
Abstract
Background/Objective: Dementia affects more than 55 million people worldwide, creating challenges for individuals and caregivers. While biological factors are well documented, the role of meaningful relationships characterized by emotional intimacy, trust, and shared experiences in dementia progression is less explored. This systematic review applies a social-ecological framework to examine how family dynamics, spousal support, caregiving experiences, and broader social connections shape cognitive health and dementia outcomes.
Methods: Studies published from 2003 to 2023 were reviewed using PubMed, PsycINFO, Scopus, and Google Scholar. Inclusion criteria focused on studies examining social, familial, or caregiving factors linked to cognitive health, excluding those focused solely on medical treatments. Thematic analysis grouped findings into family relationships, spousal dynamics, caregiving roles, and community engagement. Quality was assessed with the Mixed Methods Appraisal Tool.
Results: Meaningful relationships were linked to better cognitive resilience, while social isolation was tied to faster cognitive decline. Although caregiving could support mental health, it also increased strain that may negatively affect caregivers and people with dementia. Community engagement and friendships were protective factors, and digital tools like video calling helped reduce isolation.
Conclusions: Strengthening social relationships, supporting caregivers, and promoting social involvement are important for improving cognitive outcomes in dementia. Including social support assessments and interventions, such as caregiver training, peer groups, and technology-based engagement, may help reduce stress and slow decline. Future studies should explore culturally sensitive strategies to improve social support and reduce isolation.
Keywords: Dementia, meaningful relationships, caregiving, social isolation, cognitive health, community engagement
Introduction
Background and Context
Dementia is strongly linked to accelerated cognitive impairment and disability in older adults, affecting 55 million people globally and placing substantial emotional and financial strains on families and caregivers1’2. As the global population ages, it has become increasingly urgent to identify the factors that influence dementia progression3’4. While biological factors such as genetics and brain pathology are well established, a growing body of research has drawn attention to the role of social relationships and support systems in moderating cognitive decline5’6. In particular, meaningful relationships defined by emotional closeness, trust, and shared experiences may influence the course of cognitive health overtime5’7. Emerging evidence also suggests that digital tools, including video calls and online support groups, can play a role in reducing social isolation and maintaining meaningful connections for people with dementia8’9. While these tools do not fully replace in-person interaction, they may offer important supplementary support, particularly for those with mobility limitations or during times of restricted social contact10.
This systematic review adapts Bronfenbrenner’s Ecological Systems Theory11, which describes individuals as being shaped by multiple layers of environmental influence, including family, community, and broader social systems. In the context, this model helps explain how relational experiences affect health trajectories. By integrating this theory with concepts from psychological well-being and social determinants of health12’13, I provide a comprehensive framework for understanding dementia progression.
Problem Statement and Rationale
Although social determinants of health are increasingly recognized in dementia research, most studies focus on whether individuals are socially connected rather than how emotionally meaningful those connections are. There remains limited insight into how intimacy, trust, and shared experiences affect cognitive decline. This gap makes it difficult to design targeted interventions to slow dementia progression by improving relationship quality. Most existing literature treats social contact as a binary factor (present vs.absent), whereas this review uniquely emphasized the quality of relationships, the emotional intimacy and meaningful engagement, as a key determinant of cognitive outcomes. Addressing this gap could help identify psychosocial targets for interventions to promote cognitive resilience.
Significance and Objectives
This systematic review investigates the impact of emotionally meaningful relationships on dementia progression using the Ecological Systems Model of Dementia Progression (Figure 1). It examines how family dynamics, emotional closeness, spousal support, caregiving strain, and community engagement relate to cognitive health. It also explores how parental status and non-familial networks influence risk, particularly in individuals without children. The goal is to clarify how different types of relationships promote or hinder cognitive resilience , with specific focus on memory retention, rate of cognitive decline, and emotional well-being as key outcomes. By identifying which social factors are most protective or detrimental, this systematic research aims to pinpoint where social interventions may be most beneficial in the dementia care trajectory.
Scope and Limitations
This systematic review includes peer-reviewed studies published in English between 2003 and 2023 that investigate the association between social, familial, or caregiver factors and cognitive health or dementia outcomes. Studies were included if they used quantitative, qualitative, or mixed method approaches and focused on individuals diagnosed with dementia or those at risk. Studies focusing solely on pharmacological or medical treatments (with no social or relational variables) and non-peer-reviewed sources (conference abstracts, theses, grey literature) were excluded. The review emphasizes relational and psychosocial variables, excluding studies centered only on biomedical interventions.
Limitations of this review include reliance on self-reported data in many studies (which may introduce bias), exclusion of non-English publications (which could limit generalizability), and variation in how “meaningful” relationships were defined and measured across studies. These differences in definitions and measures may affect the comparability of findings. The scope is further constrained by available literature up to 2023 and the decision to focus on social factors, meaning other domains (like purely biological mechanisms) are beyond the present analysis.
