
Abstract
Neurodegenerative diseases (NDs) such as Alzheimer’s, Parkinson’s, and Huntington’s disease are marked by progressive neuronal loss and often subsequent cognitive decline, affecting millions of people around the world every year. However, current clinical therapeutics of NDs face a formidable obstacle called the blood-brain barrier (BBB). The blood-brain barrier (BBB) is a protective layer between brain mass and blood veins, protecting the central nervous system (CNS) through high selective permeability. This protective mechanism also blocks access to most drug-like molecules, such as biologics, nucleic acids, and neurotransmitters. Therapeutics are thus prevented from accessing the CNS in effective concentrations, which is necessary to achieve clinical soundness. In response to this challenge, nanoparticles (NPs) have recently arisen as a solution. A wide range of nanosystems holds the capability to deliver drugs, genes, and other therapeutic interventions across the BBB with higher specificity, stability, and efficacy. While there are still clinical gaps to be filled between the lab and medical applications, NPs provide a promising mechanism of overcoming the technical challenges posed by the BBB.
This review aims to address the main nanoparticle design strategies that harness endogenous transport systems for BBB penetration, as well as the nanosystems’ therapeutic potential in the context of ND treatments.
Keywords: Nanomaterials; Nanoparticle drug delivery; Blood-brain barrier; Neurodegenerative diseases
Introduction
Neurodegenerative diseases (NDs) are characterized by their effect on the central nervous system (CNS) and their dominance as a leading cause of morbidity and disability, particularly among the aging population. The most prominent neurodegenerative diseases include Alzheimer’s disease (AD), Parkinson’s disease (PD), Huntington’s disease (HD), and amyotrophic lateral sclerosis (ALS); these are all marked by the gradual loss of structure and function of neurons in the CNS. Similarly, they share several key features, including protein aggregation, neuroinflammation, buildup of oxidative stress—and the disruption and function of the blood-brain barrier (BBB). As the senior population grows across the world, the prevalence and socioeconomic burden of NDs also continue to grow, yet current treatment options remain largely symptomatic and palliative.
A major limitation to developing effective therapeutics for NDs is the difficulty of delivering pharmacologic and genetic treatments into the brain. The BBB protects the CNS by limiting the passage of hydrophilic and charged compounds, as well as other toxins that can be of harm. However, this protective function also prevents the entry of most therapeutic agents; this ultimately results in poor brain bioavailability and limited treatment efficacy.
Nanoparticle (NP)-based delivery systems have emerged as a promising platform to overcome this restrictive nature of the BBB. Engineered nanocarriers can easily utilize endogenous transport methods to bypass the BBB and effectively localize the drug or gene at hand. They can also be easily customized in size, charge, surface chemistry, and material composition to enable the controlled and targeted delivery of therapeutic payloads directly to affected regions within the CNS. In doing so, nanoparticles also offer additional advantages like improved drug solubility, prolonged circulation time, and reduced systemic toxicity.
This review explores the mechanisms by which nanoparticles interact with the BBB and their therapeutic applications in treating neurodegenerative diseases. In doing so, we aim to provide a framework for the harnessing of nanotechnology to address the common delivery challenges of CNS diseases and advance the future of precision neurotherapeutics.
Methods
This review was conducted under the goal of identifying and evaluating peer-review studies that focus on nanoparticle-based drug delivery systems designed to cross the blood-brain barrier (BBB) particularly for the treatment of neurodegenerative diseases. Literature searches were primarily performed through databases like PubMed, ScienceDirect, and Google Scholar, using keywords such as “nanoparticles,” “blood-brain barrier,” “drug delivery,” and “neurodegenerative diseases.” Search strings, particularly, used boolean operators to combine these keywords (e.g. “nanoparticles AND blood-brain barrier AND Alzheimer’s”, “Parkinson’s AND drug delivery”). Results regarding recent nanotechnology were also limited to those after January 2010.
Inclusion criteria focused on studies investigating nanoplatforms for BBB penetration, again, in the context of treating NDs. Eligible studies reported either in vitro or in vivo results that showed significant benefits against NDs. Exclusion criteria, meanwhile, included: (i) non-English Language, (ii) studies that did not report therapeutic or BBB penetration outcomes, and (iii) editorials that lacked original data or methodology. Both original research articles and selected review papers that provided mechanistical insights were included. Selected studies were noted for nanocarrier type, therapeutic cargo, BBB transport mechanism, and reported outcomes, then were sorted into different categories. These categories included the type of nanoparticle—surface functionalized, charge modified, biomimetized, et cetera—and the purpose of the carrier—gene therapy, antibody delivery, external stimulation, et cetera. Study quality was assessed qualitatively. In vitro studies with small sample sizes were classified as low quality, in vivo rodent studies with physiological results were considered moderate quality, and in vitro rodent studies with appropriate controls and both physiological and behavioral results were considered high quality. Using this scheme, around 15 studies were categorized as low quality, around 20 studies as moderate quality, and around 10 as high quality. Findings were taken mostly from moderate quality studies, but also weighted in low and high quality studies depending on the nanoparticle technique.
Results
General Pathophysiology of Neurodegenerative Diseases
Neurodegenerative diseases (NDs) in general are noted by the various cellular and molecular disruptions that drive neuronal loss within the CNS. However, these disruptions also hinder therapeutic delivery. A hallmark of many NDs—Alzheimer’s disease (AD), Parkinson’s disease (PD), Huntington’s disease (HD), and others—is the accumulation of misfolded proteins, such as amyloid-β, tau, α-synuclein, or TDP-43. These aggregated proteins often initiate cellular cascades of oxidative stress and mitochondrial dysfunction, leading to apoptosis or some form of cell death within neurons. Glial cells like microglia and astrocytes are further affected by these diseases, leading to additional chronic neuroinflammation and the release of pro-inflammatory cytokines. While initially part of the immune response, prolonged NDs leads to activation of toxic phenotypes in glial cells. This contributes to neural damage and further disease progression1‘2.
Importantly, these pathological processes also disrupt the integrity of the blood-brain barrier (BBB). The BBB, as aforementioned, normally protects the CNS from toxins and pathogens; however, in neurodegeneration, the endothelial interface is subjected to increased permeability, reduced tight junction proteins, and altered transporter activity3. This both exacerbates neuroinflammation through the entrance of inflammatory molecules into the brain and impairs nutrient waste exchange, which is crucial for neuronal survival. Simultaneously, the disrupted BBB offers an additional challenge to exogenous therapeutic entrance, which limits the access of systemically administered drugs to the CNS. Understanding and targeting these barriers is crucial in designing effective delivery methods for various NDs.
The Blood-Brain Barrier (BBB)
The BBB is a multicellular interface that divides the “blood” and the “brain,” primarily composed of brain microvascular endothelial cells that are flanked by pericytes, astrocytic endfeet, and the basement membrane. It aids in separating the blood from the brain parenchyma and protecting the CNS from blood-borne toxins and other outside materials4. Its restrictive properties are founded by the tight junction proteins—including claudins, occludin, and zonula occludens (ZO-1)—which prevent paracellular diffusion of molecules between endothelial cells that make up most of the barrier5. While endothelial cells provide the tight junctions and characterize the low transcytosis rates that form the physical barrier, pericytes act to regulate angiogenesis and BBB stability. Astrocytes secret factors that maintain junctional integrity and control nutrient exchange. Microglia, while acting as immune sentinels, also can disrupt the BBB when activated to its toxic state, contributing to neuroinflammation in disease contexts. Adherence junctions and a low rate of vesicular transcytosis also restrict extracellular compounds from entering. Highly selective mechanisms also work transport nutrients across this barrier through diffusion and transcytosis, the latter of which is mediated by receptors, transporters, and other molecules; active efflux transporters such as P-glycloprotein (P-gp) and members of the ATP-binding cassette (ABC) family all pump xenobiotics and many drugs back into the bloodstream6‘7.
As a general rule, passive diffusion is relatively limited for molecules larger than ~400-500 Da, or for strongly hydrophilic and charged compounds8‘9. While endogenous molecules like glucose, amino acids, and certain peptides are able to cross the BBB via carrier-mediated transport (CMT) and receptor-mediated transcytosis (RMT), these functions of the barrier are much too intricate and selective for exogenous drugs to be able to pass through. Along with the aforementioned transporters that pump out the molecules that even manage to enter the brain, the barrier’s mechanisms cause 98% of small-molecule drugs and nearly all biologics to fail at reaching therapeutic concentrations in the brain10.
