
Abstract
This study investigates the comparative effectiveness of aquatic therapy and land-based treatment through a mixed-methods approach that combines a literature review and case analysis of 15 comparative experiments on Osteoarthritis (OA), a type of musculoskeletal injury (MSK-I). After a month of research, (H.P) and (Y.K) accumulated 34 random controlled trial articles regarding OA and hydrotherapeutic treatment but excluded 19 due to distinct language and insufficient scores from the PEDro scale. Furthermore, all the participants were over 18 to mitigate the underdevelopment of patients. According to the literature research, rehabilitation is essential for preventing injuries and enabling participation in ongoing physical activity. In particular, aquatic therapy offers distinct environmental treatment than ordinary land-based therapy as it is conducted underwater. Despite the uniqueness of aquatic therapy, the cumulative findings indicate no statistically significant difference between hydrotherapy and land-based therapy in reducing pain, improving physical function, and raising quality of life. In addition, systematic findings suggest a lack of sufficient data from available studies and trials to confirm the general effectiveness of hydrotherapy. In addition, systematic results reveal considerable variability of insufficient data sets and unconventional development of aquatic therapy. The variability may be influenced by individual circumstances or the experiment’s environment. However, preventative treatments like land-based and aquatic therapy could help patients progressively reintegrate following an accident and significantly lessen its long-term repercussions.
Keywords: Aquatic therapy, land-based therapy, osteoarthritis, rehabilitation, injury prevention, physical activity
Introduction
Water plays a unique role in recovery compared to conventional medicine. This article, therefore, attempts to show how hydrotherapy differs from other treatments and provides better clinical results than land-based therapy.
With the unique benefits aquatic therapy offers, the cumulative experimental data will indicate that aquatic therapy shows better treatment results than typical land-based treatment in relieving pain, physical function, and quality of life.
The first section of the paper provides background information to help readers better understand how this paper approaches the research questions in depth and raises awareness of the current research amount. The second section discusses the methodology used further. Lastly, this paper analyzes, discusses, and interprets the conclusion.
Background and Context
Benefits of Exercises
Frequent exercise has significant positive effects on general health. It strengthens bones and muscles, increases energy, and improves cognitive function. It lowers the risk of developing long-term conditions like diabetes, cancer, and obesity. Diverse forms of exercise help teens develop physically, emotionally, and socially while promoting long-term health and well-being. However, there are hazards associated with physical activity. Injuries can have immediate and long-term physical effects1 such as reduced risk of obesity or cancer.
Musculoskeletal Injuries and Osteoarthritis
Musculoskeletal injuries (MSK-I) are injuries to the muscular, skeletal, or connective systems that are caused by repetitive motion, physical overexertion, and trauma. MSK-I includes disorders such as Osteoarthritis, Rheumatoid Arthritis, Osteoporosis, Fibromyalgia, and low Back Pain, which are the most common MSK-I. These include sprains, strains, fractures, dislocations, and sports-related musculoskeletal disorders in muscles, bones, nerves, ligaments, and tendons. MSK-I is one of the most influential causes of chronic pain and disability worldwide, affecting approximately 1.71 billion people, making it a major factor affecting quality of life and healthcare systems worldwide that have dramatically affected the quality of life and healthcare. In particular, MSK-I’s major contribution to sports-related injuries globally makes up the major occupational health problems, responsible for a considerable percentage of cases of desertion and lost physical performance for occupational athletes such as the NFL, NBA, etc2.
