
Gregory Kozakov1, Alyssa Rowley1
1 Burlingame High School, California, USA
Abstract
Introduction: Musculoskeletal injuries represent one of the leading causes of morbidity among athletes. These injuries pose serious consequences for both performance and long-term health. Sex-based differences in injury patterns have become increasingly identified; however, the underlying biomechanical, physiological, and recovery-related mechanisms remain under-investigated and incompletely understood. This is specifically true in female athletes, as they are heavily underrepresented in sports medicine literature.
Methods: A literature review of existing research was conducted using PubMed and Google Scholar. Articles were included if they were published in reliable peer-reviewed journals between 2010 and 2025. Articles had to include reported sex-based injury rates, severity, or recovery in collegiate or professional athletes (exceptions were made for information that is critical to understanding), and analyzed one or more of the following sports: basketball, soccer, and/or volleyball. Studies focusing on non-athlete demographics, post-surgical outcomes without prior injury, or animals, were largely excluded.
Results: Lower extremity injuries predominated across all three sports examined. Basketball athletes primarily sustained ankle sprains (15-17% of all injuries), soccer players experienced high rates of hamstring strains (1.06 per 1,000 hours of exposure and 5.87 per 1,000 hours of exposure in training and competition, respectively), and volleyball athletes faced higher risk of patellar tendinopathy from repetitive jumping, as well as upper extremity injuries due to overhead play. Several sex-based disparities were observed: male athletes sustained higher overall injury rates, while female athletes sustained more severe injuries, particularly tears to the ACL which occurred at 2-4 times the rate of males. This was associated with biomechanical factors including greater knee valgus angles and altered landing mechanics. Evidence-based prevention strategies included neuromuscular training (associated with a reduction in ankle injury risk and a 45% reduction in ACL injuries) and eccentric hamstring exercises (associated with an 86% reduction in hamstring strain recurrence). Recovery factors such as adequate sleep (≥7 hours) and adequate nutrition, including collagen supplementation and sufficient vitamin D and calcium intake, were associated with improved musculoskeletal health. That said, direct athlete-specific intervention evidence remains limited.
Discussion: The findings in this review demonstrate the large need for sex-specific injury prevention systems in competitive sports. Female athletes remain less represented in research which limits the development of evidence-based interventions tailored to their unique physiological profiles. This is significant, as it catalyzes future research to prioritize certain standards: standardized methodology, inclusive study populations, and athlete-specific recovery intervention trials stratified by sex.
Keywords: Musculoskeletal injuries, Sex-based differences, Anterior cruciate ligament (ACL), Hamstring strain, Ankle sprain, Injury prevention, Neuromuscular training, Athlete recovery
Introduction
In the United States, collegiate and professional sports hold an important role in American culture and society. Sports not only provide entertainment to a large majority of the public, but they also generate substantial economic activity, providing careers for gifted athletes across leagues such as the National Basketball Association (NBA) and National Football League (NFL). As these leagues increase the pace of play, athletes are placed under greater physical demands: this includes extended playing times, as well as shorter recovery windows. Because of this, musculoskeletal injuries have become an increasingly prominent concern, as injury rates among collegiate and professional athletes continue to rise. In sports such as basketball, soccer, and volleyball, lower extremity injuries account for the majority of all reported injuries, representing a significant burden on athletes and medical teams. Moreover, each sport places distinct biomechanical demands on athletes. For example, basketball requires explosive lateral movement and frequent jumping; soccer involves constant movement, along with short periods of sprinting and directional changes; and volleyball demands repetitive overhead striking and constant jumping, similar to basketball. Each of these sport specific demands exposes athletes to unique injury profiles that differ across sports and between male and female competitors.
A growing body of research literature has identified sex-based differences in musculoskeletal injury patterns. While male athletes generally sustain injuries at higher overall rates, female athletes experience more severe injuries, most notably anterior cruciate ligament (ACL) tears, at rates two to four times higher than their male counterparts. These disparities in statistics have been attributed to differences in biomechanical factors such as greater knee valgus angles and altered landing mechanics in female athletes, as well as other anatomical differences that influence neuromuscular control. Recovery-related factors such as sleep quality, nutritional habits, and proper training load have emerged as important factors that modulate injury risk and musculoskeletal health, though the evidence base in athlete populations remains incipient.
Although several disparities have already been recognized, significant gaps in research and literature remain. First, research on female athletes is substantially underrepresented relative to the amount of research conducted on male athletes1. This imbalance ultimately inhibits the development of sex-specific, evidence-based injury prevention protocols and rehabilitation programs. Second, few reviews have utilized injury epidemiology across multiple team sports with factors related to recovery. This is significant because it makes it extremely difficult to draw comprehensive conclusions across multiple different sports. Finally, prevention strategies are often based on male athlete data, raising skepticism about their applicability and effectiveness in female athlete populations.
This literature review aims to address these gaps by combining and synthesizing existing evidence on injury patterns, biomechanical mechanisms, and recovery-related factors across three sports, namely basketball, soccer, and volleyball, while critically noting sex-based disparities. The first central objective of this review is to characterize and compare sport-specific injury epidemiology between male and female athletes. The second objective of this review is to identify the biomechanical and physiological mechanisms that underlie the sex-based disparities that were observed. The third objective is to evaluate the evidence for injury prevention strategies across both sexes. The fourth objective is to examine how recovery factors, including sleep and nutrition, may modulate musculoskeletal injury risk. This literature review hypothesizes that sex-based differences in injury patterns are driven by biomechanical, anatomical, and training-related factors. Moreover, recovery habits interact with said variables to further influence injury risk, an interaction that catalyzes further investigation in female athlete populations.
Methods
For this narrative review, two electronic databases, PubMed and Google Scholar were used. The search terms used included the following: (“sports injuries” OR “athlete injuries”) AND (“basketball” OR “soccer” OR “volleyball”) AND (“sex” OR “gender”). Additional search terms included “knee injuries”, “ankle sprains”, “ACL injury”, “anterior cruciate ligament”, “shoulder injuries”, patellar tendinopathy”, “tendinopathy”, “overuse injuries” and were applied individually or in combination to enhance search sensitivity. Furthermore, manual searches were conducted by reviewing the reference lists of identified studies to include additional relevant research.
Approximately 115 articles were screened for relevance. Articles that met the inclusion criteria were attempted to be retrieved in full text and were then reviewed for data extraction. Ultimately, 52 studies were included in this literature review. Inclusion criteria is as follows. First, articles needed to be published in reliable, peer-reviewed journals between 2010 and 2025. Second, articles needed to report sex-based injury rates, severity, or recovery in human subjects actively participating in amateur, collegiate, or professional sports. Third, articles needed to include statistical analysis of injury prevalence, biomechanical risk factors, or lifestyle and recovery influences. Fourth, articles needed to examine one or more of the following sports: basketball, soccer, or volleyball. Exceptions to the 2010-2025 publication window were made for a small number of foundational studies published prior to 2010 that are widely cited and central to understanding of injury epidemiology in these sports. Studies were excluded based on the following criteria: articles focused exclusively on a single sex without providing data that could be contextually compared to the opposite sex; articles centered solely on post-surgical outcomes or medical techniques without addressing injury prevention; articles involving non-athlete populations (military personnel were included, as they provided valuable information regarding sleep nutrition); animal studies (however, these were referenced for nutritional data and information).
The risk of publication bias should be acknowledged as a limitation of this literature review. Article searches were restricted to solely two databases, namely PubMed and Google Scholar, and grey literature, conference proceedings, and non-English publications were not screened. Because of this, studies with negative findings that may not have been shown in these databases could be severely underrepresented. Furthermore, no formal assessment of publication vias, such as funnel plot analysis, was performed, as this literature review is not meta-analytic in design. While these constraints are consistent with the scope and resources of a narrative/literature review, they limit the comprehensiveness of recorded evidence. While the PRISMA guidelines provide a valuable reporting framework, full PRISMA compliance is conventionally applied to systematic reviews and meta-analyses rather than narrative reviews. Nevertheless, the search strategy, screening process, and inclusion/exclusion criteria were designed to reflect the principles of PRISMA.
Basketball Injury Trends and Mechanisms
Multiple studies involving amateur and professional basketball players have identified lower extremity injuries, particularly those to the knee and ankle, as the most prevalent type of injury. For example, one study analyzing 318 athletes in Canada found that the greatest number of injuries resulting in more than seven sessions of time loss involved the knee, whereas the most common injuries causing fewer than seven sessions of time loss involved the ankle2. Another study recorded that ankle and knee injuries were among the most commonly reported and occurred at substantially higher rates during the actual games than the practices3. Similar findings show that lower extremity injury incidence rates are greater in athletes competing at higher levels4 and occur 3.7 times more often in games than in practice2. Studies of basketball trauma within the National Collegiate Athletic Association (NCAA) confirmed the lower extremity being the most commonly injured area of the body accounting for more than half of all injuries recorded between men and women during competition while the sprained ankle is the most common case of lower extremity trauma5. Despite the high overall incidence rate of ankle injuries, more than half of them are non-time-loss (NTL) with a slightly higher ratio of injuries in competitions than in practices5. It is important to note that not all studies report identical injury distributions. One analysis of National Basketball Association (NBA) injury surveillance data found that lower extremity injuries were less prevalent, with lower extremity stress fractures at 4.8 per year; meniscal tears at 2.3-3.3 per year; and ACL tears at 1.5-2.6 per year. Meanwhile, concussions occurred at a rate of 9.5-14.9 cases per year6. To clarify, these figures represent estimated absolute injury incidents per NBA season across the entire league, not rates per 1,000 athlete-exposures or per individual player. The statistics reflected the burden of each injury type across NBA teams per season and should be interpreted as league-level incidence counts, not individual athlete risk estimates. Stricter medical protocols may result in higher detection and reporting rates compared to other levels of basketball. Other factors to consider when analyzing injury statistics are reinjury rate and playing time. A study analyzing 10,393 participants found that athletes who had prior ankle injuries were nearly 5 times more likely to experience reinjury7. Finally, the highest injury rates were observed in athletes who had 30+ court time minutes per game8.
