
Abstract
The United States is a unique case among high-income countries for still having a predominantly privatized healthcare system. Although privatization is defended on the basis of efficiency and patient choice, its critics argue that it worsens socioeconomic disparities. This research examines how far U.S. healthcare system privatization reinforces inequality in access, affordability, and health outcome. A mixed-method approach was used, this included a broad literature review combined with formal interviews of healthcare economists and experts. Literature was sourced from peer-reviewed literature, and interview answers were thematically coded across access, equity, efficiency, and reform strategy domains. Findings show that privatization disproportionately affects low-income and marginalized communities. Interview participants highlighted that profit-driven systems promote “cherry-picking” lucrative patients, the shutting down of rural hospitals, and cost-shifting mechanisms worsening financial pressures. Evidence also indicates that for-profit ownership is associated with worse patient outcomes, especially among vulnerable populations. However, respondents recognized that privatization can increase patient choice and decrease wait times in some settings. This research finds that privatization systematically erodes equity in American healthcare, leading to a two-tiered system in which better-off individuals have better access and outcomes. Policy change, e.g., expanding Medicaid, tightening regulation of nonprofit hospitals, and implementing hybrid systems based on Germany or Australia, can slow inequities without completely eliminating private-sector innovation.
Keywords: privatization, U.S. healthcare, socioeconomic inequality, access to care, health policy
Introduction
Healthcare has always been a controversial topic in the United States. There is a plethora of research on this issue, however not many have delved deep into how the U.S. healthcare system has been a direct contributor to growing income inequality, this paper aims to fill that gap and provide arguments for both sides; whether or not privatisation of healthcare has been a successful venture in the U.S. It is imperative to deeply understand the role of privatisation in inequality as only then can it lead to substantial reform recognising healthcare as not just a privilege, but a universal right.
One of the main characteristics of privatised healthcare is that it is individual-owned, profit-driven and has reduced public oversight models. In practice, while this may lead to better quality care for some individuals, it does not guarantee equitable outcomes; this is something that this paper will analyse in detail. Hence, the U.S. healthcare system is characterised by high costs, significant fragmentation, and disparities in access.
The U.S. government first started to lean towards a more privatised system of healthcare during Ronald Reagan’s rule, an administration marked by neoliberal policies. Unlike other wealthy nations such as the U.K. and Sweden, which had adopted a system of institutionalised healthcare, the U.S. went in the opposite direction, and as a result, approximately 80% of the 4,500 general acute care hospitals in the United States are controlled by private non-profit or for-profit organisations.1
The U.S. is unique in the fact that its healthcare system is one of the only among developed nations to be privatised. As a result, this has brought a lot of scrutiny from people worldwide, especially U.S. citizens who have had to suffer the wrath of healthcare firms prioritising profit over patients. Frustration with the U.S. healthcare system has increasingly spilt into public discourse. Many Americans, particularly those with chronic illnesses or facing unaffordable treatments, express growing distrust toward insurance providers and hospital networks. A 2023 Kaiser Family Foundation (KFF) survey found that 51 per cent of U.S. adults reported delaying or forgoing medical care due to cost2
, with the highest rates among uninsured and low-income individuals. Protests against hospital closures, such as those in rural North Carolina and New York, have drawn national media attention and highlighted systemic inequities in healthcare access. These expressions of dissatisfaction reflect a growing sentiment that healthcare in the U.S. has become a commodity inaccessible to working-class and marginalised populations, rather than a guaranteed right.
Most of the data you will come across in this paper will be secondary: collected from various sources such as CMS3 and the World Inequality Data4, as well as primary data collected through online interviews with experts in the field. The research will address several key questions:
- How has privatisation affected access to healthcare for low-income and marginalised populations?
- What impact has privatisation had on the quality and cost of care?
- To what extent has privatisation contributed to socioeconomic inequalities in health outcomes?
- Are there alternative models or reforms that could address these disparities?
The analysis will be structured into thematic sections that investigate the historical evolution of healthcare privatisation, assess its socioeconomic consequences, and propose policy-driven strategies to address systemic inequities. To structure the argument, Section II surveys the literature across themes of access, equity, and efficiency. Section III introduces theoretical tools from political economy and health economics. Section IV outlines the methodology used, while Sections V and VI will be the main summary of our research and what the way forward from here is.