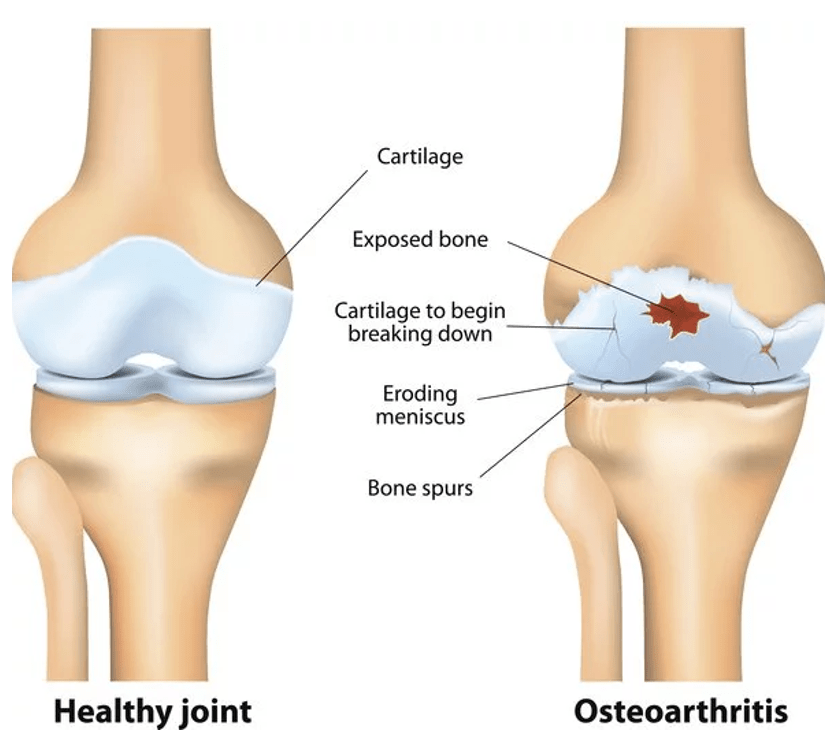
The leading disorder worldwide, Osteoarthritis (OA) is a degenerative joint most common in the knees, spine, and hands. It develops slowly and worsens over time. It affects the entire joint, including the tissues around it. It occurs when the cartilage within other joints gradually deteriorates (see Appendix A for demographic information). As cartilage breaks down, bones are put at risk of directly rubbing against each other, which causes swelling, stiffness, joint pain, reduced flexibility, and more. Factors such as aging joint damage and genetic defects are the main contributors to Osteoarthritis. Over time, this interferes with body movement and causes more discomfort.
Recovery from Injury
Limiting physical activity is necessary throughout the healing process of an ankle injury to promote proper healing without requiring a lengthy recuperation period, since OA is relatively common with a history of ankle injuries, particularly involving ligament tears, fractures, and chronic disability. After six to ten weeks in MSK-I, rehabilitation begins with physiotherapy (may start with surgery depending on the situation), which improves muscular strength and range of motion while restoring physical functionality and reducing discomfort. The overall data has shown that this more than 12-month rehabilitation period dramatically reduces pain and the risk of re-injury, demonstrating the value of physical therapy. However, note that some may take less time or more depending on the extremity of the injuries. Since inflexible joints and muscles hinder healing by decreasing blood flow and nutrient delivery, range of motion restoration and stiffness reduction are essential. Lastly, following an injury, rehabilitation speeds up recovery, builds resilience, and promotes physical performance3.
Physical Rehabilitation
Returning from an athletic injury is a painful process. Most patients receive medical and physical treatment to recover and prepare for their debut. The transition is an essential factor for patients for several reasons (To see furthure details, see Table 1 in the appendix)
Medical Treatment
There are two broad types of medical treatment: Immobilization and Medication.
Immobilization is often used for fractures, sprains, or torn muscles. Medical treatment using splints, casts, or walking boots allows the injured area to maintain stability. This technique is widely applied in biomechanics, fastening healing by forcefully stabling the wounded area4,5.
Rehabilitation
While musculoskeletal injuries have a devastating impact on overall quality of life, such as sleep and mental health, numerous studies have ascertained improved sleep, mental health, and stress management. Aquatic therapy improves balance, coordination, and mobility while reducing joint and bone stress due to water’s buoyancy. Water offers safe, practical exercises that strengthen muscles, improve endurance, and enhance quality of life-boosting confidence in movement for quicker recovery6.
