
Abstract
Thyroid eye disease (TED) is a chronic autoimmune disorder characterized by proptosis, diplopia, periorbital edema, and vision impairment, severely impacting patients’ quality of life. Conventional treatment for moderate-to-severe TED, defined by a clinical activity score (CAS) ≥4, proptosis ≥3 mm, and/or diplopia, has been limited to high-dose glucocorticoids, radiotherapy, and surgery. However, advances in understanding TED pathogenesis, particularly the roles of the insulin-like growth factor 1 receptor (IGF-1R) signaling and orbital fibroblast activation, have enabled development of targeted biological therapies including teprotumumab, the first FDA-approved IGF-1R inhibitor. Building upon these developments, this review systematically examines the evolving landscape of TED pathophysiology and its clinical translation. A comprehensive evaluation of emerging targeted therapies reveals both promising efficacy profiles and highlights potential limitations. Concurrent progress in biomarker discovery and mechanistic insights may soon enable more tailored and effective management strategies for TED patients.
Keywords: thyroid eye disease, autoimmune disorder, Graves’ disease, proptosis, teprotumumab
Introduction
First described in the early 1800s, TED, also known as Graves’ orbitopathy (GO), is a significant disorder that commonly occurs in patients with Graves’ disease (GD)1. TED is a significant disorder occurring in roughly 25% to 50% of patients with GD with an estimated prevalence of 2% and an annual incidence rate of 20 cases per 100,000 individuals2,3. Given this high proportion of GD patients developing TED, a substantial population is at risk for ocular complications. The estimated incidence of TED is 5 per 100,000 per year, with a population prevalence of about 155 per 100,0004,5.
TED follows a biphasic course, an active (inflammatory) stage and an inactive (fibrotic) stage. In the active phase, orbital tissues undergo immune-mediated inflammation driven by autoreactive T cells, B cells, and cytokine release. This manifests clinically as eyelid retraction, proptosis, diplopia, periorbital edema, and pain6,7,8. Without intervention, this phase typically lasts 6–24 months before transitioning to the inactive phase, where inflammation resolves but often results in fibrotic remodeling. This causes stable structural complications like restrictive strabismus, eyelid malposition, and in severe cases, optic neuropathy9.
The pathogenesis involves complex interactions among gender, environmental factors, and immune dysregulation, all of which contribute to the disease’s development and severity. Because autoimmunity predominantly affects women, female gender is a strong risk factor: females are three times more likely than males to develop TED10. Among environmental triggers, cigarette smoking is highly significant; smokers have a substantially increased likelihood of developing TED (OR = 4.4, 95% CI 2.88 – 6.73)11,12.
At its essence, TED involves immune dysregulation characterized by a breakdown of self-tolerance, triggering autoreactive T and B cells. These autoreactive immune cells, along with thyroid-stimulating autoantibodies (TSAbs) secreted by B cells, activate orbital fibroblasts. Once activated, fibroblasts recruit additional autoreactive T cells into the orbit. Reciprocal activation occurs between infiltrating T cells and orbital fibroblasts via MHC II and CD40/CD40L signaling pathways, fostering a proinflammatory and profibrogenic environment that promotes connective tissue remodeling13,14. Moreover, autoreactive T cells, upon recognizing antigen presented by B cells, amplify the B-cell response through costimulatory signals, generating pathogenic TSAbs that drive disease progression15.
The treatment of TED currently remains predominantly focused on alleviating its symptoms and is stage dependent. For active TED, high-dose glucocorticoids remain first-line, but provide limited long-term proptosis improvement while posing risks of metabolic complications (e.g., weight gain, diabetes, osteoporosis)16. These medications tend to be more efficacious when administered in the early stages of the disease17. Teprotumumab, the first FDA-approved targeted therapy for both active and inactive TED, inhibits IGF-1R signaling and reduces proptosis and inflammation, but its use faces challenges including high cost, side effects (e.g., hearing impairment), and uncertain efficacy in inactive disease or long-term management. Furthermore, with no currently approved drugs specifically targeting fat expansion or fibrotic remodeling in inactive TED, surgical intervention remains the standard approach to restore visual function and correct disfigurement17.
This review synthesizes evolving insights into TED pathogenesis and the expanding pipeline of novel therapies, critically evaluating their potential to change clinical practice. By exploring connections between molecular drivers and emerging treatments while addressing translational limitations and future directions, this review highlights how the convergence of disease insights, biomarker discovery, and novel targeted therapies may ultimately optimize patient outcomes.
Methods
This review was conducted through a systematic literature search to summarize the molecular mechanisms, standard of care, novel therapies, and biomarker development in TED. The search was performed on PubMed, Google Scholar, and Google Search for relevant studies published between January 1, 1980 and March 1, 2025 to ensure comprehensive coverage of current evidence. A combination of keywords and phrases was employed in the search strategy. The keywords included “thyroid eye disease”, “TED”, “Graves’ ophthalmopathy”, “thyroid stimulating hormone receptor”, “TSHR”, “IGF-1R”, “T/B cell interaction”, “Autoantibodies”, “Orbital fibroblasts”, “Hyaluronan”, “Cytokines”, “IL-6/IL-6R”, “IL-11/IL-11R”, “CD40/CD40L”, “OX40/OX40L”, “FcRn” “Tepezza”, “Linsitinib”, “K1-70”, ‘Efgartigimod”, “Batoclimab”, “Tocilizumab, “Satralizumab”, “Pacibekitug”, and “TED biomarkers”. These terms were carefully selected to cover all critical aspects related to TED pathogenesis, key molecular pathways, novel therapeutic targets, and biomarker discovery.
Inclusion criteria encompassed English-language experimental studies, clinical trials, and comprehensive reviews exploring TED molecular mechanisms, the roles of specified molecules, therapeutic agent effectiveness and safety profiles, advances in biomarkers and precision medicine. Exclusion criteria included studies that did not address the molecular mechanisms of TED, the associated molecules, or the therapeutic strategies related to the keywords. Additionally, studies that lacked sufficient data for a meaningful analysis, such as those with incomplete reporting of experimental results or unclear methodologies, were not included in this review.