Within the context of PD and AD, the high selectivity of the BBB underscores the urgent need for better, targeted delivery systems. In AD, monoclonal antibodies targeting amyloid-β show promise in plaque reduction; however, due to limited BBB permeability, they require high systemic doses, leading to an increased risk of cerebral edema and other side effects11. Similarly, small-molecule BACE1 inhibitors, a promising agent in undercutting the production of Aβ peptides, have failed in clinical trials due to insufficient brain accumulation or off-target toxicity. PD therapeutics like dopamine, as aforementioned, are also unable to cross the BBB aside from intravenous administration; L-DOPA in its place shows fluctuating therapeutic effects and long-term motor complications. MAO-B, also mentioned previously, suffers from poor CNS specificity as well. Emerging gene therapies for both AD and PD—such as siRNA or antisense oligonucleotides—are often rapidly degraded in circulation and fail to reach neurons at therapeutic concentrations.
Importantly, the BBB is not uniform across brain regions, particularly in the context of neurodegenerative diseases that directly affect neuron function or content12. In AD, vascular amyloid and pericyte degeneration tend to produce leakiness. In PD, BBB disruption is subtler, localized to the substantia nigra and striatum, where dopaminergic loss is most frequently observed. In HD, widespread permeability increases can be observed throughout the basal ganglia. These disease-specific changes can enhance or impair therapeutic delivery, underscoring the necessity of tailoring strategies to each neuropathological context.
Consequently, novel delivery methods—especially nanoparticle-based systems designed to target or temporarily traverse these barriers—are essential to treating neurodegenerative diseases.
Nanoparticle Designs and Their BBB Transport
Nanoparticles are loosely defined as solid particles made of polymers or lipids, ranging in size from 1-100 nm, though many commonly used in vivo do often stretch to 50-300 nm. Their primary purpose lies in delivery, particularly for drugs and therapeutics. These novel materials hold great prospect in their ability to be manipulated easily, both on the surface and within. Similarly, NP matrix constituents can be controlled to fit their purpose as a non-viral delivery vector; the drug loading is relatively high13‘14.
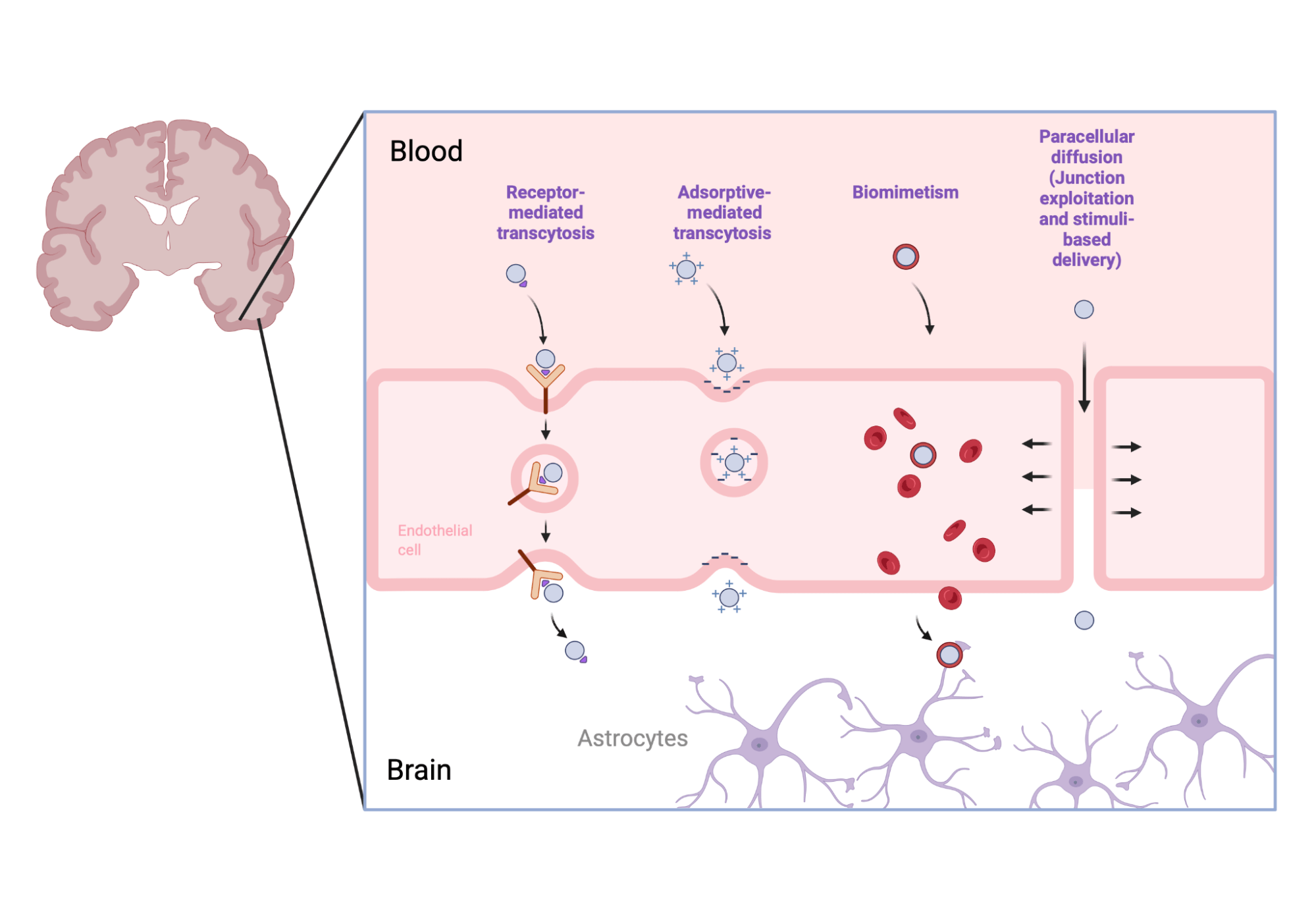
The success of these particles in effectively delivering their content depends on size, biocompatibility, and—most importantly—particular designs that enable specific interactions with the BBB. The following section seeks to analyze the core engineering strategies and their interactions with endogenous transport mechanisms. Figure 1 highlights the different pathways that these strategies take, as will be described below.
Surface Functionalization
One widely used approach involves nanoparticle systems functionalized with ligands that target endogenous transport receptors at the BBB. These designs are often targeted at receptor-mediated transcytosis (RMT). Here, large-molecule peptides or proteins attach to a specific domain on a receptor. Some receptors spur bidirectional transcytosis from the blood to brain as well as reverse-endocytosis from the brain to blood; this offers a rather fluid strategy of transporting substances throughout not just the brain, but also related circulatory systems15. The high specificity and low off-target uptake of receptor-mediated transport are also reasons why functionalized nanoparticles have remained one of the most clinically advanced designs for BBB penetration.
Common ligands include transferrin, insulin, glutathione, and synthetic peptides16. Transferrin binds to transferrin receptors that are one of the most highly expressed on brain endothelial cells, making it one of the most widely used shuttles for NP delivery. Insulin engages with insulin receptors, which are abundant yet can also vary with metabolic state and disease progression, engaging with receptor-mediated transcytosis. Glutathione leverages its role as an antioxidant and transporter substrate to both cross the BBB via corresponding transporters and reduce oxidative stress in general. Synthetic peptides can be engineered to mimic all these compounds to bind to specific endothelial receptors, and even mimic viral entry sequences for enhanced penetration.
PEGylation is a strategy widely employed to prolong circulation and shield the particle against aggregation, phagocytosis, and opsonization by coating the surface with polyethylene glycol (PEG)17. This ultimately serves to prolong the circulation half-life in the blood, leading to a greater chance for the encapsulation to take its effect. However, PEGylation can also mask targeting ligands and, with repeated dosing, induce “anti-PEG” immune responses that can ultimately limit efficacy. While it is a widely used surface customization strategy, optimizing PEG density and length is always crucial to balance stealth with targeting.
Another strategy is apolipoprotein-based coating. Apolipoprotein E (ApoE) or APoB fragments can be attached to nanoparticles, mimicking endogenous lipoproteins that naturally cross the BBB via LDL receptor-mediated pathways18. This approach has shown promise in increasing brain uptake, particularly for liposomes and polymeric NPs.
