
Abstract
Family-Centered Care (FCC) and Family-Integrated Care (FIC) have become increasingly recognized as essential approaches to neonatal intensive care unit (NICU) management globally. FCC emphasizes collaboration between healthcare providers and families to enhance infant outcomes, while FIC actively involves parents in daily infant care routines. This study examines trends in FCC and FIC over the past decade across multiple countries, including Canada, the United States, Australia, and China, with a focus on applicability in Fresno County, California. Twenty-five peer-reviewed studies from 2010 to 2025 were analyzed, highlighting improvements in infant growth, higher breastfeeding rates, reduced parental stress, and decreased hospital stays. To evaluate local awareness of FIC/FCC, a survey was conducted among 50 healthcare providers in the Central Valley, yielding 32 responses (64% response rate). Results indicated that 34% of respondents were very familiar with FIC/FCC concepts, and 59% considered family involvement extremely important. Technology played a significant role, with 69% of respondents utilizing tools like video calls and mobile apps to support family engagement. Barriers included family availability (78%), resource constraints (72%), and staff training needs (44%). Findings suggest that while FCC and FIC are widely supported globally, surveyed providers demonstrated varying levels of awareness and perceived barriers, and technology can mitigate resource and logistical challenges. Expanding education, digital tools, and awareness can improve outcomes for infants and families in the region.
Keywords: Family-Centered Care, Family-Integrated Care, Neonatal Intensive Care Unit, parental involvement, healthcare technology, Central Valley, California
Introduction
Family involvement in neonatal care is critical for infant health, parental well-being, and the overall functioning of NICUs. Family-Centered Care (FCC) promotes active collaboration between healthcare providers and families, emphasizing communication, shared decision-making, and psychological support1.
FCC emerged as an approach designed to strengthen partnerships between healthcare providers and families with the goal to improve both infant outcomes and parental wellbeing2. According to Ortenstrand et al., 2010, early clinical research showed that implementing family-centered neonatal care models can significantly reduce infant length of stay while maintaining positive clinical outcomes3. Additionally, research examining family satisfaction in pediatric and neonatal intensive care environments indicates that FCC practices contribute to improved parental perceptions of care quality and communication with healthcare providers4. Yet another strength that has been reported in European studies associated with FCC involves parent–infant bonding and greater parental engagement in neonatal care activities5.
Family-Integrated Care (FIC) extends FCC by embedding parents directly into daily care routines, fostering bonding and confidence while improving neonatal outcomes6. Recent studies have shown that FIC programs enhance parental participation and improve infant feeding outcomes in NICU settings7. Over the past decade, FCC and FIC have been implemented in various healthcare systems worldwide, including the United States, Canada, Australia, and China, often complemented by technological solutions such as mobile apps and telehealth.
This study explores how FCC and FIC are understood and practiced within healthcare settings in California’s Central Valley. The project focuses on healthcare provider perspectives, the extent of family involvement in care, and factors that may influence how these approaches are applied in local settings. By analyzing survey responses from providers in the region, the study aims to describe current practices and provide insight into how FCC and FIC are experienced in this environment.
The study aims to review global research on FCC and FIC practices in NICUs over the past decade, assess local adoption and provider familiarity in Fresno County, and identify barriers and facilitators of implementation of FCC/FIC in local settings.
The study focuses on the healthcare environment in the Central Valley and global NICU research published between 2010 and 2025. Survey respondents included physicians, pediatricians, nurses, and specialists in the region. Limitations include a modest sample size (n=32), and potential response bias owing to convenience sampling.
The study is grounded in the Social Support Theory8. emphasizing the interdependent relationship between infant outcomes and parental involvement. FCC and FIC operationalize this framework by promoting active participation and shared responsibility for neonatal care9.
Methods
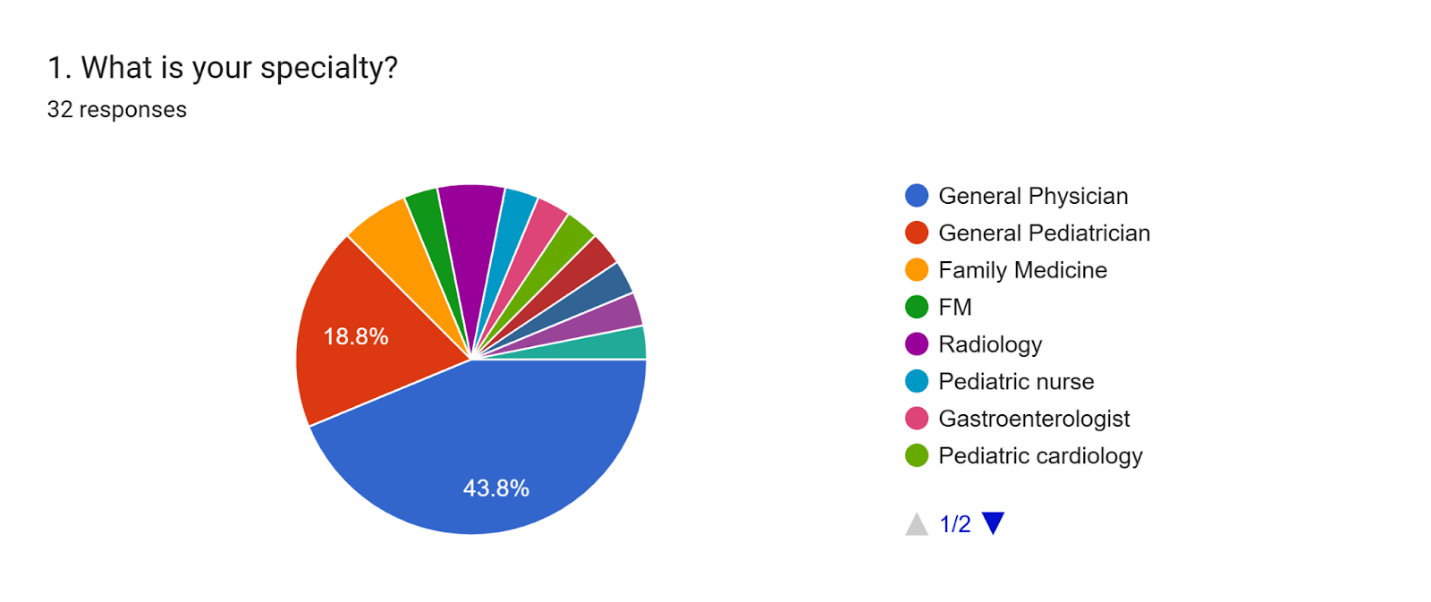
The study employed a combination of literature review and cross-sectional survey. A literature review analyzed global trends in FCC/FIC implementation, and a cross-sectional survey assessed local adoption and perspectives in the Central Valley of California. Fifty healthcare professionals were identified through publicly available hospital directories using convenience sampling from regional hospital websites (Clovis Regional Medical Center, Valley Children’s Hospital, St. Agnes, Kaiser Permanente). Thirty-two responses were received (64%), including general physicians (43.8%), pediatricians (18.8%), family medicine practitioners (9.4%), and other specialists (See Table 1 for distribution). There were 18 non-respondents; non-respondents may differ systematically from respondents in workload or engagement with FCC/FIC practices, potentially introducing non-response bias.
