in Anxiety Disorders: A Review. HSOA Journal of Psychiatry, Depression, and Anxiety. 4(1) 12 (2018). [↩]
- C. S. Estancial Fernandes, R. C. S. de Azevedo, M. Goldbaum, & M. B. A. Barros. Psychotropic use patterns: Are there differences between men and women?. PloS one. 13(11), e0207921 (2018). [↩]
- C. Maestre-Miquel, A. López-de-Andrés, Z. Ji, J. de Miguel-Diez, A. Brocate, S. Sanz-Rojo, A. López-Farre, D. Carabantes-Alarcon, R. Jiménez-García, & J. J. Zamorano-León. Gender Differences in the Prevalence of Mental Health, Psychological Distress and Psychotropic Medication Consumption in Spain: A Nationwide Population-Based Study. International Journal of Environmental Research and Public Health. 18(12), 6350 (2021). [↩]
- P. Rautio. The Non-Pharmacological Treatment Methods of Anxiety Disorders. Theseus UAS.(2021). [↩]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. (5th ed., text rev.) (2022 [↩] [↩]
- M. Olff. Sex and gender differences in post-traumatic stress disorder: an update. European Journal of Psychotraumatology. 8(sup4) (2017). [↩]
- M. Olff. Sex and gender differences in post-traumatic stress disorder: an update. European Journal of Psychotraumatology. 8(sup4) (2017). [↩]
- G. F. Mancini, S. A. Torrisi, E. M. G. Viho, O. C. Meijer, G. M. Leggio, & P. Campolongo. Interindividual and sex differences in resilience and vulnerability to post-traumatic stress disorder (PTSD): insights from animal models. Biology of Sex Differences. 16(1), 50 (2025). [↩]
- T. C. M. Bienvenu, C. Dejean, D. Jercog, B. Aouizerate, M. Lemoine, & C. Herry. The advent of fear conditioning as an animal model of post-traumatic stress disorder: Learning from the past to shape the future of PTSD research. Neuron. 109(15), 2380–2397 (2021). [↩]
- S. T. Gonzalez, V. Marty, I. Spigelman, S. P. Reise, & M. S. Fanselow. Impact of stress resilience and susceptibility on fear learning, anxiety, and alcohol intake. Neurobiology of Stress. 15, 100335 (2021). [↩]
- R. M. Shansky. Sex differences in PTSD resilience and susceptibility: Challenges for animal models of Fear Learning. Neurobiology of Stress. 1, 60–65 (2015). [↩]
- A. Gable, R. Richardson, & K. D. Baker. Estrous Cycle Impacts Fear Extinction and Relapse in Female Adolescent Rats. Developmental Psychobiology. 67(5), e70084 (2025). [↩]
- K. Lebron-Milad & M. R. Milad. Sex differences, gonadal hormones and the fear extinction network: implications for anxiety disorders. Biology of Mood & Anxiety Disorders. 2, 3 (2012). [↩]
- E. M. Glover, T. Jovanovic, K. B. Mercer, K. Kerley, B. Bradley, K. J. Ressler, & S. D. Norrholm. Estrogen levels are associated with extinction deficits in women with posttraumatic stress disorder. Biological Psychiatry. 72(1), 19–24 (2012). [↩]
- S. L. Pineles, Y. I. Nillni, G. Pinna, A. Webb, K. A. Arditte Hall, J. R. Fonda, J. Irvine, M. W. King, R. L. Hauger, P. A. Resick, S. P. Orr, & A. M. Rasmusson. Associations between PTSD-Related extinction retention deficits in women and plasma steroids that modulate brain GABAA and NMDA receptor activity. Neurobiology of Stress. 13, 100225 (2020). [↩]
- R. C. Kessler, A. Sonnega, E. Bromet, M. Hughes, & C. B. Nelson. Posttraumatic stress disorder in the National Comorbidity Survey. Archives of General Psychiatry. 52(12), 1048–1060 (1995). [↩]
- A. Pereira. Combat trauma and the diagnosis of post-traumatic stress disorder in female and male veterans. Military Medicine. 167(1), 23–27 (2002). [↩]
- K. Ginzburg, T. Ein-Dor, Z. Solomon. Comorbidity of posttraumatic stress disorder, anxiety and depression: A 20-year longitudinal study of war veterans. Journal of Affective Disorders. 123(1-3), 249-257 (2010). [↩]
- P. Spinhoven, B. W. Penninx, A. M. van Hemert, M. de Rooij, & B. M. Elzinga. Comorbidity of PTSD in anxiety and depressive disorders: Prevalence and shared risk factors. Child Abuse & Neglect. 38(8), 1320-1330 (2014). [↩]