Pathogenesis of TED
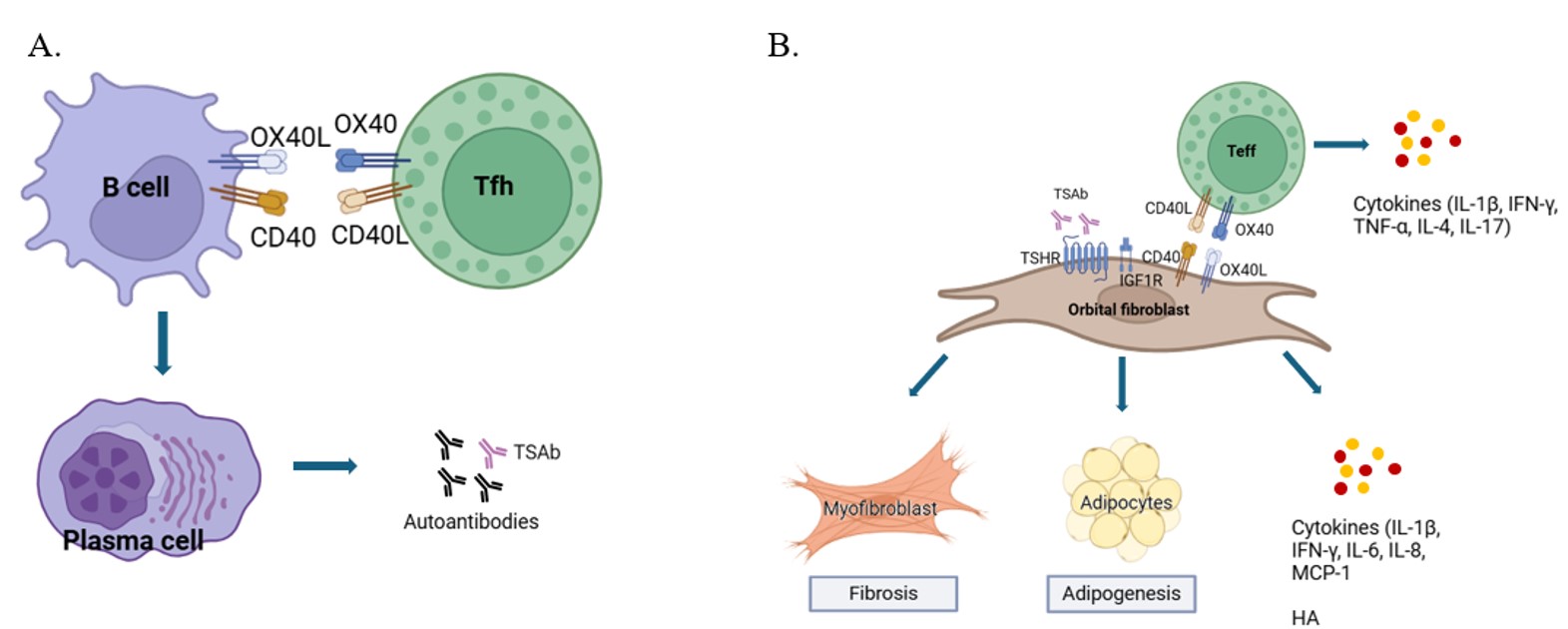
The complex interplay of immune cells, cytokines, and signaling pathways driving both active inflammation and fibrotic remodeling in TED is summarized in Figure 1. Active TED develops through an autoimmune cascade initiated by dysregulated immune cells. Antigen-presenting cells (APCs), such as dendritic cells, recognize autoantigens like the thyroid stimulating hormone receptor (TSHR) and IGF-1R overexpressed on orbital fibroblasts18,19,20. These APCs migrate to draining lymph nodes where they present autoantigens, activating naïve T cells and B cells. This process triggers the generation of follicular helper T cells (Tfh cells), effector T cells, and low-affinity IgM+ B cells21. Elevated Tfh cells, found in circulation and orbital infiltrates and linked to disease severity, critically mediate the B cell response22. CD40L on Tfh cells binds CD40 on B cells, providing essential costimulation alongside antigen recognition, which ultimately drives B cell activation, proliferation, and differentiation into high-affinity TSAb-secreting plasma cells23. Meanwhile, TSHR-autoreactive effector T cells infiltrate the orbit and activate orbital fibroblasts via CD40/CD40L and OX40/OX40L interactions, leading to the secretion of chemokines (e.g., IL-16, CXCL10), proinflammatory cytokines (IL-6, TNF-α), and profibrogenic factors (TGF-β, IL-11)24,25. Among these cytokines, IL-6 plays a central role in promoting B cell activation, plasma cell maturation, and Tfh development, whereas IL-11 drives the terminal differentiation of orbital fibroblasts into myofibroblasts via ERK/STAT3 signaling.
This differentiation process upregulates fibrosis markers (α-SMA, collagen) and promotes extracellular matrix deposition, directly contributing to restrictive strabismus, eyelid malposition, and proptosis26,27. Concurrently, TSAbs binding TSHR activate Gs/Gq signaling, driving excessive synthesis of hyaluronan (HA). As a highly hydrophilic glycosaminoglycan, HA accumulation causes osmotic swelling and tissue expansion in the orbit. Furthermore, IGF-1R signaling, either directly or via crosstalk with TSHR, synergistically enhances HA production through PI3K/Akt and MAPK pathways28. This pathogenic autoantibody activity is prolonged by the neonatal Fc receptor (FcRn), which protects TSAbs from degradation29,30. Taken together, this dysregulated network of B and T cell interactions, sustained CD40/CD40L signaling, T cell-fibroblast crosstalk, TSHR/IGF-1R synergy, excess cytokine production, and FcRn-mediated antibody recycling collectively drives acute orbital inflammation and the pathological tissue expansion characteristic of TED.
As the acute inflammatory phase subsides over months to years, unresolved tissue injury transitions toward chronic, sustained structural alterations, the hallmark of inactive TED. The core pathophysiology shifts from active inflammation to sustained mechanical impact caused by accumulated extracellular matrix components and fibrotic remodeling driven by persistent profibrogenic factors31,26,32. This fibrotic transformation involves continued myofibroblast activity that generates dense scarring within extraocular muscles through excessive collagen deposition and α-SMA expression, coupled with adipogenic fibroblast differentiation that promotes orbital fat expansion33. Residual HA-mediated edema further contributes to ongoing volume expansion. These changes result in structural damage including proptosis (from combined fibrotic fat expansion, muscle enlargement, and residual edema), restrictive myopathy (due to stiffened extraocular muscles impairing ocular motility), and eyelid retraction (resulting from fibrosis of the levator palpebrae superioris and Müller’s muscles)6,34.
Approved Targeted Therapy: Teprotumumab (for active and inactive TED)
The approval of teprotumumab for TED has been a significant breakthrough, offering patients a more effective treatment alternative to traditional glucocorticoid-based therapies. As a targeted biologic, teprotumumab exerts its therapeutic effect by inhibiting IGF-1R, thereby disrupting the pathogenic TSHR/IGF-1R signaling crosstalk in orbital fibroblasts and preventing their activation. The clinical efficacy of teprotumumab for both active inflammatory TED and chronic, low-activity disease is supported by two pivotal randomized controlled trials (RCTs). In the OPTIC study (NCT03298867), patients with active TED, defined as CAS ≥4 and disease duration <9 months, who received teprotumumab (N = 41) showed significantly greater improvements in proptosis, diplopia, and quality of life versus placebo (N = 42)35. Specifically, teprotumumab treatment resulted in a mean proptosis reduction of 2.82 mm compared to 0.54 mm with placebo, with 83% of treated patients achieving ≥2 mm improvement (versus only 10% of placebo patients). Significant benefits were also seen in diplopia (68% improvement vs 29%) and quality of life (GO-QOL score improvement of +13.8 vs +4.4). Despite these positive results, the modest cohort sizes limit statistical power for subgroup analyses and rare adverse event detection, while strict exclusion criteria (e.g., optic neuropathy, prior steroid use, or spontaneous improvement pre-baseline) constrain generalizability to severe or treatment-experienced cases. Importantly, teprotumumab’s benefits extend beyond acute disease. The subsequent Phase 4 trial (NCT04583735) demonstrated its efficacy in chronic TED (disease duration 2–10 years, CAS ≤1), with treated patients (N = 42) achieving a mean proptosis reduction of 2.41 mm versus 0.92 mm in the placebo group (N = 20), and a response rate of 62% versus 25%36.
