
Abstract
Vaccines have been a crucial part of public health for hundreds of years and have significantly reduced the fatalities from infectious diseases over time. With rapid advancements in vaccine technology, the challenge of equitable global distribution has become more important, especially for low-income countries. This paper examines the history of vaccines, from early methods to modern strategies such as mRNA and nanoparticle vaccines, highlighting the prominence of evolving immunization forms. It also explores essential organizations involved in vaccine development and distribution, such as the World Health Organization, and it compares the responses from around the world of the eradication of smallpox and the COVID-19 pandemic. The smallpox eradication was a relative success because of targeted strategies and more advantageous characteristics of the virus. Comparatively, the COVID-19 pandemic exposed weaknesses in global vaccine distribution, including the inequalities between high and low-income nations. This paper supports the prioritization of reliable, cost-effective vaccines, stronger international coordination, and better pandemic preparedness to ensure equal access globally in future health emergencies. By taking care of these challenges, global health systems can ensure vaccine accessibility to prevent inequalities later.
Keywords: vaccine distribution, vaccine history, health, vaccine advancements
Introduction
Vaccines have played a significant role for hundreds of years by preventing the spread of dangerous illnesses throughout history. The path from early techniques to modern technology used today signifies the obstacles and successes that humans have been through to fight diseases. Before the development of vaccines, infectious diseases were the main cause of death globally1. Starting with the variolation in the 16th century, scientists have continued to improve vaccination methods, leading to the eradication of smallpox and COVID-19 vaccines being created with groundbreaking speed2. The evolution of vaccination methods includes milestones such as the first smallpox vaccine technique created by Edward Jenner, Louis Pasteur’s rabies vaccine, Salk’s polio vaccine and newer mRNA vaccines1. Each advancement has contributed to the development of the science of vaccination, positively impacting global health.
Vaccine technology is still advancing rapidly, which proves the importance of continuing research in vaccinology. Presently, there are many types of vaccines, and many more forms and types are in the process of being developed. Some reliable vaccine types today are the live attenuated, inactivated, and the recombinant protein vaccine. A few newer methods include the mRNA, nanoparticle, and viral vector vaccine. There are also different forms of immunization emerging, like combined vaccines and transdermal patches3.
Because of the speed at which vaccine discoveries are being made, the global distribution of vaccines is increasingly crucial for swift response in future pandemics and resisting dangerous viruses. Allocating vaccines around the world properly is difficult, especially in low-income countries that do not have sufficient resources4. There are many other obstacles: geographically rough areas, countries overconsuming vaccines from limited supply, and the high cost of newer vaccines. The COVID-19 pandemic and the smallpox eradication are examples that show the depth of these considerations.
Different health groups like the WHO and CDC have played large roles in these events, and they continue to be of extreme significance to vaccination policies, especially because forms of vaccine distribution are underdeveloped now, and they can be developed to be more efficient and simpler to handle. The evolution of vaccine technology, from early methods like vaiolation to recent advancements such as combination vaccines, has largely progressed global health. However, to ensure the effectiveness of these innovations, it is crucial to address the challenges of global vaccine distribution to prepare for future pandemics and improve global immunity.
Methodology
This literature review explores the vast history of vaccines, organizations involving vaccination, and different examples and struggles of vaccine distribution. The goal was to gain a nuanced understanding of the evolution of vaccines, the institutional efforts that support widespread immunization, and the barriers to fair vaccine distribution. To gather the relevant sources, the PubMed database was used. The keywords “vaccine distribution, “vaccine advancement”, “global health organizations”, and “challenges of vaccination”, “vaccination rates”, and “public health in low-income countries” were used to ensure focused results. The search was limited to peer-reviewed articles published from 2002 to the present.
Articles were selected based on their connection to main parts of the review: historical breakthrough in vaccine development, the influence of health organizations such as the World Health Organization (WHO) and Centers for Disease Control and Prevention (CDC), and real- world case studies highlighting vaccine important to compare because smallpox represents an earlier era of vaccines while COVID-19 accessibility, distribution inequities, and public health infrastructure, specifically COVID-19 and the smallpox pandemic. Both time periods displays the impact of modern technology on vaccination. Also, smallpox had a slow campaign, but it was ultimately successful, and coronavirus had rapid vaccine development with inequalities in distribution. Comparing and contrasting these two cases provides the best and clearest lens through which to observe how vaccine science has evolved, how global cooperation has transformed, and what obstacles remain in achieving widespread public health goals.
Vaccine History
There are many significant moments around vaccinology in the past. One of the first recorded forms of vaccination was in China during the 16th century, named variolation. This practice arose with smallpox, which is characterized by a fever and a rash that develops into pus-filled blisters. Smallpox spreads through direct contact with infected people or objects that have been contaminated. There were three main ways of variolation as written by Chinese physician Lu. The first included putting a piece of cotton soaked in the pus from smallpox blisters into the nose, the second was breathing in dry scabs, and the last one was wearing an infected person’s clothes1. In India, people were injected with smallpox material through the skin, called cutaneous inoculation1. Some risks involving variolation included the possibility of severe smallpox and even death1. 0.5-3% of those who were variolated died, as opposed to 9.5-30% of people naturally dying from the infection1. Although variolation did not have a high rate of success, it still had significantly better odds than getting smallpox without any form of protection.