Sex-Based Disparities in Basketball Injuries
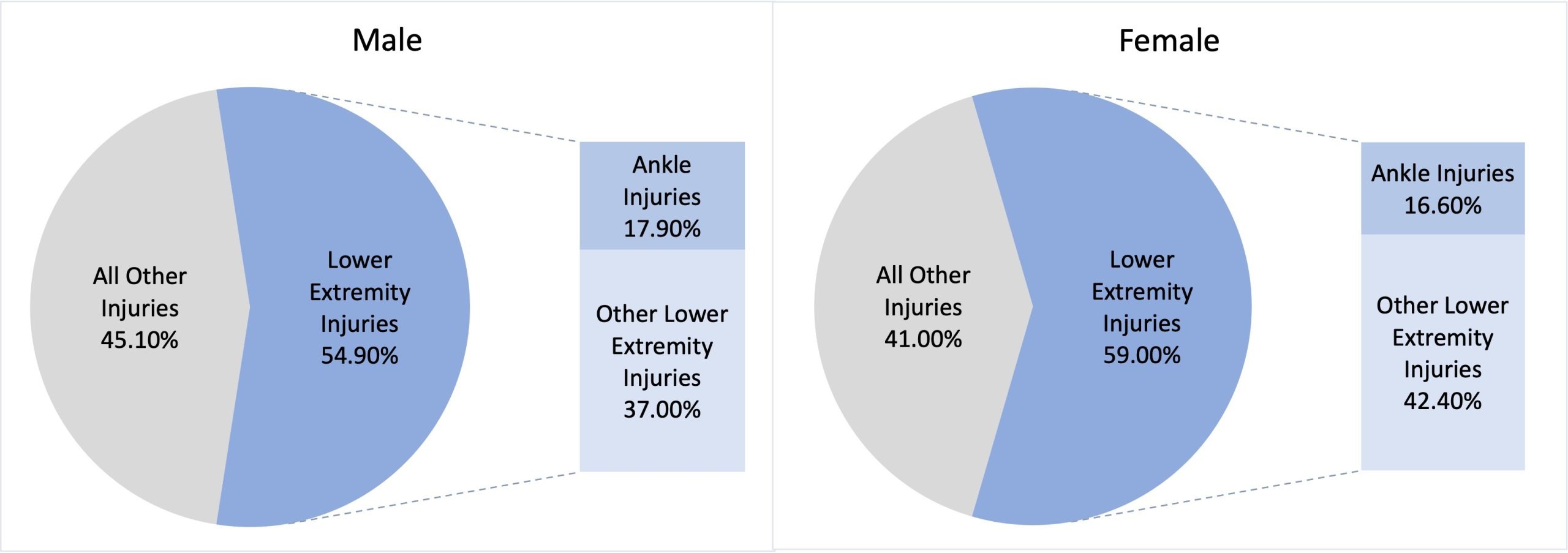
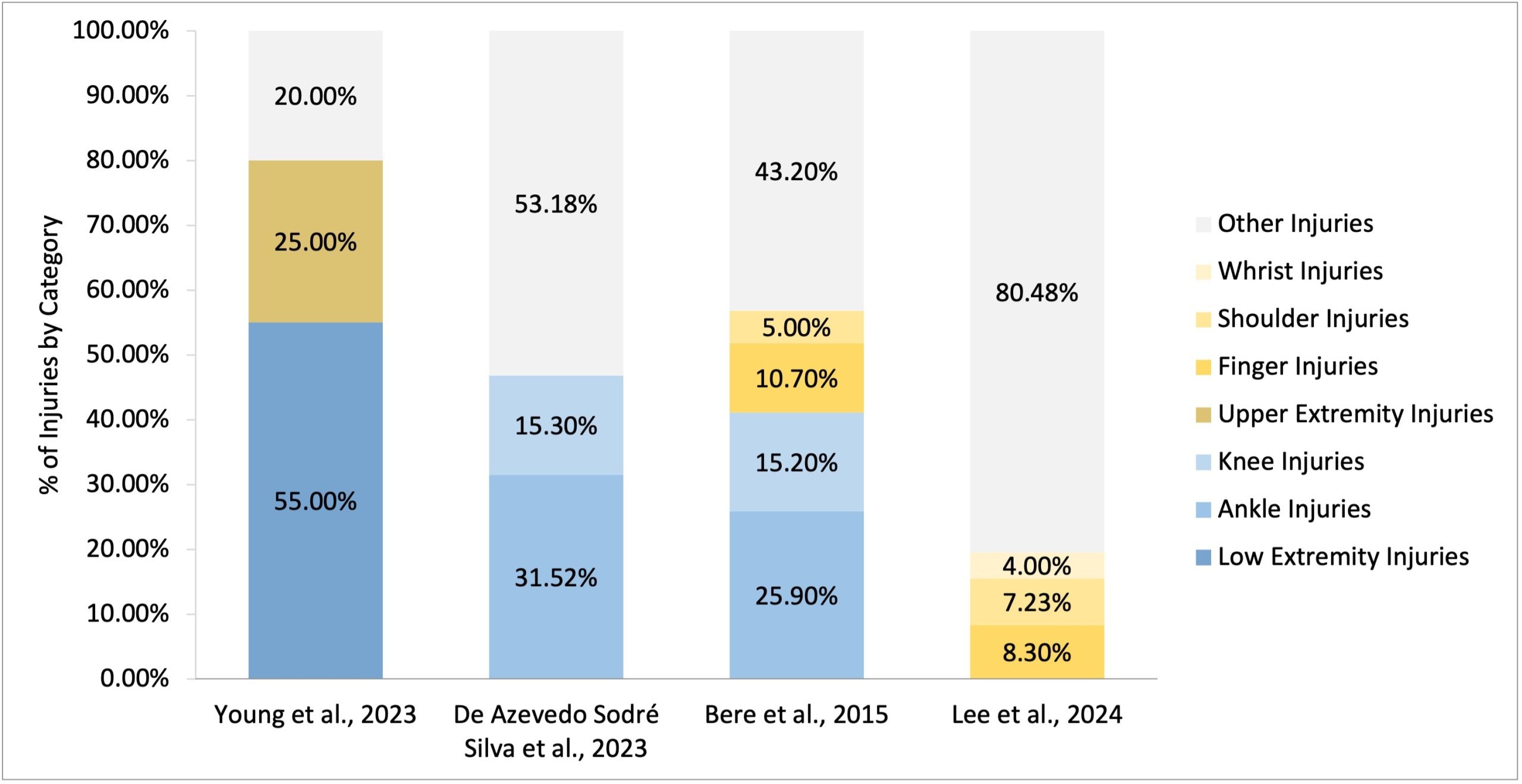
One study in this review utilized basketball injury data from the 2009/2010-2014/2015 academic years, part of the NCAA Injury Surveillance Program (NCAA-ISP). A total of 2,308 injuries during 176 team-season was reported for men, while a total of 1,631 injuries during 181-team seasons were reported for women. Men had an injury rate of 7.97 per 1,000 athlete-exposures, while women had an injury rate of 6.54 per 1,000 athlete-exposures5. The rate was higher in men than women (RR=1.22; 95% CI 1.15 to 1.30) and considered statistically significant5. Injuries to the lower extremity were the most common: in competitions, they measured at 54.9% of injuries and 59% of injuries for men and women, respectively5. While ankle injuries were the most common in the study when regarding both genders, males had a higher overall incidence rate of 17.9% while females had an incidence rate of 16.6%5 (Figure 1).
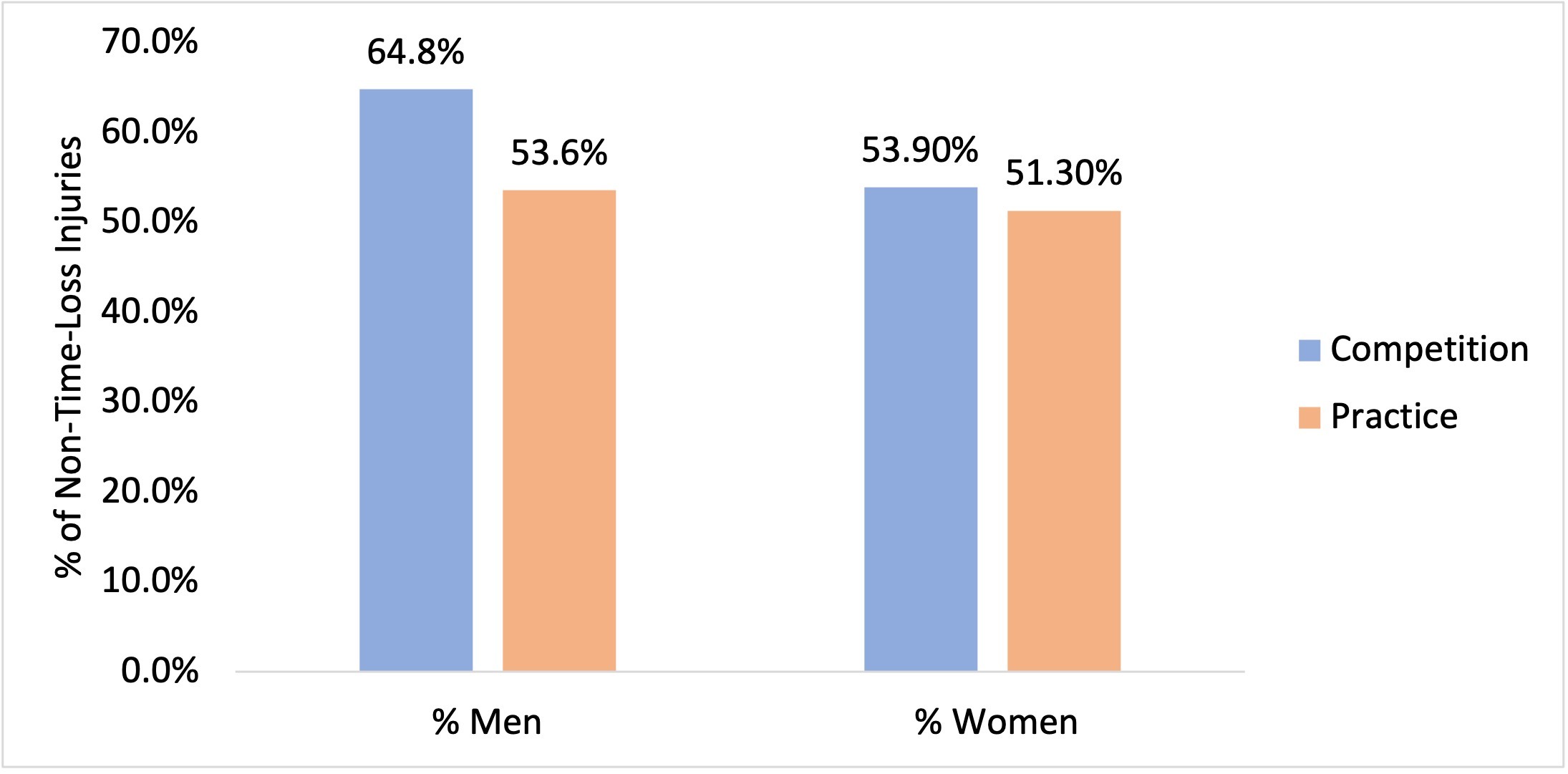
Per Zuckerman et. al, despite the high number of lower extremity injuries, more than half of all cases were non-time-loss (NTL) injuries with calculated averages of 53.95% (64.8% Male and 53.9% Female) and 52.45% (53.6% Male and 51.3% Female) in competition and practice, respectively5 (Figure 2).
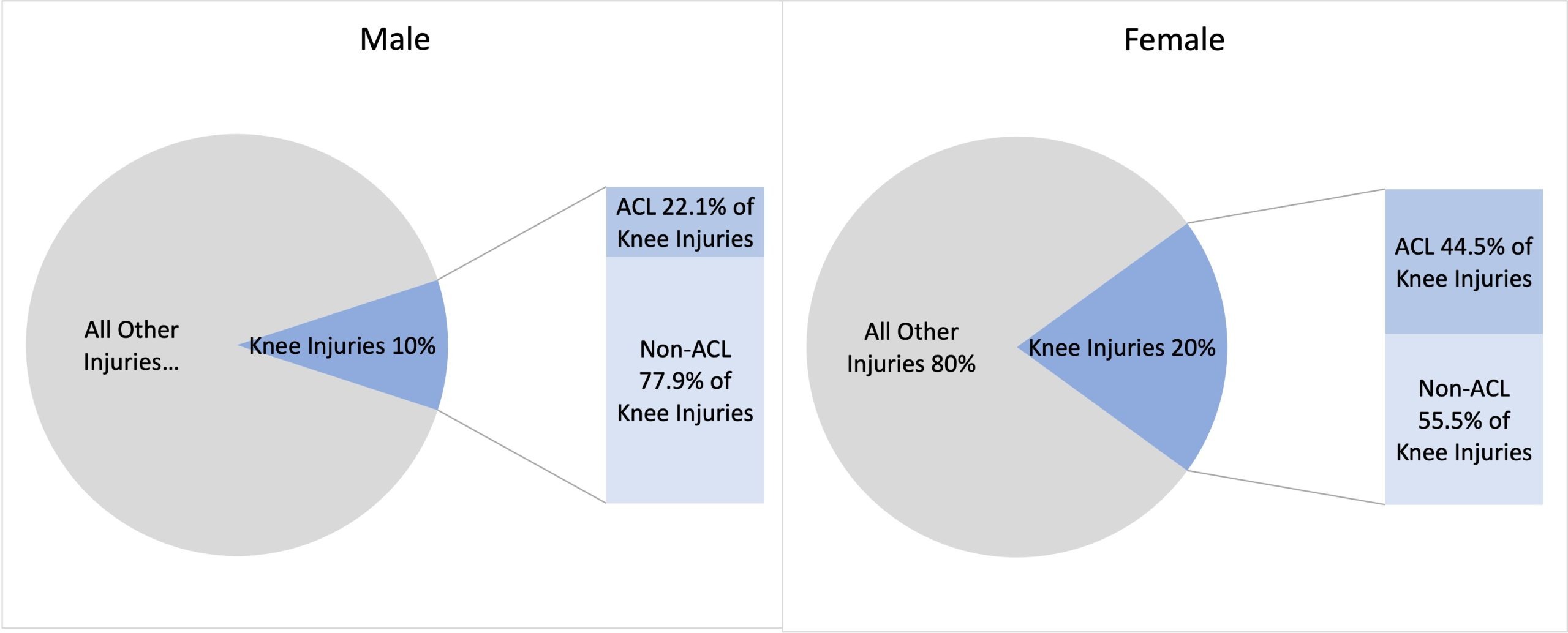
A systematic review by Milić et. al emphasized gender differences in sport injuries among adolescent males and females. Females experienced higher rates of ACL injuries than men with an incidence rate ratio (IRR) of 2.18 with 69% of injuries occurring without physical contact8. This IRR highlights a clinically meaningful difference and an effect size measure indicating the fact that females sustain ACL injuries at more than twice the rate of their male counterparts. Among young athletes, ankle injuries were most common with both males and females sustaining 49% and 46% of their injuries to the ankle, respectively8. The same article identified that the second most common injury types differed by sex: girls most frequently reported knee injuries (19% of all cases reported), whereas boys experienced more thigh injuries (10% of all cases reported)8. Furthermore, it found that in elite male basketball players, the most prevalent injuries include muscle strains (21.2%) and ankle sprains (11.9%) while elite female basketball players experience a higher rate of injuries to the lower extremity, accounting for 29.03% of all reported cases8. Another systematic review by Aksović et al. (2024) demonstrates additional differences between sports injuries in male and female basketball players. Women sustained a relatively high rate of knee injuries, accounting for 20% of all reported cases9. Men sustained a lower rate of knee injuries, accounting for 10% of all reported cases9. Moreover, among knee injuries, which occur disproportionately between sexes, the ACL is the most common injury9. Males sustain 22.1% of knee injuries to the ACL, while females sustain 45.9% of knee injuries to the ACL9 (Figure 3).