Literature Review
This paper will aim to make the best use of available research on this particular issue. Though there are an overwhelming number of detractors against privatisation, most of whose claims are backed by data, there are still those in favour of healthcare firms being privatised, citing practical theory rather than statistics or trends. This literature review was conducted using academic databases including JSTOR, PubMed, and Google Scholar. Only peer-reviewed studies from the past 20 years were included, with priority given to those focusing on U.S. healthcare and income disparities. Grey literature and opinion pieces were excluded unless cited by multiple empirical studies.
Goodair, B., & Reeves, A.5 were explicit in their critique of privatisation, citing that private healthcare firms go out of their way to admit more privately insured patients than individuals on Medicare or those who are uninsured. In fact, privatised hospitals admitted 25% fewer Medicaid patients and reduced services for low-income groups by 15–20%.5 Although, in practice, private firms will have a profit incentive to increase efficiency and production levels, this may also work the other way around, as mentioned in Goodair, B., & Reeves, A.5, nurses, cleaning staff, and administrative roles were reduced by 10–30% in private healthcare, leading to lower care quality of care. As previously alluded to, one of the major shortcomings of private healthcare is that firms tend to favour urban more than rural areas1, what this does is that people in rural areas are often left to fend for themselves and desperately scamper across to seek health insurance, which usually comes at a substantial financial cost. Private firms, at times, will even seek to cut off unprofitable services such as mental health and addiction services and blatantly aim to redirect resources towards profitable services and away from marginalised groups.6
As the National Center for Biotechnology Information7 reaffirms, it highlights the U.S.’s outlier status among other wealthy nations, spending more per capita yet lagging in health metrics compared to public-system nations, such as the U.K. It argues that the U.S. healthcare system serves as a cautionary tale, citing the astronomical costs it incurs, and despite the so-called profit motives, the U.S. still ranks unfavourably among other public health systems in many key metrics such as life expectancy. The Leonard Davis Institute of Health Economics 8 shows that privatized hospitals admitted 20% fewer uninsured patients post-transition, and that private health firms have seen profits rise by systematically excluding uninsured/underinsured patients, this plays directly into the hands of capitalist sceptics who are firm on the fact that healthcare firms ‘cherry-pick’ profitable patients, exacerbating inequality. In a survey carried out by Alayed, T. M., et al.6, 54.3% of researchers in developed nations opposed privatisation, mainly alluding to the associated reduction in costs and reduced availability for low-income households. Privatisation harms seem to be mostly acute in high-income nations, as Europe reported worsened care quality while Saudi Arabia saw reduced wait times in private hospitals.
In the same survey, 36.4% of scholars and policymakers in developing nations, such as Saudi Arabia and Iran, supported privatisation. As previously mentioned, shorter wait times have been seen in private hospitals, and it has simultaneously attracted investment to modernise infrastructure.
In Gratzer, D.9. The Cure: How Capitalism Can Save American Health Care, Gratzer vehemently advocates for capitalism in healthcare. Gratzer calls for deregulation and consumer empowerment to improve care quality and affordability, arguing that “Market mechanisms, when freed from red tape, align incentives to benefit patients.” One of the examples Gratzer cites is elective surgery centres offering lower prices through competition; he argues that privatisation drives innovation, efficiency, and patient choice by reducing bureaucratic restraints. Additionally, he associates systemic issues, such as high costs, with constant government intervention rather than capitalism itself. While Gratzer puts forward his theory that deregulation fosters innovation, his detractors argue that profit motives undermine equitable access 5
Though in practice, Gratzer’s theories may work, the U.S. has not seen any sign of that, and while Gratzer cites efficiency gains, 54% of privatised hospitals have cut mental health services6.
All in all, there is an overwhelming amount of support against privatisation, and though most of those papers focus on its costs, few explore its direct link to income inequity, which will be this paper’s unique contribution. While most in favour of privatisation cite theories to support their claims, their naysayers use data and trends to show that, particularly in the U.S., people are worse off in a private healthcare system. Alayed, T. M., et al.10 stress upon the fact that privatisation’s impact is deeply context-dependent and that its advantages are neither intrinsically advantageous nor adverse; its success hinges on markets operating at an efficient level along with robust safeguards which protect the interests of vulnerable populations.