Lactoferrin conjugation has meanwhile been investigated to exploit lactoferrin receptors highly expressed in cerebral endothelium, providing both transport and anti-inflammatory effects.
Antibody or nanobody conjugation on the surface is another area of active development. Antibodies against transferring receptor, insulin receptor, or ICAM-1 can shuttle in NPs through receptor-mediated transcytosis. Nanobodies offer advantages of improved tissue penetration, along with lower immunogenicity. However, antibody conjugations can also substantially increase NP size and complicate reproducibility. Complement activation that is sometimes triggered also presents a risk of cell lysis19.
All these ligands and surface modifications can also be used in conjunction with one another. By combining PEGylation with a ligand—or even multiple ligands—NPs can simultaneously prolong circulation and exploit multiple transport routes. Triple-targeted nanoparticles, in fact, significantly increased cargo uptake through the BBB. Like this, surface functionalization is a highly-customizable bypass strategy that shows the greatest promise for clinical translation.
While the complexity of synthesis raises regulatory challenges, surface functionalization is a versatile strategy able to bypass nonspecific transport while maintaining low immunogenicity. Optimization of ligand density, orientation, compatibility with therapeutic, and compatibility with the variable brain states across patients and diseases is a critical aspect that must always be taken into consideration.
Charge Modification
Another mechanism that nanoparticles can exploit is adsorptive-mediated transcytosis (AMT). AMT is dependent on the adsorption of particles, often charged or cationic, via their binding to negatively charged membranes of endothelial cells. Thus nanoparticles designed with positive surface charges—commonly achieved through polymers like polyethylenimine (PEI) or poly-L-lysine (PLL)—can leverage AMT to penetrate the BBB20.
Though effective, these carriers can provoke immune responses or nonspecific uptake, requiring careful charge optimization and biodegradable polymer design. Furthermore, charge-modified carriers show special promise in gene silencing strategies; they may be combined with targeting ligands to balance efficacy with selectivity.
Biomimetism
Therapeutics are also delivered through biomimetic nanoparticles that mimic the body’s own cells to avoid immune clearance and enhance circulation time. These systems are often constructed by cloaking polymeric cores with erythrocyte or platelet membranes, allowing the nanoparticles to remain in circulation longer and deliver their antibody payloads more efficiently21.
For instance, Sanaee et al. reported a significantly improved antibody half-life and circulation compared to synthetic controls when delivered within erythrocyte membrane-coated nanoparticles22. Hu et al. further advanced this concept through RV-exosome membranes that were conjugated onto nanoparticles that reacted to reactive oxidative species (ROS), a hallmark of neurodegeneration. Targeted siRNA release resulted in notable anti-inflammatory effects23.
Due to reduced phagocytic clearance and longer circulation times, biomimetic nanoparticles hold promise for long term delivery. Mass reproducibility and standardization of membrane sources still remain major hurdles for clinical adoption, though.
Junction Exploitation
Another strategy takes advantage of transient BBB modulation to temporarily enhance permeability. In this model, nanoparticle systems incorporate short-acting physiological agonists to reversibly disrupt tight junctions in the barrier and facilitate paracellular antibody entry. Kinin receptor agonists conjugated to nanoparticles encompassing anti-AD antibodies have demonstrated substantial increases in CNS antibody delivery, along with therapeutic efficacy in suppressing synapse pruning mediated by complement activation24‘25.
However, modulating tight junctions at the blood-brain barrier carries significant risks. Even transient disruption can lead to nonspecific leakage of plasma proteins, ions, and immune cells into the brain parenchyma, which can potentially trigger neuroinflammation and edema. This loss of barrier selectivity can easily expose the neural tissue to circulating pathogens, which in turn can worsen the risk of neurodegeneration26. Repeated or poorly controlled modulations of tight junctions can even cause long-term alterations in barrier recovery, compromising overall BBB integrity. Thus, while this technique allows for controlled, temporary modulation of BBB integrity, it must be carefully balanced against risks of irreversible BBB damage if used incorrectly.
Stimuli-Response
Nanoparticles can also be engineered to change behavior in response to specific triggers. These triggers can either be external—such as ultrasound or magnetic—or internal—such as pH or oxidative-stress dependent27.
Jang and Park’s usage of magnetoelectric BCFO nanoparticles showed the efficacy of such a strategy. Their NPs disaggregated A fibrils upon low-frequency magnetic stimulation, reducing plaque density in AD-induced mice28. Stimuli-responsive nanoparticles have also been used to loosen tight junctions, releasing nitric oxide under focused ultrasound to exploit the junctions and enhance dopamine delivery29.
fibrils upon low-frequency magnetic stimulation, reducing plaque density in AD-induced mice28. Stimuli-responsive nanoparticles have also been used to loosen tight junctions, releasing nitric oxide under focused ultrasound to exploit the junctions and enhance dopamine delivery29.
This approach integrates well with neuromodulatory approaches and is less toxic, compared to NPs conjugated to other chemicals. Responsive systems are ideal for applications where non-invasive activation is preferred and where drug release must be synchronized with disease microenvironments; however, further investigation is required for precise control of external stimuli and safe evaluation for clinical translation.
These nanoparticle design strategies ultimately illustrate the diverse engineering approaches that enable BBB penetration across neurodegenerative disease contexts, laying the foundation for the therapeutic applications that will be discussed in subsequent sections.
Characterizing Pharmacokinetics and Distribution of Nps
After delivery through the BBB, the majority of the injected NP dose is typically sequestered in peripheral clearance organs like the liver, spleen, or kidney30. Systemic disposition is driven by the size of the particle, surface chemistry, charge, and degradability; smaller, neutrally charged, and stealth-coated particles tend to circulate longer, while cationic or high-PDI systems are generally more rapidly opsonized to be removed by the reticuloendothelial system31. Most importantly, brain uptake is highly dependent on the transport mechanism exploited—passive leakage, receptor-mediated transcytosis, stimulus-driven accumulation, et cetera.
Once in the CNS, the fate of the NP is shaped by brain-specific clearance pathways and other intracellular processing32. The glymphatic/CSF pathways—a paravascular system exchanging cerebrospinal and interstitial fluids—facilitate convective clearance of solutes, and contribute to the removal of soluble or degradable NPs. Dysfunction of these routes in aging and neurodegeneration can prolong intraparenchymal residence and increase the risk of toxic accumulation. Cellular processing, like endosomal trafficking or lysosomal degradation, further dictates whether delivered cargo is released or destroyed. Endosomal escape is therefore a critical determinant of efficacy; if therapeutic agents like siRNA, peptides, or proteins remain trapped in endo-lysosomal compartments, they are rapidly degraded. To counter this effect, NP systems are often engineered with pH-responsive linkers, fusogenic peptides, or polymer coatings that can destabilize endosomal membranes for cytosolic release33. While rapid clearance of toxicity is also important, excessive endosomal consumption can lead to a failure in delivering therapies to a functional intracellular dose.
A variety of experimental methods have been developed to monitor these processes in vivo. Radiolabeling (e.g.  Cu,
Cu,  Zr) and Positron Emission Tomography (PET)/Single Photon Emission Computed Tomography (SPECT) scans allow quantitative tracking of whole-body and brain uptake, while Magnetic Resonance Imaging (MRI) in the case of paramagnetic nanoparticles provides anatomical resolution. Near-infrared fluorescence imaging also enables sensitive visualization in rodent models, though having limited depth for larger models. Complementary ex vivo technique—autoradiography, Inductively Coupled Plasma-Mass Spectrometry (ICP-MS) for elemental quantification of metal NPs, and fluorescence history—can verify cellular localization and organ burden. Recent methodological reviews emphasize combining some of these modalities to produce robust pharmacokinetic profiling for NP evaluation34‘35.
Zr) and Positron Emission Tomography (PET)/Single Photon Emission Computed Tomography (SPECT) scans allow quantitative tracking of whole-body and brain uptake, while Magnetic Resonance Imaging (MRI) in the case of paramagnetic nanoparticles provides anatomical resolution. Near-infrared fluorescence imaging also enables sensitive visualization in rodent models, though having limited depth for larger models. Complementary ex vivo technique—autoradiography, Inductively Coupled Plasma-Mass Spectrometry (ICP-MS) for elemental quantification of metal NPs, and fluorescence history—can verify cellular localization and organ burden. Recent methodological reviews emphasize combining some of these modalities to produce robust pharmacokinetic profiling for NP evaluation34‘35.