Variolation was the starting point for many strong vaccines in the future. Smallpox had a death toll of over 300 million people. Thus, any sort of protection was considered better than no protection for most people during that time. Eventually, this popular method started spreading to other countries. The wife of a British diplomat, Lady Montague, discovered people using variolation in Constantinople and then introduced and advocated for the idea in England1.
In 1796, Edward Jenner developed a better source of protection after studying variolation. He discovered that cowpox could be used to protect people against smallpox, so he experimented by taking a lesion from an infected milkmaid and inoculating a boy1. This method ended up being a success, and this was a large advancement in protecting people from death by disease.
Thanks to variolation and Edward Jenner’s discovery, the creation of vaccines was inevitable. In the 1880s, Louis Pasteur developed the first rabies vaccine, which was another huge step in vaccinology, although he had barely any knowledge of the biological processes of animals or humans1. In the 1930s, vaccine development became more scientific based because the electron microscope was invented1. Jonas Salk was able to develop the polio vaccine in 1955. Many researchers helped to expand knowledge involving using dead bacteria in vaccines and the relationship between antibodies and antigens. Antigens can be any substance that triggers an immune response, which leads to the production of antibodies. Later, one of the most powerful moments in vaccination was the eradication of smallpox by the WHO in 1980. It was the first human infectious disease to be eradicated globally5. Later that decade, scientists started to create the first HPV vaccine, and it became a success in 2007 when VLP vaccines were approved in many countries including the United States6.
A recent event where vaccinology was put to the test was COVID-19. 2019 and 2020 were vulnerable years worldwide, and those years showcased how far vaccine technology has come since the very beginnings of variolation. A variety of vaccines were created in record time because of the preexisting knowledge, and one of the most ingenious and new technologies among them was a vaccine platform based on mRNA1.
The Common Types of Vaccines
There are several vaccine modalities currently available. Each vaccine is made to induce a safe immune response for next time, in case the virus infects the body. Three older vaccine types are the live attenuated, inactivated, and the recombinant protein vaccines. The live attenuated vaccine is one of the oldest vaccines, and there are many ways to create it. One of which consists of pathogens from the virus that have been weakened through heat radiation or with chemicals, like formalin7. The pathogens can also be weakened through the process of passage through different cell types, called serial passage in cell culture. Repetition causes the virus to weaken because it mutates many times, causing it to become less potent than it originally was. Because of the live pathogens inside it, a light infection can be produced without the harmful disease. This causes immunity and long-lasting protection after only one injection. Although these vaccines usually need to be refrigerated, there is also a risk of the vaccine reverting to the dangerous virus strain, which would cause disease7. This would be especially dangerous to the immunocompromised.
The inactivated virus vaccine is created by treating the virus with radiation and chemicals, like formaldehyde. This destroys the virus and its ability to replicate and cause disease. The particles still carry antigens, which the immune system can recognize and trigger an immune response in return. This is a very safe vaccine because it cannot cause disease, but one might need to receive booster shots for it to help maintain immunity.
The recombinant protein type is created by using recombinant pieces of the pathogen’s genetic code to produce a protein or an antigenic component from the virus. The gene encoding the protein selected is cloned into a vector, which is introduced into host cells that can express the gene. The cells then begin to produce the protein, which is later formulated into vaccines. Once injected, antibodies are produced, and T cells are activated that can respond to antigens. These vaccines are very specific and only target certain parts of a pathogen, and this reduces the risks of dangerous reactions compared to vaccines made with whole pathogens.
Three prominent new types are the mRNA, nanoparticle, and viral vector vaccine. The mRNA vaccine is made by identifying a specific protein from the pathogen that is known to induce an immune response. The protein’s mRNA sequence is made synthetically, and the protein can be recreated using the code. The vaccine can enter a cell as it is encapsulated by a lipid nanoparticle, a coating of fat that allows the contained RNA to go directly into the cytoplasm of the cell for further translation. A large quantity of mRNA vaccines can be produced rapidly; however, they need to be stored at very cold temperatures, and multiple doses are required7. They also have particular thawing processes that they have to go through before usage8. They can be produced quickly, and they are easier to manufacture, but they are sold for more than other types of vaccines9.
Another newly popular vaccine platform is nanoparticles. This is when a particle based on proteins is created with the viral antigen of interest displayed on the nanoparticle. This platform is created to resemble the nature of a virus. This makes nanoparticles effective because they are more similar to the virus than some of the older vaccine types. The immune response is induced to be directed to the viral antigen of interest that is displayed on the nanoparticle. For a nanoparticle vaccine, a protein complex is created to resemble the real virus, but this particle doe not have DNA or RNA, rendering it a non-infectious ball of protein that can stimulate the immune system. This platform cannot replicate inside the body since it has no nucleic acid, which means that it cannot become dangerous. This vaccine has a more advanced antigen presentation, so the immune system is more likely to recognize it to be harmful and attack10.
For the viral vector vaccine, another virus is created that is different and less harmful than the original virus. This new virus also cannot replicate and become threatening to the body. It is modified to include a piece of genetic material from the original virus, usually protein. The virus utilizes the cell’s transcriptional machinery to produce replicated viral protein. This way, an immune response is generated, and memory cells can be produced. The viral vector vaccine guarantees an immune response, but the side effects, like a cold, could be debilitating to people already with diseases such as cancer.