These bodies of work show how privatisation amplifies health inequities under certain conditions. To deepen this analysis, the next section applies a theoretical framework informed by John Rawls’ theory of justice11 and Kenneth Arrow’s classic insights on healthcare market failures12
Economic Theory
In theory, the market for healthcare is divided into sections: low-income consumers and high-income consumers.
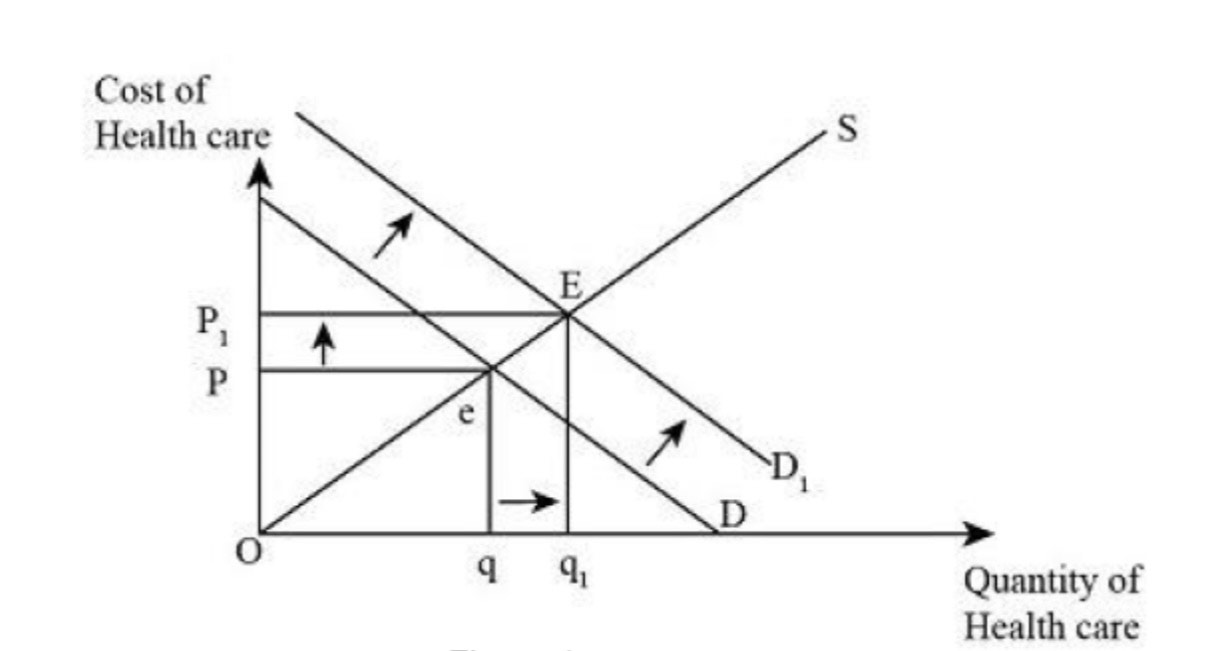
Figure 1, displayed above, is a basic demand and supply graph, illustrating how the price changes when the demand for healthcare rises. Initially, the downward-sloping demand curve and the upward-sloping supply curve meet at a point ‘e’; this point reflects a balance where healthcare is accessible at an affordable cost under public or regulated systems. A shift in demand, represented by the movement from D to D1, causes the equilibrium price to rise from e to E. This surge in demand could result from external factors such as pandemics or increased health awareness. However, price inelasticity is only part of the story. As Kenneth Arrow12 demonstrated, the healthcare market is uniquely prone to failure due to asymmetric information, uncertainty in need, and moral hazard. Providers may overtreat to increase revenue, while patients often cannot evaluate care quality or necessity. These features weaken the assumptions of rational consumer theory. Additionally, John Rawls’ theory of justice posits that systems must prioritise the worse-off, a principle that privatisation often violates by sidelining low-income groups.
