
Abstract
Adolescent substance use is a critical public health concern shaped by social influences, particularly perceptions of peer and parental approval. While prior research has often examined these influences separately, fewer studies have tested how they interact. This study used data from 10,723 adolescents in grades 6–12 from the 2023 National Survey on Drug Use and Health (NSDUH) to evaluate whether perceived peer and parental approval of alcohol use jointly predict drinking behavior. Past 30-day alcohol use was modeled using linear regression with peer approval, parental approval, their interaction, and demographic controls. The interaction between peer and parent approval was statistically significant in initial some models but was not robust to alternative model specifications. These findings suggest that the combined role of peer and parental approval may be weaker than anticipated.
Keywords: Adolescent Substance Use, Peer Influence, Parental Approval, NSDUH, Regression, Youth Risk Behavior, Social Learning Theory
Introduction
Adolescence is a time of heightened vulnerability and self-discovery, where an adolescent’s life is centered around peer opinion and identity formation1. This developmental stage is marked by an increased risk of substance use, as adolescents are more likely to engage in experimentation due to underdeveloped decision-making capacities and heightened sensitivity to social pressures23. Early initiation of substance use is associated with numerous long-term consequences, including impaired brain development, academic difficulties, mental health challenges, and engagement in risky behaviors45. Moreover, substance use during this critical developmental period significantly increases the likelihood of developing substance use disorders in adulthood6.
Recent national data from the Monitoring the Future study confirm that alcohol, cannabis, and nicotine use remain prevalent among U.S. adolescents, despite gradual declines over the past decade7. Early use is also associated with co-occurring issues such as depression, anxiety, and delinquency8. Given these consequences, it is critical to understand the psychological and social factors that predict early substance involvement.
Biological and Genetic Vulnerability
Given the potential negative effects of substance use on health, it is important to understand the predictors of adolescent substance use. Biological predispositions are one factor that can lead to substance use. Adolescence is a time of significant neurological development and heightened sensitivity to reward. Research shows that adolescents are biologically primed for risk-taking behavior due to an imbalance between the developing prefrontal cortex, which controls impulse control and decision-making, and the more rapidly maturing limbic system, which is involved in emotion and reward processing29.10 emphasize that substances such as alcohol, marijuana, and nicotine hijack the brain’s dopamine reward pathway, reinforcing compulsive behaviors and weakening executive function over time.
Genetic factors can also result in increased substance use; individuals with a family history of addiction may inherit neurobiological traits, such as altered dopamine receptor sensitivity or reduced inhibitory control, which heighten their risk of substance use disorders1112. M. N. Potenza argues that these inherited vulnerabilities often interact with environmental stressors, like trauma or peer pressure, creating a compounded risk for early-onset substance use9.
Perceptions of Peer Approval and Conformity
While biological and genetic factors contribute to adolescents’ vulnerability to early-onset substance use, they do not act alone. A critical determinant of whether these predispositions translate into actual behavior lies in social and environmental contexts. In particular, perceptions of peer and parental approval play a central role in shaping whether adolescents experiment with or regularly engage in substance use. In particular, another major factor that may influence adolescent substance use is adolescents’ perceptions of social norms. Adolescent substance use may be affected by their perceptions of descriptive norms, or their beliefs about how common substance use is among their peers, and injunctive norms, which refer to what behaviors they believe their peers approve or disapprove of13. As Cialdini and Goldstein explain, individuals often conform to these norms to gain acceptance or avoid social rejection14.
Past research has demonstrated that people will change their behavior to align with their perceptions of social norms. For example, a widely popular psychology study by S. E. Asch discovered that people are likely to conform to a group’s opinion even if the group is wrong15. More recently, Cialdini et al. conducted a study to examine how descriptive norms work in a real-world setting. They found that hanging up signs in hotel rooms which emphasized that many previous guests reused their towels (a descriptive norm) was significantly more effective at encouraging reuse of towels than signs that emphasized environmental protection16. This study highlighted how subtle cues about others’ behaviors can powerfully influence individual decisions. Although the study did not involve adolescents or substance use, it illustrates the broader psychological principle that perceptions of what others do—descriptive norms—can strongly guide personal behavior. This mechanism also helps explain why teens who believe that their peers use or approve of substances may be more likely to engage in those behaviors themselves.
Considered all together, past research suggests that when teens believe that most of their peers are using substances (descriptive norms), or that their friends approve such behaviors (injunctive norms), they should be more likely to engage in substance use themselves. Indeed, some research has demonstrated that adolescents who perceive higher rates of substance use among their peers report greater personal use of substances, even when actual peer use is lower17. These misperceptions can create a feedback loop, normalizing risky behaviors. Other studies have shown that peer approval is one of the most consistent predictors of both current use and future intentions to use substances among adolescents1819.