| Specialty | Number of Respondents | Percentage |
| Family Medicine | 3 | 9.4% |
| Gastroenterologist | 1 | 3.1% |
| General Pediatrician | 6 | 18.8% |
| General Physician | 14 | 43.8% |
| Geriatrics | 1 | 3.1% |
| Nephrologist | 1 | 3.1% |
| Pediatric Cardiology | 1 | 3.1% |
| Pediatric Nurse | 1 | 3.1% |
| Psychiatrist | 1 | 3.1% |
| Pulmonologist | 1 | 3.1% |
| Radiologist | 2 | 6.3% |
| Total | 32 | 100% |
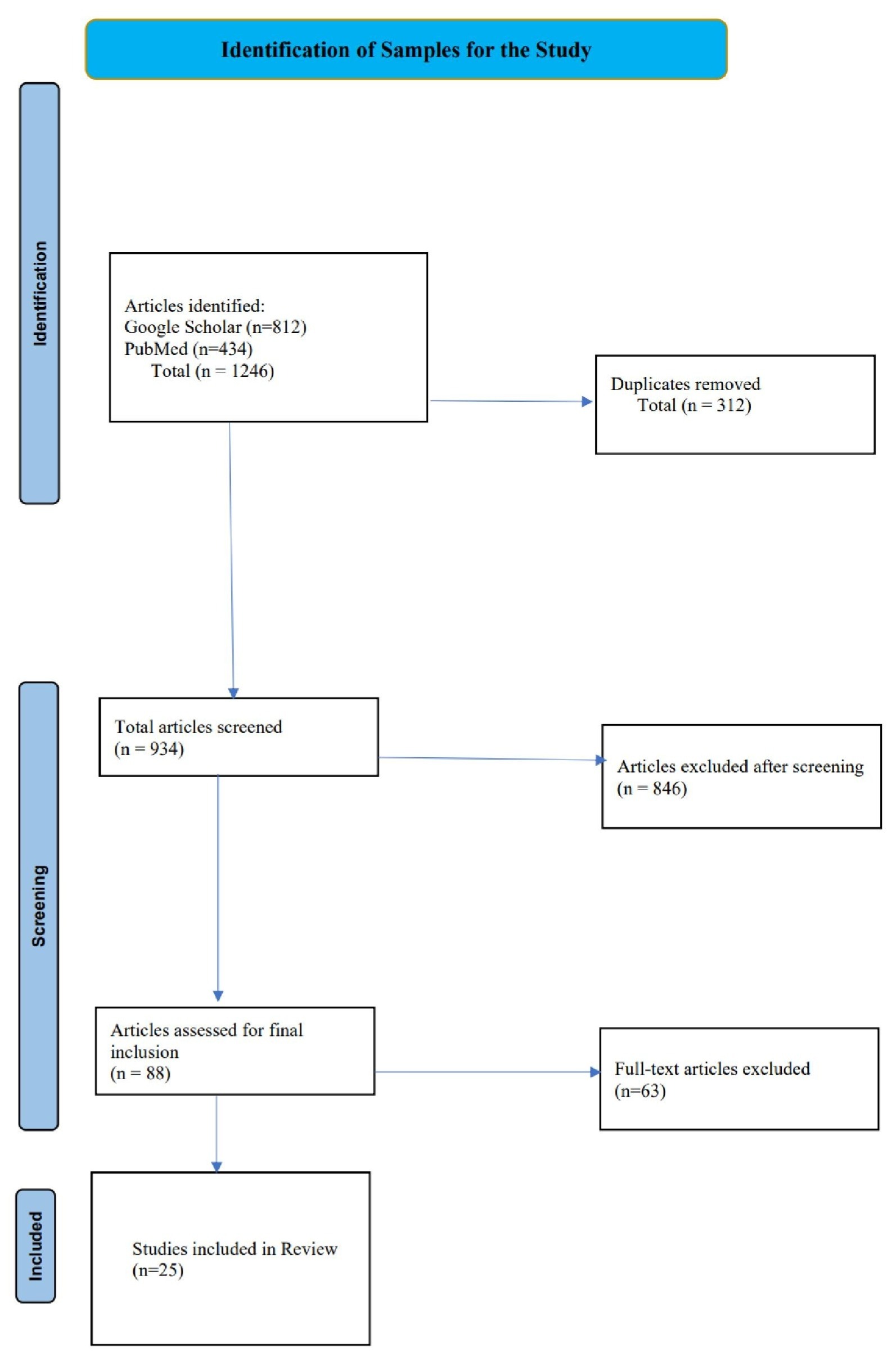
Literature Review: A structured literature search was conducted during the period August 2024–December 2025 using two large databases, Google Scholar and PubMed. See Figure 1 PRISMA workflow. The search terms utilized were: (“family integrated care” OR “family-centered care” OR FICare OR FCC) AND (NICU OR neonatal OR preterm infant) AND (family involvement OR parental participation OR technology). Peer‑reviewed studies between 2010 and 2025 were searched. Database searches identified 1,246 articles (Google Scholar n=812; PubMed n=434). After removing duplicates (n=312), 934 articles were screened by title and abstract. If the studies involved editorials, conference abstracts, non‑NICU studies, or lacked measurable outcomes, they were excluded. A total of 846 articles were excluded. Then, out of the 88 studies remaining, 25 were included based on the global nature/scale of the study, completeness, and relevance to the current study. The key findings from these studies were then tabulated for comparison.
Local Survey: The local survey, administered via email, included nine multiple-choice questions regarding FIC/FCC familiarity, family participation, use of technology, and barriers to implementation (See Appendix A for Survey details). Key variables included provider familiarity with FIC/FCC (very familiar, slightly familiar, not familiar), perceived importance of family involvement (extremely important, somewhat important, neutral), frequency of family participation (always, sometimes, rarely), comfort with increasing family involvement (very comfortable, somewhat comfortable, neutral), use and support of technology in family care (yes/no; strong support, support, neutral), and barriers to implementation (family availability, resource constraints, staff training, space limitations). Quantitative survey data collected were analyzed descriptively using frequencies and percentages.
Survey links were emailed to participants with a brief introduction explaining the study purpose. The survey was administered using Google Forms and distributed via email to selected healthcare professionals. A total of two reminder emails were sent during the two-week data collection period to improve response rates. All survey questions were multiple-choice, and all 32 responses received were complete, with no missing data; therefore, no responses were excluded from analysis. The survey was conducted anonymously, and no identifying information such as names, email addresses, or IP addresses was collected. Responses were automatically recorded in Google Forms and exported to Microsoft Excel for organization and descriptive statistical analysis. There was no formal IRB review. This study involved an anonymous survey with voluntary participation, and did not collect identifiable personal information.