Recent Advancements in Vaccine Technology
Because vaccine knowledge is progressing quickly, new advancements are constantly being created. For example, some vaccines are being combined to condense the number of injections needed during routine vaccinations3. This is beneficial because people can be protected against more than one disease in one injection, and the costs of stocking and administration of separate vaccines are reduced. An additional option to reduce costs of production is plant-based vaccines; plants can be grown on a large scale in greenhouses easily11.
Personalized vaccines are also a newer idea. Researchers can evaluate an individual’s genetic profile and predict their response to different vaccines and how many doses they could need. These vaccines are highly specific and can target certain areas of one’s genetic profile. They can also be a preventive approach. Another instance of growth includes new ways to give vaccines other than via injection. Some vaccines, including a live attenuated influenza vaccine, are being given through the nose3. This helps immunize the upper airway, matches the normal path of infection, and is easy to administer by oneself12. This form is still very new and has not been perfected yet.
Another recent discovery of vaccines is transdermal, with patches with adjuvants and microneedles that deliver antigens across the skin3. This method would induce enhanced immunity due to delayed antigen release along with being easier to administer to people with a phobia of needles13.
A different alternative that is being worked on is the growth of adjuvants, which are substances in vaccines that enhance the body’s immune response to antigens. New ones are being developed to potentially reduce the antigens needed per dose and to provide protection against many types of pathogens at once. Even though all these forms of vaccination are relatively new, they could revolutionize the future of immunization.
Organizations in Vaccine Design and Distribution
Many important organizations around the world are involved with vaccines in different ways. Some significant groups include the World Health Organization, the National Institutes of Health, the Center for Disease Control and Prevention, and the Food and Drug Administration. Three of these are US-based. All of these institutions have different roles in the vaccination process and many other roles in international health.
The WHO is a global group of the United Nations that develops policies and guidelines for many health issues. The group also leads international efforts for health emergencies by sending experts and supplies to places in need. Universal health coverage is a huge goal of this organization. In vaccination, the WHO strives for global access to vaccines and immunization programs. It helps enforce different immunization strategies around the world, especially in poor countries that need more assistance. To do this, the WHO collaborates with many governments and other international groups.
The NIH conducts research in many areas of health like specific diseases, current health needs, and public health challenges. The NIH also funds research, including vaccine studies, at different institutions and supports training programs for the next generations of health professionals. Because of this, the NIH has to coordinate with researchers and other institutions to address different obstacles in health. This organization is very significant in vaccine advancement because it conducts research on vaccine development and develops clinical trials to create vaccines. The NIH also creates guidelines surrounding the protocols of every step of vaccine production.
Next, the CDC is a key agency in the U.S. for public health. The agency’s main roles include tracking the spread of diseases and their trends, campaigns promoting healthy behaviors, epidemiological research, and analyzing a variety of statistics encompassing health. The CDC creates immunization schedules for different age groups and issues rules for vaccine administration. In case of a disease outbreak, this group can provide support to help control it. The CDC communicates with the states and also works together with international organizations.
Lastly, the FDA ensures the safety of a variety of products by reviewing them to protect the public, including food, medical devices, cosmetics, and tobacco products. Their main role is to supervise a large range of goods and make sure they meet certain standards. It also conducts its research in medical science and responds to health emergencies. This group also has a responsibility for vaccination because it inspects vaccines and approves them before they can be put on the market. The FDA also responds to disease outbreaks by making sure necessary treatments, like vaccines, are available and efficient. All of these institutions have many significant roles, especially in vaccination. Vaccines are a very complex product, and this is why many people in many different groups are required.
Smallpox Eradication vs. COVID-19 Vaccination
| Factor | COVID-19 | Smallpox |
|---|---|---|
| Virus Characteristics | Caused by SARS-CoV-2, RNA virus; spreads through respiratory droplets and aerosols; many variants | Caused by Variola virus; DNA virus; spreads via droplets and contact; no animal reservoir |
| Vaccine Properties | Multiple vaccines (mRNA, viral vector, inactivated); varying efficacy; requires 1–3 doses plus boosters; rapid development (under 1 year). | Live attenuated vaccine; high efficacy (≈95–100%); single dose; long-term immunity; developed pre-1950s. |
| Distribution Infrastructure | Massive global logistics required; cold chain essential (esp. for mRNA); various manufacturers | Simpler logistics; no ultra-cold storage needed; fewer manufacturers (centralized) |
| Governance Mechanisms | Mixed global response; WHO coordination (COVAX); national strategies varied; politics and anti-vaccine movements played role | WHO-led global eradication program; strong international collaboration; standardized strategies; high cooperation |
| Socio-Political Contexts | Highly polarized in many countries; misinformation via social media; inequalities in vaccine access | Mid–late 20th century global cooperation; less political resistance; less media-driven misinformation. |
Smallpox was officially eradicated in 1980. The smallpox eradication was very successful due to its campaign and the advantages surrounding the virus. Before eradication, this disease killed over 300 million individuals around the world5. This virus was destroyed by the WHO, except for samples kept in the United States and Russia. There were a few advantages in dealing with smallpox. First, it was easily identifiable due to its symptoms, the virus was transmitted slowly, and its vaccine was highly effective14. Also, smallpox had no animal reservoirs, meaning that it could not live and multiply in animals. This was a large factor in the success of its eradication.