Perceptions of Parental Approval and Support
Although peers are powerful socializing agents during adolescence, parental influence remains critical, particularly in early to mid-adolescence. Parents shape long-term behavior by instilling values, modeling decision-making, and providing communication, discipline, and emotional support that can reduce the likelihood of substance use20.
T. A. Wills and A. M. Yaeger categorized parenting influences into four domains: parenting practices, relationship quality, parental modeling, and family stress. Each of these factors shapes how adolescents respond to peer pressure and navigate challenging situations. Using a mediation model, they found that poor parenting, such as inconsistent discipline or low emotional support, can impair adolescents’ emotional regulation and increase susceptibility to peer influence. In contrast, their moderation model suggests that strong parent–child bonds foster resilience, allowing teens to maintain confidence and resist peer pressure even in high-risk situations21.
Other research supports this framework, showing that higher levels of parental monitoring, warmth, and communication predict lower levels of adolescent substance use222324. Moreover, the buffering effect of positive parenting appears strongest when combined with clear disapproval of substance use25.
More recent longitudinal research has emphasized the interactive nature of peer and parental influences, suggesting that parental disapproval may moderate the effects of peer norms. For example, Trucco, Colder, and Wieczorek found that adolescents with strong parental support were less likely to use substances even if they had peers who approved of or used drugs26. This aligns with findings from Wang et al., who demonstrated that parent–adolescent closeness reduced the impact of peer deviance on adolescent substance use over time27.
Theoretical Framework and Study Rationale
Taken together, past research suggests that adolescent substance use is influenced by multiple, overlapping social influences. Drawing on social learning theory, which posits that behavior is acquired through observation, imitation, and reinforcement within social contexts28, and social-ecological models of behavior, which emphasize the interactive effects of individual, family, and peer systems on development29, this study examines how these domains—peers and parents—may jointly predict adolescent substance use.
The central research question guiding this study is whether adolescents’ perceptions of peer and parental approval of alcohol use interact to influence their own alcohol use. Specifically, I explored whether adolescents who perceive both high peer approval and high parental approval of alcohol use would report the highest levels of alcohol use. This would suggest that peer and parental influences are not merely additive but amplify each other in shaping adolescent behavior.
The Present Research
In this paper, I investigate whether perceived peer approval and perceived parental approval of alcohol use predict adolescent alcohol use. These constructs are operationalized as adolescents’ beliefs about how acceptable regular alcohol use is to their close friends and parents, respectively, based on self-reported Likert-type items in the NSDUH dataset. This study examines whether these two forms of perceived approval interact to shape behavior.
One possibility is that there will be a positive interaction effect between these two social influences, with adolescents who perceive both high peer approval and high parental approval of alcohol use reporting the highest levels of alcohol use. In other words, the impact of perceived peer approval is expected to be stronger when parental approval is also high, suggesting a synergistic amplification, where combined permissive norms from both peers and parents increase substance use more than either influence alone.
Though I expect a positive interaction effect between perceived peer and parent approval of alcohol use on self-reported alcohol, it is possible that such an effect may be small. Alcohol use is likely shaped by factors—such as mental health, school climate, socioeconomic status, or broader cultural attitudes— that may limit the measurable impact of peer and parental approval in survey data. In addition, because alcohol use was self-reported, adolescents may have underreported their drinking for fear of getting in trouble, which could further weaken observed associations. In addition, because peer and parental approval were each measured with a single item in the NSDUH dataset, and the scale was limited to three response options (1–3), the measure did not allow for much variation. This restriction may have reduced the ability to detect more nuanced differences in adolescents’ perceptions of approval., such that subtle differences in perceived norms may not be fully captured. Thus, while I anticipate a positive interaction, null or modest effects may be attributable to aspects of the study design, rather than indicating that peer and parental approval do not influence adolescent alcohol use.
To test my hypothesis, I used a correlational design and analyzed data from the 2023 National Survey on Drug Use and Health (NSDUH). Multiple linear regression models were constructed to predict past 30-day alcohol use from perceived peer approval, perceived parental approval, their interaction term, and relevant demographic controls. Note that in the paper, I focus mainly on results for alcohol use, as national survey data indicates that alcohol remains the most commonly used substance among adolescents. In 2023, about 19.9% of youth ages 12–17 reported drinking alcohol in the past month, compared to lower rates for cigarette smoking and other substances (National Institute on Alcohol Abuse and Alcoholism [NIAAA], 2023). However, I ran the same analyses predicting marijuana use and cigarette use. For brevity, those results are reported in the supplementary materials.