Applications to Neurodegenerative Diseases
Antibody Delivery
Monoclonal antibody (mAb) administration to clear pathogenic proteins such as A, tau, and  -synuclein is one of the most promising AD immunotherapic treatments that have emerged in the field. Their easy production and ability to be conjugated with different drugs have led to FDA approval of various AD-treating drugs, such as Aducanumab and Lecanemab. Both of these drugs target A aggregation, forming complexes with the plaques that enable easier dissociation via microglia, astrocytes, and other immune cells36. Other drugs target tau tangles, the intracellular hallmark of AD. Less accessible than extracellular plaques, anti-tau antibodies are particularly valuable to access deeper cytosolic aggregates. However, high systemic dosage of mAbs, as required due to poor BBB permeability, increases the risk of adverse effects like amyloid-related imaging abnormalities11. Introduction of foreign material like this is also known to elicit immune responses of varying degrees, possibly deteriorating patient health. Stable delivery is also an important aspect that has yet to be perfected. Nanoparticle encapsulation improves upon this by enabling receptor-mediate transcytosis and site-specific release, directly improving the therapeutic index. In AD, such antibody-NP formulations can localize specifically to target amyloid- plaques or intracellular tau tangles, facilitating their microglial clearance and potentially restoring the synaptic environments disrupted by aggregated molecules. In PD, analogous approaches have targeted -synuclein oligomers, aiming to reduce the misfolded protein burden behind some dopaminergic neuronal loss.
-synuclein is one of the most promising AD immunotherapic treatments that have emerged in the field. Their easy production and ability to be conjugated with different drugs have led to FDA approval of various AD-treating drugs, such as Aducanumab and Lecanemab. Both of these drugs target A aggregation, forming complexes with the plaques that enable easier dissociation via microglia, astrocytes, and other immune cells36. Other drugs target tau tangles, the intracellular hallmark of AD. Less accessible than extracellular plaques, anti-tau antibodies are particularly valuable to access deeper cytosolic aggregates. However, high systemic dosage of mAbs, as required due to poor BBB permeability, increases the risk of adverse effects like amyloid-related imaging abnormalities11. Introduction of foreign material like this is also known to elicit immune responses of varying degrees, possibly deteriorating patient health. Stable delivery is also an important aspect that has yet to be perfected. Nanoparticle encapsulation improves upon this by enabling receptor-mediate transcytosis and site-specific release, directly improving the therapeutic index. In AD, such antibody-NP formulations can localize specifically to target amyloid- plaques or intracellular tau tangles, facilitating their microglial clearance and potentially restoring the synaptic environments disrupted by aggregated molecules. In PD, analogous approaches have targeted -synuclein oligomers, aiming to reduce the misfolded protein burden behind some dopaminergic neuronal loss.
Recent formulations like TMC-conjugated nanocarriers with B1/B2 kinin receptor peptides, for instance, have demonstrated significantly improved delivery of anti-C1q antibodies in deactivating proteins that modulate A accumulation. Gagnon et al. showed that kinin peptide agonists improved BBB permeability through transient disruptions, and the hydrophilic N,N,N-trimethyl chitosan (TMC) nanopolymer harnessing the power of these agonists successfully yielded up to 12-fold higher brain uptake of the antibodies compared to non-encapsulated peptides24. Similarly, PEG-PLL nanomicelles created by Amano et al. carrying Aβ-targeting antibodies enhanced brain penetration in Aβ-mutated mice and showed behavioral improvements. After peripheral administration of the nanomicelles significantly reduced brain levels of insoluble Aβ40/42 (~47%), Aβ oligomers (~65%), and other plaque burden, the nanoparticles showed successful disassembly as well37. Like this, coupling therapeutic antibodies with polymeric or lipid nanocarriers have shown improved half-life, stability, and localization compared to the naked state.
These findings generally underscore a broader trend of maximizing BBB transport through receptor- or charge-mediated mechanisms, with the goal of inducing therapeutic effects without adverse outcomes that accompany high, unstable dosing. However, such studies often emphasize proof-of-concept efficacy, neglecting key translational barriers, as is common across studies of human disease. Notably, the long-term immunogenicity of repeated mAb-NP exposure is rarely assessed, which means that the toxicity that comes with long-term mAb exposure might continue to be an issue with novel conjugations with nanomaterials. Furthermore, certain conjugation chemistries in antibody-nanoparticle platforms show unwanted aggregation of the antibodies and unwanted protein binding, demanding careful engineering and limiting the mass reproducibility of this therapeutic38.
Additionally, few studies actually compare different NP coatings for the same antibody cargo under the same in vivo conditions, limiting the understanding of optimal design parameters. It is also difficult to bridge translational gaps when in vivo studies are conducted under murine conditions, where BBB efflux mechanisms differ significantly from the human BBB.
Gene Therapy
Gene-based therapy for neurodegeneration relies on small interfering RNA (siRNA), antisense oligonucleotides, and CRISPR-Cas9 systems. These genes can either modify the mutations that often result in accumulation of toxic protein or oxidative specimens, or knock them out completely in order to prevent the ND at its core. The most common examples are downregulation of BACE1 in Alzheimer’s disease, SNCA in Parkinson’s disease, or mHTTT in Huntington’s Disease, which are behind amyloidogenic peptide production, -synuclein accumulation, and mutant huntingtin, respectively. However, naked siRNA or CRISPR systems face rapid degradation, immune recognition, and minimal BBB penetration. Nanoparticles provide an improved way of delivery by enhancing nucleic acid circulation and cell-specific delivery.
Helmschrodt et al., for instance, identified small interfering RNAs (siRNAs) that can be delivered via the 4–12 kDa branched polyethylenimine (PEI) F25-LMW complex to suppress -synuclein (SNCA) expression, which is a traceable cause to Parkinson’s. The SNCA NP successfully showed transfection without disturbance of the brain parenchyma remained intact, as well as 67 knockdown of SNCA mRNA; less SNCA proteins were observed, resulting in up to 50 knockdown in both hemispheres39. Wang et al. expanded this approach by utilizing a PEGylated poly(2-(N,N-dimethylamino) ethyl methacrylate) (PEG-PDMAEMA) particle altered with two targeting ligands, one for the BBB and one for neurons. BACE1 silencing efficacy was significantly improved, quantifying reversing A oligomer-induced synaptic injury within an A exposed murine model40. Similarly, recent work by Zhou et al. utilized the same siRNA against BACE1 with a glycosylated polymeric siRNA nanomedicine (Gal-NP@siRNA) further stabilized through a “triple-interaction” system, making use of the hydrophobic interaction between three polymers stabilized through a salt bridge. The siRNA Gal-NP complex showed significantly longer blood circulation time and half-lifetime compared to free siRNA, showing a 5.8-fold higher brain accumulation than the non-galactose NP as well41. Gene therapy using NP was also developed for HD, encapsulating siRNA targeting the mutant HTT gene that produces huntingtin. Sava et al. built their nanoparticles with chitosan cross-linked with Mangafodipir for a more stable complexation with the siRNA. An “enriched” version with cholesterol and diol modifications particularly allowed higher siRNA loading and dosing. Intranasal administration of these enriched nanoparticles were shown to achieve an HTT mRNA knockdown rate of over 50 across multiple brain regions, which far outperformed naked siRNA, reducing HTT proteins levels across the olfactory bulb, hippocampus, and striatum42.
knockdown of SNCA mRNA; less SNCA proteins were observed, resulting in up to 50 knockdown in both hemispheres39. Wang et al. expanded this approach by utilizing a PEGylated poly(2-(N,N-dimethylamino) ethyl methacrylate) (PEG-PDMAEMA) particle altered with two targeting ligands, one for the BBB and one for neurons. BACE1 silencing efficacy was significantly improved, quantifying reversing A oligomer-induced synaptic injury within an A exposed murine model40. Similarly, recent work by Zhou et al. utilized the same siRNA against BACE1 with a glycosylated polymeric siRNA nanomedicine (Gal-NP@siRNA) further stabilized through a “triple-interaction” system, making use of the hydrophobic interaction between three polymers stabilized through a salt bridge. The siRNA Gal-NP complex showed significantly longer blood circulation time and half-lifetime compared to free siRNA, showing a 5.8-fold higher brain accumulation than the non-galactose NP as well41. Gene therapy using NP was also developed for HD, encapsulating siRNA targeting the mutant HTT gene that produces huntingtin. Sava et al. built their nanoparticles with chitosan cross-linked with Mangafodipir for a more stable complexation with the siRNA. An “enriched” version with cholesterol and diol modifications particularly allowed higher siRNA loading and dosing. Intranasal administration of these enriched nanoparticles were shown to achieve an HTT mRNA knockdown rate of over 50 across multiple brain regions, which far outperformed naked siRNA, reducing HTT proteins levels across the olfactory bulb, hippocampus, and striatum42.