Unique Traits of Hydrotherapy
Hydrotherapy allows patients to recover efficiently with distinct characteristics from land-based therapy, such as pain relief, increased mobility, and freedom of movement.
Pain Relief and Aquatic Rehabilitation
Buoyancy minimizes the load on joints and injured tissues, enabling patients to perform exercises with minimal pain or risk of re-injury. Water’s resistance supports muscle strengthening and enhances cardiovascular endurance without strain. Therefore, aquatic therapy suits patients or athletes with persistent musculoskeletal disorders who cannot tolerate traditional, land-based therapies. It offers a safe therapeutic environment to reduce pain. Moreover, its buoyancy with mild resistance reduces joint strain. If joint strain worsens, it decreases flexibility and muscle growth7,8.
Underwater treatment offers new therapeutic alternatives and enables patients to relieve pain. Aquatic therapy is particularly beneficial for post-surgery rehabilitation compared to other on-ground therapies. It makes exercises more effective in strengthening muscles without excessive strain, which helps in rehabilitation and prevents further injury9.
Increased Mobility and Freedom of Movement
Specifically, Osteoarthrtitis patients often face heavy joint stress, which leads to pain, reduced mobility, and balance. However, hydrostatic pressure in water improves circulation, reduces swelling, and fastens tissue healing. Warm water relaxes the body and reduces pain and stiffness while improving mobility.
Water-based exercises, such as functional tasks, strengthening exercises, mobility exercises, and cardiovascular conditioning, allow patients and athletes to reach a broader range of motion due to hydrostatic pressure. Hydrostatic pressure helps muscular relaxation and decreases joint compression, which leads to less pain.
Based on an experiment conducted on Osteoarthritis patients, aquatic therapy programs have increased flexibility, mobility, and strength. The nonstop effort in developing aqua therapy and the rapid evolution in return allow patients to access various types of treatment and enhance overall technology10.
Problem Statement and Rationale
Osteoarthritis is one of the most prevalent musculoskeletal conditions. It affects about 528 million people worldwide, and its prevalence has increased by 113% since 199011. This finding is mainly due to the substantial increase in the population and athletes worldwide. Despite the predominant portion of the physical disorder, no treatment has been discovered to cure Osteoarthritis. The disproportionate ratio of treatment availability and prevalence of the disorder devastates the patients with MSK disorders. Osteoarthritis has no known cure despite being the most common physical disorder. Nonetheless, several studies have demonstrated that rehabilitation activities can lessen discomfort by releasing tension from tendons and muscles and regaining flexibility
Significance and Purpose
The lack of existing research is not only just related to treatment development, but also closely related to education. 83% and 53.1% of medical schools require MSK courses and Osteoarthritis, respectively. However, many studies on MSK struggle due to a lack of research, a small sample size, and a lack of standardized protocols. On the other hand, many studies have identified that the current curriculum and knowledge assessment are far behind the demand for MSK-I treatment. Therefore, this paper expands the knowledge of MSK and Osteoarthritis in medical schools. Furthermore, this paper could be a catalyst for current findings and encouragement in developing further research regarding MSK-I12,13
Objectives
Through this systematic review, this paper aims to raise awareness of the lack of resources and general knowledge of MSK. A new innovative rehabilitative approach, aquatic therapy could be a ground breaking findings to prevent and potentially cure MSK-I. Based on existing literature review, it is an analytical conjecture that aquatic therapy will offer better results than land-based therapy due to better suited for MSK-I patients by allowing easier movement with water buoyancy.
Scope and Limitations
This systematic review solely focuses on adult patients with Osteoarthritis. Adolescents have been excluded from this study due to the ongoing growth of their bodies, which would be an uncontrollable variable. Moreover, our accumulated research data consists of 18 years old or above, which makes an extensive range of age groups in this study. Moreover, there may be potential bias, as each of the studies may have utilized different methods and exercises, which could affect the conclusions’ accuracy. Moreover, the research concluded that there were insufficient data sets from reviewed 15 studies.