Methods
Dataset
I analyzed data from the 2023 National Survey on Drug Use and Health (NSDUH), a publicly available cross-sectional survey conducted annually throughout each state in the United States. This survey is administered by the Substance Abuse and Mental Health Services Administration (SAMHSA) and it is designed to measure patterns, prevalence, and challenges of substance abuse along with mental health in individuals 12 or older in the US. The original survey followed strict guidelines via the IRB, such as informed consent, confidentiality, and compliance with research standards.
Data was collected via digital face-to-face interviews and audio-assisted self-interviewing, allowing participants privacy to increase the reliability of the self-reported data. This means that the data collected for each participant is a hybrid of a self-conducted survey and a digital interview. The participants for the survey are selected to ensure diversity among many different geographic and socioeconomic groups. Importantly, no participants are identifiable.
Participants
Participants included civilian and non-institutionalized people in the US aged 12 and older living in households, shelters, college dorms, and other quarters. People involved with the military, incarcerated individuals, and those actively receiving treatment were excluded from the survey. Participants were selected through random sampling to maintain demographic diversity. For this study, I focused solely on adolescent participants– those who were in 6th through 12th grade. Participants spanned grades 6–12 (M = 8.57, SD = 1.76), indicating that most were in middle to early high school.
Measures
In this study, perceived parental approval and perceived peer approval refer to adolescents’ beliefs about how accepting or permissive their parents or close friends are of regular alcohol use. This construct does not assess emotional support, parental monitoring, or general warmth — it specifically captures approval of regular alcohol use behaviors. These were measured with single items on 3-point Likert-type scales (1 = strongly disapprove, 2 = somewhat disapprove, 3 = neither approve nor disapprove), reverse-coded so that higher scores reflect greater perceived approval. While single-item measures are less robust than multi-item scales, the limited 3-point range also restricted variability in responses, which may have attenuated observed associations. These were the only available items in the NSDUH dataset and were selected for their face validity.
Parallel measures of peer and parental approval for marijuana and cigarette use were also available in the dataset. Those analyses are reported in the Supplementary Materials.
Alcohole Use. To assess alcohol use, participants were asked, “During the past 30 days, on how many days did you drink one or more drinks of an alcoholic beverage?” and could respond with how many days (1-30). Use of marijuana and cigarettes was measured similarly.
This outcome variable was treated as a continuous measure ranging from 0 to 30 days.
The distribution of responses was positively skewed rather than normal, so the alcohol use variable was log-transformed prior to analysis to better meet the assumptions of linear regression.
Perceptions of Peer SupportApproval or Perspective Norms for Substance Use. To assess perceived peer approvalsupport for substance use, participants were asked, “How do you think your close friends would feel about you having one or two drinks of an alcoholic beverage nearly every day?”. This item was reverse-coded so that higher scores would indicate greater perceived approval , such that 1 = Strongly disapprove, 2 = Somewhat disapprove, 3 = Neither approve nor disapprove, and NA = bad data, don’t know, refused to answer, or skipped. Use of marijuana and cigarettes was measured and reverse-coded in the same manner.
Perceptions of Parental SupportApproval for Substance Use. To measure perceptions of parental support for substance use, participants were asked: “How do you think your parents would feel about you having one or two drinks of an alcoholic beverage nearly every day?”. This item was also measured on a 3-point Likert-type scale and reverse-coded so that higher scores indicate greater perceived parental approval. This item was reverse coded so that higher scores reflect higher approval, such that 1 = Strongly Disapprove, 2 = Somewhat Disapprove, 3= Neither Approve or Disapprove, and NA= bad data, don’t know, refused to answer, or skipped. Questions for Marijuana and Cigarettes were asked similarly and reverse-coded in the same manner.
Demographic Variables. Participants reported their grade level, race (1 = White, 2 = Black/African, 3 = Native Am/AK Native, 4 = Native HI/Other Pac Isl, 5 = Asian, 6 =more than one race, 7 = Hispanic)1, Poverty was measured using the POVERTY3 variable from the 2023 NSDUH dataset, which represents household income relative to the federal poverty threshold, adjusted for family size and number of children. This variable was recoded on a four-point scale: 1 = less than 100% of the poverty threshold, 2 = 100–199%, 3 = 200–299%, and 4 = 300% or more. Higher scores reflect greater income relative to the poverty line (i.e., lower poverty). Household income was measured using a four-category ordinal variable representing total family income. Income was treated as an ordinal covariate in all analyses.
Analytical Strategy
I used multiple linear regression to examine the relationship between adolescent substance use and social influences, specifically perceptions of peer and parental approval. A model for alcohol use was created using past 30-day alcohol use variables as the outcomes. Predictor variables were constructed using survey items that captured adolescent perceptions of peer approval and parental approval of each drug. Parallel regression models predicting marijuana and cigarette use were also conducted; full results and figures are reported in the Supplementary Materials.