Theoretical Framework
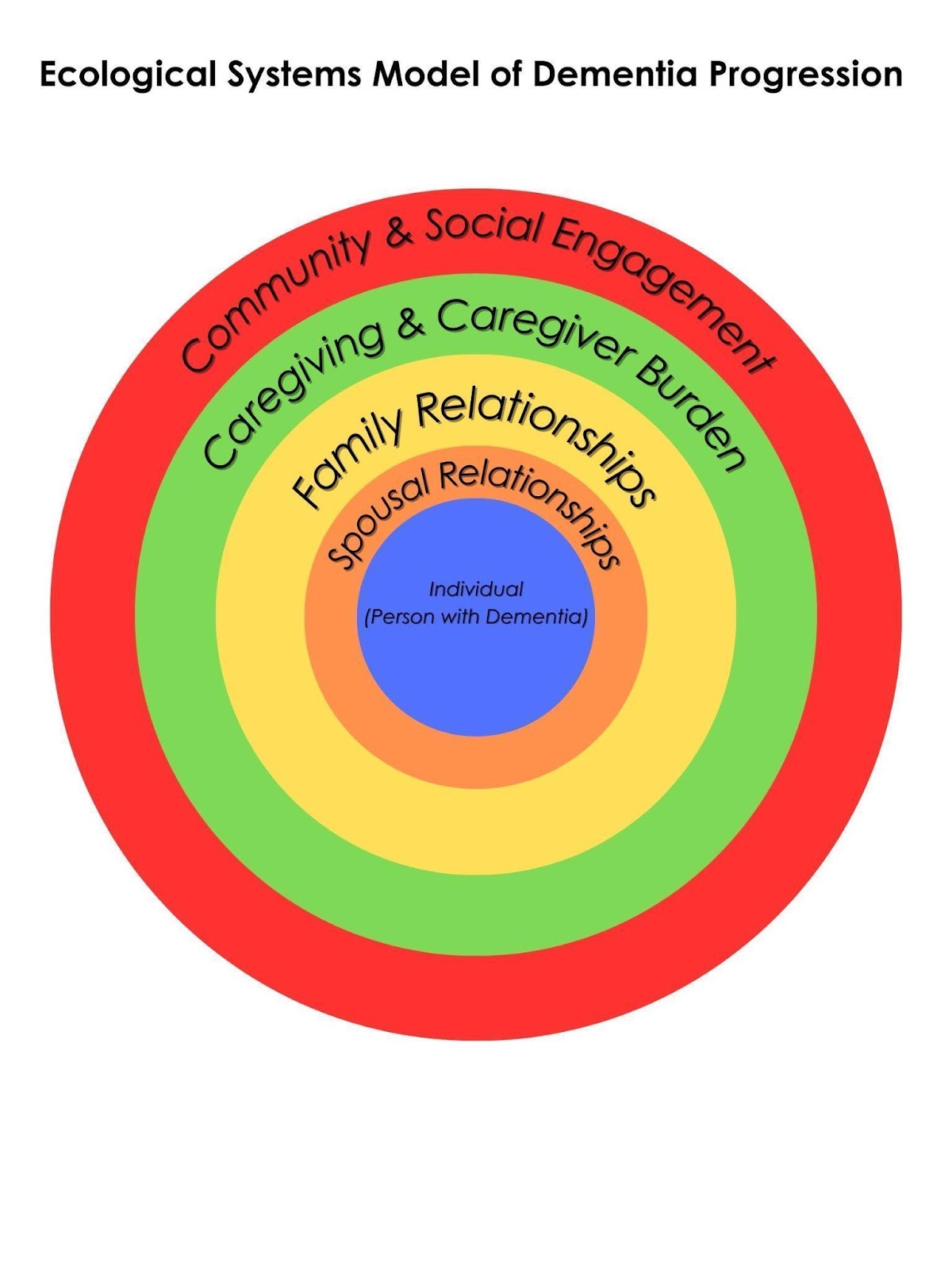
The Ecological Systems Model of Dementia Progression (Figure 1) provides the theoretical foundation for this review. Adapted from Bronfenbrenner’s ecological systems theory11, it describes how individuals are shaped by overlapping layers of social influence, including spousal relationships, family networks, caregiving systems, and community engagement. These layers interact to shape cognitive resilience, vulnerability, and overall well-being14. By integrating psychological well-being and social determinants of health15’16, the model supports a comprehensive understanding of how relationship quality contributes to dementia risk and progression. This framework also guides the structure of the Result section, where findings are organized according to these four layers of influence. Figure 1 (above) illustrates the model: the person with dementia is at the center, surrounded by successive social layers (spouse, family, caregivers, community) that collectively influence the disease course. Notably, these layers are interrelated rather than independent; interactions between the immediate and broader social environment can amplify or slow down the impacts on the individual at different stages of dementia progression.
Figure 1. Adapted Ecological Model of Dementia Progression. This model, which is called the Ecological Systems Model of Dementia Progression, illustrates how different layers of social relationships influence cognitive resilience and dementia progression. At the core is the individual with dementia, whose cognitive health is shaped by interactions with various social systems17. The first layer, spousal relationships, represents the most immediate social bond, providing emotional intimacy and cognitive engagement but also presenting challenges related to caregiving stress18’19. Surrounding this is the family network, which plays a crucial role in offering emotional and practical support, though its impact varies depending on family structure and involvement14. Beyond the family, the caregiving and caregiver burden layer includes both formal and informal caregiving networks. While caregiving can enhance well-being, excessive caregiver burden can introduce chronic stress that negatively affects both the caregiver and the individual with dementia18’19. The outermost layer, community and social engagement, encompasses broader social interactions such as friendships, community groups, faith-based organizations, volunteer work, and digital communication platforms that help mitigate isolation and enhance cognitive stimulation20’21. Each layer dynamically interacts with the others, emphasizing the importance of strong social connections in maintaining cognitive health. This model highlights the need for holistic dementia care strategies that extend beyond medical treatment to integrate social support22’23’21.