Despite these advances, most studies investigating siRNA-NP conjugations mostly assessed knockdown efficacy only in acute time windows, mostly within 7–14 days post-injection. This provides limited insight into chronic performance, or adaptive resistance long-term in the brain. Furthermore, limitations inherent to siRNA still remain, such as accidental silencing of non-target mRNA and direct activation of innate immune pathways. Dosage control of the genetic load is particularly important in order to avoid these problems, particularly considering how the inefficient endosomal escape of siRNA and the resulting bioavailability limitations—even under NP encapsulation—could easily lead to overdosage43.
Small Molecule Delivery
Small-molecule drugs, such as antioxidants, enzyme inhibitors, and kinase modulators, are perhaps the therapeutic strategy that benefit the most from nanoparticle delivery. While the most common palliative therapeutic, small molecules are often deterred from reaching their full potential by poor solubility, rapid metabolism, and limited penetration. Dopamine, for instance, serves as a cornerstone of Parkinson’s disease treatment. However, free dopamine is often metabolized before reaching the brain, unable to cross the BBB efficiently. L-DOPA, its prodrug, is favored for this reason; yet this causes long-term motor complications with chronic use. Encapsulation in PLGA or liposomal NPs offers a solution to this issue by protecting dopamine and enabling sustained release within the striatum, directly compensating for dopaminergic neuronal loss in PD.
Pahuja et al. tested dopamine-loaded PLGA nanoparticles (DA NPs) within a PD murine model. Dopamine in itself has a short plasma half-life, which further decreases the chances of absorption through the BBB. Entrapment of the dopamine within the PLGA NP increased retention time and similarly prevented rapid peripheral metabolism, ultimately resulting in improved motor function in the murine model44. Monge-Fuentes et al. further developed the use of PLGA nanoparticles loaded with dopamine by adding albumin (ALNP-DA). The ALNP-DA acted as a surface modifier to decrease reticular endothelial uptake by restricting the binding of other proteins, which led to effective localization within the striatum and hippocampal formation. Similarly, neurobehavioral tests for motor coordination and dopamine responsiveness in murine models showed significant improvement45. These nanoparticles also showed lower toxicity in vivo compared to naked dopamine. By stabilizing dopamine or its analogs, these formulations help directly compensate for the dopaminergic deficits in the striatum, which is the central pathological feature of PD behind motor dysfunction.
The efficiency of PLGA-based nanosystems has also been tested with circumin, a hydrophobic polyphenol with noticeable neuroprotective and anti-inflammatory effects for the treatment of AD. Curcumin has strong anti-tau effects, able to disaggregate tangles. However, it has poor solubility and bioavailability. NP formulations can increase curcumin stability and improve brain accumulation, converting this therapeutic into a more viable anti-tau agent. In a study from Fan et al., curcumin-loaded PLGA NPs were shown to improve cellular uptake through decreased curcumin diameter. Increased curcumin circulation ultimately reduced tau phosphorylation and oxidative damage at lower doses than bulk curcumin within the APP/PS1 mice brains, also showing adequate blood compatibility. Treated mice showed improved spatial memory46. Here, curcumin encapsulation directly counteracts the tau hyperphosphorylation and oxidative stress, linking NP stability to the reduction of two of the most critical AD hallmarks.
Overall, small molecule-harnessing nanotherapy generally utilized biodegradable carriers like PLGA, offering a good safety profile and lower biotoxicity. Another key trend is the usage of passive-targeting mechanisms, which lack receptor-mediated transport features that were prevalent in NP-mAB systems. Further investigation into the compatibility of small-molecule loads with targeting surface ligands is necessary. Additionally, these carriers also show varied degradation rates based on lactic and glycolic acid ratios, local pH, and protein corona effects, which complicates dose predictability. Like other therapeutic strategies, most results are drawn from small-cohort murine models, too, making clinical significance unclear.
Stimuli-Based Therapy
As aforementioned, stimuli-responsive NPs, triggered by pH, redox, ultrasound, or electricity, allow on-demand, localized drug release. This has shown promise in non-pharmacological therapy within the context of neurodegenerative disease. Magnetoelectric and piezoelectric nanoparticles, in particular, have shown potential in disrupting protein aggregates or stimulating neuronal activity.
For instance, disaggregation of A can also occur through NPs that oxidize the neurotoxic foldings under the excitement of magnetic fields. Magnetically responsive NPs generate localized physical forces under external fields, which can disrupt amyloid fibrils that contribute to AD. This mechanism allows physical destabilization of plaques that conventional drugs might not be able to achieve as easily. Jang et al. applied magnetoelectric BCFO nanoparticles in transgenic AD mice to explore this property. Individual administration of the BCFO NPs and low-frequency magnetic field showed no distinct morphological changes; exposure to the magnetic field in the presence of the NPs, however, disassociated the original A fibrils into stable, amorphous amyloid aggregates. Ex vivo murine brains reveal a lowered density of A plaques in the cerebral cortex47. This strategy is unique in that the NP does not merely deliver a therapeutic, but physically disrupts the amyloid fibrils and dismantles the lesions of AD that cause synaptic toxicity. Similarly, Qu’s group designed magnetic nanoparticles functionalized with a naphthalimide fluorescent probe and KLVFF peptide (MNP@NFP-pep). Not only were these NPs able to detect A oligomers through difference in fluorescence with A disaggregation, but they could also directly cause dissociation of A oligomers when exposed to alternating magnetic fields by triggering magnetothermal activity48.
These techniques overall offer the advantage of spatiotemporal precision, allowing for on-demand activation in a time-precise manner. However, this particular nature of stimuli-based nanotherapy makes it more difficult to reproduce the technical infrastructure required, such as external magnets and focused ultrasound. Clinical translatability is limited in this aspect. Furthermore, many of these studies assume uniform NP distribution across brain regions, an assumption that might not necessarily hold in more complex human brains. Most importantly, few safety evaluations exist for repeated exposure to these stimuli—particularly magnetic or ultrasonic fields—particularly in aged populations with neuroinflammatory damage. While this approach avoids systematic pharmacodynamic problems like traditional treatments do, it introduces a whole new class of risks that need to be studied further.
| Author (Year) | NP Type | Size / Charge | Targeting Ligand | Cargo | Model | Main Outcome | Limitations |
| Veszelka et al. (2021) | Polymeric/ligand-functionalized NPs | Non-targeted NP: 157 nm / -5.7 mV Triple-ligand NP (N-AGL): 193 nm / +8.9 mV | Triple combination of targeting ligands | Fluorescent tracer / marker | In vitro BBB culture model | Triple-ligand formulation enhanced nanoparticle penetration across BBB model synergistically | In vitro only; no therapeutic validation |
| Topal et al. (2020) | Solid lipid nanoparticles (SLNs) | DON-SLN: 104.6 nm / -15.2 mV ApoE-DON-SLN: 147.5 nm / -9.6 mV | ApoE-targeting | Donepezil | In vitro BBB culture (rat) | ApoE-targeted SLNs increased transfer of donepezil across BBB | No in vivo validation |
| Hu et al. (2011) | RBC-membrane-camouflaged polymeric NPs (biomimetic) | RBC-NP: 180 nm / -16 mV | RBC membrane proteins (biomimicry) | Model cargo (doxorubicin) | Mouse biodistribution studies | Prolonged circulation time, reduced immune clearance | Not tested for BBB or neurodegenerative models |
| Gagnon et al. (2023) | TMC™ polymeric nanoparticles | TMC-antibody NP: 130-165 nm / NR | B1R/B2R agonist peptides | Antibody (anti-Aβ) | Alzheimer’s mouse model | Enhanced brain antibody delivery, reduced Aβ pathology | Limited pharmacokinetic/toxicity data |
| Jang et al. (2022) | Magnetoelectric nanoparticles | NR | None | No chemical drug cargo (physical Aβ dissociation) | Alzheimer’s mouse model | Low frequency magnetic fields + magnetoelectric particles | In vitro and ex vivo only; no behavioral testing |
| Zhou et al. (2020) | BBB-penetrating siRNA nanomedicine (lipid/polymer hybrid) | siRNA NP: 118 nm / NR | BBB shuttle peptide | siRNA (BACE1) | Alzheimer’s mouse model | Lowered BACE1 expression, reduced amyloid pathology, improved cognition | Long term dosing and immune response profiling not evaluated |
| Pahuja et al. (2015) | Polymeric nanoparticles | DA NP: 119.7 nm / -2.66 mV | Lactoferrin | Dopamine | Parkinsonian rat model | Systemic nanoparticle delivery of dopamine reversed motor deficits | Rapid clearance, formulation instability |
Discussion
Overall, the development of NP-based delivery systems presents a novel shift in the treatment of neurodegenerative diseases, which have been hindered by the impermeability of the BBB. These technologies—stretching from ligand-targeted and charge-modified nanoparticles to biomimetic and stimuli-responsive systems—offer a more customizable means to overcome traditional pharmacological limitations. What ultimately distinguishes these approaches is their functional adaptability, easily tailed through surface modification, payload modulation, and responsive release to the neuropathological context.