For comparison purposes, Table 2 lists the global vs. local outcome variables that are explored in the study.
| Global Outcome Variables (Literature Review) | Local Survey Variables (Survey) |
| Infant weight gain | Reported barriers (resources, training, family availability, space) |
| Breastfeeding rates | Familiarity with FCC/FIC |
| Length of hospital stay | Comfort with family involvement |
| Parental stress levels | Perceived importance of family input |
| Communication outcomes | Family participation in daily decisions |
| Family engagement in care | Technology use in practice |
| Use of technology in care | Support for digital tools |
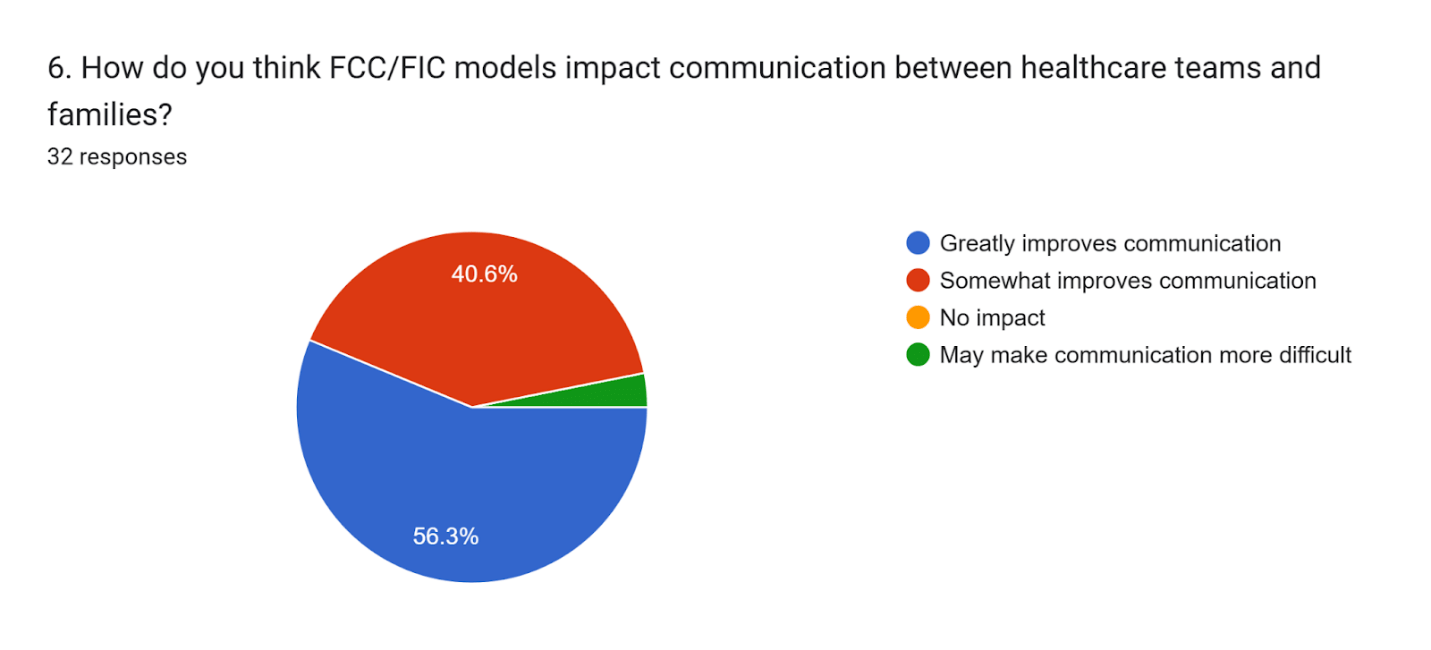
| Readmission rates | Perceived impact on communication |
Results
Analysis of twenty-five global studies (2010–2025) revealed consistent benefits of FCC and FIC (See Table 3). Technology was included in all studies in Table 3. The main benefits are summarized below, together with the corresponding studies that reported them:
- Reduced parental stress and anxiety16,5,8,10,11,14,15,17,18,12,19,20,13.
- Shorter hospital stays1,3,21,22.
| Study | Country | Sample Size | Design | Key Outcomes | Technology |
| O’Brien et al., 201310 | Canada | 42 infants | Cohort | Improved weight gain; higher breastfeeding rates | Yes |
| O’Brien et al., 201523 | Canada & Australia | 675 infants | Cluster RCT | Weight gain; reduced parental stress | Yes |
| Ding et al., 20196 | International | 19 studies | Meta-analysis | Weight gain; higher parent satisfaction | Yes |
| Franck et al., 201914,15 | USA | 225 infants | Quasi-experimental | Reduced parental stress; higher breastfeeding | Yes |
| Vetcho et al., 202021 | International | 48 studies | Integrative review | Improved parental satisfication | Yes |
| Murphy et al., 202122 | Canada | 718 infants | Cluster RCT | NICU stay reduced | Yes |
| North et al., 202217 | International | 5240 infants | Systematic review | Better growth and parental involvement | Yes |
| Waddington et al., 20219 | International | 15 studies | Literature Review | Improved feeding and parent mental health | Yes |
| Hriberšek et al., 202424 | Global | 4,836 publications | Bibliometric | Growth of FCC research globally | Yes |
| Loutfy et al., 20248 | Egypt | 223 parents | Quantitative | Lower parental stress scores | Yes |
| Lee, 202425 | South Korea | 10 studies | Review | Evidence-based FCC practice models | Yes |
| Arun Babu & Bhat, 202418 | India | 7 studies | Literature Review | Strong support for parental integration | Yes |
| Hodgson et al., 202512 | International | 20 studies | Systematic review | Improved infant and family outcomes | Yes |
| Moreno-Sanz et al., 202526 | International | 18 studies | Review | Future directions for FICare | Yes |
| Gooding et al., 20112 | International | Numerous | Observational | Improved developmental outcomes | Yes |
| Ortenstrand et al., 20103 | Sweden | 366 infants | RCT | Reduced length of stay | Yes |
| O’Brien et al., 20187 | Canada, Australia, & New Zealand | 1786 infants | Cluster-RCT | Improved infant weight gain | Yes |
| van Veenendaal et al., 20225 | Netherlands | 296 mothers | Multicenter | Improved bonding; less maternal stress | Yes |
| Latour et al., 20244 | International | 16 articles | Mixed | Future directions on FCC | Yes |
| Çimke et al., 20241 | International | 2525 studies | Bibliometric | Expansion of FCC research | Yes |
| Hodgson et al., 202412 | United States, Canada, Korea, Indonesia, Iran, Switzerland | 3,801 parents across 16 studies | Systematic review | Improved parental satisfaction, communication, emotional support | Yes |
| Ranu et al., 202415 | United States | 8 parents and 13 team providers | Qualitative | Higher breastfeeding, and shared decision-making | Yes |
| Park & Im, 202519 | South Korea | 3 Parents, 9 healthcare providers | Qualitative study | Stronger communication, increased overall familial engagement in care | Yes |
| Traylor & Ohning, 202420 | United States | 320 patient rounding events | Observational study | Improvement in teamwork and communication | Yes |
| Bellizzi et al., 202427 | International | 41 articles | Systematic review | Improved newborn outcomes, parental engagement | Yes |
FCC = Family centered care, FIC = Family integrated care.