Methodology
Search Strategy
A systematic literature search was conducted to identify peer-reviewed studies examining the relationship between meaningful social relationships and dementia progression. Searches were performed using four databases: PubMed, PsycINFO, Scopus, and Google Scholar. Keywords used included: “dementia,” “cognitive decline,” “family relationships,” “spousal support,” “caregiving burden,” “social isolation,” and “community engagement.” Filters were applied to include only articles published in English between January 2003 and December 2023. One Spanish-language article was reviewed at the abstract level for background context but was not included in the synthesis or quality assessment due to lack of full-text access. All included studies were published in English. Reference lists of relevant studies were also reviewed to identify additional sources.
Inclusion and Exclusion Criteria
Studies were included if they examined the impact of social, familial, or caregiving relationships on cognitive health or dementia outcomes. Eligible studies used quantitative, qualitative, or mixed-method designs and included participants diagnosed with dementia or those identified as at risk of cognitive impairment. Studies focusing solely on pharmacological or medical treatments without addressing social or relational factors were excluded, as were non-peer-reviewed materials such as conference abstracts, theses, or grey literature.
Screening Process and Study Selection
Titles and abstracts of approximately 120 records were screened for relevance to the research question and adherence to inclusion criteria. Studies meeting initial criteria were then reviewed in full text to confirm eligibility. This process resulted in 41 studies that were included in the final synthesis. All included studies were published in English and provided sufficient detail for thematic analysis.
Data Extraction
Data extraction was performed manually by the author, using a consistent set of key data points for each included study. Although no formal extraction table or software was used, the same information was recorded across all studies to ensure consistency. Extracted data included authorship, publication year, study design, sample characteristics, relationship type, and main findings, as well as any noted definitions of relationship quality and study limitations. Because extraction was done by a single reviewer, no inter-rater reliability checks were needed. The extracted details were used to organize studies into thematic categories for the narrative synthesis.
Synthesis Method
A narrative thematic analysis was used to identify key patterns across the studies. Findings were grouped into four major themes aligned with the Ecological Systems Model (Figure 1): spousal relationships, family dynamics, caregiving experiences, and community or social connections. Results within each theme were further organized based on their impact on cognitive health, dementia risk, and disease progression. Contradictory or inconsistent findings were noted and interpreted in relation to differences in study context or methodology. This narrative synthesis provided a structured yet flexible understanding of the relationships and their implications, allowing integration of quantitative and qualitative evidence.
Quality Assessment
Methodological quality was assessed using the Mixed Methods Appraisal Tool (MMAT)20. Studies were evaluated across five domains: clarity of research questions, appropriateness of study design, data collection methods, rigor of analysis, and alignment of conclusions with findings. Studies with limitations (e.g., small sample sizes, reliance on self-reported data, or insufficient reflexivity in qualitative designs) were interpreted cautiously during synthesis. A systematic search and screening process was followed. After excluding one Spanish-language study due to incomplete translation of key sections, 34 studies were included for analysis. These 34 studies are cited throughout the paper, alongside additional references (e.g., theoretical frameworks, epidemiological data), totaling 41 sources in the reference list.
Ethical Considerations
This systematic review analyzed existing published studies and did not involve direct interaction with human participants or collection of new data. All studies included in this review reported obtaining ethical approval from relevant institutional review boards, as stated in their original publications
Results
The Ecological Systems Model of Dementia Progression (Figure 1) and the concept of social determinants of health together offer a comprehensive framework to analyze how social factors influence cognitive health and dementia risk in older adults24’25’26. Findings from the included studies are organized into four thematic layers based on this model: (1) Spousal Relationships, (2) Family Relationships, (3) Caregiving and Caregiver Burden, and (4) Community and Social Engagement. The structure of the results emphasizes the importance of meaningful engagement, emotional depth, and social context in shaping cognitive outcomes. It is important to note that while these layers are presented separately, they often interact dynamically. For example, a supportive spouse can facilitate broader family involvement, and strong community ties may alleviate some caregiver burden, illustrating that social layers can influence each other and dementia progression in a bidirectional manner. Below, I synthesize specific results for each social ecological layer, linking relationship factors to cognitive or emotional outcomes in dementia.
Spousal Relationships and Cognitive Health
Spousal relationships represent the most immediate and emotionally significant layer of social influence in the Ecological Systems Model11. This section focuses on how the presence and quality of a spouse or long-term partner affects the cognitive functioning, emotional well-being, and dementia-related outcomes of individuals with dementia.
Several studies emphasize the protective role of spousal support in slowing cognitive decline27’19. Spouses often provide sustained emotional intimacy and cognitive stimulation, both of which are associated with increased resilience to dementia symptoms27’25. For example, individuals with dementia who reported high emotional closeness to their partners demonstrated better memory retention and executive functioning compared to those in more strained relationships25. Spouses were also found to buffer against feelings of social isolation, which has been strongly linked to accelerated cognitive decline28. In other words, a supportive marital relationship can enrich daily cognitive engagement and reduce loneliness, thereby potentially slowing the progression of dementia28’19.
However, spousal relationships also carry complexities, particularly around the caregiving role. Caregiving by a spouse is linked to elevated emotional and physical stress29. Spousal caregivers often report high levels of strain, especially in the mid to late stages of dementia progression30’29. This chronic stress can compromise their ability to provide consistent emotional support and, in some cases, contributes to poorer outcomes for both the caregiver and the patient18’30. Some studies noted that spousal caregivers experience elevated rates of depression and emotional burnout18, potentially leading to a breakdown in relational quality over time. As the disease advances, the spouse may struggle to cope, which can introduce tension or reduce the effectiveness of support despite the couple’s emotional bond30.