Strengths and Emerging Directions
A notable strength of NP systems is customizability and modularity. Ligand-functionalized particles enable the exploitation of receptor-mediated transcytosis with brain-specific targeting, as well as biomimetic coatings that prolong circulation and allow foreign materials to evade immune detection. These platforms accommodate multi-modal function, including but not limited to co-delivery of gene silencers with anti-inflammatory drugs, or pairing of diagnostic imaging with therapeutic payloads. This versatility is particularly well-suited in the context of neurodegenerative disease, where multiple pathological axes—protein aggregation, neuroinflammation, synaptic loss, oxidative stress and more—converge and vary between individuals and disease stages.
In a similar vein, another emerging frontier in NP research is co-delivery, where multiple agents are packaged into a single carrier in order to address different disease pathways. For instance, siRNA against amyloidogenic enzymes can be combined with antioxidants to both reduce plaque formation and counter oxidative stress49. In Parkinson’s models, dopamine replacement has been co-delivered with anti-inflammatory drugs to simultaneously restore neurotransmission and suppress microglial activation50. Theranostic approaches add another layer of complexity, coupling imaging agents with drugs for real-time monitoring of NP distribution and therapeutic response51. While co-delivery systems do increase complexity in formulation and regulation, they hold unique promise for addressing the multifactorial nature of NDs.
Challenges and Risks
There remain non-trivial limitations that limit the translatability of NP technology. First, the majority of delivery methods are based on highly specific molecular interactions—such as GLUT1, transferrin, or LDLR-mediated endocytosis—that can vary with age, inflammation, or stage of disease. This creates heterogeneity in the therapeutic response amongst patients, especially in elderly populations. Furthermore, the complexity in designing multifunctional NPs, particularly those that include biologically derived coatings or dual-payload structures, creates challenges in standardization, scale-up, and regulatory approval. Issues in reproducibility and quality control hinder the clinical translation of nanosystems as a widespread therapeutic. This aspect must be addressed through greater material characterization and process validation.
There is also the issue of long-term safety and pharmacokinetics, especially in the CNS, where clearance mechanisms differ from peripheral organs. The brain’s impaired lymphatic drainage, particularly in the case of neurodegenerative diseases, raises questions about the chronic accumulation of non-degradable materials, particularly in inorganic or hybrid systems. Furthermore, stimuli-responsive NPs utilize exogenous stimuli like light and electromagnetic fields. This introduces additional parameters of patient safety, dosing repeatability, and tissue selectivity.
Nanoparticle toxicity also arises not just from gross accumulation, but also from intracellular mechanisms. These approaches are essentially introducing foreign materials into the brain and can thus induce additional neuroinflammation if not carefully tailored. Metallic and carbon-based NPs, for instance, are known to catalyze electron transfer reactions, producing reactive oxygen species (ROS) that can damage membranes, proteins, and even DNA. ROS is known to be a key marker and trigger for neuroinflammation in various NDs; thus it can contribute to an exacerbation of symptoms in the cases of inflammatory NDs like AD and PD. ROS can also impair mitochondrial respiration, in turn triggering cytochrome c release and apoptotic pathways. Even degradable polymers may lead to lysosomal swelling, or disrupt calcium homeostasis within the brain, if their breakdown is too rapid. Cationic particles can destabilize membranes and compromise neuronal excitability. Ultimately, these mechanisms highlight the need to balance NP stability with degradability, ensuring therapeutic efficacy without chronic neurotoxicity.
One concern that has gained increased attention is the interaction of nanoparticles with the brain’s immune system52. The introduction of foreign, inorganic materials can easily trigger immune cascades that affect the patient in a negative way. For instance, microglia that act to recognize foreign particles engulf even the polymers considered biocompatible. While this can be beneficial for clearing excess therapeutic agents after delivery, it can also lead to the release of pro-inflammatory cytokines, nitric oxide, and reactive oxygen species, which may exacerbate the neuronal injury. In peripheral circulation, opsonization through serum proteins and macrophage recognition also reduces the bioavailability of NPs and can provoke systemic immune responses. Engineering solutions include additional PEGylation to reduce recognition, aforementioned biomimetic coatings using erythrocyte membranes or exosomes, or co-delivery of anti-inflammatory agents to reduce adverse responses. However, the question of how to deliver NPs in a way that minimizes immune-triggered neuroinflammation still remains a point of concern.
There is also the issue of translability to humans; NP circumvention of the BBB is mostly characterized in murine models, which molecularly differ from human neurosystems and thus do not guarantee effectiveness at the level of clinical trials. Most notably, rodent BBB models tend to overestimate NP penetration compared to humans, mainly due to higher expression levels of certain efflux transporters such as P-glycoprotein (P-gp/ABCB1), which can result in faster clearance of xenobiotics from the brain compared to humans. This can underestimate drug accumulation potential in human tissue. Similarly, tight junction protein composition and density also tend to differ, with human BBB endothelial cells generally being much more structurally complex and tighter in regulating paracellular permeability. Moreover, human brain endothelial cells are more heavily influenced by pericyte coverage and astrocytic interactions, which lead to critical differences in signaling pathways that control barrier integrity and immune surveillance. The discrepancy in the immune microenvironment also presents another barrier in translability between the murine to human model, as the muring BBB tends to mount a more rapid inflammatory response compared to human BBB dysfunction, which is more gradual and involves distinct cytokine networks53. As a result, the neurotoxicity or efficacy of NPs within the human brain remains unclear. Rather than rodent models, utilizing organoids or non-human primates may offer more predictive models to bridge the translational gaps.
While these challenges do not undercut the potential efficacy of NP-based therapeutics, they underscore the necessity for parallel investment in toxicology, imaging, and post-delivery monitoring technologies.
| NP Platform | Typical Size/PDI | Loading Efficiency | Release Kinetics | BBB Uptake Strategy | Strengths | Limitations/Risks |
| Polymeric NPs (PLGA) | 100-200 nm/<0.2 | 20-40% | Sustained (days-weeks) | Ligand conjugation, passive uptake | Biodegradable; good control of release | Acidic degradation byproducts; variable uptake |
| Lipid-based NPs | 80-150 nm/<0.25 | 30-50% | Hours-days | Fusion with cell membranes, ligands | High biocompatibility; easy drug loading | Instability in circulation; batch-to-batch variability |
| Cationic polymers (PEI, chitosan) | 20-100 nm/variable | 10-30% | Burst release common | Electrostatic endocytosis | Strong nucleic acid binding, endosomal escape | High cytotoxicity; membrane disruption |
| Antibody-conjugated NPs | 80-120 nm/<0.2 | 5-15% | Sustained or controlled | Receptor-mediated transcytosis | High specificity; targets plaques, tangles | Expensive; aggregation; immunogenicity |
| Peptide-modified NPs | 50-150 nm/<0.2 | 15-35% | Controlled (days) | Receptor-mediated (LRP1, RVG29) | Customizable, smaller size than antibodies | Stability issues; rapid clearance |
| Biomimetic NPs (exosomes, membranes) | 80-150 nm/<0.25 | 10-25% | Variable | Natural receptor recognition | Low immunogenicity; immune evasion | Difficult to scale; heterogeneity |
| Inorganic/magnetoelectric NPs | 20-80 nm/<0.15 | 30-60% | External stimulus-dependent | Field-responsive targeting | Multifunctional (therapy + imaging) | Long-term accumulation; ROS generation |
Limitations
This review has several limitations that must be acknowledged. First, although multiple databases were searched, the scope still reflects selection bias and does not include non-English studies altogether. Generally speaking, the review was conducted through the author’s manual search for papers rather than a formal, large-scale algorithm, which limits the number of accessed papers as well. Furthermore, no formal meta-analysis was performed, and quality classification was based on the author’s qualitative judgment. The majority of cited studies were also conducted in rodents, namely under in vitro analysis of rodent brain models, in order to discuss a wider variety of nanoparticle approaches. This limits both generalizability to humans and efficacy in behavioral improvements. Finally, publication bias can also play a big factor in filtering out unsuccessful or toxic NP formulations, leaving these preclinical outcomes underrepresented. These factors should temper the conclusions drawn here, ultimately highlighting the need for a more systematic, comparative, and translational investigations.