It is important to note that the authors described these differences in ratios as statistically significant. Similarly, female basketball players are almost four times more probable to sustain injuries to the ACL (relative risk is approximately 3.5-4.0, as summarized across multiple studies in Aksović’s systematic review, though specific p-values and confidence intervals for this estimate were not reported by Aksović et al.)9. Furthermore, according to Aksović et al. (2024), during ACL injury, female athletes exhibit greater lateral trunk lean and increased knee abduction angles compared with ACL-injured male athletes9. 3D analysis further indicated that females demonstrated a greater knee valgus angle than their male counterparts. Additionally, 3D kinematic analysis during a drop vertical jump revealed that female athletes display greater knee valgus and greater peak knee valgus during the landing phase compared to male athletes9. Collectively, these biomechanical characteristics may contribute to an increased risk and likelihood of ACL injury in female athletes. When taken together, the three studies reviewed in this section, namely Zuckerman et al; Milić et al.; and Aksović et al., follow the same pattern of findings. These studies reinforce that female basketball players sustain ACL injuries at substantially higher rates than males. However, the magnitude estimates differ (IRR 2.18 in Milić et al. vs. approximately 4-fold in Aksović et al.), reflecting possible differences in study population (multi-sport vs. basketball-specific), age ranges, and injury classification methods. This discrepancy emphasizes that pooled results should be regarded cautiously and that the ACL gap is strong in direction but may be uncertain in magnitude. While Zuckerman et al. reported a higher overall injury rate in males (RR = 1.22), Aksović et al. found females sustaining twice the rate of knee injuries specifically, bringing light to how sport-wide and joint-specific analysis can yield different, yet equally valid, conclusions. A consistent finding across all three studies is that sex-based disparities in basketball injury patterns are most notable in severe, non-contact injuries rather than overall injury frequency. This finding reinforces the importance of severity-based (or severity-stratified) reporting.
Performance Implications and Chronicity in Basketball
Ankle injuries result from acute trauma, a sudden, overwhelming, and intensely distressing event that occurs in a short period, in which the inferior tibiofibular, talocrural, and subtalar joints are unable to sustain the excess amounts of weight that said joints are undertaking11. Events like falling awkwardly on the ankle, or even landing on uneven surfaces may result in an ankle sprain or contusion. The high incidence of ankle injuries is concerning, as such injuries are strongly associated with the development of chronic ankle instability, which is associated with a high injury recurrence rate12. To that end, ankle injuries can take anywhere from 1-12 weeks to fully heal and combined with high rates of injury recurrence and development of chronic ankle instability, athletes can be unable to play for prolonged amounts of time11. Beyond the immediate loss of playing time, ankle injuries can impair proprioception, reduce vertical jump height, and limit lateral movement efficiency, key performance factors in basketball11. Persistent instability can also alter movement mechanics, which in return would increase susceptibility to secondary injuries such as knee strain or Achilles tendinopathy. Ankle injuries can also lead to the development of chronic ankle instability and osteoarthritis7. When analyzing prevention strategies, it was found that the most emphasis was placed on static and dynamic balance training, as both methods increase ankle strength and stability. Heightened proprioception and implementation of balance training not only aided in preventing ankle injuries in basketball, but in other high-risk sports too7. External ankle supports can also improve ankle stability, reducing risk of injury for basketball players. Wearing high-top shoes and ankle braces were found to reduce the risk of ankle injuries, with some studies claiming that braces are more effective than high-top shoes7. Current research indicates that secondary prevention strategies aimed at reducing reinjury risk are more effective than primary strategies designed to prevent initial injuries13. Although evidence is mixed in whether or not external ankle support or neuromuscular training is more effective7, it is likely that both forms of rehabilitation would decrease injury risk amongst athletes. A study analyzing both male and female basketball players reinforced neuromuscular warmups (which includes balance and stability exercises and multicomponent exercises) as effective in reducing injury risk14. Although the observed reduction was modest, even small decreases in injury risk were considered meaningful for both male and female athletes14. A notable point of conflict exists in the basketball prevention literature analyzed: the injury types with the greatest sex-based disparity (ACL tears, severe knee injuries) are not the same as the injury types with the highest overall frequency (ankle sprains). This is significant because prevention programs optimized for overall injury reduction, for example, general balance and proprioceptive training, may therefore have limited impact on the specific injuries that women disproportionately sustain. On the other hand, ACL-targeted neuromuscular programs are beneficial for female athletes, but have been under-implemented in male basketball populations. An approach that is sex-differentiated, rather than a single universal protocol, is necessary, and is heavily indicated by the evidence reviewed here.
Soccer Injury Epidemiology and Risk Patterns
Similarly, in professional football (soccer), a study conducted by Lopez-Valenciano et al. (2020) analyzing professional footballers in the United Kingdom found that the lower extremity had the highest injury incidence rate, occurring at an alarming frequency of 6.8 injuries per 1,000 hours of exposure15. Specifically, thigh injuries (hamstring strains, quadricep strains, abductor strains, etc.) were most common occurring at an incidence rate of 1.8 per 1,000 hours of exposure, with injuries to the knee being second to most common occurring at an incidence rate of 1.2 per 1,000 hours of exposure, and ankle injuries being third most common occurring at an incidence rate of 1.1 per 1,000 hours of exposure15. A different literature review conducted by Giza & Micheli (2005) analyzed the existing soccer injury statistics for youth players and found that knee and ankle injuries were the most common among soccer players, with injury incidence rate occurring at the calculated average of 8.55 per 1,000 hours of exposure, with an incidence rate of 2.3 per 1,000 practice hours to 14.8 per 1,000 game hours16 [Note: Giza & Micheli (2005) predates the 2010-2025 inclusion window and includes data on youth and recreational players rather than collegiate or professional athletes. This study was deemed as a foundational reference given the limited availability of female soccer injury data. However, findings should be interpreted in light of this population and date limitation.] Lopez-Valenciano’s study also found that the most frequent injury types in professional soccer involve the muscles and tendons, with muscle-related injuries accounting for 4.6 cases per 1,000 hours of exposure15. While Valenciano’s study identified the thigh as the most commonly injured lower extremity, another piece of research, conducted by Biz et al. (2021) has complemented this finding, identifying hamstring (part of the thigh) strains as the leading type of lesion in professional soccer occurring at a rate of 1.06 per 1,000 hours of exposure in training and 5.87 per 1,000 hours of exposure in competition15,17. Even though Valenciano’s study focused solely on professional male athletes, its data was contextually comparable to other research, and on this premise, was included into this review. An exception was also given to an older Giza & Micheli (2005) study due to the underrepresentation of female soccer athletes in research materials. Its dataset contained both male and female athletes and was therefore included.
Sex-Based Differences in Soccer Injury Patterns: Rates, Types, Anatomical Distribution
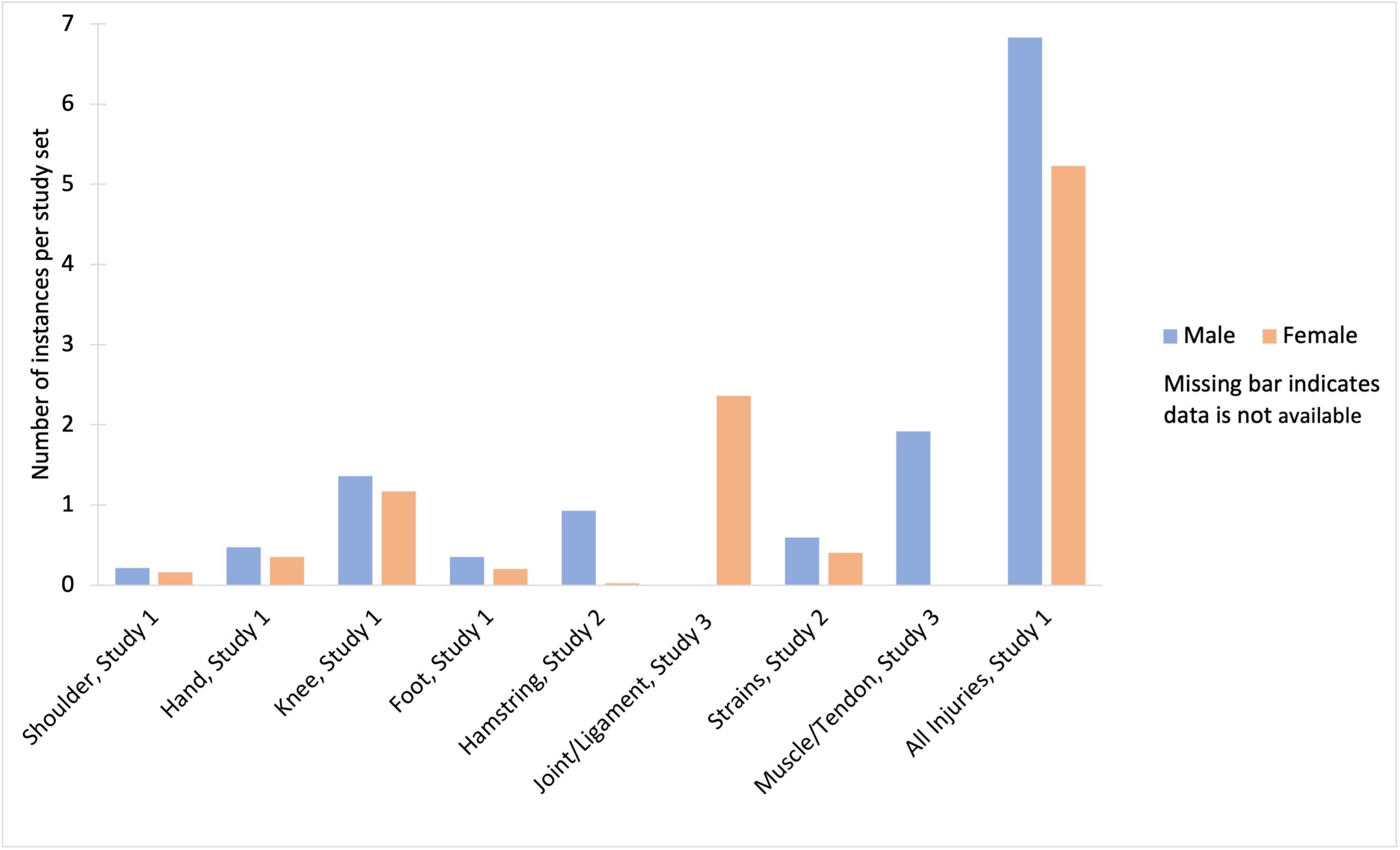
Female soccer players sustain injuries at a significantly lower overall rate than males, with 5.23 injuries per 100 players compared to 6.83 injuries per 100 players, representing a 24% lower injury rate among females (RR-0.766 CI:0.730-0.804, p<0.0001)18. Although male players experience a higher frequency of contusions, fractures, joint dislocations, and musculotendinous injuries, female players are more likely to sustain severe injuries18. Specifically, males demonstrate higher injury rates across multiple anatomical regions, including the shoulder (0.21 vs. 0.16 per 100 players [p=0.0403]), hand (0.47 vs. 0.35 per 100 players [p=0.0004), knee (1.36 vs. 1.17 per 100 players [p=0.0015]), and foot (0.35 vs. 0.20 per 100 players [p=0.0001]) when compared to females18. Another study analyzing male and female football players found that the most common type of injury grouping for males was muscle/tendon injuries (1.92 injuries per 1,000 hours [95%CI: 1.26–2.58, I2 = 99.0%]) followed by followed by joint (non-bone) and ligament (IIR = 0.97 injuries per 1,000 hours; 95%CI: 0.64–1.30, I2 = 97.4%)19. Unlike injuries in males, joint (non-bone) and ligament injuries (IIR = 2.36 injuries per 1,000 hours; 95%CI: 1.62–3.11, I2 = 59.0%) were the most common type of injury among females followed by muscle and tendon injuries (IIR = 2.01 injuries per 1,000 hours; 95%CI: 1.75–2.28, I2 = 0%)19. A third study conducted by Cross et al. (2013) compared hamstring injury rates between male and female collegiate soccer athletes. Across all NCAA soccer teams, men accounted for 4,032 strains, while women sustained 2,744 strains, corresponding to 59.5% and 40.5% of total strains, respectively. Overall, male athletes were 64% more likely to sustain hamstring injuries than female athletes (IRR, 1.64; 95% CI, 1.37-1.96)20. Moreover, men had significantly higher rates of hamstring strains than women during both competition (IRR, 2.42; 95% CI, 1.82-3.23) and practice (IRR, 1.34; 95% CI, 1.06-1.68)20 (Figure 4).