In 1958, the Soviets approved a proposal for smallpox eradication15. The WHO was already deeply involved in a program to get rid of malaria but slowly switched gears by joining the smallpox campaign after the malaria program fell apart15. The United States did not align itself with the WHO’s plan until 1967 due to changes in foreign policy. Eventually, the U.S. helped lead the agenda along with the Soviet Union, which came to be known as the Intensified Smallpox Eradication Program15. It fully succeeded in 1980 because the WHO had a platform that allowed it to be international.
The last natural outbreak was in Africa. This campaign used a strategy called ring vaccination to finally and completely eradicate smallpox. This method’s first step was identifying the infected people and those who have come into contact with them. Then, the people who were in contact with them were vaccinated, which caused a ring of immunity around the outbreak. Overall, the teamwork and clever strategies of this campaign along with the few advantages like the strong vaccine, and the eradication of smallpox were very successful.
COVID-19 was dealt with differently because of various circumstances. This virus was discovered in 2019 and caused a global pandemic. COVID-19 caused the world to experience much distress4. Significant pressures were placed on supply chains because billions of vaccines needed to be produced for people to be fully vaccinated around the world. This disease mainly spreads through respiratory droplets from coughing or sneezing. Symptoms of COVID-19 can range from mild to severe, from a fever and cough to pneumonia. Preventive methods include wearing masks and social distancing.
Vaccines were developed in record time due to new technology, but there were a variety of problems with distributing them to every country. The vaccination rate in countries like China and Australia was high because of the abundance of vaccines, which many other nations did not have4. High-income countries paid billions of dollars to acquire and create vaccines, which means that they were unfairly allocated to low-income countries because they could not afford to purchase vaccines4.
COVAX was an initiative founded that aimed to help poorer countries with vaccine availability. However, due to the wealthy countries preordering most of the vaccines, a lot of low-income countries had a disadvantage because most of their populations could not be vaccinated. This demonstrates the chaos surrounding international vaccine distribution. Another challenge included the difficult geography of many countries because vaccination camps could not be set up. Also, many of the vaccines must be kept at a certain temperature to remain stable, but multiple countries did not have the right refrigeration technology.
Lastly, there was the issue of vaccine hesitancy. False social media posts negatively impacted people’s perspectives on the COVID-19 vaccine, leading to more skepticism surrounding it. Even though coronavirus showed how far vaccine technology has come, it also revealed some weaknesses of the governments and organizations around the world.
The smallpox eradication and the COVID-19 pandemic were very different events because they both had their own respective action plans, and the viruses are also distinct. Smallpox had visible symptoms, but COVID-19 usually has respiratory symptoms. Smallpox has no animal reservoirs, whereas COVID-19 can have some, like pets or farm animals. In this particular aspect, coronavirus is harder to eradicate than smallpox, and there are other factors to take into account. Also, smallpox had an effective vaccine because the virus did not change. COVID-19 has highly effective vaccines, but it is more challenging because the virus has more variability, meaning it can mutate quickly. Boosters are recommended for this vaccine. Smallpox had been present in the world for a long time when it was finally eradicated, but COVID-19 recently appeared. These are the main disparities between these viruses’ modern situations. The smallpox eradication was handled more efficiently because of these factors and the slow, but successful campaign.
COVID-19 Vaccination Rate
Vaccination needs government and public support to be successful in protecting people from widespread infectious diseases. Some high-income countries have invested in vaccination efforts to try and prevent the spread of viruses beyond their country, but these investments were not been universally successful. However, they have been able to vaccinate their own countries in record time during COVID-19 while low-income countries barely reached 10% of their population vaccinated.