Regression models were first run without covariates and then repeated with demographic control variables (grade, race, and socioeconomic status). Because poverty and household income were highly correlated, only poverty status was retained in the final models to reduce multicollinearity. All models included interaction terms to assess whether perceptions of peer and parental approval for substance use interacted in predicting substance use outcomes. Significance was evaluated at the .05 level, with False Discovery Rate correction applied for multiple testing. All analyses were conducted in RStudio using tidyverse, dplyr, and associated packages. Missing or invalid responses were excluded through listwise deletion.
Participants with missing data on any key variables were excluded using listwise deletion. This reduced the dataset from an initial sample of 17,540 adolescents (grades 6–12) to a final analytic sample of 10,723, reflecting a 63.57% data loss. Cross-tabulations indicated that missingness was more prevalent among older students and among those reporting more frequent alcohol use. These patterns suggest that the data were not missing completely at random (MCAR), but likely missing at random (MAR). As such, interpretations of the results should consider this limitation. To account for multiple comparisons across the alcohol, marijuana, and cigarette models, False Discovery Rate (FDR) correction was applied to interaction terms. Adjusted p-values were interpreted alongside original p-values to evaluate robustness of effects.
Deviations from Pre-Registration
This study was pre-registered on the Open Science Framework, but several deviations were made during the research process to improve clarity, accuracy, and analytical focus.
First, the preregistration proposed analyzing the effects of peer approval and parental approval in separate models. However, the final models analyzed both effects in the same model and incorporated an interaction term to capture the multiplicative influence of these factors.
Second, the preregistration specified creating a composite outcome of past 30-day alcohol, marijuana, and cigarette use. Cronbach’s alpha for this composite was low (α = 0.38), indicating that these items reflect distinct forms of use rather than a single construct. To preserve validity, each substance was analyzed separately. For brevity, the main manuscript focuses on alcohol use, while marijuana and cigarette models are reported in the Supplementary Materials.
Third, the preregistration did not account for procedures in the case of skewness in the outcome variables. However, because the outcome was positively skewed, alcohol use was log-transformed to better meet the assumptions of linear regression. The log-transformed results are reported in the main paper, as they provide a more appropriate test.
Fourth, several preregistered predictors were excluded because they applied only to a subset of respondents or showed poor alignment with the constructs of interest. Excluded variables included non-alcohol substance use indicators (SEDPAST30, STIMPAST30, PAINRPAST30, PAINRPAST302, nicotine vaping), additional peer influence items (PEEROFFER, FRIENDSMJ, STUSMOKE, STUMJ, STUDRUNK), and parental variables (PRTABTDRG, FEELABTTRY).
Finally, missing data was handled using listwise deletion, which reduced the analytic sample but provided a straightforward approach for maintaining consistency across models. These deviations reflect data-informed adjustments that improve rigor while staying aligned with the theoretical goals of the preregistration.
Results
Participants
The final analytic sample consisted of 10,723 adolescents in grades 6 through 12. “Participants spanned grades 6–12 (M = 8.57, SD = 1.76). 19.7% of participants reported incomes less than $20,000, 27.0% reported $20,000–$49,999, 14.3% reported $50,000–$74,999, and 39.1% reported $75,000 or more. The average poverty score was 2.39 (SD = 0.81), meaning that most participants lived in households with incomes between 100% and 300% of the federal poverty line—that is, above the official poverty threshold but below the highest income category. In terms of race and ethnicity, the sample was diverse: 44.7% of participants identified as White, 13.81% as Black or African American, 1.84% as Native American or Alaska Native, 0.54% as Native Hawaiian or Pacific Islander, 6.17% as Asian, 6.68% as multiracial, and 26.26% as Hispanic or Latino.

Note. This table displays results from a multiple linear regression model predicting adolescents’ past 30-day alcohol use from the interaction between perceptions of peer approval and parental approval. The model also includes demographic controls of grade, race, and socioeconomic status.
To test my hypothesis and better understand the social and demographic factors influencing adolescent alcohol use, I conducted a multiple linear regression including perceived peer approval, perceived parental approval, their interaction, and demographic controls (grade, race, and socioeconomic status). Initially, the model was estimated using the raw outcome variable (past 30-day alcohol use), and the peer × parent approval interaction was statistically significant. However, because the outcome distribution was positively skewed, alcohol use was subsequently log-transformed to better meet the assumptions of linear regression. In this log-transformed model, the interaction no longer reached conventional significance thresholds, though the pattern of results remained consistent, such that the interaction effect was positive. Results from the log-transformed model are reported here, as they provide the most appropriate test of the study’s predictions.