It is important to note that the results of all three studies were reported as statistically significant, demonstrating a large and clinically meaningful effect. Across the three football (soccer) studies reviewed in this section, a consistent yet nuanced finding emerges. Both Mufty and Robles-Palazón’s studies agree that males sustain higher overall injury rates but females experience proportionally more ligament and joint injuries. However, Cross’ results may complicate this picture by showing that male soccer players sustain hamstring strains at 1.64 times the rate of females (IRR 1.64, 95% CI 1.37–1.96), which appears to contradict the general pattern of female susceptibility to severe injuries. It is important to note that Cross’s study does not appear to differentiate by injury severity, which limits the extent to which this finding can be said to challenge the broader pattern, as hamstring strains exist on a considerable spectrum: ranging from minor Grade I tears to complete Grade III ruptures. This makes direct comparisons between the two pieces of evidence difficult to substantiate. This discrepancy between males and females is best explained by the muscle-specific mechanism: hamstring strains are largely driven by eccentric loading during high-speed sprinting, a demand that is greater in male soccer athletes due to higher average sprint speeds. The collective soccer evidence suggests that sex-based injury risk is not uniform across injury types, as females are at greater risk for injuries to the ligaments, while males are at greater risk for muscle strain injuries. These findings indicate that prevention systems and protocols should be both sex and injury-specific to be effective.
Hamstring Strain Injuries in Soccer: Mechanisms, Consequences, Prevention Strategies
Hamstring strain injuries, classified as eccentric-contraction-induced skeletal muscle injuries, are characterized by excessive elongation, contracture, or, in severe cases, partial tearing of the muscle fibers17. These injuries typically occur during high-intensity sprinting, abrupt directional changes, or sudden acceleration and deceleration, with sprinting identified as the primary activity linked to hamstring injury23. Additional research also indicates that muscle weakness and strength imbalances between the quadriceps and hamstrings may detrimentally increase an athlete’s susceptibility to injury24. Furthermore, repeated strain can inhibit long-term muscle function and coordination24, which can manifest in things like reduced sprint speed, diminished kicking strength, and impaired agility. While return to sport is typically achieved within weeks of the injury, subsequent athlete performance may be impaired, and reinjury rates are high, similar to what is seen in ankle injuries25. Chronic hamstring issues may also progress into tendinopathies, which can substantially reduce training efficiency, limit explosive movement, and even pose career-ending detriments for athletes due to excessive pain26. When analyzing prevention strategies for hamstring injuries, a study by Al Attar & Hussain (2023) found that eccentric training focused on the lengthening phase of muscle contraction decreased the injury rate of hamstring muscles27. Specifically, core muscle strengthening exercise (CMSEs) such as Nordic hamstring (NH) exercise were most efficient in reducing the rate of both new and chronic hamstring injuries27. Meta-analysis from this study found a reduction of 50% of hamstring injuries in the intervention group when CMSEs were included in the protocol compared with the control group who implemented usual exercise programs27. Furthermore, in players with previous hamstring strains, they found that injury rates decreased by around 86% relative to other players who were using regular training programs27. According to Al Attar & Hussain’s study, only a single study with female athlete participation was available, so it was not possible to perform analysis based on sex differences27. Despite this limitation, complementary research supports the effectiveness of eccentric hamstring exercises and balance training in female athletes as well. Because female athletes sustain a disproportionate number of severe knee injuries, particularly anterior cruciate ligament (ACL) tears, studies have focused on identifying effective prevention strategies. In Crossley’s 2020 study, exercise programs with multiple components reduced overall injuries (IRR 0.73, 95% CI 0.59 to 0.91) and ACL injuries (IRR 0.55, 95% CI 0.32 to 0.92)28. For exercise-based strategies (single-component and multicomponent), hamstring injuries were also reduced (IRR 0.40, 95% CI 0.17 to 0.95)28. Furthermore, according to Crossley et al. (2020), there is low-level evidence that multicomponent, exercise-based programs reduce overall and ACL injuries by 27% and 45%, respectively28. Although this research primarily targeted women, these programs also significantly reduced ACL injury rates in males, with reductions found in athletes of both sexes (OR=0.50; 95% CI 0.41 to 0.59), and female athletes specifically (OR=0.33; 95% CI 0.27 to 0.41)28. Throughout this section, a notable finding is that effective interventions, such as Nordic hamstring exercises (86% recurrence reduction) and multicomponent neuromuscular programs (45% ACL reduction), target different injury types and different populations. For example, Nordic exercises address the predominant male hamstring strain risk, while ACL programs primarily benefit female athletes, as they sustain higher ACL injury rates. This suggests that optimal soccer injury prevention requires a parallel rather than unified protocol. Males should perform eccentric hamstring loading exercises while females should perform neuromuscular ACL training exercises. The substantially lower female Odds Ratio for ACL injuries with neuromuscular training (0.33 vs 0.50 for both sexes combined) further reinforces the notion that females receive disproportionate benefits from these programs. This is significant because it highlights how sex-based implementation, if implemented, is evidence based.
Volleyball Injury Patterns: Prevalence and Distribution Across Upper and Lower Extremities
In the sport of volleyball, the lower extremity is the most commonly injured part of the body, accounting for between 50–60% of all injuries29. In a separate study of professional volleyball players, of all incidences reported, ankle injuries were the most commonly reported injuries across volleyball athletes, accounting for 25.9% of all injuries30. The knee was reported second most common accounting for 15.2% of all injuries recorded in the study30. Another study conducted by de Azevedo et al. similarly found that ankle injuries were most prevalent, accounting for 31.52% of injuries31. It also found that the knee sustained the second highest injury site percentage when it came to lower extremities, occurring at 15.3%31. Second to lower extremity injuries, upper extremity injuries accounted for 20-30% of all injuries reported29. In the same study analyzing professional volleyball players, it found that injuries to the fingers were most common, accounting for 10.7% of all upper extremity incidents reported30. Shoulder injuries were the second most common upper extremity injury, accounting for 5% of all upper extremity incidences30. Another study analyzing both male and females from the National Electronic Injury Surveillance System for volleyball further reinforced this data, finding that the top 3 most commonly injured areas of the upper extremities were the finger (33.2%), shoulder (28.9%), and the wrist (16%) for both men and women32 (Figure 5).
The four studies reviewed in this section, namely Young et al., Bere et al, de Azevedo et al., and Lee et al, present a largely consistent finding among volleyball injury distribution. These studies indicate that ankle and knee injuries dominate the lower extremities, while shoulder, wrist, and finger injuries dominate the upper extremity. However, one discrepancy arose that is worth noting: Bere et al, which analyzed world-class FIVB athletes, reported lower overall injury rates than studies of youth and collegiate populations, highlighting that injury risk may not be linear in correspondence to volleyball level, and may actually be lower at elite levels of play. This may be due to the fact that technique, conditions, and medical support are more sophisticated at higher levels of play. This contrasts with the finding found in basketball literature, where higher competition levels were largely associated with higher injury rates. This is significant because it may highlight that the relationship between competition level and injury risk may be specific to certain sports. Moreover, it demonstrates that findings from elite volleyball populations may not be generalized for recreational or developmental athlete demographics.
Sex-Based Disparities: Volleyball Injury Rates, Anatomical Distribution, Injury Mechanics
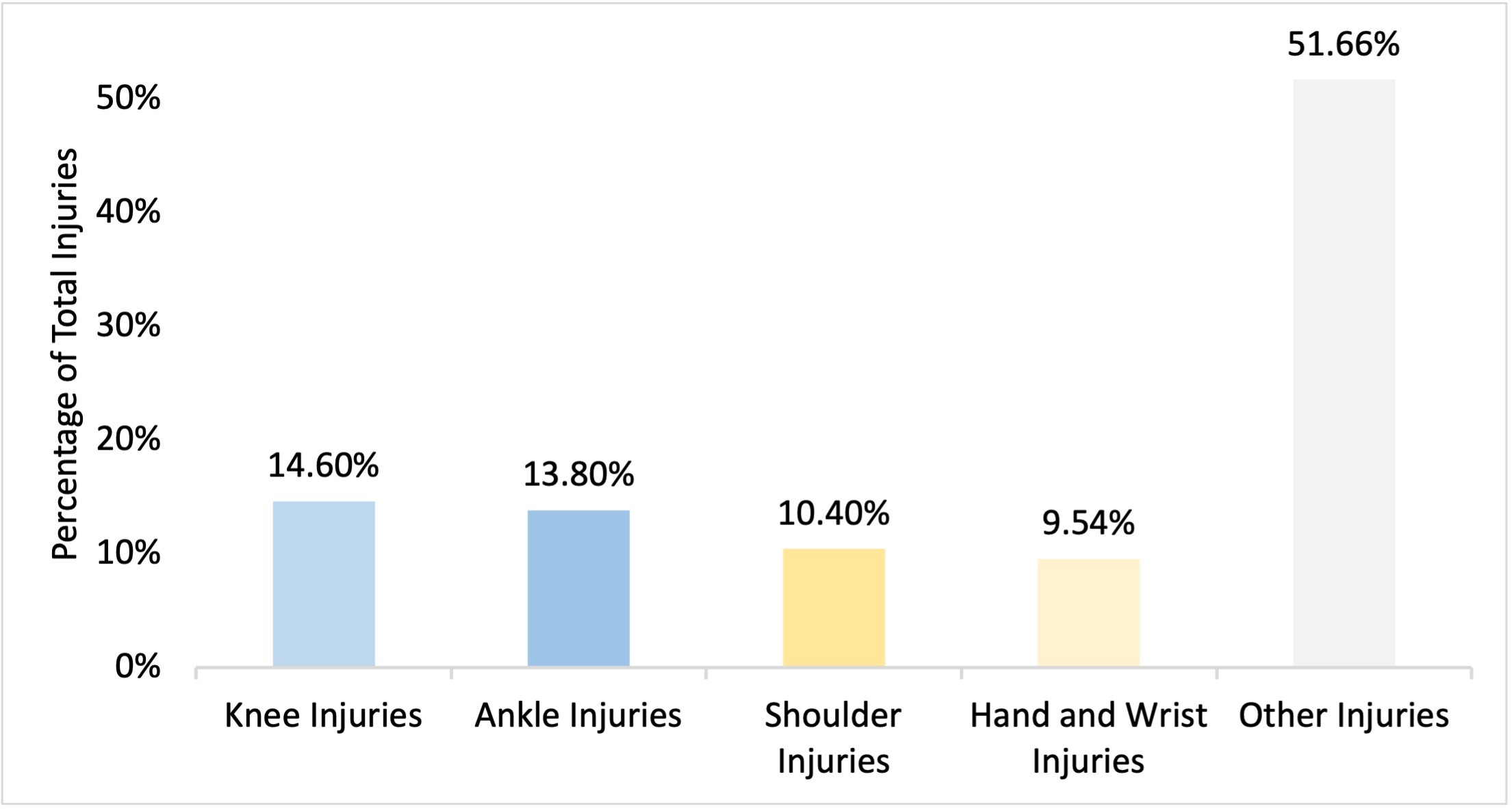
In two volleyball studies, the (volleyball) match injury incidences were 4.4 and 12.2 per 1,000 hours for females and 3.8 and 11.7 per 1,000 hours for males37. Zech et al. did not indicate p-values or confidence intervals for these sex-based comparisons, and the overlap in ranges across the two studies suggests these differences may not be statistically significant. This was acknowledged by the authors in their original meta-regression analysis. Studies focusing exclusively on female volleyball players reported that knee injuries were the most prevalent, accounting for 14.6% of all injuries, followed closely by ankle injuries at 13.8%38. Similarly, an investigation of male athletes from a Brazilian volleyball team corroborated these findings, identifying the knee (111 injuries per 1,000 athletes) and ankle (69 injuries per 1,000 athletes) as the most frequently injured anatomical regions39. One study conducted by Kilic et al. did find that men ultimately have a higher risk for ankle injuries compared to adult women (Risk Ratio of 3.2)40, and a large effect size indicated that males are more than three times as likely as females to sustain injuries in volleyball. However, confidence intervals and p-values for this estimate were not reported in this reviewed source. Data focusing on the general male population showed a statistically significant risk for patellar tendinopathy (OR (odds ratio) of 2.0 95% CI (confidence interval) 1.1–3.5); meanwhile, male volleyball players have increased risk of developing patellar tendinopathy (OR 2.6 95% CI 1.3–5.2). There was no similar data for females and female volleyball players41,42. Both odds ratios exclude 1.0 from their confidence intervals, confirming that these numbers are statistically significant. However, the absence of equivalent female data inhibits any direct sex-based comparisons. In addition to lower-extremity injuries, upper-extremity injuries were also reported for women, with shoulder injuries accounting for 10.4% of all injuries and hand and wrist injuries accounting for 9.54%38. Furthermore, it was found that both noncontact and overuse injuries constituted a majority of all incidences reporting, accounting for 22.71% and 26.12% of all injury incidences reported in women, respectively38 (Figure 6).