Furthermore, analysis of long-term follow-up data for teprotumumab from pooled open-label extension studies of three clinical studies showed sustained improvements up to 51 weeks post-treatment37. Key findings included high responder rates for CAS (91.2%), diplopia (72.9%), and proptosis (67.9%), alongside significant quality-of-life enhancements37. However, durability analyses revealed that 37% (11/30) of patients who initially responded to teprotumumab treatment in the OPTIC trial experienced proptosis relapse during the 48-week follow-up period, though 60% of these patients responded again to retreatment. These findings position teprotumumab as an important advancement in active and chronic TED treatment, though longer-term studies with larger cohorts are needed to fully evaluate sustained efficacy and optimal retreatment approaches.
Despite its efficacy, teprotumumab is associated with various adverse effects, including muscle spasms, nausea, alopecia, diarrhea, and fatigue. Hyperglycemia (8-15% of patients) and hearing impairment (12–20% of patients) are particularly concerning and have prompted FDA warning labels for both effects38,39,40. The hyperglycemia risk stems directly from teprotumumab’s mechanism of action by inhibiting IGF-1R and interfering with insulin-mediated glucose regulation41. Therefore, diabetic patients require close monitoring and may need adjusted glycemic control during treatment. Equally noteworthy are the auditory complications, which were reported in 12% of patients in the Phase 2/3 trials and up to 22% in chronic TED patients with most cases being reversible. However, emerging evidence suggests hearing impairment may be more frequent than initially reported, with some cases progressing to permanent hearing loss42,43,44. The risk appears substantial, as teprotumumab use is associated with a 24-fold increased likelihood of any hearing disorder45. Clinical observations reveal that approximately 50% of patients with abnormal baseline audiometry experience significant hearing deterioration during treatment46. The spectrum of auditory effects ranges from mild symptoms like tinnitus and ear fullness to profound deafness. This ototoxicity likely reflects the drug’s on-target effects, given IGF-1’s well-established role in auditory function. Preclinical models show that IGF-1-deficient mice develop premature hearing loss due to inner ear degeneration, while humans with IGF-1 deficiencies (e.g., Laron syndrome) frequently exhibit hearing impairment47,48. Given these risks, baseline audiometry and ototoxicity monitoring are strongly recommended for teprotumumab treatment.
Emerging targeted therapies in clinical development
Therapies targeting active inflammatory TED
IGF-1R small molecule inhibitors
The emergence of oral IGF-1R small-molecule inhibitors marks a strategic shift in TED therapy, addressing the intravenous dosing limitations of teprotumumab. Linsitinib, a potent tyrosine kinase inhibitor, binds the IGF-1R cytoplasmic domain to disrupt TSHR/IGF-1R crosstalk and downstream signaling pathways49. Recently, the Phase 2b/3 LIDS trial (NCT05276063) evaluating linsitinib in active, moderate-to-severe TED reported topline results: oral administration (150 mg twice daily) achieved a statistically significant 52% proptosis responder rate (≥2 mm reduction at week 24) versus placebo50. While this represents a clinically meaningful effect approaching teprotumumab’s benchmark despite differential administration routes, additional studies will be needed to fully characterize linsitinib’s safety profile and long-term efficacy compared to existing therapies.
TSHR antagonists
Since the pathogenesis of TED involves improper TSHR activation on orbital fibroblasts by TSAbs, blocking this interaction represents a promising therapeutic strategy. This approach is exemplified by K1-70, a high-affinity human monoclonal TSHR-blocking antibody that prevents receptor stimulation by TSAbs51. Recent Phase I clinical trial data (NCT02904330) in 18 Graves’ disease patients (44% with orbitopathy) demonstrated K1-70’s favorable safety profile, with no serious adverse events reported and only mild-moderate fatigue and diarrhea observed52. K1-70 showed clear dose-dependent pharmacodynamic effects. Doses of 25 mg IM, 50 mg IV, and 150 mg IV consistently reduced free triiodothyronine/free thyroxine while elevating thyroid stimulating hormone within 28 days, confirming target engagement. Notably, 8/18 subjects showed clinically meaningful TED improvements, including reductions in proptosis (up to 8 mm), decreased conjunctival redness, and resolution of photosensitivity and grittiness, with benefits persisting beyond the 100-day study period. These early positive results suggest K1-70’s potential to ameliorate both thyroid dysfunction and orbital pathology; however, they require further confirmation in controlled Phase II studies.
FcRn antagonists
FcRn antagonists offer a novel therapeutic strategy for TED by interfering with immunoglobulin G (IgG) salvage pathways. FcRn mediates IgG protection from lysosomal degradation, thereby extending the half-life of pathogenic TSAbs that drive TED pathogenesis29,53. By blocking FcRn, these therapies promote accelerated degradation of pathogenic autoantibodies. Efgartigimod, an engineered Fc fragment that blocks IgG salvage via FcRn binding and approved for other autoantibody-mediated diseases, is currently being evaluated in a Phase 3 TED trial (NCT06307613), with results expected in 202754,55. Similarly, batoclimab, an anti-FcRn antibody, demonstrated potent pharmacodynamic effects in two clinical trials (NCT03922321, NCT03938545)56. Treatment resulted in rapid, dose-dependent reductions in total IgG (75–80% with 680 mg; P <0.001) and TSH receptor autoantibodies (30–60%; P <0.05–0.001). Early proptosis improvements were observed at weeks 4–13 (P <0.05), and significant reductions in orbital muscle volume occurred at week 12 (−4.1 cc with 680 mg; P <0.03). However, the primary endpoint (week 12 proptosis response) was not met due to early trial termination due to unanticipated LDL-C elevations (59% with 680 mg; P <0.001). While early results have been mixed, the rationale for FcRn antagonism in TED remains compelling because it directly targets the autoimmune mechanism through depletion of pathogenic TSAbs. Nevertheless, confirmation of safety and robust efficacy for key endpoints such as proptosis reduction will require Phase 3 trial results.
IL-6/IL-6R antagonists
The IL-6 pathway has emerged as a promising therapeutic target in TED, supported by its well-established role in disease pathogenesis. Tocilizumab, a first-generation IL-6 receptor antibody, has demonstrated therapeutic potential in clinical trials. In an investigator-initiated randomized trial (NCT01297699), tocilizumab demonstrated superior efficacy versus placebo in corticosteroid-resistant TED patients with 93.3% achieving ≥2-point CAS reduction compared to 58.8% in the control group. Notably, 86.7% reached inactive disease status (CAS <3) and reduced proptosis (−1.5 mm)57. These findings were reinforced by an observational study of 12 patients with active, corticosteroid-resistant, moderate-to-severe TED, where all participants achieved both at least a 2-point CAS reduction and inactive disease (CAS <3) within six weeks of treatment58. However, both studies noted limitations, including modest effects on diplopia, small sample sizes, short follow-up (≤40 weeks), and exclusion of high-risk groups (e.g., smokers). The safety profile appeared generally acceptable, with transient hypercholesterolemia and rare infections being the most notable adverse events. Development of newer anti-IL-6 agents continues, though clinical data remain preliminary. Satralizumab, an anti-IL-6 antibody with extended half-life, is currently being evaluated in two Phase 3 trials (NCT05987423, NCT06106828) in patients with both active and inactive TED. Its prospect of monthly dosing regimen may offer advantages in patient convenience and compliance59. Similarly, pacibekitug or TOUR-006, previously known as PF-04236921, is a fully human monoclonal anti-IL-6 antibody and now undergoing Phase 2b development60. Importantly, neither agent has completed pivotal trials for TED indication, and their efficacy and safety profiles in this specific population are not yet established.