Though perceived peer approval of alcohol use had a positive relationship with self-reported alcohol use, it was not a statistically significant predictor (B = 0.02, p = .825, 95% CI [–0.19, 0.24]). Perceived parental approval was also very weakly associated with self-reported alcohol use and was not a statistically significant predictor (B = –0.15, p = .445, 95% CI [–0.54, 0.24]).
The interaction between perceived peer and parental approval of alcohol use was also not statistically significant in the log-transformed model (B = 0.09, p = .252, 95% CI [–0.06, 0.24]). Nevertheless, the estimated marginal means supported the hypothesized trend: adolescents who perceived both high peer and high parental approval reported the greatest alcohol use. Predicted log alcohol use was highest for participants who reported both high peer and parental approval (M = 1.147, SE = 0.116), compared to participants who reported high peer approval and –low parental approval (M = 0.533, SE = 0.239), low peer approval and–high parental approval (M = 0.897, SE = 0.080), and low peer approval and parental approval (M = 0.679, SE = 0.051). Back-transformed to raw days of use in the past 30 days, these means corresponded to using alcohol 3.15 days, 2.45 days, 1.97 days, and 1.70 days per month, respectively. This descriptive pattern suggests that alcohol use tended to be highest when both peer and parental approval were permissive, consistent with the idea that adolescents may be especially likely to drink when neither of their primary social environments establishes strong anti-use norms.
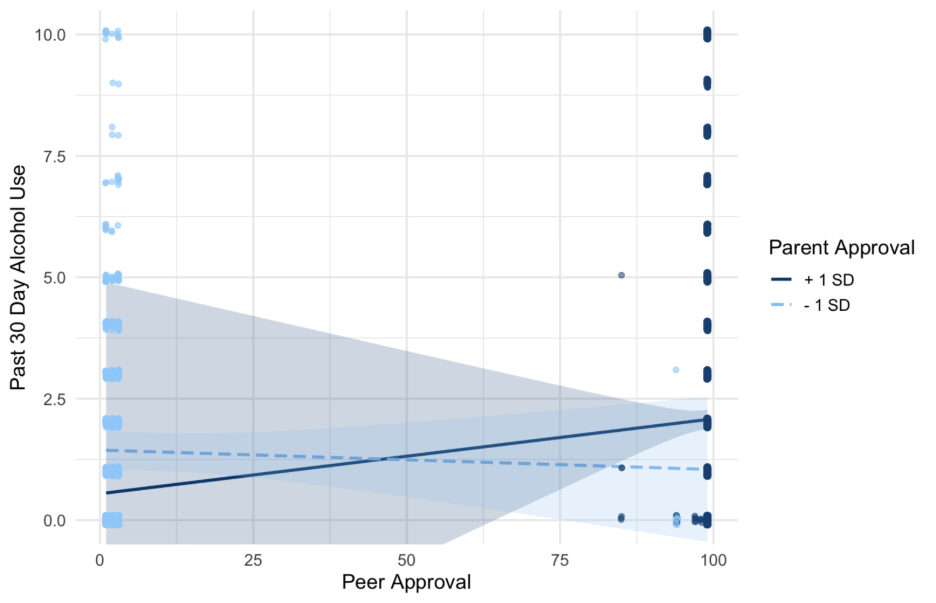
Note. This figure illustrates the interaction between perceived peer and parental approval in predicting adolescents’ past 30-day alcohol use. The Y-axis has been adjusted to enhance visual clarity. The slopes suggest a possible trend consistent with the hypothesized interaction, with alcohol use highest when both peer and parental approval are high. However, the interaction effectis pattern did not reach statistical significance in the log-transformed model.
Finally, among the demographic variables, none emerged as statistically significant predictors of alcohol use in the final model. Grade level showed a small, positive but non-significant association (B = 0.06, p = .167, 95% CI [–0.02, 0.14]), suggesting that alcohol use may increase slightly with grade, though this effect did not reach significance in the present analyses. This contrasts with national survey data showing that alcohol use often becomes more common in later high school years. The effects of socioeconomic were also non-significant.
Discussion
This study examined the impact of the perception of parental approval for drug use and the perception of peer approval for drug use on self-reported alcohol use using the 2023 National Survey on Drug Use and Health6. Although peer approval showed stronger correlational relationships with substance use than parental approval, neither variable independently predicted alcohol use in the regression model. After log transformation, the peer–parent interaction did not reach statistical significance, though the pattern of results was consistent with the exploratory hypothesis that adolescents who perceived both high peer and high parental approval tended to report the highest alcohol use. While this trend is consistent with theories of social influence, it did not reach statistical significance, and should therefore be interpreted cautiously as exploratory. Parallel models for marijuana and cigarette use, reported in the Supplementary Materials, showed similar non-significant interaction effects.