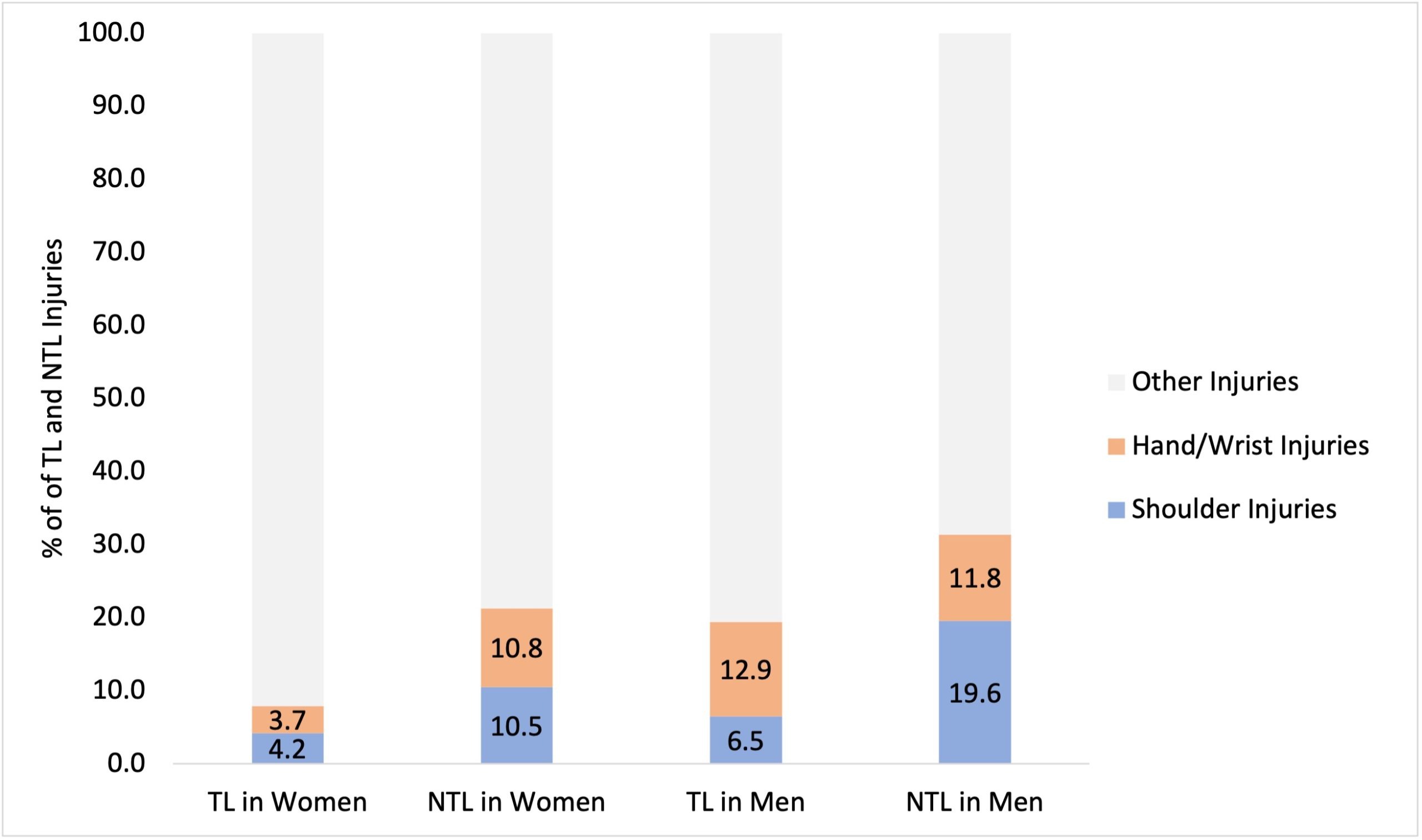
A study analyzing injury surveillance data from the NCAA found that shoulder injuries accounted for 4.2% of all time-loss (TL) injuries and 10.5% of all NTL injuries for women44. However, shoulder injuries accounted for 6.5% of all TL injuries and 19.6% of all NTL injuries for men44. Hand/wrist injuries accounted for 3.7% of all TL injuries and 10.8% of all NTL injuries for women. For men, hand/wrist injuries accounted for 12.9% of all TL injuries and 11.8% of all NTL injuries44 (Figure 7).
The sex-based volleyball evidence reviewed in this section presents contradictions that are worth noting. Zech et al. reported higher match injury incidences in female athletes (4.4-12.2 per 1,000 hours) compared to males (3.8-11.7 per 1,000 hours), indicating that females are more vulnerable to injuries overall. However, Kilic et al. reported a higher ankle injury risk in males (RR = 3.2). Despite this difference, these findings are not necessarily in conflict. Zech et al. ‘s ranges overlap and are not reported as statistically significant, while the Kilic et al. estimate is specific to ankle injuries. When taken together, these findings may suggest that males could be at greater risk for the most common injury (ankle sprains), while females may experience a greater and broader distribution of injury types, a finding consistent with the prior basketball and soccer findings. The predominance of noncontact (22.71%) and overuse (26.12%) injuries in female volleyball athletes further characterizes females’ injury profiles. This is significant because it shows that injuries to female volleyball athletes may be driven by accumulated load rather than acute trauma, highlighting training volume, recovery times, and proper technique as modifiable risk factors. These factors may be particularly relevant for female athlete injury prevention.
Volleyball Discussion: Mechanisms and Prevention of Knee and Shoulder Injuries
Injuries to the knee can include things like patellofemoral pain syndrome, patellar tendinopathy (Jumper’s Knee), knee sprain, or knee ligament tears30. Injuries to the patellar region are most commonly noncontact in nature45, and often result from overuse or improper landing mechanics. Injuries to the patellar region are most notable in sports that involve jumping, an action that is very common in volleyball45. The repeated action of jumping and landing, actions that are weight-bearing activities46, significantly increases an athlete’s susceptibility to developing patellar injuries. While lower extremity injuries are common amongst volleyball players, so are upper extremity injuries, like shoulder injuries and injuries to the hand/fingers/wrist. Throwing/smashing/spiking is considered one of the fastest human motions performed, and maximum humeral internal rotation velocity reaches about 7000° to 7500° per second47. Extreme amounts of external rotation in the range of 165° to 175° are also achieved by the throwing extremity during the late cocking phase (when the hitter’s dominant arm is drawn back into maximum external rotation after takeoff to prepare for acceleration)47. When shoulder revolutions occur in sequence, events that happen when spiking the ball in volleyball, the shoulder joint, or glenohumeral joint, gets put under increased load, and leaves athletes susceptible to shoulder injury47. Shoulder injuries are not only influenced by overuse but also by poor and improper or diminished biomechanics (likely results of fatigue from sport). Factors such as strength imbalances, deficits in the external rotators, and improper scapular positioning have been shown to increase the risk of shoulder injury48. For males with shoulder injuries, prevention/intervention should focus on stretching and increasing the flexibility of the posterior shoulder capsule, strengthening of the posterior cuff, and restoration of flexibility and muscle balance of the scapular muscles49. For women, however, the findings were less consistent. Based on four studies reporting female-specific outcomes, the literature review identified very low–certainty evidence of an association between shoulder range of motion and shoulder injury in females50. Similarly, analysis of five studies revealed very low–certainty evidence linking reduced shoulder strength to increased injury rates in female athletes50. Despite these limitations, the review found very low–certainty evidence that shoulder exercise programs incorporating strength, stability/control, and sport-specific exercises reduced shoulder injury rates by 51% among females across multiple sports, including volleyball50. The evidence examined for both knee and shoulder injuries in the sport of volleyball highlights a recurring theme that is seen throughout this literature review. The evidence is much more available and more developed for males than females; however, where female data does exist, it suggests greater responsiveness to intervention protocols. The odds ratios for male-predominant patellar tendinopathy are unable to be compared due to lack of female data, and the shoulder intervention evidence in females carries a very low certainty rating despite a meaningful 51% reduction in injury estimates. This pattern should manifest in investments in higher quality female-specific trials rather than the conclusion that evidence is insufficient. Moreover, it highlights a structural problem in volleyball literature; namely, that studies are frequently designed around male athlete populations or are not stratified by sex. This is significant because it leaves female-specific risk and prevention estimates severely underpowered and underrepresented. It is critical to address this gap before sex-specific volleyball prevention systems can be developed with confidence.
The Role of Nutrition and Sleep in Musculoskeletal Health and Injury Prevention
For this section, there is an important note on evidence quality. The following section reviews nutrition and sleep as factors that have been proposed as modulators of musculoskeletal health and injury risk. It is important to note that none of the studies cited in this section are athlete-specific intervention trials conducted on basketball, soccer, or volleyball players. The evidence consists primarily of general population observational studies, aging cohorts, military personnel samples, and animal models. Because of this, this section should be read as hypothesis background, identifying plausible biological systems and associations that warrant investigation in competitive athlete populations, rather than as primary evidence of effectiveness in the populations examined. These findings are presented and connected to the specific injury types most prevalent in the three sports examined in this literature review to illustrate the theoretical relevance of these recovery factors. It is not to imply established relationships between factors.