Conclusion
In summary, nanoparticle-based technologies have emerged as a promising tool in treating neurodegenerative diseases, offering an effective, multifaceted solution to one of the most persistent challenges in CNS therapeutics: the blood-brain barrier. By leveraging mechanisms of absorption such as receptor-mediated transcytosis, charge-based adsorption, and stimuli-responsive modulation, engineered nanoparticles have shown promise in improving the pharmacokinetics and overall efficacy of therapeutic agents. These innovations not only show robust preclinical outcomes—such as reduced plaque burden, gene knockdown, and behavioral improvements—but also expand the conceptual toolkit for neurotherapeutics. However, the translational pathway between lab results and real-life applications continues to face challenges, such as issues in immunogenicity, long-term accumulation, manufacturing scalability, and interspecies variability.
To make NP platforms more applicable in the clinical setting, future studies must move beyond proof-of-concept demonstrations and more towards systematic, comparative investigations that evaluate efficacy and safety across more diverse models. This might include utilizing humanized organoids, or non-human primate systems—under a solid ethical frame—that better replicate the complexity of the human BBB and CNS. Furthermore, in order to improve reproducibility and regulatory compliance, standardization in NP manufacturing, surface functionalization, and in vivo testing protocols is critical. Integrating diagnostic and therapeutic functionalities together into NP systems to enhance real-time monitoring of disease progression and treatment response is also a promising branch that should be emphasized. Through combined progress in bioengineering, neuroscience, and regulatory science, nanoparticles offer a promising role as a potential component of future strategies against neurodegeneration.
References
- R. N. L. Lamptey, B. Chaulagain, R. Trivedi, A. Gothwal, B. Layek, J. Singh, A review of the common neurodegenerative disorders: current therapeutic approaches and the potential role of nanotherapeutics. Int J Mol Sci. 23, 1851 (2022). [↩]
- B. N. Dugger, D. W. Dickson, Pathology of neurodegenerative diseases. Cold Spring Harb Perspect Biol. 9, a028035 (2017). [↩]
- E. G. Knox, M. R. Aburto, G. Clarke, The blood-brain barrier in aging and neurodegeneration. Mol Psychiatry. 27, 2659-2673 (2022). [↩]
- H. Kadry, B. Noorani, L. Cucullo, A blood–brain barrier overview on structure, function, impairment, and biomarkers of integrity. Fluids Barriers CNS. 17, 69 (2020). [↩]
- N. J. Abbott, L. Rönnbäck, E. Hansson, Astrocyte-endothelial interactions at the blood-brain barrier. Nat Rev Neurosci. 7, 41-53 (2006). [↩]
- Y. Zhou, Z. Peng, E. S. Seven, R. M. Leblanc, Crossing the blood-brain barrier with nanoparticles. J Control Release. 270, 290-303 (2018). [↩]
- G. C. Terstappen, A. H. Meyer, R. D. Bell, W. Zhang, Strategies for delivering therapeutics across the blood–brain barrier. Nature Reviews Drug Discovery. 20, 362-383 (2021). [↩]
- S.G.G. Arachchige, R. Rienzie, N. M. Adassooriya, Nanocarrier-mediated drug delivery systems for neurodegenerative diseases. In: M. Rai, A. Yadav (eds) Nanobiotechnology in Neurodegenerative Diseases. Springer, Cham (2019). [↩]
- W. M. Pardridge, The blood-brain barrier: bottleneck in brain drug development. Neurotherapeutics. 2, 3-14 (2005). [↩]
- W. M. Pardridge, The blood-brain barrier and neurotherapeutics. Neurotherapeutics. 2, 1-2 (2005). [↩]
- D. S. Knopman, D. T. Jones, M. D. Greicius, Failure to demonstrate efficacy of aducanumab: an analysis of the EMERGE and ENGAGE trials as reported by Biogen, December 2019. Alzheimer’s & Dementia. 17, 696-701 (2021). [↩] [↩]
- P. M. Carvey, B. Hendey, A. J. Monahan, The blood-brain barrier in neurodegenerative disease: a rhetorical perspective. J Neurochem. 111, 291-314 (2009). [↩]
- C. Spuch, O. Saida, C. Navarro, Advances in the treatment of neurodegenerative disorders employing nanoparticles. Recent Pat Drug Deliv Formul. 6, 2-18 (2012). [↩]
- S. G. G. Arachchige, R. Rienzie, N. M. Adassooriya, Nanocarrier-mediated drug delivery systems for neurodegenerative diseases. In: M. Rai, A. Yadav (eds) Nanobiotechnology in Neurodegenerative Diseases. Springer, Cham (2019). [↩]
- G. C. Terstappen, A. H. Meyer, R. D. Bell, Strategies for delivering therapeutics across the blood-brain barrier. Nat Rev Drug Discov. 20, 362-383 (2021). [↩]
- S. Veszelka, M. Mészáros, G. Porkoláb, A. Szecskó, N. Kondor, G. Ferenc, T. F. Polgár, G. Katona, Z. Kóta, L. Kelemen, T. Páli, J. P. Vigh, F. R. Walter, S. Bolognin, J. C. Schwamborn, J. S. Jan, M. A. Deli, A triple combination of targeting ligands increases the penetration of nanoparticles across a blood-brain barrier culture model. Pharmaceutics. 14, 86 (2021). [↩]
- J. S. Suk, Q. Xu, N. Kim, J. Hanes, L. M. Ensign, PEGylation as a strategy for improving nanoparticle-based drug and gene delivery. Adv Drug Deliv Rev. 99, 28-51 (2016). [↩]
- G. R. Topal, M. Mészáros, G. Porkoláb, A. Szecskó, T. F. Polgár, L. Siklós, M. A. Deli, S. Veszelka, A. Bozkir, ApoE-targeting increases the transfer of solid lipid nanoparticles with donepezil cargo across a culture model of the blood-brain barrier. Pharmaceutics. 13, 38 (2020). [↩]
- M. Kumari, A. Acharya, P. T. Krishnamurthy, Antibody-conjugated nanoparticles for target-specific drug delivery of chemotherapeutics. Beilstein J Nanotechnol. 14, 912-926 (2023). [↩]
- F. Hervé, N. Ghinea, J. M. Scherrmann, CNS delivery via adsorptive transcytosis. AAPS J. 10, 455-472 (2008). [↩]
- C. J. Hu, L. Zhang, S. Aryal, C. Cheung, R. H. Fang, L. Zhang, Erythrocyte membrane-camouflaged polymeric nanoparticles as a biomimetic delivery platform. Proc. Natl. Acad. Sci. U.S.A. 108, 10980-10985 (2011). [↩]
- M. Sanaee, K. G. Ronquist, E. Sandberg, J. M. Morrell, J. Widengren, K. Gallo, Antibody-loading of biological nanocarrier vesicles derived from red-blood-cell membranes. ACS Omega. 9, 22711-22718 (2024). [↩]
- Y. Hu, M. Zhao, H. Wang, Y. Guo, X. Cheng, T. Zhao, H. Wang, Y. Zhang, Y. Ma, W. Tao, Exosome-sheathed ROS-responsive nanogel to improve targeted therapy in perimenopausal depression. J Nanobiotechnology. 21, 261 (2023). [↩]
- M. Gagnon, M. Savard, T. M. H. Tran, L. Vincent, A. Moquin, P. Tremblay, X. Roucou, Y. Dory, F. Gobeil, Evaluation of novel B1R/B2R agonists containing TMC\texttrademark{} nanoparticles for targeted brain delivery of antibodies in a mouse model of Alzheimer disease. Molecules. 28, 5206 (2023). [↩] [↩]