Methodology Overview
Through a systematic approach, editor (H.P) and (Y.K) thoroughly gathered 34 relevant articles to our research question but excluded 19 of them due to various issues and potential biases that may be caused. After, we utilized standardized mean difference (SMD), to accurately compare data from different articles. Then, this paper visualized the data conclusion with figures and tables.
Results & Statistical Analysis
Outcomes are solely focused on the level of pain, physical function, and quality of life reported by included studies in people with musculoskeletal conditions. Studies with more than two reported interests above were prioritized by their significance level.
The systematic review was conducted by extracting article data and converting it to standardized mean differences (SMDs) with 95% confidence intervals to compare each data set. By using SMD, it allows researchers to effectively compare data sets with different sample sizes, overall quality of comparability, and accuracy. Negative signs were required to derive the scale directions (Aquatic Therapy was derived to negative signs, and land-based therapy was derived to positive signs). In other words, the absolute value of SMD represents the level of effectiveness presented by each study. SMD values of 0.2-0.5 are considered small, 0.5-0.8 are considered medium, and values > 0.8 are considered significant.
The data tables and graphs based on gathered data indicate the meaningful outliers and variances. These factors reflect on the ongoing development of therapeutic principles, which led to considerable outliers. Moreover, the factors suggest global effort in therapeutic research to set stable principles and make more data sets accessible to the public.
Interpretation
Referring to Table 2, it suggests that SMD varies significantly depending on how the authors conducted the experiments. In addition, CI (95%) indicates that the experimental data result is reliable, meaning that 95% of the data sets lie on the SMD. However, the combined SMD value is almost zero. No significant differences in SMD were found in terms of hydrotherapy efficacy. Although combining all the sums of SMDs suggested hydrotherapy was more effective, the lack of prior research and data needs to be considered. neglecting tIn other words, the sample size is too small to conclude that hydrotherapy is more effective than land-based therapy in relieving pain, restoring body function, and improving the quality of life.
Despite the existence of other musculoskeletal conditions such as Rheumatoid Arthritis, Osteoporosis, Fibromyalgia, or lower Back Pain, the systematic approach of the research was not able to analyze the effectiveness of the conditions and conclude due to lack of current experimental data and literature reviews.
According to Figure 2, studies such as Fransen (2007), Lim (2010), Stener-Victorin (2004), and Wyatt (2001) found that water exercise has a negative SMD value, whereas land exercise has a negative SMD value for Water exercise ranged from -2.95 (Stener-Victorin, 2004) to -0.39 (Patrick, 2001), indicating consistent effectiveness. On the other hand, land-based exercises such as Hale (2012), Wang (2011) and Slouma (2024) have SMD values mostly near zero or sometimes positive. This indicates a moderate improvement compared to the aquatic treatment.
Analysis & Insights
Studies conducted during 2000–2010 report more substantial effectiveness for aquatic exercise, while studies in 2022–2024 reflect variability. The leading cause of this factor is potentially improved land-based exercise techniques or methodologies. The limited effort of aquatic therapy development has led to a shift in focus to land-based therapy, as it is more accessible to the public and requires no facility. However, the lack of global effort to examine the effectiveness of aquatic therapy has led to insufficient resources. The number of experiments conducted during the early 2000s was significantly larger than during the 2020s.
As shown in Figure 2, outliers in this systematic review indicate tremendous SMD values, such as Stener-Victorin (2004), with SMD = -2.95, significantly larger than other experimental data (SMD range: -0.50 to 0.50) and Slouma (2024) appears to be an outlier with SMD = 1.8. Refer to Figure 1, it indicates the wide range of outliers: Stener-Victorin (2004) and Slouma (2024), which increases the variance of the combined SMD. In other words, the variance in combined SMD may lead to the systematic review’s disproportionate impact. The variance points to uncontrollable variables such as sample size and different methods. Alternatively, the combined experimental conditions and SMD skew more toward the water treatment.