CD40/CD40L antagonists
Inhibition of CD40/CD40L signaling presents a multipronged therapeutic opportunity in TED as it targets several disease mechanisms including activation of B cells, induction of pathogenic TSAb secretion, and direct activation of orbital fibroblasts. Early clinical support for this approach comes from a Phase 2 trial of iscalimab (NCT02713256), an anti-CD40 monoclonal antibody, in Graves’ disease patients (N = 15). Treatment (10 mg/kg IV every 2–4 weeks for 12 weeks) yielded significant thyroid hormone normalization without rescue medication in 7 patients (47%), and universal reductions in TSAbs (mean 66% reduction, P <0.001)61. Of particular interest, two patients with coexisting orbitopathy exhibited improvements in eye symptoms following treatment. However, iscalimab’s efficacy in TED remains preliminary. Similarly, Lu AG22515, a novel anti-CD40L single-chain variable fragment fusion protein, is currently undergoing Phase 1b evaluation for TED (NCT06557850)62. As of now, no clinical efficacy data have been reported for this agent.
Therapies targeting fibrosis and orbital remodeling
IL-11 antagonist
An emerging strategy to address irreversible fibrotic remodeling in chronic/inactive TED focuses on IL-11, which is significantly elevated in the serum and orbital connective tissues of TED patients, with levels correlating with CAS and disease severity25. Moreover, the therapeutic rationale is further strengthened by the predominant expression of IL-11Rα on orbital fibroblasts. Preclinical studies have demonstrated that anti-IL-11 antibodies effectively inhibit myofibroblast differentiation and collagen synthesis in vitro, suggesting therapeutic potential for preventing or reversing established fibrosis. Early clinical evaluation is now underway with the Phase 1/2a trial of LASN01 (NCT05331300), which is assessing safety, tolerability, efficacy, and pharmacokinetics in healthy subjects as well as patients with pulmonary fibrosis or TED63. Unlike conventional anti-inflammatory therapies, IL-11 antagonism offers a pathway-specific strategy targeting fibrotic progression.
Comparative analysis of therapeutic options and treatment selection framework
The rapidly evolving therapeutic landscape for moderate-severe TED necessitates a nuanced approach to treatment selection, balancing efficacy, safety, accessibility, and disease phase-specific considerations. Current options span conventional immunosuppressants, targeted biologics, and surgical interventions, each with distinct risk-benefit profiles64. For active inflammatory TED, disease management prioritizes immunosuppression to halt immune-mediated orbital damage. Glucocorticoids serve as a cost effective first-line anti-inflammatory anchor, effectively suppressing immune activity in 58-83% of patients65,66. However, their utility is constrained by minimal impact on proptosis or diplopia and significant metabolic risks (hepatotoxicity at >8 g cumulative doses)67,68. In contrast, teprotumumab demonstrates superior efficacy for proptosis reduction (83% vs. 10% placebo) and diplopia improvement (68% vs. 29%), positioning it as the preferred option for moderate-to-severe TED with significant proptosis or diplopia35. However, clinicians must balance its efficacy against substantial costs and risks of ototoxicity and hyperglycemia, which require baseline audiometry and glycemic monitoring. Radiotherapy offers an alternative for progressive diplopia unresponsive to pharmacotherapy but is contraindicated in patients <35 years or with diabetic retinopathy due to theoretical carcinogenic and retinopathy risks.
Emerging oral and targeted agents show promise but remain investigational. Linsitinib offers convenience over IV-administered teprotumumab. However, its efficacy trails teprotumumab’s benchmarks, and long-term safety data are pending. K1-70 reduced proptosis by up to 8 mm in early trials, but its Phase 1 status warrants validation in larger controlled studies. Tocilizumab shows promise in steroid-refractory cases (93.3% CAS reduction vs. 58.8% placebo) but requires long-term data on diplopia and fibrosis. Efgartigimod, currently in Phase 3 trials for TED, accelerates degradation of pathogenic TSAbs, potentially disrupting core autoimmune drivers without ototoxicity. However, its clinical efficacy in TED remains unconfirmed.
In chronic inactive TED, the therapeutic focus shifts to surgical rehabilitation for irreversible structural sequelae69. Surgical rehabilitation follows a strict sequence: orbital decompression for proptosis, strabismus surgery for diplopia, and eyelid correction for retraction. These interventions are performed only after achieving euthyroidism and disease stability, as surgery during active disease exacerbates inflammation and compromises outcomes70,71. The emerging anti-fibrotic biologic LASN01 represents a novel intervention for fibrosis, but its Phase 1/2a status necessitates cautious optimism pending robust clinical validation.
Discussion
TED presents significant therapeutic challenges due to its biphasic nature, transitioning from an active inflammatory phase driven by complex immune pathways to a chronic fibrotic phase. While teprotumumab’s IGF-1R inhibition represents a landmark advancement with proven efficacy, its high incidence of hearing loss along with systemic side effects like hyperglycemia underscores the vulnerability of on-target, off-tissues to IGF-1R inhibition in TED. This mechanistic insight informs future development of novel therapies, prioritizing next-generation IGF-1R antibodies with enhanced tissue selectivity for orbital fibroblasts or alternative non-IGF-1R targeting mechanisms. One conceptual strategy could involve a bispecific antibody design that simultaneously targets IGF-1R and fibroblast activation protein (FAP), a cell surface marker predominantly expressed on activated fibroblasts during the fibroinflammatory phase of TED72. By leveraging FAP’s restricted expression in activated fibroblasts, this approach may mitigate hair cell toxicity. FAP has emerged as a potential delivery target in multiple fibrotic diseases, though investigations into FAP-directed optimization of IGF-1R antagonists for TED remain unexplored73,74. Meanwhile, the therapeutic pipeline continues to diversify with several non-IGF-1R targeted agents in clinical development. These emerging therapies, if successfully developed, could significantly expand treatment options for both active and chronic TED patients, particularly those unsuitable for current IGF-1R-targeted therapies.
Additionally, teprotumumab’s efficacy is often limited by disease relapse, potentially linked to persistent memory B cells and long-lived plasma cells that sustain autoantibody generation75. Given the role of IL-6 in driving B cell proliferation, differentiation into plasma cells, and antibody production, tocilizumab has been shown to decrease memory B cell populations and reduce immunoglobulin levels in autoimmune diseases like SLE and RA76. This suggests a theoretical rationale for combining teprotumumab with tocilizumab or making a bispecific antibody, which could potentially target both orbital fibroblast activation via IGF-1R inhibition and modulating humoral immune responses via IL-6 blockade. Supporting this approach, in vitro studies have revealed that teprotumumab only partially inhibits IL-6 production by activated human fibroblasts, indicating that supplementary IL-6 blockade could offer additional therapeutic benefits77. Such a dual-targeting strategy may achieve synergistic suppression of disease mechanisms while enabling dose reduction of both agents, potentially decreasing the risk of ototoxicity and other adverse effects.