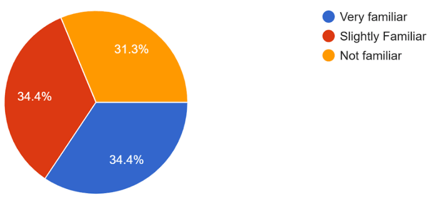
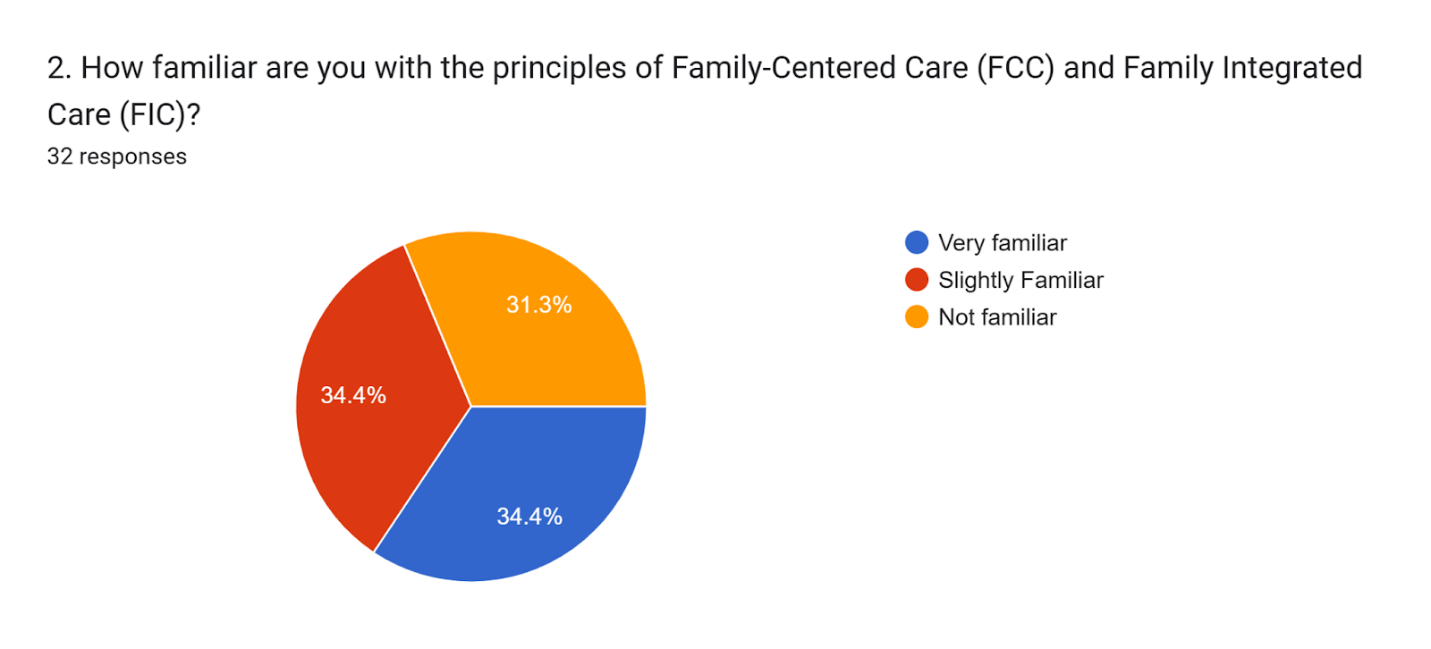
Survey findings indicated that 11 respondents (34%; 95% CI, 18% to 51%) were very familiar with FIC/FCC, 11 (34%; 95% CI, 18% to 51%) slightly familiar, and 10 (31%; 95% CI, 15% to 47%) not familiar. See Figure 2.
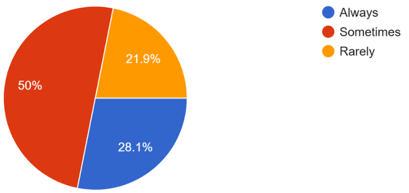
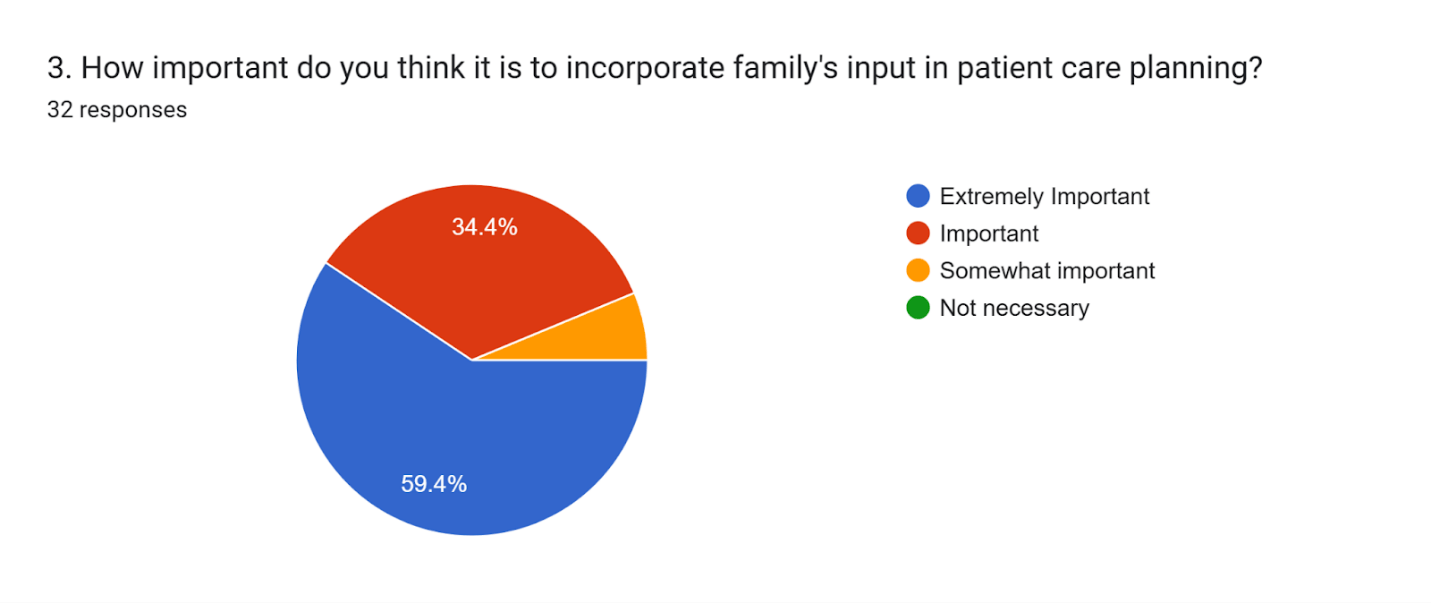
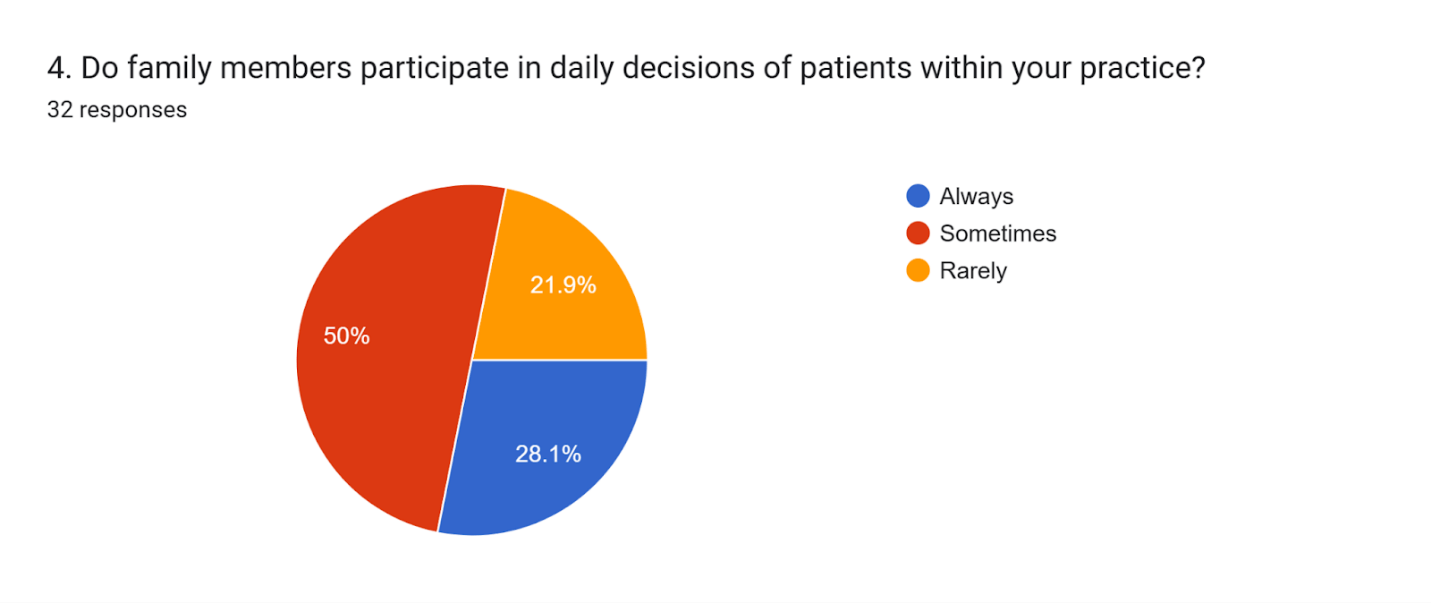