Beyond well-known market failures, the U.S. healthcare system has increasingly shifted toward financialization, where hospitals and insurers prioritise profitability and shareholder value over patient outcomes. This trend is evident in the rise of private equity ownership of hospitals, aggressive billing practices, and the consolidation of providers to maximise revenue. At the same time, the system remains dominated by the biomedical model, which treats health primarily through clinical procedures and pharmaceuticals while neglecting social determinants like housing, income, and nutrition. These non-medical factors, which strongly influence health outcomes, are often sidelined in privatised systems that allocate resources based on financial return rather than community need.
In a privatised system, suppliers will capitalise on this heightened demand by increasing prices. As a result, low-income patients, who are already extremely price-sensitive, will have reduced access to care due to prices rising to P1. Low-income households may find it difficult to afford these increased prices and may suffer from worsening health outcomes. On the contrary, wealthier households will be able to absorb these rises in costs, so low-income households will be the ones that suffer the most from this. Additionally, if supply is inflexible, such as due to limited hospital beds, there would be a further escalation in prices, which would significantly harm marginalised groups. This theory falls in line with studies that imply that privatised systems prioritise profitability over equitable access5
. The assumption that efficiency is best measured through profitability or throughput overlooks broader metrics such as equity, long-term health outcomes, and population-level well-being.
One economic theory which stays the same for both income groups is that healthcare will always be a price-inelastic service, meaning that even if the price rises, the demand will still stay the same, as shown in the graph below.

This graph represents a case for a perfectly inelastic good. In this case, the y-axis represents the price of healthcare, while the x-axis represents the quantity of healthcare. As the price goes up, the demand for healthcare stays the same as it is a necessity good and people will need to consume it in any circumstance, this further illustrates how low-income groups are left worse off in a private healthcare system, as previously established by the Stanford Institute for Economic Policy Research 1
Methodology
As briefly touched upon before, this paper will be making use of a structured interview to help answer our research question. This study used structured interviews conducted via email, with a predefined set of questions. An advantage of this type of interview is that the interviewees will be able to answer the questions in their own time and will be able to give as long and detailed an answer as they like. The interview consists of four questions:
- How would you describe the current state of the U.S. healthcare system in terms of accessibility, affordability, and quality?
- To what extent has privatisation contributed to socioeconomic inequalities in healthcare access and treatment?
- How do financial incentives in a privatised healthcare system influence medical decision-making and patient care?
- What policies or reforms could help reduce inequalities in the U.S. healthcare system while maintaining efficiency?
To conduct interviews, 40 healthcare experts and economists were contacted via email. Notable respondents included Professor Mark Pauly from the University of Pennsylvania and Professor Sherry Glied from NYU Wagner School. Interview responses were coded using thematic analysis across four domains: access, equity, efficiency, and reform strategies. Only public statements were used, and no personal or identifying information was collected. The first question, “How would you describe the current state of the U.S. healthcare system in terms of accessibility, affordability, and quality?” aims to establish a basic understanding of the healthcare system by examining three crucial aspects. Accessibility is a major issue attributed to the U.S. healthcare system; for example, nearly 30 million Americans remain uninsured, while even those with insurance often face months-long wait times for specialists. Affordability analyses the financial burden on patients; studies show 40% of Americans avoid seeking treatment due to exorbitant costs. Quality aims to assess outcomes such as patient safety errors, a metric in which the U.S. underperforms compared to peer nations despite spending far more per capita. This will help identify systemic strengths and weaknesses to allow for further discussion.
The second question, “To what extent has privatisation contributed to socioeconomic inequalities in healthcare access and treatment?” delves into how privatisation potentially widens gaps in access and treatment based on income, race, or geography. For instance, privatised insurers often cherry-pick healthier patients to minimise costs. It reflects on whether profit-driven models prioritise certain groups over others, exacerbating disparities in who receives timely, adequate care.
The third question, “How do financial incentives in a privatised healthcare system influence medical decision-making and patient care?” investigates how profit incentives in privatised systems might lead to clinical choices, such as favouring costly treatments or carrying out unnecessary procedures for revenue. Private hospitals may cut spending in rural areas or may direct resources to more affluent neighbourhoods, further worsening the low-quality levels in low-income areas. It raises the question of whether financial goals conflict with ethical care, potentially compromising patient outcomes or equality. The question highlights how market-driven forces worsen existing social inequities.