Beyond biological complexities, the therapeutic landscape for TED is also shaped by economic realities that starkly impact patient access. As the first FDA-approved biologic for TED, teprotumumab’s pricing model, unmatched by direct competitors, creates significant financial barriers for patients78. A single vial in the US costs between $14,900 and 16,300, and the 24-week treatment requires 8 infusions. Even with insurance, out-of-pocket costs from co-pays, deductibles, and coinsurance impose a heavy burden, while limited coverage or resource constraints in lower-income settings often deny access to this new therapy79. Compounding the issue, the absence of robust cost-effectiveness studies comparing novel biologics to standard therapies such as glucocorticoids renders it difficult to justify premium pricing. Without transparent reimbursement strategies or value-based models, healthcare providers face ethical dilemmas in balancing therapeutic efficacy with economic sustainability for patients and healthcare systems.
Parallel to these economic challenges, TED diagnosis faces persistent limitations. To date, no robust biomarker has yet achieved the robustness needed for rapid TED diagnosis or treatment outcome prediction, but recent advances in biomarker discovery hold promise to improve TED management. Currently, thyrotropin receptor antibodies (TRAbs) remain the only validated biomarker in clinical use for GD and TED. High TRAb levels are associated with development of TED in patients with GD, and TRAb levels are correlated with inflammatory activity80,81. However, its clinical utility for TED is limited since high TRAb titers do not reliably predict TED development in all GD patients. TSAbs are more specific for stimulatory antibodies and correlate better with TED severity and specificity82. Elevated TSAb levels may serve as a strong indicator that patients are likely to respond favorably to TSHR and FcRn antagonists which disrupt autoantibody-driven fibroblast activation and reduce pathogenic antibody persistence. The cytokine profile in TED patients reveals additional potential biomarkers, with IL-6 levels demonstrating strong correlation with CAS and potentially guiding anti-IL-6 therapy use83,84,85. For fibrosis progression, elevated TGF-β and IL-11 levels are emerging as valuable indicators of fibrosis severity and potential predictors of response to anti-fibrotic treatments25. While no biomarker has yet achieved ideal diagnostic or prognostic performance, these advances represent significant progress toward personalized TED management.
In summary, the treatment paradigm for TED is evolving from broad immunosuppression toward precision therapies targeting disease-specific pathways. While teprotumumab’s success confirms IGF-1R inhibition as a validated approach, its limitations, including ototoxicity, relapse risk, and high cost, highlight the need for alternative strategies. Emerging agents against TSHR, FcRn, IL-6, and CD40/CD40L offer more specific modulation of both inflammation and fibrotic processes, while oral options like linsitinib may improve treatment adherence. Concurrent advances in biomarker research, particularly the characterization of TSAb, IL-6, and TGF-β profiles are paving the way for more tailored approaches to TED management. As clinical evidence grows, the combination of pathway-specific treatments with patient characteristics could lead to improved outcomes across different disease stages, from active inflammation to chronic fibrosis, with potentially fewer adverse effects.

| Abbreviation | Full Name |
| APC | Antigen-Presenting Cell |
| CAS | Clinical Activity Score |
| FAP | Fibroblast Activation Protein |
| FcRn | Neonatal Fc Receptor |
| GO | Graves’ Orbitopathy |
| HA | Hyaluronan |
| IGF-1R | Insulin-like Growth Factor-1 Receptor |
| RCT | Randomized Controlled Trial |
| TED | Thyroid Eye Disease |
| Tfh | T Follicular Helper (cell) |
| TRAb | Thyrotropin Receptor Antibodies |
| TSAb | Thyroid-Stimulating Antibodies |
| TSHR | Thyroid-Stimulating Hormone Receptor |
| Note: | |
| TSAb (stimulatory) is a subset of TRAb (includes blocking/neutral antibodies) | |
References
- H. Bürgi, Thyroid eye disease: a historical perspective. Orbit, 28 226-230 (2009). [↩]
- J. Muñoz-Ortiz, M. C. Sierra-Cote, E. Zapata-Bravo, L. Valenzuela-Vallejo, M. A. Marin-Noriega, P. Uribe-Reina, J. P. Terreros-Dorado, M. Gómez-Suarez, K. Arteaga-Rivera and A. De-La-Torre, Prevalence of hyperthyroidism, hypothyroidism, and euthyroidism in thyroid eye disease: a systematic review of the literature. Systematic reviews, 9 1-12 (2020 [↩]
- J. A. Garrity and R. S. Bahn, Pathogenesis of graves ophthalmopathy: implications for prediction, prevention, and treatment. Am J Ophthalmol, 142 {HYPERLINK “https://www.ncbi.nlm.nih.gov/pubmed/16815265”} 147-153 (2006). [↩]
- L. Bartalena, E. Piantanida, D. Gallo, A. Lai and M. L. Tanda, Epidemiology, natural history, risk factors, and prevention of Graves’ orbitopathy. Frontiers in Endocrinology, 11 615993 (2020 [↩]
- L. Boulakh, B. Nygaard, T. Bek, J. Faber, S. Heegaard, P. B. Toft, H. E. Poulsen, A. P. Toft-Petersen, H. B. Hesgaard and C. Ellervik, Nationwide incidence of thyroid eye disease and cumulative incidence of strabismus and surgical interventions in Denmark. JAMA ophthalmology, 140 667-673 (2022). [↩]
- T. H. Osaki, L. G. Monteiro and M. H. Osaki, Management of eyelid retraction related to thyroid eye disease. Taiwan Journal of Ophthalmology, 12 12-21 (2022 [↩] [↩]
- A. C. Chang, M. A. Ting, C. Y. Liu, D. O. Kikkawa and B. S. Korn, Managing the esthetic patient with thyroid eye disease. International Ophthalmology Clinics, 61 161-173 (2021 [↩]
- L. Bartalena, Prevention of Graves’ ophthalmopathy. Best Practice & Research Clinical Endocrinology & Metabolism, 26 371-379 (2012). [↩]
- J. M. Neigel, J. Rootman, R. I. Belkin, R. A. Nugent, S. M. Drance, C. W. Beattie and J. A. Spinelli, Dysthyroid optic neuropathy: the crowded orbital apex syndrome. Ophthalmology, 95 1515-1521 (1988). [↩]