The results of my analysis contribute to insights in fields such as adolescent psychology and public health. The positive relationship between peer approval and alcohol use supports research on normative behavior and social learning2814. As stated in my introduction, adolescents are extremely sensitive to perceived peer norms—both descriptive and injunctive—and mirror the behaviors of those around them1317. This aligns with Bandura’s theory of social learning and various research on conformity2815. My analysis and others have found that adolescents want to fit in with their social groups and often engage in risky behaviors they believe are normal or encouraged by friends1417.
My findings also support the importance of parental influence, especially during adolescence, a critical developmental period202221. Even as adolescents become more involved with peers, parental approval is still associated with lower rates of drug use2123. Although parental approval did not independently predict alcohol use in this sample, its role in moderating peer influence suggests that parent messages may still serve as a protective buffer—particularly when peer norms are permissive. The significance of both influences affects our understanding of adolescent behavior, showing that peer and parental environments must be considered together29.
My findings also align with family systems theory, which suggests that adolescent behavior is influenced by multiple overlapping influences30. A relevant study by Bernburg, Thorlindsson, and Sigfusdottir found that teens who lived in neighborhoods with weak supervision, high stress, and no sense of community were more likely to use substances, even if their parents were involved or highly disapproving29. This supports social disorganization theory, which argues that environments lacking structure and support enable risky behavior29.
Building on this, Lander, Howsare, and Byrne explain that substance abuse isn’t always about parenting alone—it often reflects the overall health of the household30. While my analysis did not directly assess family dynamics or emotional roles, this framework offers a useful lens to interpret how broader family stressors may contribute to adolescent vulnerability. For instance, when one family member is suffering, such as a parent with addiction, it can affect everyone in the home. Teens in these situations may experience emotional neglect or trauma even in the absence of direct abuse. They may also experience parentification, where they take on adult responsibilities prematurely and lack emotional regulation and support. Although not measured in this dataset, such dynamics may help explain why some adolescents turn to substances to cope. Mafa and Makhubele support this idea in their research involving parents of children in substance abuse programs. These parents described feeling extreme guilt, helplessness, and isolation. Their findings illustrate how the emotional dynamics within a family, not just individual parenting decisions, influence adolescent outcomes31. These teens may not be “bad” kids making bad choices—they may simply carry emotional burdens that no child should have to carry alone.
Based on these findings, prevention efforts should address how peer and parental norms interact—particularly for older adolescents, whose risk of alcohol use increases with age and exposure to permissive social settings21. For schools, this could involve implementing peer-led programs that reshape social norms around substance use, such as social norms marketing campaigns or student ambassador models that emphasize healthy behaviors. Families could benefit from parent education workshops that teach caregivers how to clearly communicate disapproval of substance use while remaining emotionally supportive. These programs should specifically address how even subtle forms of parental permissiveness can amplify peer influence. Policymakers might support these efforts by funding family-school partnerships or integrating adolescent-focused modules into public health campaigns that reinforce both parental monitoring and peer resistance skills. Together, these targeted strategies may help create a more consistent network of disapproval around underage substance use.
Future research might combine the psychological factors investigated here with biological predictors such as genetic predispositions1112. This would allow researchers to see whether certain adolescents are more biologically vulnerable to peer or parental influences. A longitudinal study would be especially valuable for clarifying the directionality and developmental timing of peer and parental influence on substance use. Tracking adolescents over time would allow researchers to determine whether perceived approval precedes increases in substance use, or if substance use shapes perceptions of peer and parent norms.
Future studies could include repeated measures of perceived approval, actual substance use behaviors, and relationship quality (e.g., parental warmth, peer closeness) across multiple developmental stages. Growth curve modeling or cross-lagged panel designs could be used to examine changes and reciprocal effects over time. This approach would also allow researchers to identify critical windows—such as transitions into high school—when adolescents may be most sensitive to social influences.
This study had several limitations. First, it relied on cross-sectional data, which prevents any claims about causality29. Although significant associations were observed, the direction of these relationships remains uncertain. Second, all data were self-reported, which introduces the possibility of social desirability bias and underreporting, particularly around sensitive topics like substance use6. Third, the dataset excludes high-risk adolescents who are incarcerated, institutionalized, or have dropped out of school, limiting generalizability6.
Several preregistered variables were excluded from the final models due to conceptual misalignment, inconsistent coding, or high missingness. These included non-alcohol substance use indicators (e.g., SEDPAST30, STIMPAST30), peer influence items (e.g., PEEROFFER, FRIENDSMJ), and additional parental variables (e.g., PRTABTDRG, FEELABTTRY). Additionally, peer and parental approval were assessed using single-item measures. While these were face valid and consistent across substances, they did not allow for internal reliability assessment and may not fully capture the complexity of perceived norms.