These findings demonstrate a dual dynamic in spousal relationships. While emotional closeness and a shared history can serve as cognitive protectors for the person with dementia25’19, the burden of caregiving may erode those very supports over time30’29. The variability in outcomes linked to spousal relationships highlights the importance of evaluating not just the presence of a partner, but the quality and sustainability of that relationship in the context of dementia care. Interventions that help spousal caregivers manage stress (e.g., respite care, counseling, support groups31 could preserve the positive aspects of the marital bond for longer, thereby benefiting cognitive health in the patient. In summary, high-quality spousal relationships appear to promote cognitive resilience32, whereas strained or unsupported spousal caregiving situations can accelerate cognitive and emotional decline18’29.
Family Relationships and Cognitive Health
Family relationships represent the second layer of social influence in the Ecological Systems Model of Dementia Progression. This category includes relationships with adult children, siblings, and extended family members who may provide emotional support, companionship, and informal caregiving. The availability and quality of these broader family ties can meaningfully shape cognitive and psychological outcomes in individuals with dementia14’21.
Several studies show that close involvement from adult children or other family members is associated with improved emotional well-being and slower cognitive decline for the person with dementia27’33. Frequent contact, regular conversations, and emotional closeness with family have been linked to better memory retention and fewer behavioral symptoms in dementia patients13. In some cases, multi-generational involvemeem, such as interaction with both children and grandchildren, appears to enhance emotional resilience in older adults living with cognitive impairment14. Family members can provide reinforcement of orientation (e.g., reminding about time, place, life events) and a sense of continuity and identity for the individual with dementia, which can translate into more stable cognitive functioning day to day13’14.
However, not all family dynamics are protective. Tension, unresolved conflict, emotional distance, or unequal caregiving responsibilities within a family can increase stress for both the person with dementia and their relatives11’34. For instance, one family member carrying most of the caregiving load may experience burnout18’29, while other relatives remain less involved, leading to resentment or guilt that the person with dementia can often sense34. Some studies note that family caregivers may lack dementia-specific knowledge, resulting in inconsistent or even ineffective support strategies at home35. Geographic distance or emotional disengagement among family members can also be associated with greater social isolation for the person with dementia and has been linked to poorer cognitive outcomes36’28. In such cases, even if family members exist, their limited or strained involvement provides little benefit and can sometimes heighten anxiety or confusion for the patient36’28 (for example, sporadic contact might be disorienting or upsetting).
Ultimately, the quality of these familial relationships rather than their mere presence determines whether they serve as protective or harmful influences in dementia27’14. Emotionally meaningful engagement, open communication, and consistent involvement by family appear to be critical in preserving cognitive functioning and delaying progression of dementia-related symptoms13’33. By contrast, families characterized by conflict, lack of support, or absence of communication may inadvertently contribute to faster decline or psychological distress11’34. These results reinforce that it is not enough for individuals with dementia to have family around; what matters most is that family interactions are positive, supportive, and regular13’14. Interventions like family counseling or education programs could help improve family dynamics (for instance, by aligning caregiving expectations and teaching effective communication techniques), thereby maximizing the cognitive and emotional benefits of family involvement27’31.
Caregiving and Caregiver Burden
The third layer of the Ecological Systems Model of Dementia Progression includes both formal and informal caregiving systems. This layer highlights the complex role that caregiving plays in shaping cognitive outcomes for individuals with dementia, particularly when the caregiver is a close family member or spouse19’29. While caregiving can provide emotional support and stability for the person with dementia19, it can also introduce chronic stress, burnout, and emotional strain for both the caregiver and the care recipient if the burden becomes overwhelming18’29.
Multiple studies underscore the dual nature of caregiving in the context of dementia. On one hand, sustained caregiver involvement is associated with greater emotional security for the person with dementia, improved daily routines, and more opportunities for cognitive stimulation25’19. Informal caregivers who are deeply involved (especially those co-residing or present daily) often provide consistent interaction and personalized care that can help reduce anxiety and behavioral disturbances in individuals with dementia25’19. These close caregiving relationships frequently serve as a daily buffer against the psychological effects of cognitive loss25. For example, a dedicated caregiver might regularly engage the person in conversation, orientation exercises, or memory games, which can slow cognitive deterioration and provide comfort.
On the other hand, caregiver burden can significantly impair these benefits. High levels of stress, emotional fatigue, and physical exhaustion are frequently reported among family caregivers, particularly as dementia symptoms worsen or care demands increase over time30’29. Prolonged caregiver strain has been linked to negative outcomes, including lower quality of care, greater emotional detachment on the part of the caregiver, and an increased risk of institutionalization (nursing home placement) for the patient18’30. In some cases, studies found that markers of caregiver distress (such as depressive symptoms or chronic anxiety in the caregiver) correlate with faster cognitive deterioration in the person receiving care30’29. This may be because a stressed or depressed caregiver is less able to provide stimulating and attentive care18, or because the emotional climate in the caregiving relationship becomes tense, which can adversely affect the patient’s cognitive and emotional state30.
These findings underscore that caregiving, while often grounded in strong relational bonds19, can become a risk factor if adequate support is not in place30’29. The balance between supportive care and caregiver strain is a critical mediator of cognitive and emotional outcomes in dementia progression29. When caregivers receive external support (respite services, support groups, training, etc.31 and practice self-care, they are better able to maintain a positive and stimulating environment for the person with dementia19’31. Conversely, unsupported caregivers may inadvertently contribute to a more rapid decline due to stress and burnout18’29. In practical terms, this suggests that healthcare providers and policy makers should monitor caregiver well-being as part of dementia care. Interventions like respite care, caregiver skill-building workshops, and counseling for caregiver stress could indirectly benefit patients by sustaining the caregivers’ ability to provide high-quality, engaging care31.