- S. Ramesh, J. Sharpe, R. Penne, J. Haller, F. Lum, A. Y. Lee, C. S. Lee, S. Pershing, J. W. Miller and A. Lorch, Thyroid eye disease and its vision-threatening manifestations in the academy IRIS registry: 2014-2018. American journal of ophthalmology, 253 74-85 (2023). [↩]
- M. F. Prummel and W. M. Wiersinga, Smoking and risk of Graves’ disease. JAMA, 269 479-482 (1993 [↩]
- P. Vestergaard, Smoking and thyroid disorders–a meta-analysis. European Journal of Endocrinology, 146 153-161 (2002). [↩]
- S. E. Feldon, D. J. Park, C. W. O’Loughlin, V. T. Nguyen, S. Landskroner-Eiger, D. Chang, T. H. Thatcher and R. P. Phipps, Autologous T-lymphocytes stimulate proliferation of orbital fibroblasts derived from patients with Graves’ ophthalmopathy. Investigative Ophthalmology & Visual Science, 46 3913-3921 (2005 [↩]
- Y. Hiromatsu, D. Yang, T. Bednarczuk, I. Miyake, K. Nonaka and Y. Inoue, Cytokine profiles in eye muscle tissue and orbital fat tissue from patients with thyroid-associated ophthalmopathy. The Journal of Clinical Endocrinology & Metabolism, 85 1194-1199 (2000). [↩]
- G. M. Lehmann, S. E. Feldon, T. J. Smith and R. P. Phipps, Immune mechanisms in thyroid eye disease. Thyroid, 18 959-965 (2008). [↩]
- R. Pofi, G. Caratti, D. W. Ray and J. W. Tomlinson, Treating the side effects of exogenous glucocorticoids; can we separate the good from the bad? Endocrine Reviews, 44 975-1011 (2023). [↩]
- M. Moledina, E. M. Damato and V. Lee, The changing landscape of thyroid eye disease: current clinical advances and future outlook. Eye, 1-13 (2024). [↩] [↩]
- R. Fernando, O. Caldera and T. J. Smith, Therapeutic IGF-I receptor inhibition alters fibrocyte immune phenotype in thyroid-associated ophthalmopathy. Proceedings of the National Academy of Sciences, 118 e2114244118 (2021 [↩]
- A. Feliciello, I. Ciullo, G. Fenzi, G. Bonavolonta, A. Porcellini and E. Avvedimento, Expression of thyrotropin-receptor mRNA in healthy and Graves’ disease retro-orbital tissue. The Lancet, 342 337-338 (1993 [↩]
- A. E. Heufelder and R. S. Bahn, Evidence for the presence of a functional TSH-receptor in retroocular fibroblasts from patients with Graves’ ophthalmopathy. Experimental and Clinical Endocrinology & Diabetes, 100 62-67 (1992). [↩]
- H. Drexhage, Are there more than antibodies to the thyroid-stimulating hormone receptor that meet the eye in Graves’ disease? Endocrinology, 147 9-12 (2006). [↩]
- H. Bisnauthsing, H. Y. E. Chan, H. Y. M. Chan, C. Y. S. So, W. X. Chen, H. K. Ng, S. C. J. Cheng, C. C. Pang, C. C. Tham and K. C. Kam-lung, An abundance of follicular helper T cells in peripheral blood associated with thyroid stimulating immunoglobulin level in the thyroid eye disease. Investigative Ophthalmology & Visual Science, 64 423-423 (2023). [↩]
- M. A. Mintz and J. G. Cyster, T follicular helper cells in germinal center B cell selection and lymphomagenesis. Immunological Reviews, 296 48-61 (2020). [↩]
- A. E. Kuriyan, R. P. Phipps and S. E. Feldon, The eye and thyroid disease. Current Opinion in Ophthalmology, 19 499-506 (2008 [↩]
- P. Wu, B. Lin, S. Huang, J. Meng, F. Zhang, M. Zhou, X. Hei, Y. Ke, H. Yang and D. Huang, IL-11 Is Elevated and Drives the Profibrotic Phenotype Transition of Orbital Fibroblasts in Thyroid-Associated Ophthalmopathy. Frontiers in Endocrinology, 13 846106 (2022). [↩] [↩] [↩]
- P. Wu, B. Lin, S. Huang, J. Meng, F. Zhang, M. Zhou, X. Hei, Y. Ke, H. Yang and D. Huang, IL-11 Is Elevated and Drives the Profibrotic Phenotype Transition of Orbital Fibroblasts in Thyroid-Associated Ophthalmopathy. Frontiers in Endocrinology, 13 846106 (2022 [↩] [↩]
- P. Travers, M. J. Walport, C. Janeway and K. P. Murphy, Janeway’s Immunobiology. (2008). [↩]
- C. C. Krieger, S. Neumann, R. F. Place, B. Marcus-Samuels and M. C. Gershengorn, Bidirectional TSH and IGF-1 receptor cross talk mediates stimulation of hyaluronan secretion by Graves’ disease immunoglobins. The Journal of Clinical Endocrinology & Metabolism, 100 1071-1077 (2015). [↩]
- R. J. Ober, C. Martinez, C. Vaccaro, J. Zhou and E. S. Ward, Visualizing the site and dynamics of IgG salvage by the MHC class I-related receptor, FcRn. The Journal of Immunology, 172 2021-2029 (2004 [↩] [↩]
- D. C. Roopenian, G. J. Christianson, T. J. Sproule, A. C. Brown, S. Akilesh, N. Jung, S. Petkova, L. Avanessian, E. Y. Choi and D. J. Shaffer, The MHC class I-like IgG receptor controls perinatal IgG transport, IgG homeostasis, and fate of IgG-Fc-coupled drugs. The Journal of Immunology, 170 3528-3533 (2003). [↩]
- G. M. Lehmann, S. E. Feldon, T. J. Smith and R. P. Phipps, Immune mechanisms in thyroid eye disease. Thyroid, 18 959-965 (2008 [↩]
- S. Ugradar, J. Kang, A. L. Kossler, E. Zimmerman, J. Braun, A. R. Harrison, S. Bose, K. Cockerham and R. S. Douglas, Teprotumumab for the treatment of chronic thyroid eye disease. Eye, 36 1553-1559 (2022). [↩] [↩]
- A. E. Kuriyan, R. P. Phipps and S. E. Feldon, The eye and thyroid disease. Current Opinion in Ophthalmology, 19 499-506 (2008). [↩]
- M. J. Davies and P. J. Dolman, Levator muscle enlargement in thyroid eye disease-related upper eyelid retraction. Ophthalmic Plastic & Reconstructive Surgery, 33 35-39 (2017). [↩]
- R. S. Douglas, G. J. Kahaly, A. Patel, S. Sile, E. H. Thompson, R. Perdok, J. C. Fleming, B. T. Fowler, C. Marcocci and M. Marinò, Teprotumumab for the treatment of active thyroid eye disease. New England Journal of Medicine, 382 341-352 (2020). [↩] [↩]
- R. S. Douglas, S. Couch, S. T. Wester, B. T. Fowler, C. Y. Liu, P. S. Subramanian, R. Tang, Q. T. Nguyen, R. N. Maamari and S. Ugradar, Efficacy and safety of teprotumumab in patients with thyroid eye disease of long duration and low disease activity. The Journal of Clinical Endocrinology & Metabolism, 109 25-35 (2024). [↩]
- G. J. Kahaly, P. S. Subramanian, E. Conrad, R. J. Holt and T. J. Smith, Long-term efficacy of teprotumumab in thyroid eye disease: follow-up outcomes in three clinical trials. Thyroid, 34 880-889 (2024). [↩] [↩]