Nineteen respondents (59%; 95% CI, 39% to 73%) considered family involvement extremely important, and only two (6%; 95% CI, 1% to 14%) considered it somewhat important. Family participation in daily decision-making was reported as always by 9 (28%; 95% CI, 12% to 43%), sometimes by 16 (50%; 95% CI, 32% to 67%), and rarely by 7 (22%; 95% CI, 7% to 36%). See Figure 3.
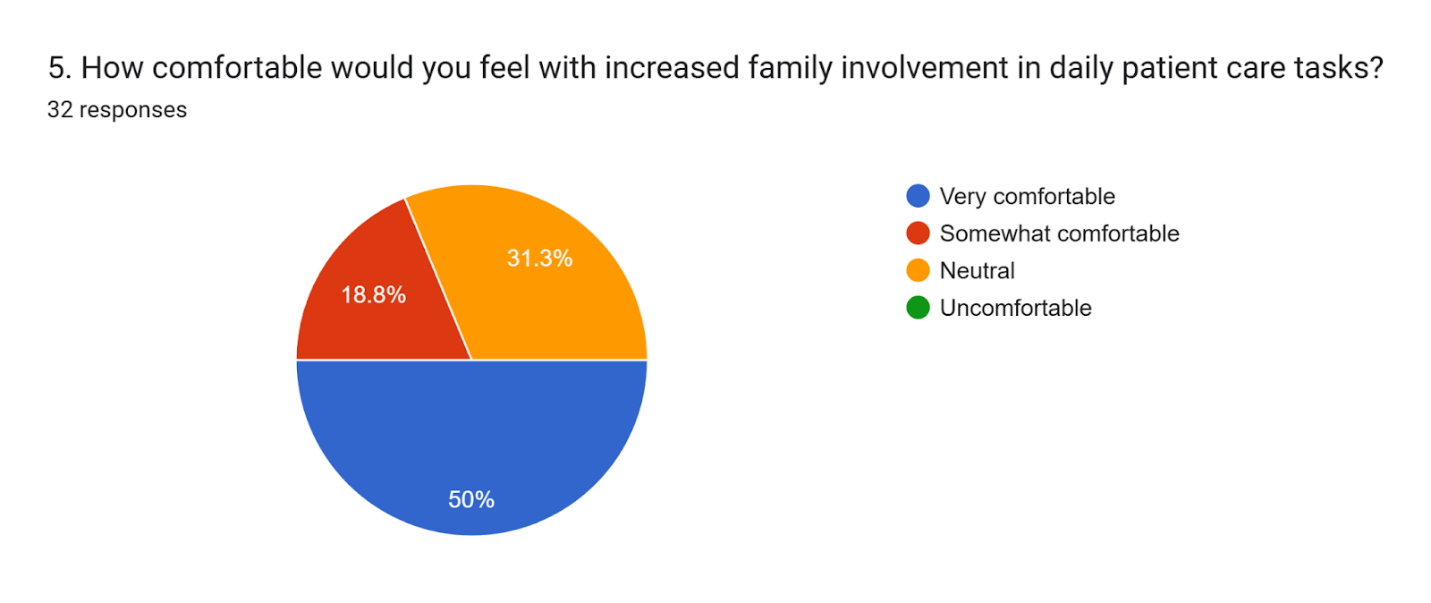
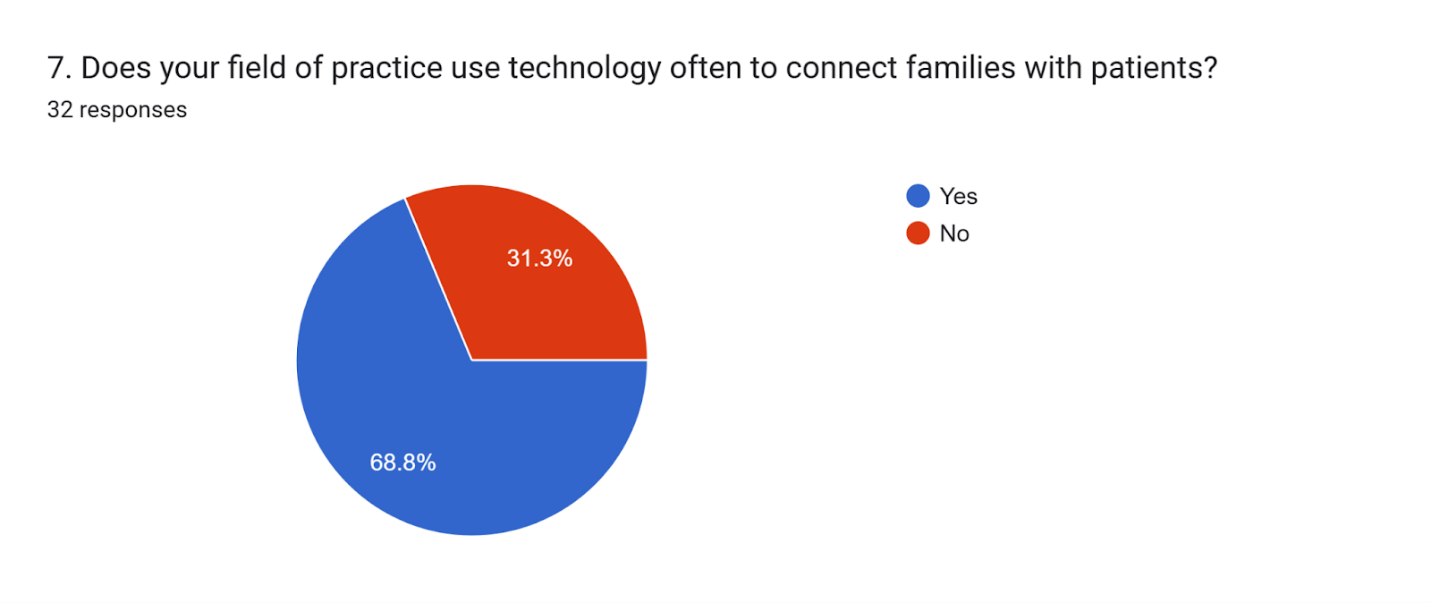