Community and Social Engagement
Community and social engagement form the outermost layer of the Ecological Systems Model. This layer includes social connections beyond the immediate family or caregiving context, such as friendships, participation in community groups, faith-based organizations, volunteer work, and online or digital communication platforms23’37. These broader social networks play an important role in reducing isolation and maintaining cognitive stimulation for individuals with dementia or those at risk of dementia.
Studies show that sustained engagement in community activities is associated with delayed cognitive decline and better psychological well-being in older adults38’37. Regular participation in social activities, such as group discussions, clubs, religious gatherings, cultural events, or volunteering provides cognitive stimulation and emotional fulfillment for seniors, including those with mild dementia38’37. These activities often involve conversation, problem-solving, or physical movement, all of which can help exercise the brain32’37. For example, attending a weekly book club or community center class can offer structured mental engagement and a sense of purpose, which may translate into slower memory loss or improved mood. Importantly, community programs can also give caregivers a break while providing the person with dementia an opportunity for social interaction37.
Digital platforms and virtual interactions have also been shown to reduce isolation and help maintain continuity in social connection, especially during periods of physical limitation or when in-person engagement is not possible39’40 (such as during a pandemic or for homebound individuals). While online socialization (video chats, social networks for seniors, etc.) may not fully replicate the cognitive and emotional benefits of in-person connections, they can nevertheless provide meaningful interaction that prevents complete social withdrawal41. Some reviewed articles noted that technology-based social contact (like regular video calls with friends/family or participating in virtual support groups) can improve mood and reduce feelings of loneliness in persons with dementia, which might indirectly support cognitive functioning by reducing depression and stress39’40.
Notably, the benefits of community engagement extend even to individuals who lack traditional family support23’42. Several studies suggest that robust community networks can compensate for limited familial involvement23’37. For older adults without children or close family38’37, friendships and community ties have been found to serve as strong predictors of emotional well-being and cognitive stability. In other words, a person with dementia who is embedded in a supportive community (neighbors, church members, peers at a senior center) may experience similar protective effects as someone with a supportive family23’42. These community relationships can provide emotional affirmation, oversight (people checking in on them), and cognitive stimulation through shared activities.
However, the protective effects of community and social relationships depend on their frequency, emotional depth, and perceived meaningfulness35’41. Simply being a member of a community group is not enough if the individual does not feel truly connected or if interactions remain superficial41. Meaningful engagement where the person feels valued, heard, and emotionally supported appears necessary to reap cognitive benefits35’41. Furthermore, overstimulation or stressful social encounters (for instance, large noisy gatherings that cause anxiety) would not be beneficial. Thus, the quality of community engagement matters just as much as participation itself41.
In sum, community and social engagement provide a critical outer layer of protection in dementia progression23’37. While not a substitute for close family or spousal ties, meaningful connections in broader social environments offer a valuable source of emotional support, cognitive enrichment, and a sense of inclusion. These findings reinforce the idea that “it takes a village” to support cognitive health, communities can play a key role in enriching the lives of people with dementia and potentially slowing their decline. Programs that facilitate social participation (community memory cafés, adapted recreational activities, senior volunteer opportunities, etc.) or technologies that connect isolated seniors should be considered integral to comprehensive dementia care strategies40’23.
Discussion
This review highlights how different types of meaningful relationships influence dementia progression, emphasizing that it is the quality of those relationships, the emotional support, psychological security, and consistent engagement they provide, that matters most. By organizing findings through the lens of an Ecological Systems Model11, I integrate diverse social layers to explain how relationships impact cognitive outcomes at various points in the disease trajectory. The evidence confirms and extends previous work on the social determinants of health11’43 by focusing not only on the presence of social ties but also on their depth and meaningfulness. While prior research often treats social contact as a binary variable, for example, living alone versus not, present versus absent support, this review synthesizes findings showing that emotionally meaningful engagement is more predictive of cognitive resilience than frequency of interaction alone. For instance, emotionally secure spousal bonds, engaged and supportive adult children, and high-quality caregiver support were consistently associated with slower cognitive decline, whereas relational strain, family detachment, or high caregiver burden were linked to faster deterioration in cognitive abilities.
These findings have practical implications for dementia care and public health. Regular social support assessments could be incorporated into dementia screening and care planning to identify patients who are at higher risk of social isolation or relationship-related stress. Clinicians might use simple questionnaires to gauge the patient’s satisfaction with their social interactions and the caregiver’s level of strain. Patients identified as socially isolated or caregivers identified as overwhelmed could be flagged for additional support services. Policymakers and care organizations should consider models of care that include structured relational interventions, such as family therapy or counseling to improve communication, community-building programs that connect patients with peers or volunteers, and respite care access for overwhelmed caregivers. Importantly, this review suggests that interventions need to target relationship quality. For example, simply increasing the number of social visits may not help if those interactions lack emotional connection. Programs that facilitate meaningful engagement like reminiscence therapy groups, intergenerational activity programs, or dementia-friendly community events could provide both cognitive stimulation and emotional comfort44.
The dual role of caregiving protection through emotional engagement yet potentially harmful due to chronic stress is supported by evidence showing that sustained caregiver involvement improves patient stability19, while prolonged strain accelerates cognitive decline30’29. The effect of caregiving on dementia outcomes appears to shift based on factors like the caregiver’s coping capacity, access to external support, the quality of the pre-existing relationship, and the stage or severity of the patient’s symptoms. Caregivers with strong coping skills, social support of their own, and regular respite opportunities tend to maintain supportive relationships with the person with dementia. In contrast, those under prolonged, unsupported stress may experience burnout that undermines the well-being of both parties18. This indicates that caregiver interventions (training, support groups, stress management resources) are not just about caregiver health, they are integral to patient health as well.