- R. S. Douglas, G. J. Kahaly, A. Patel, S. Sile, E. H. Thompson, R. Perdok, J. C. Fleming, B. T. Fowler, C. Marcocci and M. Marinò, Teprotumumab for the treatment of active thyroid eye disease. New England Journal of Medicine, 382 341-352 (2020 [↩]
- R. S. Douglas, S. Couch, S. T. Wester, B. T. Fowler, C. Y. Liu, P. S. Subramanian, R. Tang, Q. T. Nguyen, R. N. Maamari and S. Ugradar, Efficacy and safety of teprotumumab in patients with thyroid eye disease of long duration and low disease activity. The Journal of Clinical Endocrinology & Metabolism, 109 25-35 (2024 [↩]
- F. A. Mukit, A. Manley, A. B. Patel, M. Hashemi, J. F. Laplant, J. C. Fleming, B. T. Fowler, J. Laplant and B. Fowler, Side Effects and Adverse Events After Treatment With Teprotumumab for Thyroid Eye Disease: A Retrospective Observational Case Series. Cureus, 16 (2024). [↩]
- L. Amarikwa, A. Mohamed, S. H. Kim, A. L. Kossler and C. Dosiou, Teprotumumab-related hyperglycemia. The Journal of Clinical Endocrinology & Metabolism, 108 858-864 (2023). [↩]
- J. A. Keen, T. Correa, C. Pham, A. D. Claussen, M. R. Hansen, K. D. Carter and E. M. Shriver, Frequency and patterns of hearing dysfunction in patients treated with teprotumumab. Ophthalmology, 131 30-36 (2024 [↩]
- I. Belinsky, F. X. Creighton Jr, N. Mahoney, C. K. Petris, A. B. Callahan, A. A. Campbell, M. Kazim, H. H. Lee, M. K. Yoon and L. R. D. Glass, Teprotumumab and hearing loss: case series and proposal for audiologic monitoring. Ophthalmic Plastic & Reconstructive Surgery, 38 73-78 (2022 [↩]
- C. M. Sears, A. D. Azad, L. Amarikwa, B. H. Pham, C. J. Men, D. N. Kaplan, J. Liu, A. R. Hoffman, A. Swanson and J. Alyono, Hearing dysfunction after treatment with teprotumumab for thyroid eye disease. American Journal of Ophthalmology, 240 1-13 (2022). [↩]
- G. McGwin Jr, C. Owsley and M. G. Vicinanzo, Teprotumumab-Related Hearing Loss: A Large-Scale Analysis and Review of Voluntarily Reported Patient Complaints to the Food and Drug Administration (FDA). Ophthalmic Plastic & Reconstructive Surgery, 40 639-642 (2024). [↩]
- R. S. Douglas, E. Parunakian, J. Tolentino, E. Malkhasyan, J. Geng, M. Sherman and S. Ugradar, A prospective study examining audiometry outcomes following teprotumumab treatment for thyroid eye disease. Thyroid, 34 134-137 (2024). [↩]
- Á. García-Mato, B. Cervantes, S. Murillo-Cuesta, L. Rodríguez-de la Rosa and I. Varela-Nieto, Insulin-like growth factor 1 signaling in mammalian hearing. Genes, 12 1553 (2021 [↩]
- J. Attias, O. Zarchi, B. I. Nageris and Z. Laron, Cochlear hearing loss in patients with Laron syndrome. European Archives of Oto-Rhino-Laryngology, 269 461-466 (2012). [↩]
- M. J. Mulvihill, A. Cooke, M. Rosenfeld-Franklin, E. Buck, K. Foreman, D. Landfair, M. O’Connor, C. Pirritt, Y. Sun and Y. Yao, Discovery of OSI-906: a selective and orally efficacious dual inhibitor of the IGF-1 receptor and insulin receptor. Future Medicinal Chemistry, 1 1153-1171 (2009). [↩]
- Sling Therapeutics Announces Positive Topline Results from Phase 2b/3 LIDS Clinical Trial of Oral Small Molecule Linsitinib in Patients with Thyroid Eye Disease. {HYPERLINK “https://www.slingtx.com/2025/01/14/sling-therapeutics-announces-positive-topline-results-from-phase-2b-3-lids-clinical-trial-of-oral-small-molecule-linsitinib-in-patients-with-thyroid-eye-disease/”} (2025). [↩]
- M. Evans, J. Sanders, T. Tagami, P. Sanders, S. Young, E. Roberts, J. Wilmot, X. Hu, K. Kabelis and J. Clark, Monoclonal autoantibodies to the TSH receptor, one with stimulating activity and one with blocking activity, obtained from the same blood sample. Clinical Endocrinology, 73 404-412 (2010). [↩]
- J. Furmaniak, J. Sanders, P. Sanders, Y. Li and B. Rees Smith, TSH receptor specific monoclonal autoantibody K1‐70TM targeting of the TSH receptor in subjects with Graves’ disease and Graves’ orbitopathy—Results from a phase I clinical trial. Clinical Endocrinology, 96 878-887 (2022). [↩]
- M. Pyzik, L. K. Kozicky, A. K. Gandhi and R. S. Blumberg, The therapeutic age of the neonatal Fc receptor. Nature Reviews Immunology, 23 415-432 (2023). [↩]
- P. Ulrichts, A. Guglietta, T. Dreier, T. van Bragt, V. Hanssens, E. Hofman, B. Vankerckhoven, P. Verheesen, N. Ongenae and V. Lykhopiy, Neonatal Fc receptor antagonist efgartigimod safely and sustainably reduces IgGs in humans. The Journal of Clinical Investigation, 128 4372-4386 (2018 [↩]
- L. Zhu, L. Li and J. Wu, FcRn inhibitors: Transformative advances and significant impacts on IgG-mediated autoimmune diseases. Autoimmunity Reviews, 103719 (2024). [↩]
- G. J. Kahaly, P. J. Dolman, J. Wolf, B. C. Giers, H. M. Elflein, A. P. Jain, A. Srinivasan, L. Hadjiiski, D. Jordan and E. A. Bradley, Proof-of-concept and randomized, placebo-controlled trials of an FcRn inhibitor, batoclimab, for thyroid eye disease. The Journal of Clinical Endocrinology & Metabolism, 108 3122-3134 (2023). [↩]
- J. V. Perez-Moreiras, J. J. Gomez-Reino, J. R. Maneiro, E. Perez-Pampin, A. R. Lopez, F. M. R. Alvarez, J. M. C. Laguarta, A. del Estad Cabello, M. G. Sorroche and E. E. Gregori, Efficacy of tocilizumab in patients with moderate-to-severe corticosteroid-resistant Graves orbitopathy: a randomized clinical trial. American Journal of Ophthalmology, 195 181-190 (2018). [↩]
- G. Boutzios, S. Chatzi, A. V. Goules, A. Mina, G. C. Charonis, P. G. Vlachoyiannopoulos and A. G. Tzioufas, Tocilizumab improves clinical outcome in patients with active corticosteroid-resistant moderate-to-severe Graves’ orbitopathy: an observational study. Frontiers in Endocrinology, 14 1186105 (2023). [↩]
- D. Ezra, A. Collins, M. Stan, Z. Haskova, T. Kuenzel, G. Spicer, M. Triyatni and O. Idowu, Interleukin-6 (IL-6) Receptor Signalling Inhibition With Satralizumab in Thyroid Eye Disease (TED): Phase 3 SatraGO-1 and SatraGO-2 Trial Design. The 42nd Annual Meeting of the European Society of Ophthalmic Plastic & Reconstructive Surgery (ESOPRS), (2024). [↩]
- D. Hutton, Targeting IL-6 inflammation: A promising frontier in treating thyroid eye disease. {HYPERLINK “https://www.ophthalmologytimes.com/view/targeting-il-6-inflammation-a-promising-frontier-in-treating-thyroid-eye-disease”} (2024). [↩]