The final analytic sample was derived using listwise deletion, which excluded participants with missing data on any model variable. This likely reduced the sample size and potentially introduced bias, particularly if missingness was not random. For example, older adolescents or heavier alcohol users may have been underrepresented. Furthermore, although demographic covariates (e.g., grade, race, income) were included, the study may also be affected by residual confounding from unmeasured variables such as mental health, parenting quality, or school environment.
Finally, this study did not account for broader contextual factors such as family structure, school climate, or neighborhood characteristics, which likely influence adolescent substance use. For example, adolescents from single-parent or economically strained households may experience different levels of parental monitoring or emotional availability, which could affect how parental approval messages are received. Similarly, school environments with strong prevention programs, teacher support, or positive peer cultures may buffer against risky behaviors. Lastly, neighborhood-level disadvantage or disorganization—including exposure to violence, lack of recreational resources, or low community cohesion—has been associated with increased substance use among youth29. Future research should incorporate multi-level data to better understand how these structural factors interact with peer and parental influences.
Although this study focused on adolescents aged 12 to 18, it did not examine developmental differences within this age range. Prior research suggests that peer and parental influences may operate differently depending on developmental stage, with parental approval exerting greater influence in early adolescence and peer norms becoming more dominant in later adolescence1. By analyzing the full adolescent sample as a single group, the study may have missed important age-related variations in the interaction between peer and parental approval. Future research should explore whether these social influences function differently across grade levels or developmental stages, potentially revealing critical periods of vulnerability or protection.
Conclusion
In summary, findings from this study indicate that adolescent substance use is influenced by multiple interacting factors. Teens are shaped by their peers, families, and broader social environments. During this vulnerable stage of development, both peer and parent messages can significantly impact behavior. When both sources reinforce risky behaviors—or when positive parental guidance is absent—adolescents may be more likely to engage in substance use, whether to cope or conform to perceived norms.
These findings suggest that effective interventions must consider the combined influence of peer and parental environments. Rather than focusing solely on individual responsibility or punishment, prevention efforts should prioritize creating supportive social conditions, both at home and in schools. Strategies might include programs that strengthen parent–child communication, teach adolescents how to resist peer pressure, and foster positive peer networks.
To truly support youth, we must look beyond surface-level behaviors and address the underlying social, emotional, and environmental conditions that shape their choices. By doing so, we can promote healthier developmental trajectories and reduce the risk of substance use during adolescence.
Supplementary Materials
Supplementary tables and figures provide full regression results and interaction plots for marijuana and cigarette use. These materials are available at: https://1drv.ms/w/c/f67203a914dcac15/EbAIR97WQL5Ms-kA6IempUABe3eIyUxxce-ZLOZuZCu1NQ?e=8GEuWC
Acknowledgments
I would like to thank my research mentor, Sydney Garcia, for her guidance throughout this project, especially in helping me understand the data analysis process, teaching me how to conduct quality research, and refining my methodology. I am also grateful to the Substance Abuse and Mental Health Services Administration (SAMHSA) for making the 2023 National Survey on Drug Use and Health publicly available, which provided the foundation for this research. Special thanks to my mom and Dad, who have always supported my academic goals, for their encouragement during this process, and to my twin brother Owen for inspiring me in everything I do.