The rise of digital communication in recent years presents a complex but promising picture. Digital tools like video calls mitigate isolation and maintain social engagement, particularly for homebound individuals40, though they cannot fully substitute in-person interactions40’45. For individuals with mobility limitations or whose families are geographically dispersed, technology can reduce isolation and keep them engaged with loved ones. Future studies should explore in greater depth whether different forms of digital engagement can foster the same emotional depth as face-to-face interactions, or if they primarily provide superficial social maintenance. Operationalizing “meaningfulness” in virtual versus physical interactions will be essential as our society increasingly turns to digital solutions for connecting with homebound elders.
Cultural and regional norms also emerged as an important contextual factor shaping social relationships in dementia. For example, studies suggest that in collectivist cultures, extended families frequently co-reside or share caregiving responsibilities46’14, reducing individual burden and fostering emotional continuity for individuals with dementia. In contrast, individualistic societies often place primary caregiving duties on spouses47’19, increasing stress and necessitating external support systems. Comparative studies and a few included in this review suggest that differences in family structure, expectations of filial piety, and community cohesion can influence outcomes. This underscores that recommendations may need tailoring: what works in one cultural context like relying on family caregivers may not in another, and vice versa. Dementia care strategies should be culturally sensitive, leveraging existing social strengths, for instance, faith communities in some cultures, and addressing specific gaps such as lack of extended family nearby in others.
Mechanisms behind social isolation’s impact on dementia deserve special attention. The evidence implies two primary pathways: cognitive stimulation and stress modulation. A lack of social interaction reduces opportunities to engage memory, language, and other cognitive faculties, reflecting the principle of cognitive reserve, where sustained mental and social activity helps delay neurodegeneration32. Socially isolated individuals miss out on conversations, shared activities, and environmental cues that can help reinforce cognition. Concurrently, isolation often may contribute to loneliness, depression, and chronic stress (elevated cortisol levels, etc.), which are known to have neurotoxic effects and exacerbate cognitive decline48. In my synthesis, I explicitly noted that social isolation likely accelerates decline by reducing cognitive stimulation and increasing chronic stress. This suggests that interventions to reduce isolation (e.g., senior center programs, befriending services, community transportation for those who cannot drive) could have a real biological impact by preventing stress-related neurodegeneration and by keeping the mind active.
Finally, the synthesis using the Ecological Systems Model provides a holistic understanding: it shows that interventions and policy changes are needed at multiple levels. At the microsystem level, we must support couples and families in maintaining positive relationships (through counseling, education, respite). At the mesosystem level (community), we should expand community-based programs and dementia-friendly social environments. At the exosystem and macrosystem levels, policies should mandate caregiver support, promote social inclusion in healthcare planning, and possibly incentivize community organizations to include seniors with cognitive impairment. Viewing dementia through a social-ecological lens reinforces that treatment is not just about managing plaques and tangles in the brain; it’s also about enriching the social world around the person.
In summary, meaningful social relationships act as a form of cognitive reserve32 or resilience in the face of neurodegeneration. High-quality emotional connections, whether with a spouse, family member, friend, or community appear to bolster the mind against decline, whereas social disconnection and poor relationship quality can remove that safety net and hasten cognitive impairment. Dementia care should therefore extend beyond pharmacological treatments and cognitive training to actively foster and maintain the social and relational health of patients and their caregivers.
Conclusion
Relational factors should be considered alongside clinical measures in dementia care. This review’s findings suggest that regular assessments of a patient’s social support network and relationship quality could help identify individuals at greater risk of rapid decline. For example, simple screening questions about loneliness or satisfaction with support could become part of routine dementia evaluations. When social risk factors are identified, structured interventions such as caregiver training programs, emotional support groups for families, or community engagement programs may offer important emotional buffering and cognitive stimulation that help slow the disease progression. The evidence presented here indicates that strengthening meaningful relationships, ensuring they are positive and supportive, and alleviating relationship-related stress are viable targets for improving dementia outcomes.
Future research should examine how digital communication tools, cultural expectations, and even biological pathways interact with social relationships in dementia. Investigating the effectiveness of virtual relationships compared to in-person engagement will clarify whether different forms of connection provide comparable benefits to patients. Additionally, more longitudinal studies across diverse populations are needed to confirm causal links between relationship quality and dementia progression, and to guide inclusive care models that can work in various cultural settings. Further studies could explore whether strengthening relational bonds via programs like buddy systems is linked to better cognitive outcomes or delayed transitions to nursing homes.
By centering the emotional and relational context of individuals with dementia, this review reinforces the importance of holistic care strategies. Effective dementia care must extend beyond medical treatment to address the broader social environment of the patient. Policies and care guidelines should treat social health as a vital sign, something to be monitored and nurtured. In practice, this could mean healthcare teams including social workers or community navigators who connect families to resources, or memory clinics running caregiver workshops and patient social activities as part of their services. It also means advocating at the policy level for caregiver respite funding, dementia-friendly community initiatives, and perhaps even public awareness campaigns about staying connected with those who have dementia.
In conclusion, meaningful relationships act as both a buffer and a bridge buffering individuals with dementia against the worst effects of cognitive decline, and bridging them to resources and experiences that enhance quality of life. Strengthening these relationships and mitigating social risks is not only beneficial for patients and caregivers on a personal level, but also has broader implications for public health (potentially reducing healthcare utilization by delaying severe decline or institutionalization). Dementia is not only a neurological condition but also a social one. Addressing it requires enriching the social ecology around the patient. By doing so, we can improve outcomes and uphold the dignity and well-being of those living with dementia.