- A. C. Barbano, W. F. van der Mei, T. A. deRoon-Cassini, E. Grauer, S. R. Lowe, Y. J. Matsuoka, M. O’Donnell, M. Olff, W. Qi, A. Ratanatharathorn, U. Schnyder, S. Seedat, R. C. Kessler, K. C. Koenen, A. Y. Shalev, & International Consortium to Prevent PTSD. Differentiating PTSD from anxiety and depression: Lessons from the ICD-11 PTSD diagnostic criteria. Depression and Anxiety. 36(6), 490–498 (2019). [↩]
- C. R. Proença, J. C. Markowitz, B. M. Coimbra, H. Cogo-Moreira, M. R. Maciel, A. F. Mello, & M. F. Mello. Interpersonal psychotherapy versus sertraline for women with posttraumatic stress disorder following recent sexual assault: a randomized clinical trial. European Journal of Psychotraumatology. 13(2), 2127474 (2022). [↩]
- R. J. Avery, M. D. Eisenberg, & K. I. Simon. The impact of direct-to-consumer television and magazine advertising on antidepressant use. Journal of Health Economics. 31(5), 705–718 (2012). [↩]
- D. Kharadi, K. Patel, D. Rana, & V. Patel. Off-label drug use in Psychiatry Outpatient Department: A prospective study at a Tertiary Care Teaching Hospital. Journal of Basic and Clinical Pharmacy. 6(2), 45–49 (2015). [↩]
- C. Schrader, & A. Ross. A Review of PTSD and Current Treatment Strategies. Missouri Medicine. 118(6), 546–551(2021). [↩]
- T. E. Galovski, L. M. Blain, C. Chappuis, & T. Fletcher. Sex differences in recovery from PTSD in male and female interpersonal assault survivors. Behaviour Research and Therapy. 51(6), 247–255 (2013). [↩]
- N. C. Woitowich, A. Beery, & T. Woodruff. A 10-year follow-up study of sex inclusion in the biological sciences. eLife. 9, e56344 (2020). [↩]
- M. Waltz, J. A. Fisher, A. D. Lyerly, & R. L. Walker. Evaluating the National Institutes of Health’s Sex as a Biological Variable Policy: Conflicting Accounts from the Front Lines of Animal Research. Journal of Women’s Health. 30(3), 348–354 (2021). [↩]
- K. Reue & A. P. Arnold. Inclusion of Sex as a Biological Variable in Biomedical Sciences at the Undergraduate Level and Beyond. Journal of Women’s Health. 32(8), 891–896 (2023). [↩]
- E. G. Willcutt. The prevalence of DSM-IV attention-deficit/hyperactivity disorder: a meta-analytic review. Neurotherapeutics : The Journal of the American Society for Experimental NeuroTherapeutics. 9(3), 490–499 (2012). [↩]
- J. Gershon. A meta-analytic review of gender differences in ADHD. Journal of Attention Disorders. 5(3), 143–154 (2002). [↩]
- E. W. Skogli, M. H. Teicher, P. N. Andersen, K. T. Hovik, & M. Øie. ADHD in girls and boys-gender differences in co-existing symptoms and executive function measures. BMC Psychiatry. 13, 298 (2013). [↩]
- S. Young, N. Adamo, B. B. Ásgeirsdóttir, P. Branney, M. Beckett, W. Colley, S. Cubbin, Q. Deeley, E. Farrag, G. Gudjonsson, P. Hill, J. Hollingdale, O. Kilic, T. Lloyd, P. Mason, E. Paliokosta, S. Perecherla, J. Sedgwick, C. Skirrow, K. Tierney, K. van Rensburg, & E. Woodhouse. Females with ADHD: An expert consensus statement taking a lifespan approach providing guidance for the identification and treatment of attention-deficit/ hyperactivity disorder in girls and women. BMC Psychiatry. 20(1), 404 (2020). [↩]
- A. G. Eng, J. M. Phan, E. A. Shirtcliff, T. A. Eisenlohr-Moul, P. K. Goh, & M. M. Martel. Aging and Pubertal Development Differentially Predict Symptoms of ADHD, Depression, and Impairment in Children and Adolescents: An Eight-Year Longitudinal Study. Research on Child and Adolescent Psychopathology. 51(6), 819–832 (2023). [↩]
- A. Mlodnicka, M. Mansolf, A. Chandran, I. M. Aris, C. A. Calub, S. Ahmad, A. Shapiro, D. Cochran, B. Restrepo, R. Schmidt, I. Hertz-Picciotto, D. Bennett, D. R. Gold, T. M. O’Shea, L. Leve, J. B. Schweitzer, & program collaborators for Environmental influences on Child Health Outcomes*. Prediction of internalizing and externalizing symptoms in late childhood from attention-deficit/hyperactivity disorder symptoms in early childhood. Development and Psychopathology. 37(2), 815–824 (2025). [↩]