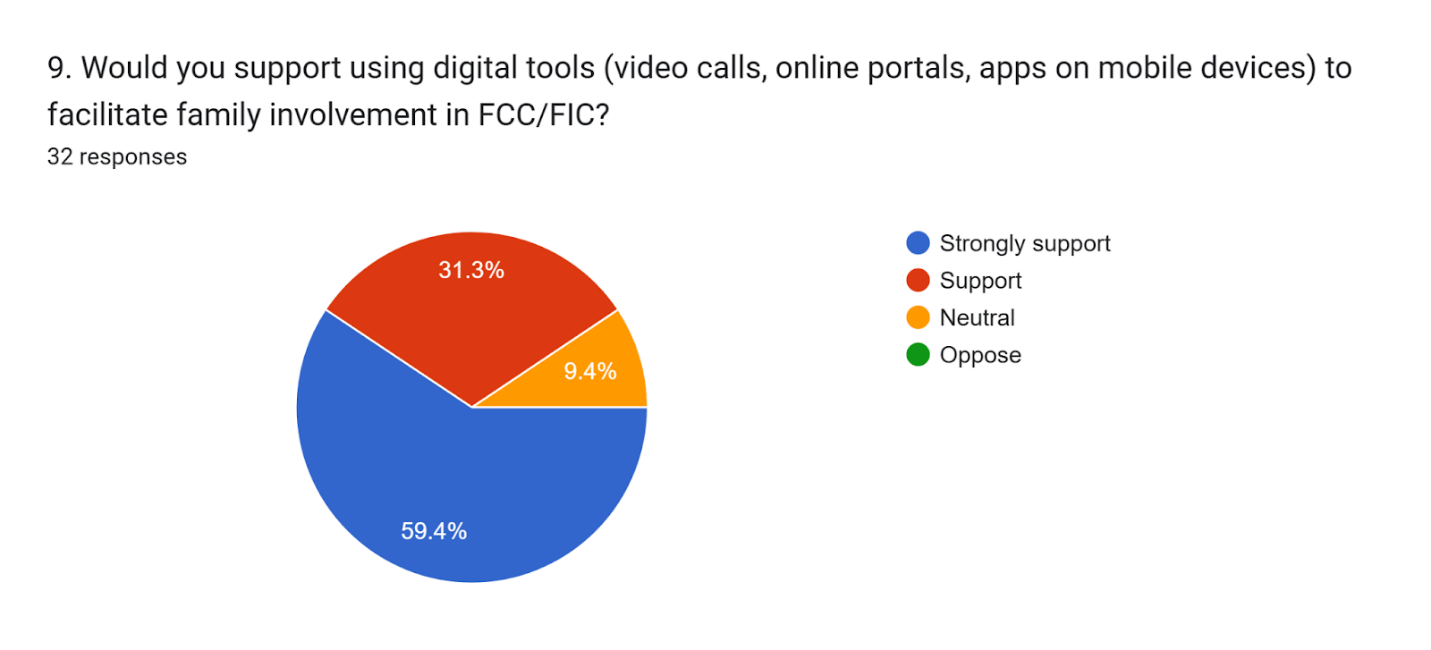
Comfort with increasing family involvement was reported as very comfortable by 16 (50%; 95% CI, 33% to 67% ), somewhat comfortable by 6 (19%; 95% CI, 4% to 34%), and neutral by 10 (31%; 95% CI, 15% to 47%). Technology use was reported by 22 respondents (69%; 95% CI, 52% to 84%), and 19 (59%; 95% CI, 42% to 76%) strongly supported the expansion of digital tools in FCC/FIC programs.