Acknowledgement
I sincerely thank my mentor, Dr. Mandy Rounds, for her invaluable guidance and support throughout this research. Her expertise and encouragement were crucial to its completion.
References
- Garre-Olmo, J., Epidemiology of Alzheimer’s disease and other dementias. Rev. Neurol. 66, 377–386 (2018). [↩]
- Ferri, C. P. et al., Global prevalence of dementia: a Delphi consensus study. Lancet Lond. Engl. 366, 2112–2117 (2005). [↩]
- Kuwayama, S., Tarraf, W., González, K. A., Márquez, F. & González, H. M., Life-Course Multidisciplinary Psychosocial Predictors of Dementia Among Older Adults: Results from the Health and Retirement Study. Innov. Aging igae092 (2024). [↩]
- Longevity, T. L. H., Mental health deserves attention at all ages. Lancet Healthy Longev. 5, (2024). [↩]
- A. Ablitt and others, Living with dementia: A systematic review of the influence of relationship factors. Aging Ment. Health, 13, 497–511 (2009). [↩] [↩]
- H. B. Edwards and others, Quality of family relationships and outcomes of dementia: a systematic review. BMJ Open, 8, e015538 (2018). [↩]
- J. La Fontaine & J. R. Oyebode, Family relationships and dementia: a synthesis of qualitative research including the person with dementia. Ageing Soc., 34, 1243–1272 (2014). [↩]
- S. R. Cotten and others, Impact of internet use on loneliness and contact with others among older adults: cross-sectional analysis. J. Med. Internet Res., 15, e39 (2013). [↩]
- L. Nguyen and others, EXPLORING VIDEO CHAT FOR SOCIAL ENGAGEMENT IN OLDER ADULTS WITH AND WITHOUT COGNITIVE IMPAIRMENT. in vol. 3, S932–S932 (2019). [↩]
- W. J. Chopik, The Benefits of Social Technology Use Among Older Adults Are Mediated by Reduced Loneliness. Cyberpsychology Behav. Soc. Netw., 19, 551–556 (2016). [↩]
- PDF, Bronfenbrenner’s Ecological Systems Theory. ResearchGate (2024). [↩] [↩] [↩] [↩] [↩] [↩] [↩]
- Alegría, M., NeMoyer, A., Falgas, I., Wang, Y. & Alvarez, K., Social Determinants of Mental Health: Where We Are and Where We Need to Go. Curr. Psychiatry Rep. 20, 95 (2018). [↩]
- Hendrie, K., Tampi, R., Jeste, D. & Joshi, P., Social Determinants of Health in Dementia. Am. J. Geriatr. Psychiatry 32, S7 (2024). [↩] [↩] [↩] [↩] [↩]
- La Fontaine, J. & Oyebode, J. R., Family relationships and dementia: a synthesis of qualitative research including the person with dementia. Ageing Soc. 34, 1243–1272 (2014). [↩] [↩] [↩] [↩] [↩] [↩] [↩] [↩]
- Alegría, M., NeMoyer, A., Falgas, I., Wang, Y. & Alvarez, K., Social determinants of mental health: where we are and where we need to go. Curr. Psychiatry Rep. 20, 95 (2018). [↩]
- Hendrie, K., Tampi, R., Jeste, D. & Joshi, P., Social determinants of health in dementia. Am. J. Geriatr. Psychiatry 32, S7 (2024). [↩]
- Ablitt, A., Jones, G. V. & Muers, J., Living with dementia: A systematic review of the influence of relationship factors. Aging Ment. Health 13, 497–511 (2009). [↩]
- Alves, L. C. de S. et al., Burnout syndrome in informal caregivers of older adults with dementia: A systematic review. Dement. Neuropsychol. 13, 415–421 (2019). [↩] [↩] [↩] [↩] [↩] [↩] [↩] [↩] [↩] [↩] [↩]
- Schulz, R., Beach, S. R., Czaja, S. J., Martire, L. M. & Monin, J. K., Family Caregiving for Older Adults. Annu. Rev. Psychol. 71, 635–659 (2020). [↩] [↩] [↩] [↩] [↩] [↩] [↩] [↩] [↩] [↩] [↩] [↩] [↩]
- Hong, Q. N. et al., The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Educ. Inf. 34, 285–291 (2018). [↩] [↩]
- Podgorski, C. A., Anderson, S. D. & Parmar, J., A Biopsychosocial-Ecological Framework for Family-Framed Dementia Care. Front. Psychiatry 12, (2021). [↩] [↩] [↩]
- Fingerman, K. L., Huo, M., Ng, Y. T. & Zarit, S. H., Social Relationships and Cognitive Development in Adulthood. in The Cambridge Handbook of Cognitive Aging: A Life Course Perspective (eds. Gutchess, A. & Thomas, A. K.) 350–366 (Cambridge University Press, Cambridge, 2020. [↩]
- Livingston, G. et al., Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. The Lancet 396, 413–446 (2020). [↩] [↩] [↩] [↩] [↩] [↩] [↩]
- Hansen, T., Slagsvold, B. & Moum, T., Childlessness and Psychological Well-Being in Midlife and Old Age: An Examination of Parental Status Effects Across a Range of Outcomes. Soc. Indic. Res. 94, 343–362 (2009). [↩]
- Norton, M. C. et al., Caregiver-recipient closeness and symptom progression in Alzheimer disease. The Cache County Dementia Progression Study. J. Gerontol. B. Psychol. Sci. Soc. Sci. 64, 560–568 (2009). [↩] [↩] [↩] [↩] [↩] [↩] [↩]