While musculoskeletal and flexibility exercises are among the most effective ways to reduce injury risk, physical and nutritional habits may play an important role in maintaining ligament, tendon and bone health. Despite emerging evidence, there is relatively little research regarding the relevance of diet, specifically in primary tendinopathies51. Because ligaments and tendons are primarily composed of Type I collagen, the majority of collagen-based supplemental treatments were associated with improvements in conditions like tendinopathy52, a problem common among athletes participating in sports examined in this paper. Because of the high prevalence of patellar tendinopathy in volleyball players and achilles/ankle tendon injuries in basketball players displayed in earlier sections, these associations are theoretically relevant. That said, it should be emphasized that the cited studies were not conducted in these athletic populations and their findings cannot be directly applied. Collagen, however, is not the only supplement that individuals may take in order to lower pain in conditions like tendinopathy. Studies show that several other compounds like, Methyl-sulfonyl-methane, Arginine, Curcumin, Boswellia serrata, and Bromelain were found to be associated with reduced pain, all compounds that can be consumed through supplements52. While these supplements may be harder to get a hold of due to their unknown effects to the common person, supplements like Vitamin C, also known as ascorbic acid, pose beneficial effects as well. Animal studies have shown that Vitamin C supported both tendon and bone healing, as well as ligament graft healing53. It must be acknowledged that this evidence comes from exclusively animal trials, which fall outside the written inclusion criteria of this review. Because of this, these findings are presented as hypothesis-generating background only and cannot be extrapolated to competitive athletes without supported human data. There is less human data, so further research should be conducted. Moreover, many studies have reported that high-protein diets are linked to increased production of IGF-1, a compound that is essential to osteotrophic growth and leads to increased bone mineral content54. High-protein diets are especially recommended to individuals undergoing large loads of training, as protein requirements are larger for individuals who participate in intense physical activity54. Consumption of polyunsaturated fatty acids, such as Omega-3 fatty acid chains also may lead to increased bone health. One study showed that individuals who reported higher consumption of omega-3 fatty acids had higher hip bone mineral density (BMD) than subjects who reported lower intake54. [Note: despite falling outside of the specific publication date criteria, the information provided by this study was deemed foundational, and therefore included in this literature review]. Other data has shown that adequate intake of other vitamins such as calcium, potassium, and vitamin D, which can either be consumed through whole food or supplementation, is associated with improved bone health outcomes in active populations, though the direct causal role in injury prevention among competitive athletes has not been established in trials. The theoretical relevance to the sports reviewed is plausible given the occurrence of lower extremity stress fractures at a rate of approximately 4.8 per NBA season and the documented role of bone mineral density in stress fractures susceptibility. That said, no included study directly links nutritional supplementation to stress fracture reduction in athlete populations54,55.
Though diet plays a significant role in ligament and bone health, sleep, something that many people take for granted, has been increasingly associated with recovery outcomes and musculoskeletal health. Evidence shows that disruption to circadian rhythm as well as sleep disturbances may alter bone formation, metabolism, and structure56. These negative effects may lead to increased fracture risk. Moreover, data suggests that less than 7 hours of sleep for periods of at least 14 days has been associated with 1.7 times greater risk of musculoskeletal injury57. This association is theoretically relevant to the high-reinjury rates observed for ankle sprains and hamstring strains in the sports examined in this literature review, though this cited study did not examine basketball, soccer, or volleyball athletes and does not permit sport-specific conclusions. In U.S Army Special Operation Forces soldiers, individuals who are similarly active like athletes, soldiers who slept less than 4 hours were 2.35 times more likely to experience a musculoskeletal injury compared to those who slept 8 or more hours58. It is important to note that military personnel were not inside the stated inclusion criteria of this review. However, they were included as context given the absence of comparable athlete sleep-injury data, and these findings should be considered hypothesis-gathering rather than applicable to collegiate or professional athletes. Because 95% of the 7,576 soldiers analyzed were male, more research should be conducted for women’s statistics and data. When data was stratified by age, older individuals were found to have a significantly higher risk of injury than their younger counterparts across all groups with different sleep duration58. Furthermore, longitudinal studies indicate that adherence to healthy sleeping patterns has resulted in individuals with 17% reduction in the risks of incident falls, and 28% reduction of risk of fractures59. This may be manifested in the fact that sleep and circadian disturbances cause sleepiness and decreased vigilance to environmental hazards, which in return is associated with an increased risk of falls and fractures56. The prior findings come from a general aging cohort rather than an athlete population and are included as supporting evidence only. Direct athlete participation and replication is needed before the evidence can be applied to competitive athletes One study, conducted by Yang et al., analyzing 10,346 individuals found that poor sleep patterns including short sleep duration and long sleep duration both posed an increased risk of low BMD60. Evidence suggests that an inactive lifestyle may pose severe detriments to BMD60. Prolonged daily sitting had harmful effects towards BMD, and physical activity mitigated the increased risk of low BMD associated with irregular sleep patterns and prolonged sedentary behavior60. This study analyzed general population samples and lacked stratification by sex; it is presented as contextual background. Interpretation is not directly applicable to athlete populations.
Combining nutrition and sleep evidence with the injury findings from the three sports reveals both opportunities and limitations. The opportunity is that there are multiple supplemental recovery pathways, including collagen supplementation for tendon health, adequate Calcium and vitamin D for BMD, and sufficient sleep for neuromuscular recovery and injury risk reduction, that could be applied through practical and low-cost means. However, the limitation of these findings is that nearly all of this evidence derives from general population studies, military samples, or animal models, (none of which are sex-stratified) that don’t support extrapolation for athlete populations. Because of this, it is unknown whether female athletes would obtain greater, equal, or lesser benefit from these recovery systems and protocols compared to male athletes. The absence of athlete-specific, sex-stratified recovery intervention data is not a small limitation, it is fundamental and significant as it limits the ability to make evidence-based recommendations for males and females in basketball, soccer, and volleyball athlete populations.
Summary of Findings
The convergent finding across all three sports reviewed is that lower extremity injuries dominate injury profiles; however, the specific injury types and their unique distributions differ in ways that reflect each sport’s demands rather than random variation. Basketball and volleyball epidemiology shares ankle sprain as the most frequent injury, consistent with the repetitive jumping, direction changing, and landing mechanics common in both sports. Soccer, by contrast, exhibits a different injury profile dominated by hamstring strains, linked to the high-speed sprinting and eccentric loading demands. This across-sport pattern suggests that injury risk is not a function of athletic intensity, but it is shaped by different movement demands, a finding with direct implications for sport-specific prevention programs.
The sex-based disparity in ACL injury risk represents the most consistent and clinically significant finding across studies. The incidence rate ratio of 2.18 reported by Milić et al. and the four times relative risk reported by Aksović et al. are consistent, but neither fully accounts for potential confounding factors such as differences in exposure time, competition level, or reporting practices between male and female populations. The biomechanical explanations, namely greater knee valgus angles, altered landing mechanics, ligamentous laxity, are well supported, but derive largely from laboratory “drop-jump” studies, where athletes are told what to do, rather than in-game injury analyses, raising questions about validity. Taken together, the evidence demonstrates a multifaceted model in which anatomical and neuromuscular factors interact to elevate ACL risk in female athletes. However, no single factor has been demonstrated to be independently sufficient in nature. This has important ramifications. Prevention programs targeting only one mechanism are unlikely to achieve maximal efficiency. The 45% ACL injury reduction observed with multicomponent training programs supports this interpretation.
An apparent contradiction in the evidence needs to be explained. Male athletes consistently show higher overall injury rates, yet female athletes sustain more severe injuries, particularly ACL tears and joint/ligament injuries. This pattern reflects a meaningful distinction between injury frequency and injury severity. Male athletes may sustain more lower grade injuries (contusions, minor muscle strains) given their longer training times and contact exposure, while the biomechanical vulnerability of female athletes exposes them to fewer but more extreme injuries. This is an important distinction, as aggregate injury rate comparisons may understate the injury burden on female athletes if severity is not accounted for. Surveillance systems that count injuries without accounting for severity or time-loss will produce misleading sex-based comparisons. This is a significant methodological limitation that several included studies share and that future research must address through specifically stratified reporting.
The recovery section of this literature review reveals a critical gap between existing evidence and athlete-specific evidence. While sleep deprivation, poor nutrition, and inadequate mineral, vitamin, or supplement intake are plausibly linked to increased musculoskeletal injury risk, the evidence for most of these associations derive from general population studies, military population samples, or animal models rather than from intervention trials in athlete populations. This does not invalidate the plausibility of these relationships, but it does not mean that these recommendations for athletes are to be extrapolated with certainty. Furthermore, the field lacks randomized controlled trials examining sleep and nutritional interventions specifically in female athlete populations, stratified by sport and other related factors.
When taken together, these findings suggest that the field of sports injury prevention would benefit from three suggested shifts. First, the field should move from sex-aggregated to sex-stratified study designs as a default rather than an exception. Second, the field should adopt standardized injury classification systems that account for severity and time-loss consistently across sports and institutions. Third, the field should conduct athlete-specific recovery intervention trials that can account for the current gap between plausibility derived from mechanics and clinical evidence. Moreover, the underrepresentation of female athletes in literature is not merely a methodological shortcoming, it is a systematic inequality with real consequences for the quality of care that female athletes receive. Addressing this gap is both a scientific and ethical priority for the field of sports medicine.
Limitations
Conducting this research presented several limitations, highlighting extreme gaps in existing literature. One major limitation is the lack of consistency in study methodology, particularly in how many injuries are both recorded and classified. Differences in methodology make direct comparisons across a plethora of different studies difficult, and sometimes even sometimes dangerous, as data can be misleading. As a result, injury incidence rates may vary due to true differences, as well as because of inconsistent reporting standards. Additionally, many studies differ in their scope of analysis. Some studies may have focused solely on specific injury types such as ankle sprains or ACL tears, whereas other studies included all injuries regardless of severity and relevance to the primary research goal. This difference can lead to both overrepresentation and underrepresentation of injuries across several sports, even further making synthesis of several studies difficult. Another limitation is the uneven representation of competition level. Many studies vaguely define where their athletes are competing, making it difficult to pick studies which fit the criteria of professional athletes. Another factor that is unevenly represented is age and age groups. Many studies also vaguely define their age groups, making it difficult to create correlations between certain injuries and ages. The biggest limitation though is the uneven representation of sex or gender. There are significantly less studies examining solely females, or even females and males together. This imbalance makes it difficult to find data to apply to certain groups, thus making the search for valid rehabilitation techniques even more difficult.
Future Directions
To mitigate these limitations and improve future research, researchers should prioritize standardization across sports injury-related studies to improve the comparability of results. Establishing things like definitions for injury classification, cause, and severity would allow for more accurate synthesis between many studies, reducing the risk of misleading conclusions. Additionally, future studies should clearly define their scope of analysis and state whether they examined specific injury types or included all reported injuries. Clearly establishing injury inclusion criteria would minimize overrepresentation and underrepresentation of injuries and improve transparency among people trying to interpret data. Another measure that should be taken is greater specificity regarding demographics/population. Future studies should clearly define competition level, age range, and athletic background, avoiding vague phrasing like “elite”, and “adult”, to allow for comparison across specific populations. Age-specific analysis would help identify certain developmental risk factors and would prompt targeted prevention for the correct relative age group. Most importantly, future research must address the immense underrepresentation of female athletes. Studies should focus on always including female demographics, or even focusing on them separately, as applying male data to females, who often are different from males, could be dangerous and unhelpful. Moreover, improving disparities among gender research will enable more accurate identification of injury patterns and rehabilitation needs across multiple populations. This shift is almost essential for developing evidence-based, and inclusive injury prevention/recovery protocols that can be applied across all athlete demographics.
Conclusion
This narrative review synthesizes evidence on musculoskeletal injury patterns across basketball, soccer, and volleyball, with particular attention to sex-based differences and the theoretical role of recovery factors. Lower extremity injuries predominate across all three sports, but their distribution is sport-specific. Ankle sprains are most prevalent in basketball and volleyball, while hamstring strains dominate in soccer. A consistent and clinically significant finding is that female athletes sustain ACL and joint-ligament injuries at substantially higher rates than males, driven by a combination of biomechanical and neuromuscular factors. Male athletes, however, sustain higher overall and muscle-strain injury rates. Evidence-based prevention strategies, including multicomponent neuromuscular programs and eccentric hamstring loading, show injury reductions, with female athletes obtaining disproportionate benefit from ACL-targeted programs. Recovery factors such as sleep and nutrition are biologically plausible modifiers of musculoskeletal health, but the available evidence mainly comes from non-athlete populations and cannot (yet) be directly applied to competitive athletes. Female athletes remain substantially underrepresented in the sports medicine literature, constraining the development of sex-specific and evidence-based protocols across all three sports reviewed. Addressing this disparity through specifically stratified study designs, standardized injury classification, and athlete-specific recovery trials is the most crucial step for the field of sports medicine.