Discussion
Musculoskeletal injuries significantly impact physical growth, performance, and health. One of the most prevalent MSK-I, Osteoarthritis, is a degenerative joint condition that affects overall body functions such as hands, knees, and spine, which is the subject of this study. Osteoarthritis is characterized by stiffness, pain, limited mobility, and cartilage destruction. Age, joint injury, and inheritance are common factors. Osteoarthritis hinders everyday tasks and athletic performance by affecting bone production, muscle growth, and mobility. However, increasing awareness of the injury risks and hydrotherapeutic treatment can help reduce the occurrence of re-injury and effectively reduce the recovery time.
Restatement of Key Findings
The systematic review identified insignificant differences in results between hydrotherapy and land therapy due to the lack of evidence from the constrained number of articles examined and reviewed. Further research and examination are essential to validate the effectiveness of aquatic therapy for the sake of development in rehabilitation systems, particularly aquatic therapy.
Connection to Objectives
Certain benefits, such as buoyancy and safety with hydrostatic pressure, are only available through aquatic treatment. However, the review’s conclusions show little difference between land-based and aquatic therapy. This is mainly because there aren’t enough studies and experiments to properly compare the two, which makes it harder to conclude.
Limitations
A lack of prior studies has resulted in an overall lack of awareness of the advantages and benefits of aquatic therapy and associated treatments. Moreover, included studies must meet RCT and English studies, which limits the magnitude of the articles included. Other than Osteoarthritis, musculoskeletal conditions such as Rheumatoid Arthritis, Osteoporosis, Fibromyalgia, and low Back Pain were excluded in this systematic research due to a lack of experimental data. Furthermore, these hindrances of therapeutic research could impact the future treatment in MSK-I, such as leading to permanent damage to the patients’ joint with no practical cure.
Although there is no significant difference between the two, the systematic results of hydrotherapy are marginally better than those on land. With the uniqueness of hydrotherapy, further research is needed to examine comparative studies with diverse populations and other treatments. It is, therefore, necessary to determine the depth of effectiveness of hydrotherapy. More investigation and experimental research are required to grasp its full potential and maximize its application for medicinal objectives
Implications and Significance
The results of this thorough literature analysis and methodical investigation highlight important gaps in our knowledge and treatment of musculoskeletal (MSK) disorders, especially in relation to the efficacy of hydrotherapy. A more focused strategy is required to optimize impact, even while the report emphasizes the necessity for increased research activities. Future studies should focus on exploring hydrotherapy’s role beyond osteoarthritis and evaluating its advantages for illnesses including rheumatoid arthritis, post-surgical rehabilitation, and chronic lower back pain, rather than making a broad demand for further studies. Furthermore, in order to fortify the body of data and create more precise therapeutic guidelines, more rigorous approaches—such as extensive randomized controlled trials (RCTs), long-term longitudinal studies, and comparative effectiveness research—are necessary.
Closing Thoughts & Recommendations
The lack of proper treatment of MSK conditions remains a challenging public health concern, affecting millions of patients with the conditions worldwide. Tieing back to the key founding of this research, the constant inssufficiency of research from the medical department highlights the need for a concerted global initiative aimed at raising awareness and conducting comprehensive studies on MSK disorders. Such effort will enhance the quality of research and increase the resources to have public access, overall fostering the benefits.
Methods
Despite the lack of knowledge of current MSK-I, the importance of studying aquatic therapy is to share and open up a potential possibility of physical therapy by providing a cost-effective methodology and workouts, which could improve pain management, mobility, and rehabilitation solutions for various patient populations.
Systematic reviews are a fundamental component of validated, evidence-based research. This is because they reduce bias and improve the reliability of results by following an open, systematic process. It provides a detailed overview of a specific research area based on high-quality commercial data. In addition, the systematic review ensures that the results are reliable for independent verification. Systematic reviews expand knowledge and practice by increasing the clarity and overall applicability of research findings.