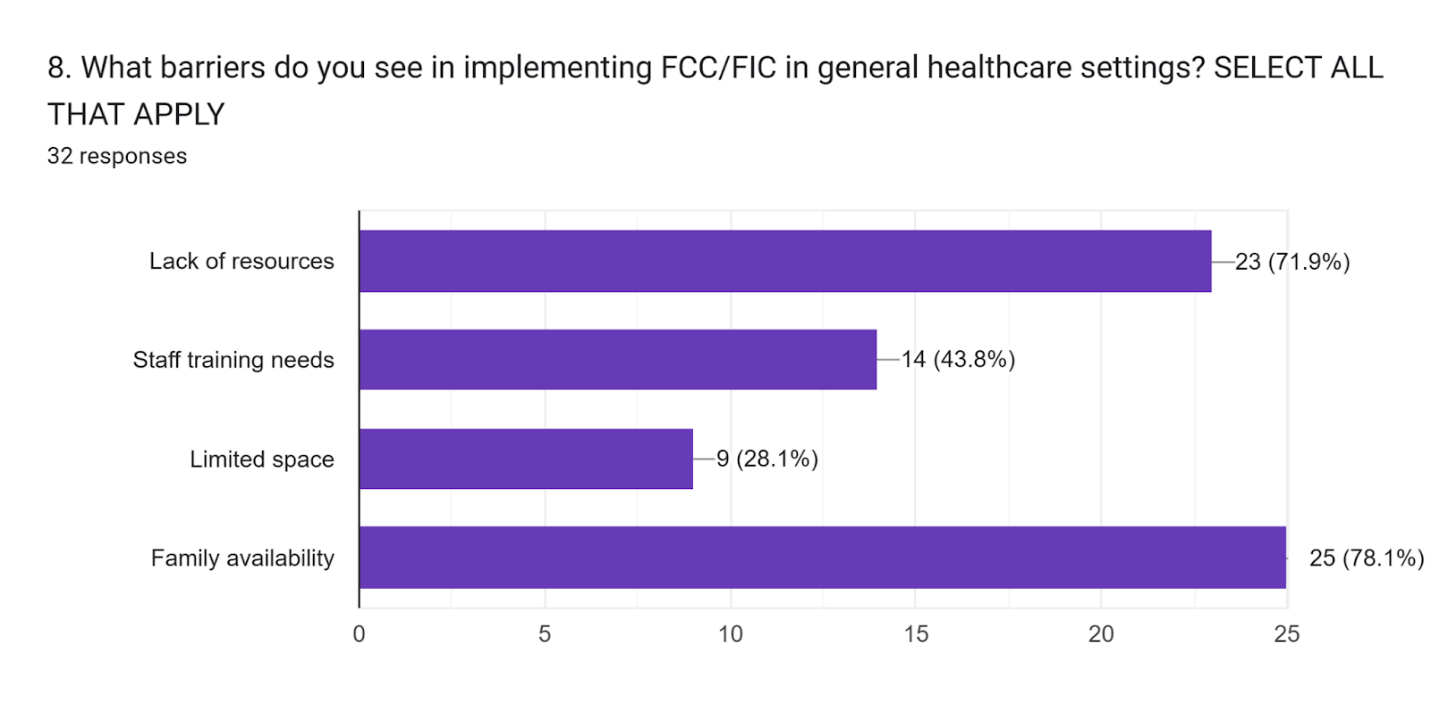
Barriers included family availability (78%; 95% CI, 62% to 93%), lack of resources (72%; 95% CI, 58% to 88%), staff training needs (44%; 95% CI, 26% to 61%), and limited space (28%; 95% CI, 12% to 43%). See Table 4.
(The complete survey questionnaire and results are presented in Appendix A.)
| Barrier | Number of Respondents | Percentage |
| Family Availability | 25 | 78% |
| Lack of Resources | 23 | 72% |
| Staff Training Needs | 14 | 44% |
| Limited Space | 9 | 28% |
Discussion
The global studies used in this research demonstrate strong benefits of FCC and FIC, including enhanced infant growth, higher breastfeeding rates, and reduced parental stress. More recent research conducted between 2024 and 2025 on FCC and FIC further supports these findings, adding greater rigor and contemporary relevance to the evidence base12,18,26.
Locally, some of the relationships between key survey variables were examined in more detail. The providers who reported being “very familiar” with FCC/FIC were more likely to report being “very comfortable” with increased family involvement, suggesting a positive relationship between familiarity and confidence. Further, there were some noticeable differences across specialties; for instance, general physicians most frequently reported lack of resources and staff training as barriers, while family availability was identified across nearly all roles. In smaller specialties such as psychiatry and nephrology, family availability was often the primary barrier, while radiology respondents more commonly reported staff training needs. In addition, respondents who reported using technology in their practice were also more likely to support expanding digital tools.
Further, survey results show that while Central Valley providers value family involvement, awareness and perceived readiness vary due to resource, training, and space constraints. Technology is widely supported as a facilitator of family participation. These findings indicate that FCC and FIC principles can improve healthcare outcomes in rural and semi-urban settings when supported by digital tools and staff training. The study results support broader adoption of family-centered approaches beyond NICUs to pediatric and geriatric care24,25.
All research objectives were addressed: global trends were reviewed, local adoption assessed, barriers identified, and the role of technology highlighted. Recommendations include implementing targeted staff training on FIC/FCC principles, increasing access to digital tools for remote family engagement, conducting follow-up research including family perspectives, and exploring expansion of FCC/FIC models to adult and geriatric care.
Based on the barriers identified among surveyed providers, more specific and actionable strategies can be proposed. To address family availability, healthcare systems could implement scheduled virtual visitation options, such as video calls during rounds or designated update times, allowing families to participate despite time or location constraints. To address staff training needs, institutions could develop structured FCC/FIC training modules and workshops to improve provider familiarity and confidence. For resource constraints, hospitals could allocate funding toward family engagement programs, including digital communication platforms or designated staff roles. Additionally, to address space limitations, facilities could consider flexible visitation policies or adapting care environments to better accommodate family presence. These targeted strategies directly address the barriers identified in the local survey.
Limitations of this study include a small sample size (n=32). Perhaps, future studies can incorporate larger sample sizes so the results derived from the current study can be verified and strengthened.
To conclude, the systematic review of recent literature in FCC and FIC shows that integrating families into patient care and leveraging technology can greatly improve patient health outcomes. When families are included, they can better understand the patient’s condition and care plan. Further, using technology in healthcare also makes communication and monitoring easier. The Fresno County healthcare providers who participated in the survey showed limited familiarity with FCC/FIC concepts. However, they were willing to incorporating these approaches into their practice. Although survey participants reported certain barriers to implementation, these challenges can be addressed through appropriate measures, enabling the Fresno County patient care system to achieve improved patient outcomes comparable to those reported in the global literature.
Acknowledgments
I am very grateful to all the healthcare professionals in Fresno County, California who participated in the survey and contributed their valuable insights.
Appendix A. Survey
Email sent:
Hello, my name is Simran Rana, and I am a junior with a strong career interest in the medical field. Over the past year, I have been working on a research project focused on Family-Centered Care (FCC) and Family-Integrated Care (FIC), specifically exploring how the California Central Valley trends in FCC and FIC compare with the global trends.
As part of my study, I have created a brief survey for healthcare professionals in the region. I would greatly appreciate your time and input in completing this short survey. There are a total of 9 multiple choice questions and it should take about a minute of your time!
Thank you so much for your time and support!