References
- L. Steinberg. Cognitive and affective development in adolescence. Trends in Cognitive Sciences. 9, 69–74 (2005). [↩] [↩] [↩]
- B. J. Casey, S. Getz, A. Galvan. The adolescent brain. Developmental Review. 28, 62–77 (2008). [↩] [↩] [↩]
- L. M. Squeglia, J. Jacobus, S. F. Tapert. The influence of substance use on adolescent brain development. Clinical EEG and Neuroscience. 40, 31–38 (2009). [↩]
- K. C. Winters, C. Y. S. Lee. Likelihood of developing an alcohol and cannabis use disorder during youth: Association with recent use and age. Drug and Alcohol Dependence. 92, 239–247 (2008). [↩]
- S. Levy. Adolescent substance use: A public health priority. Pediatrics. 143, e20182752 (2019). [↩]
- Substance Abuse and Mental Health Services Administration. 2023 National Survey on Drug Use and Health (NSDUH): Methodological Summary and Definitions. U.S. Department of Health and Human Services (2023). [↩] [↩] [↩] [↩]
- L. D. Johnston, R. A. Miech, P. M. O’Malley, J. G. Bachman, J. E. Schulenberg, M. E. Patrick. Monitoring the Future National Survey Results on Drug Use, 1975–2022: Overview, Key Findings on Adolescent Drug Use. Institute for Social Research, University of Michigan (2023). [↩]
- K. M. King, W. G. Iacono, M. McGue. Childhood externalizing and internalizing psychopathology in the prediction of early substance use. Addiction. 99, 1548–1559 (2004). [↩]
- M. N. Potenza. Neurobiology of addiction: An overview. Psychiatric Times. 20, 1–8 (2003). [↩] [↩]
- J. C. Coleman, R. H. Kay. Adolescence and Health: Problems and Prevention. Wiley (1981). [↩]
- N. D. Volkow, T. K. Li. The neuroscience of addiction. Nature Neuroscience. 8, 1429–1430 (2005). [↩] [↩]
- G. R. Uhl, R. W. Grow. The burden of complex genetics in brain disorders. Archives of General Psychiatry. 61, 223–229 (2004). [↩] [↩]
- R. B. Cialdini, C. A. Kallgren, R. R. Reno. A focus theory of normative conduct: A theoretical refinement and reevaluation of the role of norms in human behavior. Advances in Experimental Social Psychology. 24, 201–234 (1991). [↩] [↩]
- R. B. Cialdini, N. J. Goldstein. Social influence: Compliance and conformity. Annual Review of Psychology. 55, 591–621 (2004). [↩] [↩] [↩]
- S. E. Asch. Opinions and social pressure. Scientific American. 193, 31–35 (1955). [↩] [↩]
- R. B. Cialdini, R. R. Reno, C. A. Kallgren. Managing social norms for persuasive impact. Social Influence. 3, 142–146 (2008). [↩]
- B. Borsari, K. B. Carey. Peer influences on college drinking: A review of the research. Journal of Substance Abuse. 13, 391–424 (2001). [↩] [↩] [↩]
- K. A. Maxwell. Friends: The role of peer influence across adolescent risk behaviors. Journal of Youth and Adolescence. 31, 267–277 (2002). [↩]
- B. Simons-Morton, T. Farhat. Recent findings on peer group influences on adolescent smoking. The Journal of Primary Prevention. 31, 191–208 (2010). [↩]
- B. J. Biddle, B. J. Bank, M. M. Marlin. Parental and peer influence on adolescents. Social Forces. 58, 1057–1079 (1980). [↩] [↩]
- T. A. Wills, A. M. Yaeger. Family factors and adolescent substance use: Models and mechanisms. Current Directions in Psychological Science. 11, 182–185 (2002). [↩] [↩] [↩]
- L. Steinberg. We know some things: Parent–adolescent relationships in retrospect and prospect. Journal of Research on Adolescence. 11, 1–19 (2001). [↩] [↩]
- S. J. Latendresse, R. J. Rose, R. J. Viken, L. Pulkkinen, J. Kaprio, D. M. Dick. Parenting mechanisms in links between parents’ and adolescents’ alcohol use behaviors. Alcoholism: Clinical and Experimental Research. 32, 322–330 (2008). [↩] [↩]
- E. C. Hair, K. A. Moore, S. B. Garrett, T. Ling, K. Cleveland. The continued importance of quality parent–adolescent relationships during late adolescence. Journal of Research on Adolescence. 18, 187–200 (2009). [↩]
- T. J. Dishion, R. J. McMahon. Parental monitoring and the prevention of child and adolescent problem behavior: A conceptual and empirical formulation. Clinical Child and Family Psychology Review. 1, 61–75 (1998). [↩]
- E. M. Trucco, C. R. Colder, W. F. Wieczorek. Vulnerability to peer influence: A moderated mediation study of early adolescent alcohol use initiation. Addictive Behaviors. 36, 729–736 (2011). [↩]
- M. T. Wang, T. J. Dishion, E. A. Stormshak, J. B. Willett. Trajectories of family management practices and early adolescent behavioral outcomes. Developmental Psychology. 47, 1324–1341 (2015). [↩]
- A. Bandura. Social Learning Theory. Prentice-Hall (1977). [↩] [↩] [↩]
- J. G. Bernburg, T. Thorlindsson, I. D. Sigfusdottir. The roots of social capital: The role of youth participation in local community settings in fostering civic engagement and reducing substance use. Acta Sociologica. 52, 159–187 (2009). [↩] [↩] [↩] [↩] [↩] [↩]
- L. Lander, J. Howsare, M. Byrne. The impact of substance use disorders on families and children: From theory to practice. Social Work in Public Health. 28, 194–205 (2013). [↩] [↩]
- I. Mafa, J. Makhubele. The impact of substance abuse on parenting. Journal of Social Work Practice. 24, 175–186 (2010). [↩]



{kind=link}