Search Strategy & Inclusion Criteria & Quality Assessment
The systematic review focused on assessing participants’ levels of pain relief (PR), physical function (PF), and quality of life (QL). Moreover, the duration interval (DI) and the session length (SL) of the treatment on the participants were measured for further insights and the validity of data sets. Lastly, the PEDro score14. was scored out of 10 to assist readers in assessing whether a clinical trial presents reliable and meaningful results for use in clinical practice (Refer to Table 1 in the appendix).
The duration of the literature search was November 15, 2024 – December 07, 2024. The main research engine for public experiments was Google Scholar, and if paywalls blocked the article, we asked for a PDF file through email for permission. Then, a reviewer (T.P.) independently selected studies based on title and abstracts. Then, Y.K. chose studies with the following requirements:
Age Group
Studies were included to determine whether the experiments conducted were random controlled trials (RCTs), with participants > 18 years of age, to mitigate the variance adolescents’ underdeveloped bodies may cause. Moreover, participants had to be diagnosed with Osteoarthritis.
Experimental Group
The included studies comprised at least one control group (land-based therapy) and one experimental group (hydrotherapy) to actively compare treatments’ effectiveness in different environments. Studies of aquatic exercise focused on endurance, flexibility, strength, resistance, and aerobic exercise training are included. Other methods, such as spa therapy, were excluded due to their lack of scientific effectiveness and unusual consequences. Studies with explained data of mean, standard deviation, and sample size were selected to calculate standardized mean differences and confidence intervals. For a good-quality systemic research review, studies of low quality have been excluded based on the Physiotherapy Evidence Database (PEDro) scale (Under 5 out of 10).
Data Extraction
Due to the lack of recent studies, publication dates and research designs have been overlooked when considering extracted data points. In that way, we were able to hold reasonable numbers of data sets without excluding additional gathered studies.
The meta-analysis was conducted and measured using standardized mean differences (SMDs) and confidence intervals (CIs). This method helps compare data with different scales (Refer to Equations 1 and Equation 2 for further explanation).
Equations
(1) 
(2) 
The Cohen’s D formula, derived from a website named Social Science Statistics (2024), is expressed in the equations above. M stands for mean, and SD stands for standard deviation. Given samples from two normal populations of size n1 and n2 with sample means 𝜇1 and 𝜇2 known standard deviations 1 2, the test statistic compares the means15
(3) 
The confidence interval formula, as derived by Staff (2023), is expressed as the equation above. x means point estimate, an unknown variable to estimate the value to approximate the actual value. z stands for the z score, which is the number of standard errors to extend on either side of the point estimate. stands for standard deviation, and n stands for sample number. Based on a specified confidence level (95%), the confidence interval for a standardized mean difference (SMD) gives a range of values that the genuine effect size (population parameter) is likely to fall within16.
Synthesis Method
Thematically synthesized gathered data is a method suited for a systematic approach, as it involves identifying and analyzing data across multiple studies. Here are the following steps for implementing thematic synthesis.
Extracting Data
Begin by extracting data from multiple studies and labeling key information from the studies included in the review. Data extraction includes reading through the key findings from included articles, which guides interpretation with validated information.
Developing Descriptive Themes
After the extraction, the next step is to describe the data and gather them together to develop insights. In this study, visualizing data with different graphs allowed us to conclude with acumen. Such summarizing key ideas of descriptive themes allows superficial interpretation.
Generating Analytical Themes
This step moves beyond summarized data to interpretation and synthesis, generating new insights with answers to the research question. With the gathered summary, developing from descriptive themes creates overarching analytical themes, such as linking the conclusion to existing theoretical frameworks and highlighting relationships between themes to identify patterns that foster and improve the quality of the research findings.
Acknowledgements
I want to express my sincere gratitude to Hyeongbin Chu for his valuable guidance in designing the systematic approach and methodologies.
I want to extend my appreciation to Jenny Jung for her helpful proofreading, which has helped me improve this paper, and for her insightful ideas and recommendations for further improvement.