- J. R. Wu, Y. Hernandez, K. F. Miyasaki, E. J. Kwon, Engineered nanomaterials that exploit blood-brain barrier dysfunction for delivery to the brain. Advanced Drug Delivery Reviews. 197, 114820 (2023). [↩]
- Y. Hashimoto, M. Campbell, Tight junction modulation at the blood-brain barrier: current and future perspectives. Biochimica et Biophysica Acta (BBA) – Biomembranes. 1862, 183298 (2020). [↩]
- X. Chen, D. Wu, Z. Chen, Biomedical applications of stimuli-responsive nanomaterials. MedComm. 5, e643 (2024). [↩]
- J. Jang, C. B. Park, Magnetoelectric dissociation of Alzheimer’s -amyloid aggregates. Sci Adv. 8, eabn1675 (2022). [↩]
- T. Kim, H. J. Kim, W. Choi, Y. M. Lee, J. H. Pyo, J. Lee, J. Kim, J. Kim, J. H. Kim, C. Kim, W. J. Kim, Deep brain stimulation by blood-brain-barrier-crossing piezoelectric nanoparticles generating current and nitric oxide under focused ultrasound. Nat Biomed Eng. 7, 149-163 (2023). [↩]
- J. Nowak-Jary, B. Machnicka, In vivo biodistribution and clearance of magnetic iron oxide nanoparticles for medical applications. Int J Nanomedicine. 18, 4067-4100 (2023). [↩]
- F. Alexis, E. Pridgen, L. K. Molnar, O. C. Farokhzad, Factors affecting the clearance and biodistribution of polymeric nanoparticles. Molecular Pharmaceutics. 5, 505-515 (2008). [↩]
- R. Liu, W. Jia, Y. Wang, C. Hu, W. Yu, Y. Huang, L. Wang, H. Gao, Glymphatic system and subsidiary pathways drive nanoparticles away from the brain. Research (Wash D C). 2022, 9847612 (2022). [↩]
- N. Desai, A. Kumar, D. Patel, V. Shah, R. Murthy, Achieving endo/lysosomal escape using smart nanosystems for efficient cellular delivery. Molecules. 29, 3131 (2024). [↩]
- M. Kumar, P. Kulkarni, S. Liu, N. Chemuturi, D. K. Shah, Nanoparticle biodistribution coefficients: a quantitative approach for understanding the tissue distribution of nanoparticles. Advanced Drug Delivery Reviews. 194, 114708 (2023). [↩]
- R. Kumar, I. Roy, T. Y. Ohulchanskky, L. A. Vathy, E. J. Bergey, M. Sajjad, P. N. Prasad, In vivo biodistribution and clearance studies using multimodal organically modified silica nanoparticles. ACS Nano. 4, 699-708 (2010). [↩]
- A. Barrera-Ocampo, Monoclonal antibodies and aptamers: the future therapeutics for Alzheimer’s disease. Acta Pharm Sin B. 14, 2795-2814 (2024). [↩]
- A. Amano, N. Sanjo, W. Araki, Peripheral administration of nanomicelle-encapsulated anti-Aβ oligomer fragment antibody reduces various toxic Aβ species in the brain. J Nanobiotechnol. 21, 36 (2023). [↩]
- M. H. Zaleski, J. Yang, A. Tsourkas, D. Issadore, Conjugation chemistry markedly impacts toxicity and biodistribution of targeted nanoparticles, mediated by complement activation. Advanced Materials. 37, 2409945 (2024). [↩]
- C. Helmschrodt, S. Höbel, S. Schöniger, A. Bauer, J. Bonicelli, M. Gringmuth, S. A. Fietz, A. Aigner, A. Richter, F. Richter, Polyethylenimine nanoparticle-mediated siRNA delivery to reduce -synuclein expression in a model of Parkinson’s disease. Mol Ther Nucleic Acids. 9, 57-68 (2017). [↩]
- P. Wang, X. Zheng, Q. Guo, P. Yang, X. Pang, K. Qian, W. Lu, Q. Zhang, X. Jiang, Systemic delivery of BACE1 siRNA through neuron-targeted nanocomplexes for treatment of Alzheimer’s disease. J Control Release. 279, 220-233 (2018). [↩]
- Y. Zhou, F. Zhu, Y. Liu, M. Zheng, Y. Wang, D. Zhang, Y. Anraku, Y. Zou, J. Li, H. Wu, X. Pang, W. Tao, O. Shimoni, A. I. Bush, X. Xue, B. Shi, Blood-brain barrier-penetrating siRNA nanomedicine for Alzheimer’s disease therapy. Sci Adv. 6, eabc7031 (2020). [↩]
- V. Sava, O. Fihurka, A. Khvorova, J. Sanchez-Ramos, Enriched chitosan nanoparticles loaded with siRNA are effective in lowering Huntington’s disease gene expression following intranasal administration. Nanomedicine. 24, 102119 (2020). [↩]
- J. Zhou, K. T. Shum, J. C. Burnett, J. J. Rossi, Nanoparticle-based delivery of RNAi therapeutics: progress and challenges. Pharmaceuticals. 6, 85-107 (2013). [↩]
- R. Pahuja, K. Seth, A. Shukla, R. K. Shukla, P. Bhatnagar, L. K. S. Chauhan, P. N. Saxena, J. Arun, B. P. Chaudhari, D. K. Patel, Trans-blood brain barrier delivery of dopamine-loaded nanoparticles reverses functional deficits in parkinsonian rats. ACS Nano. 9, 4850-4871 (2015). [↩]
- V. Monge-Fuentes, A. Biolchi Mayer, M. R. Lima, Dopamine-loaded nanoparticle systems circumvent the blood-brain barrier restoring motor function in mouse model for Parkinson’s disease. Sci Rep. 11, 15185 (2021). [↩]
- S. Fan, Y. Zheng, X. Liu, W. Fang, X. Chen, W. Liao, X. Jing, M. Lei, E. Tao, Q. Ma, X. Zhang, R. Guo, J. Liu, Curcumin-loaded PLGA-PEG nanoparticles conjugated with B6 peptide for potential use in Alzheimer’s disease. Drug Deliv. 25, 1091-1102 (2018). [↩]
- J. Jang, C. B. Park, Magnetoelectric dissociation of Alzheimer’s β-amyloid aggregates. Sci Adv. 8, eabn1675 (2022). [↩]
- Z. Du, N. Gao, Y. Guan, Rational design of a “sense and treat” system to target amyloid aggregates related to Alzheimer’s disease. Nano Res. 11, 1987-1997 (2018). [↩]
- T. Nguyen, H. T. Doan, K. T. Quan, T. D. Nguyen, T. T. Nguyen, D. H. Nguyen, C. W. Mai, C. N. Nguyen, B. T. Mai, H. V. Le, Astaxanthin-loaded brain-permeable liposomes for parkinson’s disease treatment via antioxidant and anti-inflammatory responses. Journal of Nanobiotechnology. 23, https://doi.org/10.1186/s12951-025-03104-8 (2025). [↩]
- S. Castellani, M. di Gioia, I. d’Angelo, A. Paladini, A. Bochicchio, F. Sisucci, S. Carbone, A. M. Giannelli, P. Iacovelli, P. Berna, M. Conese, Dopamine and citicoline-co-loaded solid lipid nanoparticles as multifunctional nanomedicines for parkinson’s disease treatment by intranasal administration. Pharmaceutics. 16, 1048 (2024). [↩]
- J. García-Pardo, A. Novio, J. Nador, A. Cavaliere, S. Suárez-García, A. Lope-Piedrafita, M. Candiota, C. Romero-Giménez, M. Vila, J. Cabana, D. Ruiz-Molina, Bioinspired theranostic coordination polymer nanoparticles for intranasal dopamine replacement in parkinson’s disease. ACS Nano. 15, 8592-8609 (2021). [↩]
- R. Mohammapdour, H. Ghandehari, Mechanisms of immune response to inorganic nanoparticles and their degradation products. Adv Drug Deliv Rev. 180, 114022 (2022). [↩]
- N. M. O’Brown, S. J. Pfau, C. Gu, Bridging barriers: a comparative look at the blood-brain barrier across organisms. Genes Dev. 32, 466-478 (2018). [↩]



{kind=link}