- G. J. Kahaly, M. N. Stan, L. Frommer, P. Gergely, L. Colin, A. Amer, I. Schuhmann, P. Espie, J. S. Rush and C. Basson, A novel anti-CD40 monoclonal antibody, iscalimab, for control of Graves hyperthyroidism—a proof-of-concept trial. The Journal of Clinical Endocrinology & Metabolism, 105 696-704 (2020). [↩]
- Lundbeck initiates clinical trial in immunology for Lu AG22515 in Thyroid Eye Disease. {HYPERLINK “https://www.pharmiweb.com/press-release/2024-10-03/lundbeck-initiates-clinical-trial-in-immunology-for-lu-ag22515-in-thyroid-eye-disease”} (2024). [↩]
- A Study to Evaluate the Safety, Preliminary Efficacy, and Pharmacokinetic Properties of LASN01 in Healthy Subjects and in Patients With Pulmonary Fibrosis or Thyroid Eye Disease. {HYPERLINK “https://clinicaltrials.gov/study/NCT05331300”} (2024). [↩]
- H. B. Burch, P. Perros, T. Bednarczuk, D. S. Cooper, P. J. Dolman, A. M. Leung, I. Mombaerts, M. Salvi and M. N. Stan, Management of thyroid eye disease: a consensus statement by the American Thyroid Association and the European Thyroid Association. European thyroid journal, 11 (2022). [↩]
- L. Bartalena, G. Krassas, W. Wiersinga, C. Marcocci, M. Salvi, C. Daumerie, C. Bournaud, M. Stahl, L. Sassi and G. Veronesi, Efficacy and safety of three different cumulative doses of intravenous methylprednisolone for moderate to severe and active Graves’ orbitopathy. The Journal of Clinical Endocrinology & Metabolism, 97 4454-4463 (2012 [↩]
- G. J. Kahaly, S. Pitz, G. Hommel and M. Dittmar, Randomized, single blind trial of intravenous versus oral steroid monotherapy in Graves’ orbitopathy. The Journal of Clinical Endocrinology & Metabolism, 90 5234-5240 (2005). [↩]
- C. Marcocci, T. Watt, M. A. Altea, A. K. Rasmussen, U. Feldt-Rasmussen, J. Orgiazzi, L. Bartalena and E. G. o. G. Orbitopathy, Fatal and non-fatal adverse events of glucocorticoid therapy for Graves’ orbitopathy: a questionnaire survey among members of the European Thyroid Association. European Journal of Endocrinology, 166 247-253 (2012 [↩]
- R. Le Moli, L. Baldeschi, P. Saeed, N. Regensburg, M. P. Mourits and W. M. Wiersinga, Determinants of liver damage associated with intravenous methylprednisolone pulse therapy in Graves’ ophthalmopathy. Thyroid, 17 357-362 (2007). [↩]
- H. B. Burch, P. Perros, T. Bednarczuk, D. S. Cooper, P. J. Dolman, A. M. Leung, I. Mombaerts, M. Salvi and M. N. Stan, Management of Thyroid Eye Disease: A Consensus Statement by the American Thyroid Association and the European Thyroid Association. Thyroid, 32 {HYPERLINK “https://www.ncbi.nlm.nih.gov/pubmed/36480280”} 1439-1470 (2022). [↩]
- T. Fayers, P. M. Fayers and P. J. Dolman, Sensitivity and responsiveness of the patient-reported TED-QOL to rehabilitative surgery in thyroid eye disease. Orbit, 35 328-334 (2016 [↩]
- T. Woo, C. Li, S. Ganesananthan, R. Rajendram, J. Uddin, R. W. Lee, C. Dayan and P. Taylor, The effect of ophthalmic surgery for graves’ orbitopathy on quality of life: A systematic review and meta-analysis. Thyroid, 32 177-187 (2022). [↩]
- H. Li, Y. Wang, J. Zhou, D. You, L. Song, M. Wang, M. Zhao, C. Zhang, Y. Zhang and Y. Lin, Evaluation of fibroinflammatory activity in thyroid eye disease using [18F] AlF-NOTA-FAPI-04 PET/CT: A prospective study. European Journal of Nuclear Medicine and Molecular Imaging, 52 1890-1900 (2025). [↩]
- J. Lee, J. Byun, G. Shim and Y.-K. Oh, Fibroblast activation protein activated antifibrotic peptide delivery attenuates fibrosis in mouse models of liver fibrosis. Nature communications, 13 1516 (2022 [↩]
- H. Aghajanian, T. Kimura, J. G. Rurik, A. S. Hancock, M. S. Leibowitz, L. Li, J. Scholler, J. Monslow, A. Lo and W. Han, Targeting cardiac fibrosis with engineered T cells. Nature, 573 430-433 (2019). [↩]
- D. Strianese and F. Rossi, Interruption of autoimmunity for thyroid eye disease: B-cell and T-cell strategy. Eye, 33 191-199 (2019). [↩]
- P. Bhargava and P. Calabresi, Novel therapies for memory cells in autoimmune diseases. Clinical & Experimental Immunology, 180 353-360 (2015). [↩]
- H. Chen, T. Mester, N. Raychaudhuri, C. Y. Kauh, S. Gupta, T. J. Smith and R. S. Douglas, Teprotumumab, an IGF-1R blocking monoclonal antibody inhibits TSH and IGF-1 action in fibrocytes. The Journal of Clinical Endocrinology & Metabolism, 99 E1635-E1640 (2014). [↩]
- C. Dosiou and A. L. Kossler, Thyroid eye disease: navigating the new treatment landscape. Journal of the Endocrine Society, 5 bvab034 (2021). [↩]
- P. Perros and L. Hegedüs, Teprotumumab in thyroid eye disease: wonder drug or great divider? European Thyroid Journal, 12 (2023). [↩]
- G. J. Kahaly, C. Wüster, P. D. Olivo and T. Diana, High titers of thyrotropin receptor antibodies are associated with orbitopathy in patients with Graves disease. The Journal of Clinical Endocrinology & Metabolism, 104 2561-2568 (2019 [↩]
- F. Nicolì, G. Lanzolla, M. Mantuano, I. Ionni, B. Mazzi, M. Leo, A. Sframeli, C. Posarelli, M. Maglionico and M. Figus, Correlation between serum anti-TSH receptor autoantibodies (TRAbs) and the clinical feature of Graves’ orbitopathy. Journal of Endocrinological Investigation, 44 581-585 (2021). [↩]
- K. Ponto, T. Diana, H. Binder, N. Matheis, S. Pitz, N. Pfeiffer and G. Kahaly, Thyroid-stimulating immunoglobulins indicate the onset of dysthyroid optic neuropathy. Journal of endocrinological investigation, 38 769-777 (2015). [↩]
- I. Molnár and C. Balazs, High circulating IL-6 level in Graves’ ophthalmopathy. Autoimmunity, 25 91-96 (1997 [↩]
- E. Kishazi, M. Dor, S. Eperon, A. Oberic, N. Turck and M. Hamedani, Differential profiling of lacrimal cytokines in patients suffering from thyroid-associated orbitopathy. Scientific reports, 8 10792 (2018 [↩]
- D. Huang, N. Xu, Y. Song, P. Wang and H. Yang, Inflammatory cytokine profiles in the tears of thyroid-associated ophthalmopathy. Graefe’s Archive for Clinical and Experimental Ophthalmology, 250 619-625 (2012). [↩]



{kind=link}