Last but not least, I would like to thank my co-authors, who supported me throughout the plotting of graphs, practical research, and data gathering.
Supplementary Visuals


Appendix A
| Table 1: Study Intervention | ||||||||
| Study | Age (year), Mean ± SD | Outcome Assessed | DI (week) | SL (# of sessions per week) | PEDro score (1-10) | Sample Size | ||
| PR | PF | QL | ||||||
| Belza 200220 | 68.60±5.40 | ✔ | ✔ | ✔ | 20 | 60mins *1-7 | 5 | 35 |
| Cochrane200521 | 69.86±6.82 | ✔ | ✔ | ✔ | 52 | 60mins*2 | 7 | 100 |
| Foley200322 | 73.00± 8.20 | ✔ | ✔ | ✔ | 6 | 30mins*3 | 7 | 35 |
| Fransen 200723 | 70.00±6.30 | ✔ | ✔ | ✔ | 12 | 60mins *2 | 8 | 41 |
| Hale 201224 | 73.60±1.50 | ✔ | ✔ | 12 | 60mins * 2 | 8 | 16 | |
| Hinnman 200625 | 63.30±9.50 | ✔ | ✔ | ✔ | 20 | 45-60min*2 | 8 | 50 |
| Lim 201026 | 65.70±8.90 | ✔ | ✔ | ✔ | 8 | 40min*3 | 7 | 25 |
| Patrick 200127 | 65.70±N/A | ✔ | ✔ | ✔ | 20 | 45-60min*2-7 | 6 | 25 |
| Stener-Victorin 200428 | 70.30±N/A | ✔ | ✔ | ✔ | 5 | 30min*2 | 5 | 45 |
| Wang 200729 | 66.70±5.60 | ✔ | ✔ | ✔ | 12 | 60min*3 | 7 | 38 |
| Wang 201130 | 69.30±13.30 | ✔ | ✔ | 12 | 60min*3 | 6 | 84 | |
| Lund 200831 | 65.00±12.60 | ✔ | ✔ | ✔ | 8 | 50min*2 | 6 | 27 |
| Wyatt 200132 | NR | ✔ | ✔ | 6 | N/A*3 | 6 | 45 | |
| Murugavel 202233 | 20.89±1.78 | ✔ | ✔ | 12 | 45mins *3 | 5 | 10 | |
| Slouma 202434 | 59.1±10.3 | ✔ | ✔ | ✔ | 8 | 60mins *3 | 5 | 30 |
| Table 2: Data Table | ||||
| Study | Condition | SMD | Aquatic Therapy | Land-Based Therapy |
| Belza 2002 20 | OA | -0.09 | -0.46 | 0.29 |
| Cochrane200521 | OA | -0.27 | -0.5 | -0.05 |
| Foley200322 | OA | 0 | -0.48 | 0.48 |
| Fransen 200723 | OA | -0.71 | -1.13 | -0.3 |
| Hale 2012 24 | OA | 0.21 | -0.46 | 0.88 |
| Hinnman 200625 | OA | -0.49 | -0.97 | -0.02 |
| Lim 201026 | OA | -0.71 | -1.32 | -0.1 |
| Patrick 200127 | OA | -0.12 | -0.39 | 0.15 |
| Stener-Victorin 200428 | OA | -1.75 | -2.95 | -0.54 |
| Wang 200729 | OA | -0.51 | -1.16 | 0.14 |
| Wang 201130 | OA | -0.22 | -0.3 | 0.63 |
| Lund 200831 | OA | -0.04 | -0.6 | 0.51 |
| Wyatt 200132 | OA | -0.86 | -1.49 | -0.22 |
| Murugavel 202233 | OA | -0.97 | -1.1 | 0.13 |
| Slouma 202434 | OA | 1.51 | -0.6 | 1.8 |
| Total (95% CI) | Combined | -0.29 | -0.96 | 0.26 |
References
- Department of Orthopedics. (2021). Psychosocial impacts of sports-related injuries in athletes. Current Sports Medicine Reports, 20(2), https://journals.lww.com/acsm-csmr/fulltext/2021/02000/Psychosocial_Impacts_of_Sports_related_Injuries_in.10.aspx [↩]
- National Center for Chronic Disease Prevention and Health Promotion. (n.d.). Epidemiology of musculoskeletal injuries among sedentary individuals. Medicine & Science in Sports & Exercise. https://journals.lww.com/acsm-msse/fulltext/2002/05000/epidemiology_of_musculoskeletal_injuries_among.17.aspx [↩]