The fourth question, “What policies or reforms could help reduce inequalities in the U.S. healthcare system while maintaining efficiency?” seeks possible solutions to balancing equity and efficiency. Potential methods include capping out-of-pocket expenses for necessary services, controlling prescription prices to prevent exploitation, and expanding Medicaid in all states to include low-income adults. It invites even more ideas like expanding existing public programs, regulating healthcare prices, or even adopting hybrid models, such as public-private partnerships, that other systems use to achieve both goals.
In short, all these questions will help to lead us to a conclusive answer for our research question. The concepts used in analysis were operationalized as follows: ‘access’ included both geographical and financial barriers to care; ‘equity’ referred to fairness in outcomes across income brackets; ‘profit’ was interpreted in terms of revenue retention versus reinvestment; and ‘efficiency’ focused on service delivery with minimal waste and delay
Results and Discussion
Most of the interviewees were in agreement that privatised healthcare has directly led to uneven access to care between low-income and high-income households. Privatisation has led to a dual system where wealthier individuals can access higher-quality, faster care through private insurance while lower-income groups face barriers to care. Private spending tends to reduce political support for public healthcare funding, potentially worsening disparities.
Key themes from the interview responses included systemic underinsurance, market distortion, rural service loss, and political resistance to reform. It was also reiterated that due to financial incentives, private healthcare encourages cost-shifting, where hospitals charge higher prices to privately insured patients to compensate for lower public reimbursement rates . This system also promotes the overuse of high-margin services while discouraging unprofitable care, affecting equitable access. As Shery Giled notes, “Catastrophic out-of-pocket health care costs disproportionately impact middle-income Americans with employer coverage, with significant financial burdens that challenge affordability.”
They further highlight that privatisation exacerbates medical deserts in rural and minority communities, where hospital closures and service cuts force patients to travel long distances for care. According to the National Rural Health Association 13, over 180 rural hospitals have closed in the U.S. since 2010. States with higher degrees of privatisation experienced steeper declines in rural access. Healthcare’s inherent market failures were also emphasised, rendering profit-driven models incompatible with universal access. For example, a 2023 study in JAMA Pediatrics14 revealed that children treated at for-profit dialysis facilities had a twofold higher risk of death compared to those at nonprofit centres.
Additionally, it was also noted that single-payer-like systems do not do a consistently better job of controlling physician incomes but do achieve some administrative cost savings compared to more fragmented systems. While single-payer systems reduce administrative costs, they don’t always control physician salaries or total healthcare spending better than other universal systems. This, along with the view that privatisation can undermine public healthcare funding, raises concerns about the long-term sustainability of a market-driven healthcare approach. Private insurance often leads to reduced political support for public healthcare spending, which can result in underfunding and weaker access to care for lower-income populations.
Despite the overwhelming support against privatisation, the answers provided by the interviewees did a fair job in providing a balanced argument, citing factors such as privatisation allows for greater patient choice, giving individuals access to a variety of providers, insurance plans, and treatment options rather than being limited to government-funded programs, this can be seen by the fact that in the U.S., people with private insurance often have access to more specialists and faster care compared to those relying on Medicaid. On top of this, single-payer systems in countries like Canada and the UK face longer wait times for non-urgent procedures due to budget constraints.
It is important to acknowledge that the correlation between privatisation and health disparities may be mediated by additional factors, including pre-existing socioeconomic inequalities, geographic variations in infrastructure, and state-level political differences. While this paper identifies strong associations, causation remains complex and partially contingent on contextual variables.
Conclusion
The privatisation of the U.S. healthcare system has had significant effects on access, cost, and equity. While proponents argue that privatisation fosters efficiency, innovation, and patient choice, the evidence overwhelmingly suggests that it has exacerbated socioeconomic inequalities. The findings of this paper reinforce that privatisation disproportionately impacts low-income and marginalised communities by reducing access to affordable care, shifting financial burdens onto patients, and prioritising profitability over equitable health outcomes.
Privatisation’s role in cost-shifting, where hospitals charge higher prices to privately insured patients to compensate for lower public reimbursement rates, further worsens disparities. Additionally, studies have shown that for-profit healthcare systems lead to reduced services for uninsured and Medicaid patients, exacerbating the divide between those with and without comprehensive insurance. This creates a two-tier system where wealthier individuals receive superior care while lower-income groups struggle with affordability and accessibility.