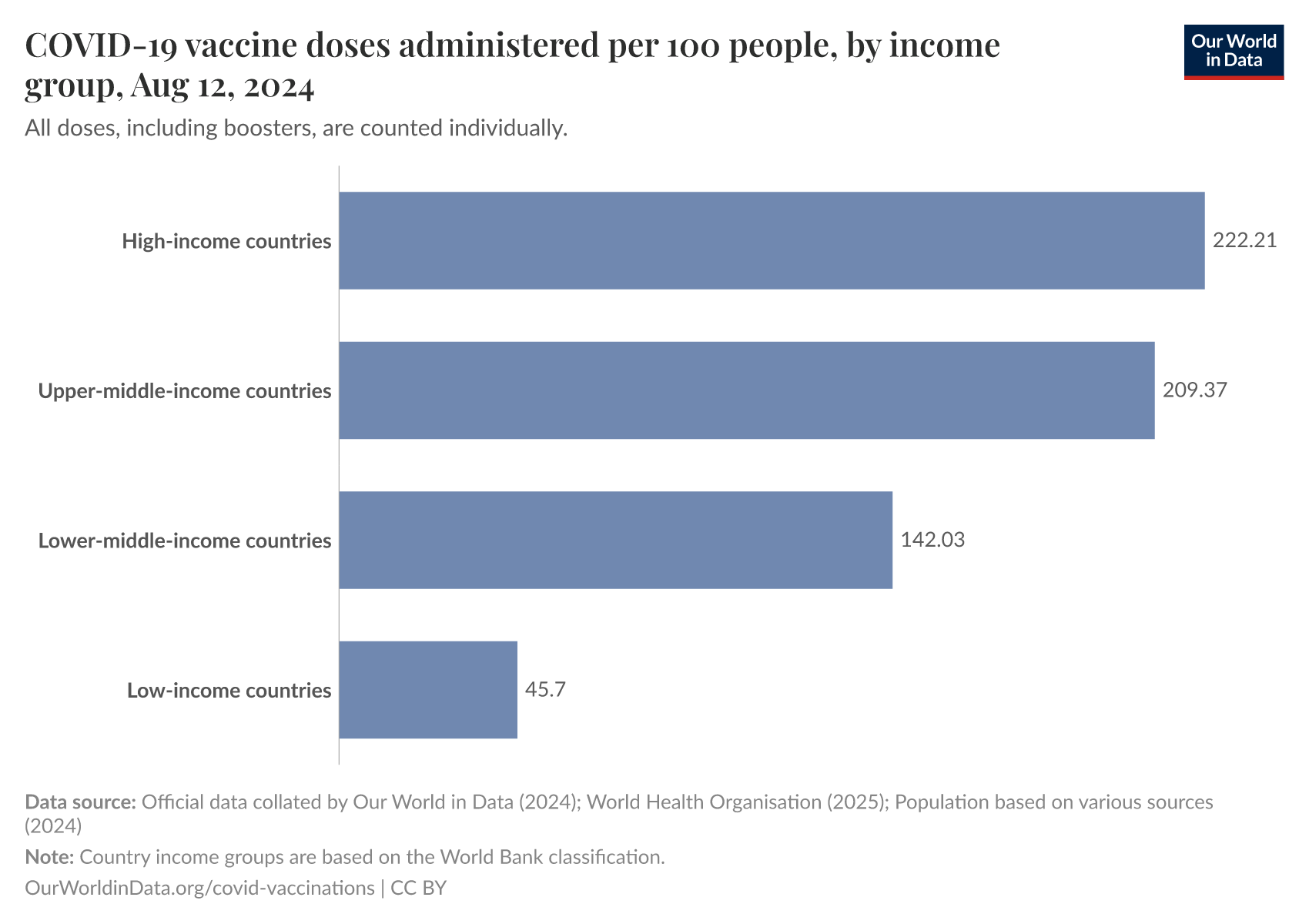
This graph shows the COVID-19 vaccine doses administered per 100 people categorized by the country’s income group. As pictured, the countries with the highest income had 233,77 doses administered per 100 people as of August 12, 2024, while the countries with the lowest income only had 45.7 doses administered per 100 people as of August 12, 2024. This shows the correlation between the country’s income group and how many people within that country are successful in becoming vaccinated. The largest amount of vaccinated people belongs to the high-income countries while the smallest amount of vaccinated people belongs to the low-incomes countries. The disparity found in this graph demonstrates the need to make vaccines accessible for everyone.
Other Obstacles in Vaccination
There are many factors to the vaccination rates in each country besides the wealth of a country; some of the most significant ones include politics and public opinion. There has always been
vaccine hesitancy starting from the days of Jenner’s smallpox vaccine, but it was especially present during COVID-19 due to the heavy impact of political division in public health States republican leaning counties have generally suffered higher death rates from COVID-19 due to some republican leaders downplaying the risks of the virus and the importance of Vaccination16. People who have declared that they are Democrats are significantly more likely to receive vaccinations than those who belong to radical parties or do not feel close to any party at all17.
A significant event that sparked the anti-vaccination movement was a faulty article being published about the MMR vaccine causing autism16. The movement developed through the usage of social media on apps such as Facebook, and more recently, TikTok18. This skepticism grew during the coronavirus pandemic, especially because some vaccines were developed in record times. Some people thought the vaccines were rushed and too new, and many wanted to wait until the vaccines were proven to be safe and effective19. Over time, more may be willing to receive COVID-19 vaccines because they are more likely to be perfected and trusted.
There are also some disparities with vaccine acceptance between various races, different income groups and age groups. African Americans had higher skepticism compared to others about the flu and influenza vaccines17‘20. In a 2016 national U.S. survey, White adults were the most likely unemployed people and those with lower incomes have a lower vaccine acceptance rate. However, other studies were unable to conclude that there is a clear association between economic status and vaccine hesitancy. Because of this, there is no general consensus on income level affecting vaccine acceptance17. The 19-30 years old age group were the least likely to respond that they would get the flu vaccine. As the age went up, people were more likely to accept vaccination.
Discussion
The COVID-19 pandemic displayed large flaws in global vaccine distribution, accessibility, and action plans, which demonstrated the need for a more efficient strategy for future pandemics. One way is to prioritize the use of reliable, older vaccines, which have proven their efficiency in manufacturing21. These vaccines generally do not require restricting temperature controls, making them simpler to distribute internationally, especially in nations with limited resources.
Additionally, they are less costly to manufacture and purchase, providing a cost-effective solution that would be very beneficial to lower-income countries. This approach could reduce the inequalities seen during the world’s most recent pandemic because the more expensive vaccines with newer technologies were only suited for wealthier countries. Vaccines made with mRNA are an example because while they are innovative, they are costly and require certain storage conditions. This vaccine type increased the financial and logistical burdens globally during COVID-19, especially in developing countries. Comparatively, established vaccine types, with decades of research and use behind them, could serve as a more reliable option in future pandemics. Using older vaccines would take pressure off global supply chains to globally provide enough new vaccines with vials, syringes, and stabilizing agents21.