Supplementary Material
References
- R. W. Paul, J. H. Sonnier, E. E. Johnson, A. T. Hall, A. Osman, G. M. Connors, K. B. Freedman, M. E. Bishop. Inequalities in the evaluation of male versus female athletes in sports medicine research: a systematic review. The American Journal of Sports Medicine. Vol. 51, pg. 3335–3342, 2023 https://doi.org/10.1177/03635465221131281 [↩]
- W. H. Meeuwisse, R. Sellmer, B. E. Hagel. Rates and risks of injury during intercollegiate basketball. The American Journal of Sports Medicine. Vol. 31, pg. 379–385, 2003 https://doi.org/10.1177/03635465030310030901 [↩] [↩]
- J. Vicentini, R. Mercer, F. J. Simeone. Basketball: biomechanics and imaging findings of common injuries. 2025 [↩]
- E. Stojanović, O. Faude, M. Nikić, A. T. Scanlan, D. Radovanović, V. Jakovljević. The incidence rate of acl injuries and ankle sprains in basketball players: a systematic review and meta-analysis. Scandinavian Journal of Medicine & Science in Sports. Vol. 33, pg. 790–813, 2023 https://doi.org/10.1111/sms.14328 [↩]
- S. Zuckerman, A. Wegner, K. Roos, A. Djoko, T. Dompier, Z. Kerr. Injuries sustained in national collegiate athletic association men’s and women’s basketball, 2009/2010-2014/2015. 2016 [↩] [↩] [↩] [↩] [↩] [↩] [↩] [↩] [↩]
- J. Lian, F. Sewani, I. Dayan, P. B. Voleti, D. Gonzalez, I. M. Levy, V. Musahl, A. Allen. Systematic review of injuries in the men’s and women’s national basketball association. The American Journal of Sports Medicine. Vol. 50, pg. 1416–1429, 2022 https://doi.org/10.1177/03635465211014506 [↩]
- J. B. Taylor, K. R. Ford, A.-D. Nguyen, L. N. Terry, E. J. Hegedus. Prevention of lower extremity injuries in basketball: a systematic review and meta-analysis. Sports Health. Vol. 7, pg. 392–398, 2015 https://doi.org/10.1177/1941738115593441 [↩] [↩] [↩] [↩] [↩]
- V. Milić, O. Radenković, I. Čaprić, R. Mekić, N. Trajković, O. Špirtović, A. Koničanin, M. Bratić, R. Mujanović, A. Preljević, B. Murić, I. Kahrović. Sports injuries in basketball, handball, and volleyball players: systematic review. Life (Basel, Switzerland). Vol. 15, pg. 529, 2025 https://doi.org/10.3390/life15040529 [↩] [↩] [↩] [↩] [↩]
- N. Aksović, S. Bubanj, B. Bjelica, M. Kocić, L. Lilić, M. Zelenović, D. Stanković, F. Milanović, L. Pajović, I. Čaprić, V. Milić, T. Dobrescu, C. Sufaru. Sports injuries in basketball players: a systematic review. Life (Basel, Switzerland). Vol. 14, pg. 898, 2024 https://doi.org/10.3390/life14070898 [↩] [↩] [↩] [↩] [↩] [↩] [↩]
- N. Aksović, S. Bubanj, B. Bjelica, M. Kocić, L. Lilić, M. Zelenović, D. Stanković, F. Milanović, L. Pajović, I. Čaprić, V. Milić, T. Dobrescu, C. Sufaru. Sports injuries in basketball players: a systematic review. Life (Basel, Switzerland). Vol. 14, pg. 898, 2024 https://doi.org/10.3390/life14070898 [↩]
- J. McKeon, M. Hoch. The ankle-joint complex: a kinesiologic approach to lateral ankle sprains. 2019 [↩] [↩] [↩]
- M. Herzog, Z. Kerr, S. Marshall, E. Wikstrom. Epidemiology of ankle sprains and chronic ankle instability. 2019 [↩]
- G. S. Schiftan, L. A. Ross, A. J. Hahne. The effectiveness of proprioceptive training in preventing ankle sprains in sporting populations: a systematic review and meta-analysis. Journal of Science and Medicine in Sport. Vol. 18, pg. 238–244, 2015 https://doi.org/10.1016/j.jsams.2014.04.005 [↩]
- A. C. Davis, N. P. Emptage, D. Pounds, D. Woo, R. Sallis, M. G. Romero, A. L. Sharp. The effectiveness of neuromuscular warmups for lower extremity injury prevention in basketball: a systematic review. Sports Medicine – Open. Vol. 7, pg. 67, 2021 https://doi.org/10.1186/s40798-021-00355-1 [↩] [↩]
- A. López-Valenciano, I. Ruiz-Pérez, A. Garcia-Gómez, F. J. Vera-Garcia, M. De Ste Croix, G. D. Myer, F. Ayala. Epidemiology of injuries in professional football: a systematic review and meta-analysis. British Journal of Sports Medicine. Vol. 54, pg. 711–718, 2020 https://doi.org/10.1136/bjsports-2018-099577 [↩] [↩] [↩] [↩]
- E. Giza, L. J. Micheli. Soccer injuries. Medicine and Sport Science. Vol. 49, pg. 140–169, 2005 https://doi.org/10.1159/000085395 [↩]
- C. Biz, P. Nicoletti, G. Baldin, N. L. Bragazzi, A. Crimì, P. Ruggieri. Hamstring strain injury (hsi) prevention in professional and semi-professional football teams: a systematic review and meta-analysis. International Journal of Environmental Research and Public Health. Vol. 18, pg. 8272, 2021 https://doi.org/10.3390/ijerph18168272 [↩] [↩]
- S. Mufty, P. Bollars, L. Vanlommel, K. Van Crombrugge, K. Corten, J. Bellemans. Injuries in male versus female soccer players: epidemiology of a nationwide study. Acta Orthopaedica Belgica. Vol. 81, pg. 289–295, 2015 [↩] [↩] [↩]
- F. J. Robles-Palazón, A. López-Valenciano, M. De Ste Croix, J. L. Oliver, A. García-Gómez, P. Sainz de Baranda, F. Ayala. Epidemiology of injuries in male and female youth football players: a systematic review and meta-analysis. Journal of Sport and Health Science. Vol. 11, pg. 681–695, 2022 https://doi.org/10.1016/j.jshs.2021.10.002 [↩] [↩]
- K. M. Cross, K. K. Gurka, S. Saliba, M. Conaway, J. Hertel. Comparison of hamstring strain injury rates between male and female intercollegiate soccer athletes. The American Journal of Sports Medicine. Vol. 41, pg. 742–748, 2013 https://doi.org/10.1177/0363546513475342 [↩] [↩]
- K. M. Cross, K. K. Gurka, S. Saliba, M. Conaway, J. Hertel. Comparison of hamstring strain injury rates between male and female intercollegiate soccer athletes. The American Journal of Sports Medicine. Vol. 41, pg. 742–748, 2013 https://doi.org/10.1177/0363546513475342 [↩]
- F. J. Robles-Palazón, A. López-Valenciano, M. De Ste Croix, J. L. Oliver, A. García-Gómez, P. Sainz de Baranda, F. Ayala. Epidemiology of injuries in male and female youth football players: a systematic review and meta-analysis. Journal of Sport and Health Science. Vol. 11, pg. 681–695, 2022 https://doi.org/10.1016/j.jshs.2021.10.002 [↩]
- D. A. Opar, M. D. Williams, A. J. Shield. Hamstring strain injuries: factors that lead to injury and re-injury. Sports Medicine (Auckland, N.Z.). Vol. 42, pg. 209–226, 2012 https://doi.org/10.2165/11594800-000000000-00000 [↩]
- G. Freckleton, T. Pizzari. Risk factors for hamstring muscle strain injury in sport: a systematic review and meta-analysis. British Journal of Sports Medicine. Vol. 47, pg. 351–358, 2013 https://doi.org/10.1136/bjsports-2011-090664 [↩] [↩]
- J. T. Hickey, D. A. Opar, L. J. Weiss, B. C. Heiderscheit. Hamstring strain injury rehabilitation. Journal of Athletic Training. Vol. 57, pg. 125–135, 2022 https://doi.org/10.4085/1062-6050-0707.20 [↩]
- M. Kjær, J. Petersen, M. R. Dünweber, J. L. Andersen, L. Engebretsen, S. P. Magnusson. Dilemma in the treatment of sports injuries in athletes: tendon overuse, muscle strain, and tendon rupture. Scandinavian Journal of Medicine & Science in Sports. Vol. 35, pg. e70026, 2025 https://doi.org/10.1111/sms.70026 [↩]
- W. S. A. Al Attar, M. A. Husain. Effectiveness of injury prevention programs with core muscle strengthening exercises to reduce the incidence of hamstring injury among soccer players: a systematic review and meta-analysis. Sports Health. Vol. 15, pg. 805–813, 2023 https://doi.org/10.1177/19417381231170815 [↩] [↩] [↩] [↩] [↩]
- K. M. Crossley, B. E. Patterson, A. G. Culvenor, A. M. Bruder, A. B. Mosler, B. F. Mentiplay. Making football safer for women: a systematic review and meta-analysis of injury prevention programmes in 11 773 female football (soccer) players. British Journal of Sports Medicine. Vol. 54, pg. 1089–1098, 2020 https://doi.org/10.1136/bjsports-2019-101587 [↩] [↩] [↩] [↩]
- W. K. Young, W. Briner, D. M. Dines. Epidemiology of common injuries in the volleyball athlete. Current Reviews in Musculoskeletal Medicine. Vol. 16, pg. 229–234, 2023 https://doi.org/10.1007/s12178-023-09826-2 [↩] [↩]
- T. Bere, J. Kruczynski, N. Veintimilla, Y. Hamu, R. Bahr. Injury risk is low among world-class volleyball players: 4-year data from the fivb injury surveillance system. British Journal of Sports Medicine. Vol. 49, pg. 1132–1137, 2015 https://doi.org/10.1136/bjsports-2015-094959 [↩] [↩] [↩] [↩] [↩]
- A. de Azevedo Sodré Silva, L. B. Sassi, T. B. Martins, F. S. de Menezes, F. Migliorini, N. Maffulli, R. Okubo. Epidemiology of injuries in young volleyball athletes: a systematic review. Journal of Orthopaedic Surgery and Research. Vol. 18, pg. 748, 2023 https://doi.org/10.1186/s13018-023-04224-3 [↩] [↩]