- Sundström, A., Westerlund, O., Mousavi-Nasab, H., Adolfsson, R. & Nilsson, L.-G., The relationship between marital and parental status and the risk of dementia. Int. Psychogeriatr. 26, 749–757 (2014). [↩]
- Edwards, H. B. et al., Quality of family relationships and outcomes of dementia: a systematic review. BMJ Open 8, e015538 (2018). [↩] [↩] [↩] [↩] [↩]
- Guarnera, J., Yuen, E. & Macpherson, H., The Impact of Loneliness and Social Isolation on Cognitive Aging: A Narrative Review. J. Alzheimers Dis. Rep. 7, 699–714 (2023). [↩] [↩] [↩] [↩]
- Truzzi, A. et al., Burnout in familial caregivers of patients with dementia. Rev. Bras. Psiquiatr. Sao Paulo Braz. 1999 34, 405–412 (2012). [↩] [↩] [↩] [↩] [↩] [↩] [↩] [↩] [↩] [↩] [↩] [↩] [↩]
- Mittelman, M. S. et al., Longitudinal study: understanding the lived experience of couples across the trajectory of dementia. BMC Geriatr. 21, 558 (2021). [↩] [↩] [↩] [↩] [↩] [↩] [↩] [↩] [↩] [↩]
- Vandepitte, S., Putman, K., Verhaeghe, S., Verdonck, C. & Annemans, L., Effectiveness of respite care in supporting informal caregivers of persons with dementia: a systematic review: Impact of dementia respite care in supporting caregivers. Int. J. Geriatr. Psychiatry 31, (2016). [↩] [↩] [↩] [↩] [↩]
- Fratiglioni, L., Paillard-Borg, S. & Winblad, B., An active and socially integrated lifestyle in late life might protect against dementia. Lancet Neurol. 3, 343–353 (2004). [↩] [↩] [↩] [↩]
- Joshi, P. et al., Social connections as determinants of cognitive health and as targets for social interventions in persons with or at risk of Alzheimer’s disease and related disorders: a scoping review. Int. Psychogeriatr. 36, 92–118 (2024). [↩] [↩]
- Rabanal, L. I., Chatwin, J., Walker, A., O’Sullivan, M. & Williamson, T., Understanding the needs and experiences of people with young onset dementia: a qualitative study. BMJ Open 8, e021166 (2018). [↩] [↩] [↩]
- Boss, L., Kang, D.-H. & Branson, S., Loneliness and cognitive function in the older adult: a systematic review. Int. Psychogeriatr. 27, 541–553 (2015). [↩] [↩] [↩]
- Elovainio, M. et al., Association of social isolation, loneliness and genetic risk with incidence of dementia: UK Biobank Cohort Study. BMJ Open 12, e053936 (2022). [↩] [↩]
- Peng, C., Hayman, L. L., Mutchler, J. & Burr, J., Friendship and Cognitive Functioning among Married and Widowed Chinese Older Adults. J. Gerontol. B. Psychol. Sci. Soc. Sci. (2021). [↩] [↩] [↩] [↩] [↩] [↩] [↩] [↩]
- Fortune, D., Whyte, C. & Genoe, R., The interplay between leisure, friendship, and dementia. Dement. Lond. Engl. 20, 2041–2056 (2021). [↩] [↩] [↩]
- Chopik, W. J., The Benefits of Social Technology Use Among Older Adults Are Mediated by Reduced Loneliness. Cyberpsychology Behav. Soc. Netw. 19, 551–556 (2016). [↩] [↩]
- Cotten, S. R., Anderson, W. A. & McCullough, B. M., Impact of internet use on loneliness and contact with others among older adults: cross-sectional analysis. J. Med. Internet Res. 15, e39 (2013). [↩] [↩] [↩] [↩] [↩]
- Piolatto, M. et al., The effect of social relationships on cognitive decline in older adults: an updated systematic review and meta-analysis of longitudinal cohort studies. BMC Public Health 22, 278 (2022). [↩] [↩] [↩] [↩] [↩]
- Nie, Y. et al., Social networks and cognitive function in older adults: findings from the HAPIEE study. BMC Geriatr. 21, 570 (2021). [↩] [↩]
- Svanberg, E., Spector, A. & Stott, J., The impact of young onset dementia on the family: a literature review. Int. Psychogeriatr. 23, 356–371 (2011). [↩]
- Orrell, M. et al., The impact of individual Cognitive Stimulation Therapy (iCST) on cognition, quality of life, caregiver health, and family relationships in dementia: A randomised controlled trial. PLoS Med. 14, e1002269 (2017). [↩]
- Sokolov, A. A., Collignon, A. & Bieler-Aeschlimann, M., Serious video games and virtual reality for prevention and neurorehabilitation of cognitive decline because of aging and neurodegeneration. Curr. Opin. Neurol. 33, 239–248 (2020). [↩]
- Dandibhotla, S., Impact of Psychosocial and Cultural Factors on the Prevalence of Dementia in Asian Populations: A Rapid Review of the Literature. Master Public Health Capstone Present. (2024). [↩]
- Kim, Y. & Schulz, R., Family caregivers’ strains: comparative analysis of cancer caregiving with dementia, diabetes, and frail elderly caregiving. J. Aging Health 20, 483–503 (2008). [↩]
- Lupien, S. J., McEwen, B. S., Gunnar, M. R. & Heim, C., Effects of stress throughout the lifespan on the brain, behaviour and cognition. Nat. Rev. Neurosci. 10, 434–445 (2009). [↩]



{kind=link}