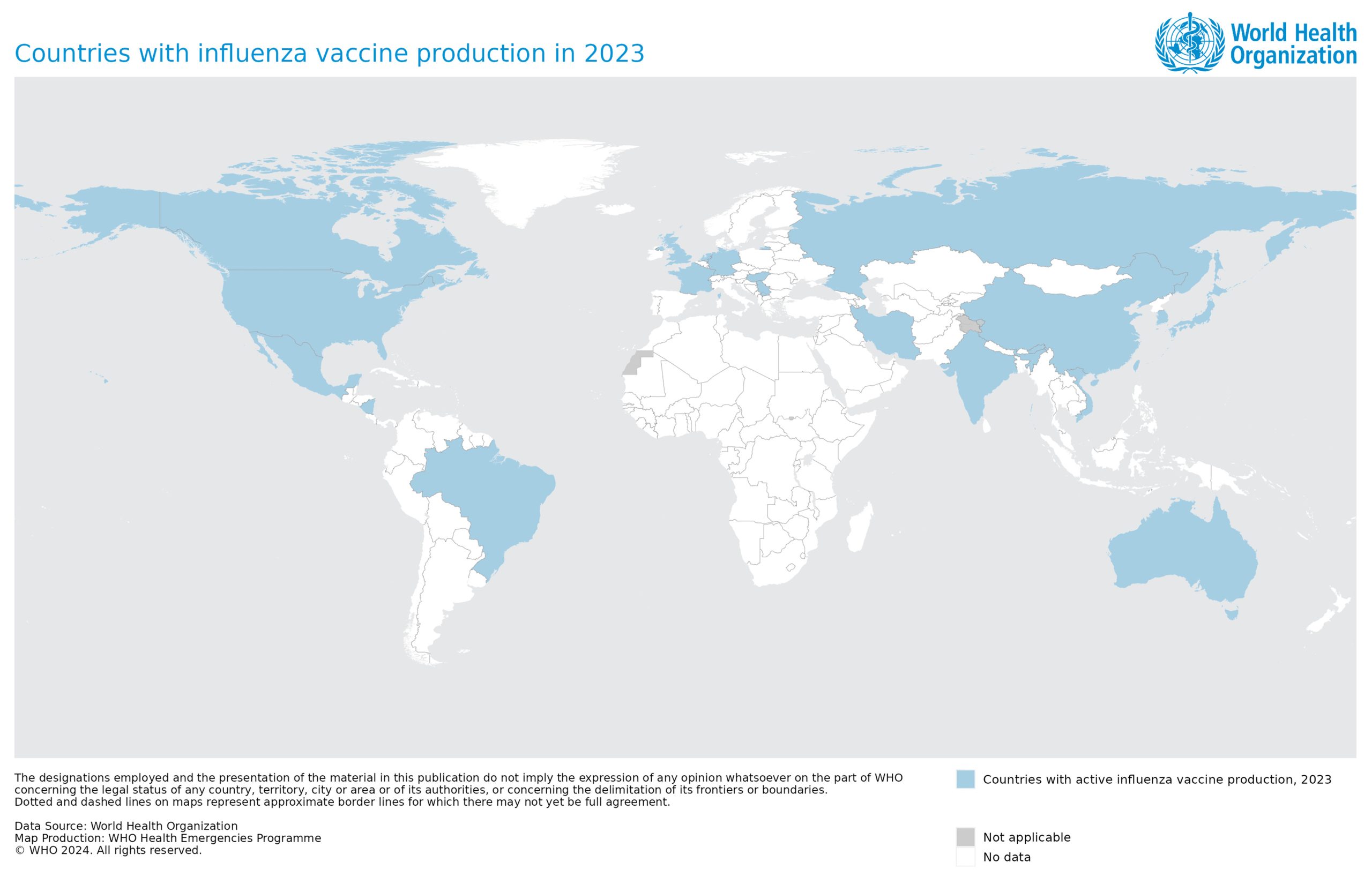
Source: World Health Organization
This graph displays the countries that have full influenza vaccine production in 2023: United States, Mexico, Brazil, Argentina, United Kingdom, France, Germany, Italy, Netherlands, Belgium Hungary, Russia, China, India, Japan, South Korea, Thailand, Vietnam, Kazakhstan, Indonesia and Australia. Only 22 out of 195 countries have full influenza vaccine production capabilities as of 2023, which shows that vaccine production still has a room to develop. Almost half of these countries were present in the 50 richest countries in the world based on GDP per capita in 2023, according to Worlddata.info. Low-income countries also took months longer than middle and high-income countries to distribute enough vaccines to cover their 65+ population22. This contributes to the fact that wealthier countries generally have more vaccination capabilities. The net cost of vaccination includes capital, staff, and vaccine substance, which some countries may not be able to afford9. Because of the disparity, there should be an improved way for higher income countries to work with lower income countries.