- Wagemans, J., Bleakley, C., Taeymans, J., Schurz, A. P., Kuppens, K., Baur, H., & Vissers, D. (2022). PLOS ONE, 17(2). https://doi.org/10.1371/journal.pone.0262023 [↩]
- Sports Injuries: Types, Treatment and Prevention. (2024). Cleveland Clinic. Retrieved from https://my.clevelandclinic.org/health/diseases/22093-sports-injuries [↩]
- I., A. A. H. (n.d.). Use of prescription drugs in athletes. PubMed. Retrieved from https://pubmed.ncbi.nlm.nih.gov/18489193/ [↩]
- Gilbert, K. (2024). Key benefits of aquatic physical therapy. Benchmark Physical Therapy. Retrieved from https://www.benchmarkpt.com/blog/key-benefits-of-aquatic-physical-therapy/ [↩]
- Kamioka, H., Tsutani, K., Okuizumi, H., Mutoh, Y., Ohta, M., Handa, S., … Honda, T. (n.d.). Effectiveness of aquatic exercise and balneotherapy: A summary of systematic reviews based on randomized controlled trials of water immersion therapies. PubMed Central. Retrieved from https://pmc.ncbi.nlm.nih.gov/articles/PMC3900774/ [↩]
- Carayannopoulos, A. G., Han, A., & Burdenko, I. N. (2020). The benefits of combining water and land-based therapy. PubMed Central. Retrieved from https://pmc.ncbi.nlm.nih.gov/articles/PMC7056478/ [↩]
- Staff, S. (2024). The benefits of aquatic therapy for rehabilitation. SCSR Therapy. Retrieved from https://scsrtherapy.net/the-benefits-of-aquatic-therapy-for-rehabilitation/ [↩]
- Osteoarthritis. (n.d.). Mayo Clinic. Retrieved from https://www.mayoclinic.org/diseases-conditions/osteoarthritis/symptoms-causes/syc-20351925 [↩]
- Department of Orthopedics. (2021). Psychosocial impacts of sports-related injuries in athletes. Current Sports Medicine Reports, 20(2), https://journals.lww.com/acsm-csmr/fulltext/2021/02000/Psychosocial_Impacts_of_Sports_related_Injuries_in.10.aspx [↩]
- Young, S., & Collins, T. (2022). The benefits of combining water and land-based therapy. International Journal of Therapy and Rehabilitation, 29(9), 1–12. https://doi.org/10.12968/ijtr.2021.0083 [↩]
- Sabesan, V. J., Schrotenboer, A., Habeck, J., Lombardo, D., Stine, S., Jildeh, T. R., & Meiyappan, A. (2018). Musculoskeletal education in medical schools: A survey of allopathic and osteopathic medical students. PubMed Central. Retrieved from https://pmc.ncbi.nlm.nih.gov/articles/PMC6132304/ [↩]
- PEDro scale. (2020). PEDro. Retrieved from https://pedro.org.au/english/resources/pedro-scale/ [↩]
- Effect size calculator for T-test. (n.d.). Social Science Statistics. Retrieved from https://www.socscistatistics.com/effectsize/default3.aspx [↩]
- Staff, I. (2023). Guide to calculating confidence intervals. IntelliSurvey. Retrieved from https://blog.intellisurvey.com/guide-to-calculating-confidence-intervals/ [↩]



{kind=link}