- P. M. Lee, E. M. Snyder, K. K. Obana, D. Trofa, L. Lee, J. You. Prevalence of upper extremity volleyball injuries within different adult age groups: a comprehensive analysis of national data from 2013-2022. Orthopaedic Journal of Sports Medicine. Vol. 12, pg. 23259671241298586, 2024 https://doi.org/10.1177/23259671241298586 [↩]
- 16, pg. 229–234, 2023 https://doi.org/10.1007/s12178-023-09826-2 [↩]
- T. Bere, J. Kruczynski, N. Veintimilla, Y. Hamu, R. Bahr. Injury risk is low among world-class volleyball players: 4-year data from the fivb injury surveillance system. British Journal of Sports Medicine. Vol. 49, pg. 1132–1137, 2015 https://doi.org/10.1136/bjsports-2015-094959 [↩]
- A. de Azevedo Sodré Silva, L. B. Sassi, T. B. Martins, F. S. de Menezes, F. Migliorini, N. Maffulli, R. Okubo. Epidemiology of injuries in young volleyball athletes: a systematic review. Journal of Orthopaedic Surgery and Research. Vol. 18, pg. 748, 2023 https://doi.org/10.1186/s13018-023-04224-3 [↩]
- P. M. Lee, E. M. Snyder, K. K. Obana, D. Trofa, L. Lee, J. You. Prevalence of upper extremity volleyball injuries within different adult age groups: a comprehensive analysis of national data from 2013-2022. Orthopaedic Journal of Sports Medicine. Vol. 12, pg. 23259671241298586, 2024 https://doi.org/10.1177/23259671241298586). [↩]
- A. Zech, K. Hollander, A. Junge, S. Steib, A. Groll, J. Heiner, F. Nowak, D. Pfeiffer, A. L. Rahlf. Sex differences in injury rates in team-sport athletes: a systematic review and meta-regression analysis. Journal of Sport and Health Science. Vol. 11, pg. 104–114, 2022 https://doi.org/10.1016/j.jshs.2021.04.003 [↩]
- A. Chandran, S. N. Morris, L. B. Lempke, A. J. Boltz, H. J. Robison, C. L. Collins. Epidemiology of injuries in national collegiate athletic association women’s volleyball: 2014-2015 through 2018-2019. Journal of Athletic Training. Vol. 56, pg. 666–673, 2021 https://doi.org/10.4085/1062-6050-679-20 [↩] [↩] [↩]
- A. Haupenthal, T. Bufon, M. C. Dos Santos, L. M. Matte, E. Dell’Antonio, F. M. Franco, N. C. P. do Amaral, L. Dos Santos Costa, G. S. Nunes. Injuries and complaints in the brazilian national volleyball male team: a case study. BMC Sports Science, Medicine & Rehabilitation. Vol. 15, pg. 77, 2023 https://doi.org/10.1186/s13102-023-00687-3 [↩]
- O. Kilic, M. Maas, E. Verhagen, J. Zwerver, V. Gouttebarge. Incidence, aetiology and prevention of musculoskeletal injuries in volleyball: a systematic review of the literature. European Journal of Sport Science. Vol. 17, pg. 765–793, 2017 https://doi.org/10.1080/17461391.2017.1306114 [↩]
- A. J. de Vries, H. van der Worp, R. L. Diercks, I. van den Akker-Scheek, J. Zwerver. Risk factors for patellar tendinopathy in volleyball and basketball players: a survey-based prospective cohort study. Scandinavian Journal of Medicine & Science in Sports. Vol. 25, pg. 678–684, 2015 https://doi.org/10.1111/sms.12294 [↩]
- A. De Vries, H. Van Der Worp, R. Diercks, I. Van Den Akker-Scheek, J. Zwerver. 26 risk factors for patellar tendinopathy: a survey- based prospective cohort study. in Abstracts pg. A17–A18, BMJ Publishing Group Ltd and British Association of Sport and Exercise Medicine, 2014 https://doi.org/10.1136/bjsports-2014-094114.26 [↩]
- A. Chandran, S. N. Morris, L. B. Lempke, A. J. Boltz, H. J. Robison, C. L. Collins. Epidemiology of injuries in national collegiate athletic association women’s volleyball: 2014-2015 through 2018-2019. Journal of Athletic Training. Vol. 56, pg. 666–673, 2021 https://doi.org/10.4085/1062-6050-679-20 [↩]
- C. M. Baugh, G. S. Weintraub, A. J. Gregory, A. Djoko, T. P. Dompier, Z. Y. Kerr. Descriptive epidemiology of injuries sustained in national collegiate athletic association men’s and women’s volleyball, 2013-2014 to 2014-2015. Sports Health. Vol. 10, pg. 60–69, 2018 https://doi.org/10.1177/1941738117733685 [↩] [↩] [↩]
- A. Theodorou, G. Komnos, M. Hantes. Patellar tendinopathy: an overview of prevalence, risk factors, screening, diagnosis, treatment and prevention. Archives of Orthopaedic and Trauma Surgery. Vol. 143, pg. 6695–6705, 2023 https://doi.org/10.1007/s00402-023-04998-5 [↩] [↩]
- D. Y. Gaitonde, A. Ericksen, R. C. Robbins. Patellofemoral pain syndrome. American Family Physician. Vol. 99, pg. 88–94, 2019 [↩]
- A. M. Cools, A. G. Maenhout, F. Vanderstukken, P. Declève, F. R. Johansson, D. Borms. The challenge of the sporting shoulder: from injury prevention through sport-specific rehabilitation toward return to play. Annals of Physical and Rehabilitation Medicine. Vol. 64, pg. 101384, 2021 https://doi.org/10.1016/j.rehab.2020.03.009 [↩] [↩] [↩]
- B. Forthomme, V. Wieczorek, A. Frisch, J.-M. Crielaard, J.-L. Croisier. Shoulder pain among high-level volleyball players and preseason features. Medicine and Science in Sports and Exercise. Vol. 45, pg. 1852–1860, 2013 https://doi.org/10.1249/MSS.0b013e318296128d [↩]
- A. M. Cools, F. R. Johansson, D. Borms, A. Maenhout. Prevention of shoulder injuries in overhead athletes: a science-based approach. Brazilian Journal of Physical Therapy. Vol. 19, pg. 331–339, 2015 https://doi.org/10.1590/bjpt-rbf.2014.0109 [↩]
- E. E. Heming, E. S. Gibson, K. B. Friesen, C. L. Martin, M. Martin, M. Asker, C. Blauwet, G. S. Bullock, H. Fredriksen, J.-M. Galarneau, K. A. Hayden, J. H. Lee, A. B. Mosler, G. Myklebust, B. M. Pluim, J. S. Thornton, J. L. Whittaker, R. Whiteley, K. M. Crossley, M. Møller, C. A. Emery. Prevention strategies and modifiable risk factors for upper extremity injury: a systematic review and meta-analysis for the female, woman and/or girl athlete injury prevention (fair) consensus. British Journal of Sports Medicine. Vol. 59, pg. 1587–1598, 2025 https://doi.org/10.1136/bjsports-2025-109907 [↩] [↩] [↩]
- A. Scott, C. Nordin. Do dietary factors influence tendon metabolism? Advances in Experimental Medicine and Biology. Vol. 920, pg. 283–289, 2016 https://doi.org/10.1007/978-3-319-33943-6_27 [↩]
- A. Hijlkema, C. Roozenboom, M. Mensink, J. Zwerver. The impact of nutrition on tendon health and tendinopathy: a systematic review. Journal of the International Society of Sports Nutrition. Vol. 19, pg. 474–504, 2022 https://doi.org/10.1080/15502783.2022.2104130 [↩] [↩]
- N. N. DePhillipo, Z. S. Aman, M. I. Kennedy, J. P. Begley, G. Moatshe, R. F. LaPrade. Efficacy of vitamin c supplementation on collagen synthesis and oxidative stress after musculoskeletal injuries: a systematic review. Orthopaedic Journal of Sports Medicine. Vol. 6, pg. 2325967118804544, 2018 https://doi.org/10.1177/2325967118804544 [↩]
- C. Lorincz, S. L. Manske, R. Zernicke. Bone health: part 1, nutrition. Sports Health. Vol. 1, pg. 253–260, 2009 https://doi.org/10.1177/1941738109334213 [↩] [↩] [↩] [↩]
- L. S. Tabatabai, D. E. Sellmeyer. Nutritional supplements and skeletal health. Current Osteoporosis Reports. Vol. 19, pg. 23–33, 2021 https://doi.org/10.1007/s11914-020-00651-x [↩]
- C. M. Swanson, W. M. Kohrt, O. M. Buxton, C. A. Everson, K. P. Wright, E. S. Orwoll, S. A. Shea. The importance of the circadian system & sleep for bone health. Metabolism: Clinical and Experimental. Vol. 84, pg. 28–43, 2018 https://doi.org/10.1016/j.metabol.2017.12.002 [↩] [↩]
- K. Huang, J. Ihm. Sleep and injury risk. Current Sports Medicine Reports. Vol. 20, pg. 286–290, 2021 https://doi.org/10.1249/JSR.0000000000000849 [↩]
- T. Grier, E. Dinkeloo, M. Reynolds, B. H. Jones. Sleep duration and musculoskeletal injury incidence in physically active men and women: a study of u.s. army special operation forces soldiers. Sleep Health. Vol. 6, pg. 344–349, 2020 https://doi.org/10.1016/j.sleh.2020.01.004 [↩] [↩]
- T. Zhou, X. Dai, Y. Yuan, Q. Xue, X. Li, M. Wang, H. Ma, Y. Heianza, L. Qi. Adherence to a healthy sleep pattern is associated with lower risks of incident falls and fractures during aging. Frontiers in Immunology. Vol. 14, pg. 1234102, 2023 https://doi.org/10.3389/fimmu.2023.1234102 [↩]
- H. Yang, B. Li, H. Li, M. Zhou, B. Li, J. Guo, H. Zhong, S. Liu, Q. Zhang, C. Xing, G. Ning. The independent and joint association between physical activity, sleep duration and daily sitting time with bone mineral density: a real world study from nhanes 2007-2018. Bone. Vol. 189, pg. 117264, 2024 https://doi.org/10.1016/j.bone.2024.117264 [↩] [↩] [↩]



{kind=link}
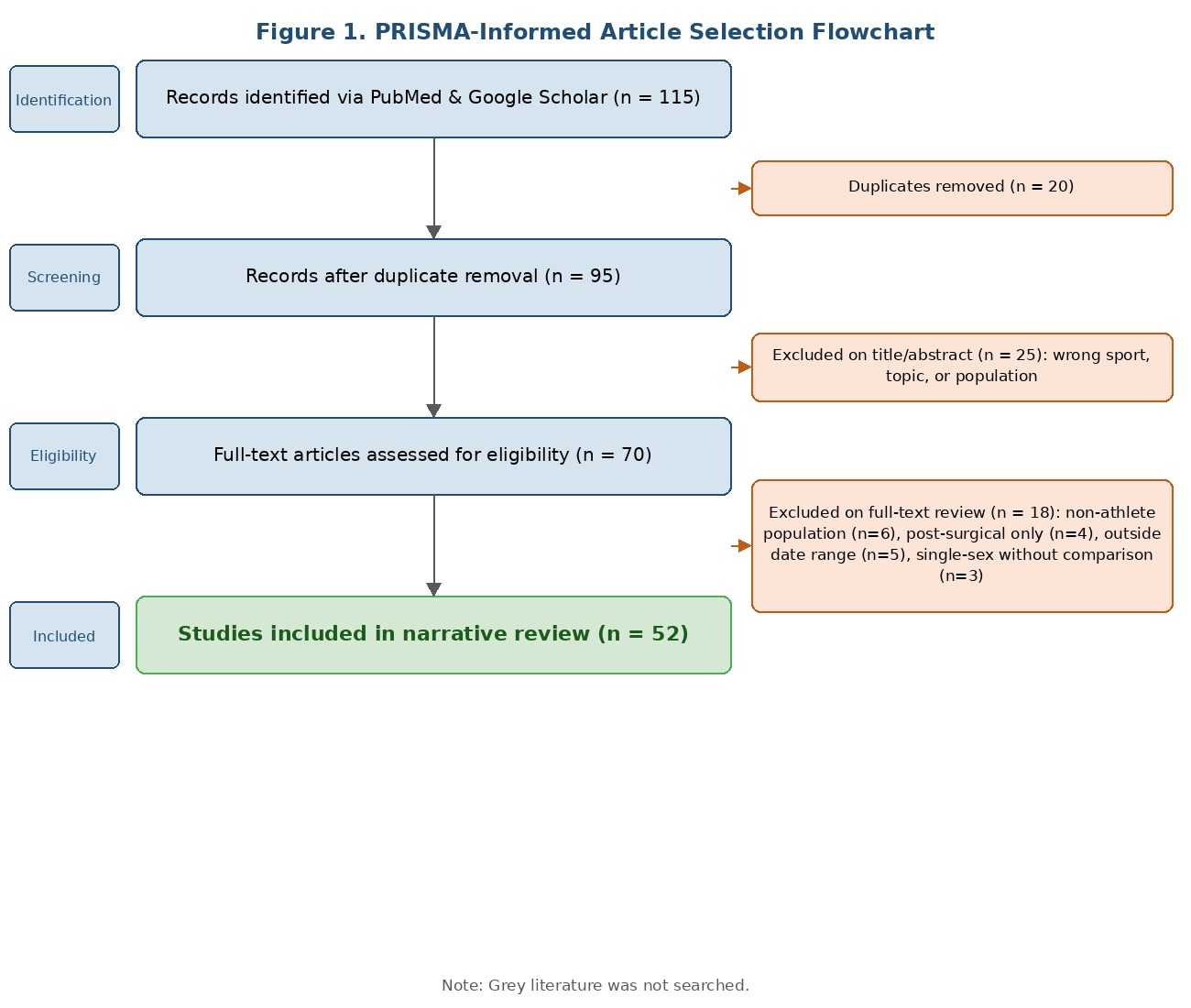{kind=link}