Best Regards,
Simran Rana
Survey Questions & Results
References
- S. Çimke, D. Y. Gürkan, & S. Polat. Research on family-centered care in pediatric patients: a bibliometric analysis. Journal of Pediatric Nursing, 76, 199–206 (2024). [↩] [↩] [↩]
- J. S. Gooding, L. G. Cooper, A.I. Blaine, L. S. Franck, J.L. Howse, & S.D. Berns. Family support and family-centered care in the neonatal intensive care unit: Origins, advances, and challenges. Pediatrics, 127, e507–e517 (2011). [↩] [↩]
- A. Ortenstrand, B. Westrup, E.B. Broström, I. Sarman, S. Akerström, T. Brune & B. Jacobsson. The Stockholm Neonatal Family Centered Care Study: Effects on length of stay and infant outcomes. Pediatrics, 125, e278–e285 (2010). [↩] [↩] [↩]
- J.M. Latour, J.E. Rennick and A. van den Hoogen. Editorial: Family-centered care in pediatric and neonatal critical care settings. Front. Pediatr. 12:1402948. doi: 10.3389/fped.2024.1402948 (2024). [↩] [↩]
- N.R. van Veenendaal, A.A.M.W van Kempen, B.F.P. Broekman et al. Association of a Zero-Separation Neonatal Care Model With Stress in Mothers of Preterm Infants. JAMA Netw Open.;5(3):e224514. doi:10.1001/jamanetworkopen.2022.4514 (2022). [↩] [↩] [↩]
- X. Ding, L. Zhu, R. Zhang, L. Wang, T.T. Wang & J.M. Latour. Effects of family-centred care interventions on preterm infants and parents in neonatal intensive care units: a systematic review and meta-analysis of randomised controlled trials. Australian Critical Care, 32(1), 63–75 (2019). [↩] [↩] [↩]
- K. O’Brien, K. Robson, M. Bracht, M. Cruz, K. Lui, R. Alvaro, O. da Silva, et. al; FICare Study Group and FICare Parent Advisory Board. Effectiveness of Family Integrated Care in neonatal intensive care units on infant and parent outcomes: A multicentre, multinational, cluster‑randomised controlled trial. The Lancet Child & Adolescent Health, 2(4), 245–254 https://doi.org/10.1016/S2352‑4642(18)30039‑7 (2018). [↩] [↩] [↩]
- A. Loutfy, M.A. Zoromba, M.A. Mohamed et al. Family-centred care as a mediator in the relationship between parental nurse support and parental stress in neonatal intensive care units. BMC Nurs 23, 572. https://doi.org/10.1186/s12912-024-02258-4. (2024). [↩] [↩] [↩]
- C. Waddington, N.R., van Veenendaal, K. O’Brien, N. Patel & International Steering Committee for Family Integrated Care. Family integrated care: supporting parents as primary caregivers in the neonatal intensive care unit. Pediatric Investigation, 5(02), 148–154 (2021). [↩] [↩] [↩]
- K. O’Brien, M. Bracht, K. Macdonell, T. McBride, K. Robson, L. O’Leary, & S. K. Lee. A pilot cohort analytic study of Family Integrated Care in a Canadian neonatal intensive care unit. BMC Pregnancy and Childbirth, 13(Suppl 1), S12 (2013). [↩] [↩] [↩] [↩]
- K. O’Brien, M. Bracht, K. Robson, X.Y. Ye, L. Mirea, M. Cruz, & S. K. Lee. Evaluation of the Family Integrated Care model of neonatal intensive care: a cluster randomized controlled trial in Canada and Australia. BMC pediatrics, 15(1), 210 (2015). [↩] [↩] [↩]
- C. R. Hodgson, R. Mehra, & L.S. Franck. Infant and Family Outcomes and Experiences Related to Family-Centered Care Interventions in the NICU: A Systematic Review. Children, 12(3), 290 (2025). [↩] [↩] [↩] [↩] [↩]
- S. Bellizzi, C. M. P. Napodano, & P. Murgia. Family-centered care for newborns: A global perspective and review. Journal of Tropical Pediatrics, 70(5), fmae026. https://doi.org/10.1093/tropej/fmae026 (2024). [↩] [↩]
- L. S. Franck, R.M. Kriz, R. Bisgaard, D.M. Cormier, P. Joe, P.S. Miller, & Y. Sun. Comparison of family centered care with family integrated care and mobile technology (mFICare) on preterm infant and family outcomes: a multi-site quasi-experimental clinical trial protocol. BMC pediatrics, 19(1), 469 (2019). [↩] [↩] [↩]
- J. Ranu, J.L. Rosenthal et al. A qualitative intervention evaluation of neonatal virtual family-centered rounds. Hospital Pediatrics, 14(6), 463–473. https://doi.org/10.1542/hpeds.2023-007554 (2024). [↩] [↩] [↩] [↩]
- J.M. Latour, J.E. Rennick and A. van den Hoogen. Editorial: Family-centered care in pediatric and neonatal critical care settings. Front. Pediatr. 12:1402948. doi: 10.3389/fped.2024.1402948 (2024). [↩]
- K. North, R. Whelan, L.V. Folger, H. Lawford, I. Olson, S. Driker & A.C. Lee. Family involvement in the routine care of hospitalized preterm or low birth weight infants: a systematic review and meta-analysis. Pediatrics, 150(Supplement 1) (2022). [↩] [↩]
- T. Arun Babu, & B.V. Bhat. Deciphering Physicians’ Perspectives on Fostering Family Integration in the Care of Preterm Infants in Neonatal Intensive Care Units. Indian Journal of Pediatrics, 91(4), 325-326 (2024). [↩] [↩] [↩]
- Y. A. Park & Y. Im. Exploration of family-centered care in NICUs: A grounded theory methodology. Qualitative Health Research, 35(10–11). https://doi.org/10.1177/10497323241298928 (2025). [↩] [↩]
- A. M. Traylor & B. Ohning. Can family members be teammates in the NICU? An observational investigation of family-centered teamwork in the neonatal intensive care unit. Journal of Interprofessional Care, 39(3), 429–437. https://doi.org/10.1080/13561820.2024.2405989 (2024). [↩] [↩]
- S. Vetcho, M. Cooke, & A.J. Ullman. Family-centred care in dedicated neonatal units: an integrative review of international perspectives. Journal of Neonatal Nursing, 26(2), 73–92 (2020). [↩] [↩]
- M. Murphy, V. Shah, & K. Benzies. Effectiveness of Alberta Family-Integrated Care on neonatal outcomes: A cluster randomized controlled trial. Journal of Clinical Medicine, 10(24), 5871 (2021). [↩] [↩]
- K. O’Brien, M. Bracht, K. Robson, X.Y. Ye, L. Mirea, M. Cruz, & S. K. Lee. Evaluation of the Family Integrated Care model of neonatal intensive care: a cluster randomized controlled trial in Canada and Australia. BMC pediatrics, 15(1), 210 (2015). [↩]
- M. Hriberšek, F. Eibensteiner, N. Bukowski, A.W.K. Yeung, A.G. Atanasov, & E. Schaden. Research areas and trends in family-centered care in the 21st century: a bibliometric review. Frontiers in Medicine, 11, 1401577 (2024). [↩] [↩]
- J. Lee. Neonatal family-centered care: evidence and practice models. Clin Exp Pediatr. Apr; 67(4):171-177. doi: 10.3345/cep.2023.00367. Epub 2023 Jun 14. PMID: 37321589; PMCID: PMC10990654 (2024). [↩] [↩]
- B. Moreno‐Sanz, M.T. Alferink, K. O’Brien, & L.S. Franck. Family integrated care: State of art and future perspectives. Acta Paediatrica, 114(4), 710-730 (2025). [↩] [↩]
- S. Bellizzi, C. M. P. Napodano, & P. Murgia. Family-centered care for newborns: A global perspective and review. Journal of Tropical Pediatrics, 70(5), fmae026. https://doi.org/10.1093/tropej/fmae026 (2024). [↩]