To ensure fair distribution and effective vaccination campaigns, strong international collaboration is critical. Representatives from strong health organizations, such as the WHO or the CDC, could be dispatched to assist weaker, poorer countries that have minimal resources to encourage and administer vaccines23. These experts could provide guidance, training, and resources to help these countries implement successful vaccination plans that are tailored to their specific needs and obstacles. An already existing example that is similar to this idea is China, which supplied vaccines to 110 countries during COVID-1923. Another significant aspect is managing vaccine supply to prevent the hoarding seen in relatively wealthy countries during the influenza pandemic in 2009 and even during COVID-1921. There was already a scarce number of vaccines, and the demand of doses exceeded it23. While many wealthier nations ordered excessive vaccine doses, many poorer countries were left with inadequate supplies for their population, worsening the obstacles in vaccine distribution.
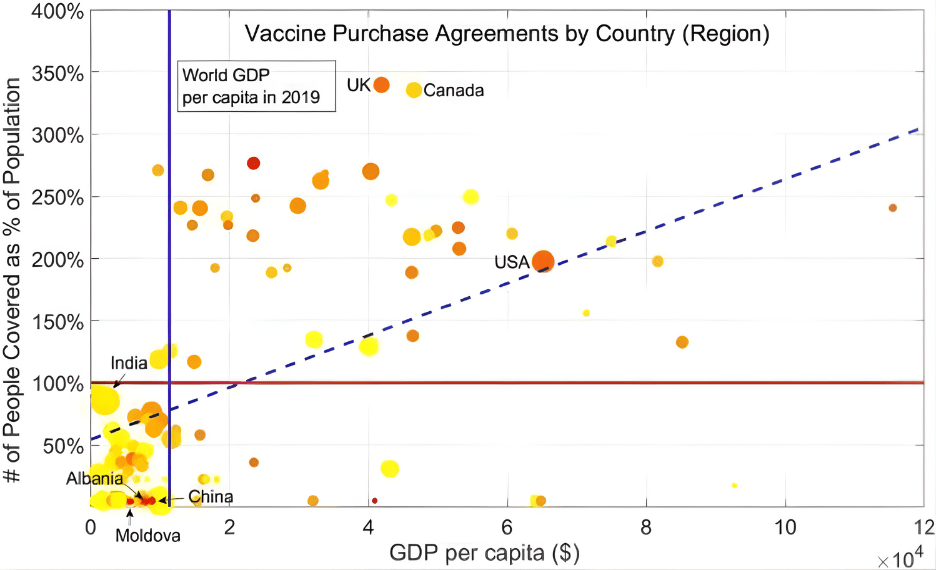
Source: Bloomberg and World Bank data
Scarce resources to vaccinate their citizens24. The United States bought enough doses to
This graph displays wealthier countries (based on GDP per capita) like the United States and Canada purchasing excessive vaccines for their population sizes. The hoarding of vaccines by countries like these takes a toll on other poorer countries like Albania because it leaves them with vaccinate more than three times its population, while Albania could only buy enough to vaccinate about 5% of its population24.
COVAX attempted to fix this issue by allowing lower income countries to purchase vaccines at lower prices, and all countries would be unable to purchase more than 20% of their population. However, this would need a substantial amount of funding, and some nations would find other ways to obtain vaccines that would harm the supply that COVAX has21. Keeping track of the number of vaccines a country has bought overall from various companies and putting in place a cap on the quantity of vaccines any country can order based on their population size and needs could lead to a more equitable distribution globally.
Also, preparation for future pandemics should be a global priority. Studies have shown that the effectiveness of vaccines varies based on geographical areas, making it harder to come up with one simple solution25. Lower and higher income nations could meet regularly, bringing together their leading health organizations to discuss these differences and develop the best methods to deal with potential pandemics. This collaboration would allow for the sharing of resources and knowledge, which would ensure that every nation will always be prepared to respond quickly and effectively to a future health crisis. By learning from the obstacles faced during the COVID-19 pandemic, the international community can build a better global health system that is capable of protecting everyone, no matter where they are from.
On a social perspective, trust in healthcare providers over politicians should be restored to combat the increase in vaccine hesitancy in different countries18. In places like the United States that have deeply divided political parties, it may be more complicated to join forces to protect citizens due to fundamental disagreements. However, this could possibly be a viable solution in other places where political parties have more overlap and are willing to work together to ensure vaccination health.
Conclusion
Vaccines are extremely important to the world and have been for a long time. Vaccines’ extensive history around the world has led vaccine technology to where it is today, advanced and progressing at breakneck speed. The variety of vaccines, including the six previously mentioned, is proof of the many trials and errors across history and the successes being reached today. For instance, the meaningful accomplishment of smallpox eradication showcased the strengths of health systems around the world can have. The COVID-19 pandemic showed some of the weaknesses with vaccine distribution that could be worked on in the future.
As vaccine technology is rapidly progressing, the challenge of global allocation of vaccines is also becoming more significant, as shown during the coronavirus pandemic. Because they contribute to international health security and many other issues, vaccines are substantial to humans. Although, all of their many benefits go to waste if they cannot be properly distributed to people. This is why more effective strategies, like using cheaper, more experienced vaccine types, need to be discussed and agreed upon for implementation in future pandemics. Global cooperation is important and every nation should be aware of that in order to successfully allocate vaccines. By addressing these challenges, the world can create a stronger global health system prepared for future threats. All in all, vaccines are becoming more meaningful every day, and they should be accessible for everyone to utilize for their health.