Moving forward, reforms should focus on balancing quality with fairness, ensuring that financial incentives do not compromise healthcare access for marginalised populations. Policies such as raising Medicaid reimbursement rates, increasing oversight of nonprofit hospitals, and expanding public insurance options could help mitigate the negative effects of privatisation while maintaining a level of competition that fosters innovation.
International comparisons confirm that universal healthcare can coexist with strong private-sector participation. Germany’s system of regulated competition combines nonprofit sickness funds and private insurers under government oversight. It achieves near-universal coverage and superior access while spending less per capita than the U.S.15. Australia employs a dual-tier model: public Medicare ensures baseline services, while private insurance offers elective procedures and private hospital access. In 2024, Australia ranked first overall among ten high-income countries according to the Commonwealth Fund’s Mirror, Mirror report16, reflecting excellent equity, administrative efficiency, and health outcomes. By contrast, the U.S. ranked last in overall performance. With more than half of Australians holding private coverage and both nations maintaining strong access and outcomes, these examples show it is possible to combine private innovation with universal equity through careful regulation and public investment.
Ultimately, while privatisation in the U.S. healthcare system is deeply embedded, this paper has shown that its unchecked expansion poses a significant risk to healthcare equity. Without meaningful reform, disparities will likely worsen, undermining the fundamental principle that healthcare should be a universal right rather than a privilege dictated by financial status.
References
- Stanford University, SIEPR. (2021). Study: When public hospitals go private, low-income patients lose. [↩] [↩] [↩]
- KFF (Kaiser Family Foundation). “Health Care Debt in the U.S.: The Broad Consequences of Medical and Dental Bills.” June 16, 2023. https://www.kff.org/health-costs/report/kff-health-care-debt-survey/ [↩]
- CMS. (2023). National Health Expenditure Data. https://www.cms.gov/data-research/statistics-trends-and-reports/national-health-expenditure-data/historical#:~:text=The%20data%20are%20presented%20by,spending%20accounted%20for%2017.6%20percent. [↩]
- World Inequality Database. (2023). United States. https://wid.world/country/usa/ [↩]
- Goodair, B., & Reeves, A. (2024). The Lancet Public Health, 9(3), e199–e206. [↩] [↩] [↩] [↩] [↩]
- The Nation’s Health. (2024). Health care privatization trend raises concerns about inequities. https://www.thenationshealth.org/content/54/8/1.4 [↩] [↩] [↩]
- NCBI. (2008). Privatizing health care is not the answer: Lessons from the United States. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2565716/ [↩]
- Werner, R. M. (2023). Testimony before the Pennsylvania House Health Committee on the impact of hospital privatization. Leonard Davis Institute of Health Economics. Retrieved from https://www.legis.state.pa.us/WU01/LI/TR/Transcripts/2023_0376_0004_TSTMNY.pdf [↩]
- Gratzer, D. (2006). The Cure: How Capitalism Can Save American Health Care. [↩]
- Alayed, T. M., et al. (2024). Saudi Journal of Medicine and Medical Sciences, 12, 125–133. [↩]
- Rawls, J. (1971). A theory of justice. Harvard University Press. [↩]
- Arrow, K. J. (1963). Uncertainty and the welfare economics of medical care. The American Economic Review, 53(5), 941–973. [↩] [↩]
- NRHA. (2025). Top 5 policies to transform rural health.https://www.ruralhealth.us/blogs/2025/01/top-5-policies-to-transform-rural-health [↩]
- Rees, J. M., Tanguturi, V., Erickson, K. F., Shen, J. I., & Winkelmayer, W. C. (2023). Association of for-profit ownership of dialysis facilities with mortality among pediatric patients receiving maintenance dialysis. JAMA Pediatrics, 177(11), 1120-1128. [↩]
- OECD. (2023). Health at a Glance 2023: OECD Indicators. Organisation for Economic Co-operation and Development. https://www.oecd.org/health/health-at-a-glance/ [↩]
- Commonwealth Fund. (2024). *Mirror, Mirror 2024: A Portrait of the Failing U.S. Health System*. Retrieved from https://www.commonwealthfund.org/publications/fund-reports/2024/sep/mirror-mirror-2024 [↩]



{kind=link}