- S. L. Regan, M. T. Williams, & C. V. Vorhees. Review of rodent models of attention deficit hyperactivity disorder. Neuroscience and Biobehavioral Reviews. 132, 621–637 (2022). [↩]
- F. M. Kok, Y. Groen, A. B. M. Fuermaier, & O. Tucha. The female side of pharmacotherapy for ADHD-A systematic literature review. PloS One. 15(9), e0239257 (2020). [↩]
- What Is a Substance Use Disorder? https://www.psychiatry.org/patients-families/addiction-substance-use-disorders/what-is-a-substance-use-disorder (2024). [↩]
- Substance Abuse and Mental Health Services Administration. 2021 NSDUH Annual National Report. https://www.samhsa.gov/data/report/2021-nsduh-annual-national-report (2023). [↩]
- C. G. Imperio, F. R. Levin, & D. Martinez. The Neurocircuitry of Substance Use Disorder, Treatment, and Change: A Resource for Clinical Psychiatrists. The American Journal of Psychiatry. 181(11), 958–972 (2024). [↩]
- CDC. Treatment of Substance Use Disorders. https://www.cdc.gov/overdose-prevention/treatment/index.html (2024). [↩]
- R. K. McHugh, V. R. Votaw, D. E. Sugarman, & S. F. Greenfield. Sex and Gender Differences in Substance Use Disorders. Clinical Psychology Review. 66, 12–23 (2018). [↩]
- E. Baraona, C.S. Abittan, K. Dohmen, M. Moretti, G. Pozzato, Z. W. Chayes, C. Schaefer, & C. S Lieber. Gender differences in pharmacokinetics of alcohol. Alcoholism, Clinical and Experimental Research. 25(4), 502–507 (2001). [↩]
- S. Chaudhary, Y. Chen, H. K. Wong, H. H. Chao, & C. R. Li. Alcohol misuse and negative emotion processing in neurotypical drinkers: Sex differences in behavioral and neural markers. Psychiatry Research: Neuroimaging. 358, 112174 (2026). [↩]
- A. M. White. Gender Differences in the Epidemiology of Alcohol Use and Related Harms in the United States. Alcohol Research : Current Reviews. 40(2), 01 (2020). [↩]
- S. Seedat, K. M. Scott, M. C. Angermeyer, P. Berglund, E. J. Bromet, T. S. Brugha, K. Demyttenaere, G. de Girolamo, J. M. Haro, R. Jin, E. G. Karam, V. Kovess-Masfety, D. Levinson, M. E. Medina Mora, Y. Ono, J. Ormel, B. E. Pennell, J. Posada-Villa, N. A. Sampson, D. Williams, R. C. Kessler. Cross-national associations between gender and mental disorders in the World Health Organization World Mental Health Surveys. Archives of General Psychiatry. 66(7), 785–795 (2009). [↩]
- A. A. Alvanzo, C. L. Storr, R. Mojtabai, K. M. Green, L. R. Pacek, L. N. La Flair, B. A. Cullen, & R. M. Crum. Gender and race/ethnicity differences for initiation of alcohol-related service use among persons with alcohol dependence. Drug and Alcohol Dependence. 140, 48–55 (2014). [↩]
- H. Kim & E. R. Duval. Social interaction anxiety and depression symptoms are differentially related in men and women. Current Psychology. 42, 22526–22537 (2022). [↩]
- S. F. Greenfield, A. J. Brooks, S. M. Gordon, C. A. Green, F. Kropp, R. K. McHugh, M. Lincoln, D. Hien, & G. M. Miele. Substance Abuse Treatment Entry, Retention, and Outcome in Women: A Review of the Literature. Drug and Alcohol Dependence. 86(1), 1–21 (2007). [↩]
- S. Heidari, T. F. Babor, P. De Castro, S. Tort, & M. Curno. Sex and Gender Equity in Research: rationale for the SAGER guidelines and recommended use. Research Integrity and Peer Review. 1(2), (2016). [↩]
- J. G. Regensteiner & K. Templeton. Review of the Influences of Sex Differences on Health and Disease: What Is the Role of Journals?. The Journal of Bone and Joint Surgery: American Volume. 106(19), 1809–1813 (2024). [↩]
- N. Kokras, & C. Dalla. Sex differences in animal models of psychiatric disorders. British Journal of Pharmacology. 171(20), 4595-4619 (2014). [↩]


 and Fluoroform (CHF3) using Molecular Dynamics")
{kind=link}