References
- Montero, David A., et al. “Two centuries of vaccination: historical and conceptual approach and future perspectives.” Frontiers in public health 11 (2024): 1326154. [↩] [↩] [↩] [↩] [↩] [↩] [↩] [↩] [↩] [↩] [↩]
- Kantarcioglu, Bulent, et al. “An update on the status of vaccine development for SARS- CoV-2 including variants. Practical considerations for COVID-19 special populations.” Clinical and Applied Thrombosis/Hemostasis 28 (2022): 10760296211056648. [↩]
- Plotkin, Stanley A. “Vaccines: past, present and future.” Nature medicine 11.Suppl 4 (2005): S5-S11. [↩] [↩] [↩] [↩]
- Yarlagadda, Harshani, et al. “COVID-19 vaccine challenges in developing and developed countries.” Cureus 14.4, 2022 [↩] [↩] [↩] [↩]
- Simonsen, Kari A., and Jessica Snowden. “Smallpox.” (2017). [↩] [↩]
- Frazer, Ian H. “The HPV vaccine story.” ACS Pharmacology & Translational Science 2.3 (2019): 210-212. [↩]
- Gupta, Sonal, and Sabine Pellett. “Recent developments in vaccine design: from live vaccines to recombinant toxin vaccines.” Toxins 15.9 (2023): 563. [↩] [↩] [↩]
- Yarnoff, Benjamin, et al. “Time and cost of administering COVID-19 mRNA vaccines in the United States.” Human Vaccines & Immunotherapeutics 17.11 (2021): 3871-3875. [↩]
- Light, Donald W., and Joel Lexchin. “The costs of coronavirus vaccines and their pricing.” Journal of the Royal Society of Medicine 114.11 (2021): 502-504. [↩] [↩]
- Bezbaruah, Rajashri, et al. “Nanoparticle-based delivery systems for vaccines.” Vaccines 10.11 (2022): 1946. [↩]
- Venkataraman, Srividhya, et al. “Combating human viral diseases: will plant-based vaccines be the answer?.” Vaccines 9.7 (2021): 761. [↩]
- Chavda, Vivek P., et al. “Intranasal vaccines for SARS-CoV-2: From challenges to potential in COVID-19 management.” Drug discovery today 26.11 (2021): 2619-2636. [↩]
- Lee, Michelle S., Catherina X. Pan, and Vinod E. Nambudiri. “Transdermal approaches to vaccinations in the COVID-19 pandemic era.” Therapeutic Advances in Vaccines and Immunotherapy 9 (2021): 25151355211039073. [↩]
- Board on Health Promotion, and Disease Prevention. Scientific and Policy Considerations in Developing Smallpox Vaccination Options: A Workshop Report. National Academies Press, 2002. [↩]
- Bristol, Nellie. “Smallpox Eradication: A Model for Global Cooperation.” CSIS Blog 17 (2023). [↩] [↩] [↩]
- Albrecht, Don. “Vaccination, politics and COVID-19 impacts.” BMC public health 22.1 (2022): 96. [↩] [↩]
- Troiano, Gianmarco, and Alessandra Nardi. “Vaccine hesitancy in the era of COVID-19.” Public health 194 (2021): 245-251. [↩] [↩] [↩]
- Smith, Naomi, and Tim Graham. “Mapping the anti-vaccination movement on Facebook.” Information, Communication & Society 22.9 (2019): 1310-1327. [↩] [↩]
- Hammershaimb, E. Adrianne, James D. Campbell, and Sean T O’Leary. “Coronavirus disease-2019 vaccine hesitancy.” Pediatric Clinics of North America 70.2 (2022): 243. [↩]
- Kini, Aniket, et al. “Differences and disparities in seasonal influenza vaccine, acceptance, adverse reactions, and coverage by age, sex, gender, and race.” Vaccine 40.11 (2022): 1643- 1654. [↩]
- Wouters, Olivier J., et al. “Challenges in ensuring global access to COVID-19 vaccines: production, affordability, allocation, and deployment.” The Lancet 397.10278 (2021): 1023- 1034. [↩] [↩] [↩] [↩]
- Ferranna, Maddalena. “Causes and costs of global COVID-19 vaccine inequity.” Seminars in Immunopathology. Vol. 45. No. 4 Berlin/Heidelberg: Springer Berlin Heidelberg, 2024. [↩]
- Su, Yiqing, Yanyan Li, and Yanggui Liu. “Common demand vs. limited supply—how to serve the global fight against COVID-19 through proper supply of COVID-19 vaccines.” International Journal of Environmental Research and Public Health 19.3 (2022): 1339. [↩] [↩] [↩]
- Li, Zhehan, Jiajun Lu, and Jiamin Lv. “The inefficient and unjust global distribution of COVID-19 vaccines: from a perspective of critical global justice.” INQUIRY: The Journal of Health Care Organization, Provision, and Financing 58 (2021): 00469580211060992. [↩] [↩]
- Larkin, Andrew, et al. “How missing evidence-based medicine indicators can inform COVID-19 vaccine distribution policies: a scoping review and calculation of indicators from data in randomised controlled trials.” BMJ open 12.12 (2022): e063525. [↩]



{kind=link}