
Abstract
This study investigated the relationship between social-emotional learning (SEL) constructs and explored preliminary mental health outcomes following a social-emotional learning (SEL) intervention in elementary students through the Cognitive-Behavioral Framework. Using a two-wave design, the study examined elementary school students through baseline assessment (Wave 1, N = 31, ages = 7-12) and single-group pre-post analysis (Wave 2, N = 6, ages = 7-9) due to inability to collect control group data. The majority of participants were Asian, with the remainder representing mixed-race, White, and other ethnic backgrounds. The research examined relationships between emotional regulation, internalizing problems, and self-esteem utilizing the Strengths and Difficulties Questionnaire (SDQ) for internalizing problems, Panorama Education’s Emotional Regulation Assessment, and the modified Rosenberg Self-Esteem Scale, while considering cultural and developmental contexts. Baseline analyses revealed an unexpected negative relationship between emotional regulation and self-esteem (β = -0.29, p = 0.08), contrary to hypotheses. Internalizing problems showed minimal association with self-esteem. The intervention phase showed modest improvements, though changes were not statistically significant given the small sample size. Due to recruitment challenges, Wave 2 analyses were limited to pre-post comparisons without a control group. Findings suggest complex relationships between social-emotional constructs in elementary students and highlight the importance of cultural considerations and adequate sample sizes in SEL intervention research. Results provide preliminary insights for future controlled studies examining social-emotional learning effectiveness across diverse populations.
Keywords: social-emotional learning, mental health, elementary students, Cognitive-Behavioral Framework, intervention effectiveness, cultural adaptation
Introduction
One in five children aged 3-17 years experiences a mental health disorder, yet only 50% of those needing services receive them1,2. The COVID-19 pandemic intensified this crisis, with youth depression and anxiety symptoms doubling and emergency department visits for mental health concerns increasing by 24% for children ages 5-11 and 31% for adolescents ages 12-173. These alarming statistics underscore the urgent need for effective, accessible mental health interventions in schools.
Mental health challenges disproportionately affect marginalized communities. For example, Black and Hispanic children are significantly less likely to receive mental health care compared to their White peers, with only 42% of Black children and 36% of Hispanic children with mental health conditions receiving treatment, compared to 53% of White children4. In contrast, Asian youth appear to face even greater disparities, with just 4.4% of Asian children reported to partake in recent mental health treatment in 2023, compared to 12.5% of African Americans, 10.3% of Hispanic, and 18.3% of White children. Only 3.1% had received counseling or therapy and merely 2.3% had taken medication5. These figures highlight that Asian youth are among the least likely to access mental health services in the US. Additionally, children from low-income families face substantial barriers, with those from low-income households being four times more likely to experience mental health problems than children from higher-income families6.
Schools serve as primary mental health providers, with 58% of youth receiving services in educational settings7. However, significant gaps persist: while 55% of U.S. public schools screen for mental health issues, only 42% provide treatment services8. The most common barriers include insufficient mental health staff coverage (55%), inadequate funding (54%), and poor access to licensed professionals (49%)9. Due to these inabilities by the majority (58%) of US public schools, only Washington D.C. and Idaho meet the nationally recommended ratio of school psychologists per 500 students, in contrast to states such as West Virginia, Missouri, Texas, Alaska, and Georgia which have ratios exceeding one psychologist per 4,000 students, indicating significant disparities in access to mental health professionals, perhaps contributing to issues with funding and coverage10. Given these substantial barriers to traditional mental health services, schools are increasingly turning to evidence-based prevention programs that can be delivered by educational staff to reach larger numbers of students.
Socio-Emotional Learning as an Evidence-Based Intervention
Social-Emotional Learning (SEL) has become a central focus in educational research and practice due to its role in promoting students’ self-awareness, emotional regulation, interpersonal skills, and academic success11,12. A growing amount of research supports the value of universal, school-based SEL interventions, as meta-analyses have shown that school-based SEL programs can improve social-emotional capabilities, prosocial behaviors, and academic performance while reducing internalizing problems13. Elementary school children (ages 7-12) represent a particularly critical target for SEL interventions. During this developmental stage, children develop foundational emotional regulation skills and coping strategies that persist into adolescence and adulthood14. Research indicates that early intervention during elementary years is particularly effective, with effect sizes ranging from 0.3 to 0.7 for various mental health outcomes15.
Despite this promise, gaps remain in that many SEL interventions have lacked strong foundations, are inconsistently implemented, or lack rigorous examination, especially in areas outside of the US16,17. Additionally, there have been few studies that have adequately investigated how student characteristics, such as gender and behavior, moderate outcomes. Existing research on the previous topics is often mixed and yields contradictory results18,19. To understand the mechanisms through which SEL interventions may influence children’s emotional development, this study draws upon the Cognitive-Behavioral Framework, which provides a clear theoretical foundation for examining how thoughts, emotions, and behaviors interact to influence mental health outcomes.
Theoretical Framework: Cognitive-Behavioral Framework
This study is grounded in the Cognitive-Behavioral Framework (CBF), which emphasizes how thoughts, emotions, and behaviors interact to influence mental health outcomes20,21. CBF suggests that children’s emotional regulation, self-esteem, and coping skills develop through the interconnection between cognitive processes and behavioral responses, which can be modified through targeted interventions22. This framework is particularly relevant for understanding how school-based social-emotional learning interventions might impact students’ mental health outcomes by providing them with strategies to recognize and modify maladaptive thought patterns and develop healthier emotional responses23.
The CBF provides a clear mechanism for how SEL interventions can improve student well-being, as it focuses on teaching specific skills to identify certain emotional states, challenge negative thought patterns, and practice adaptive coping behaviors24. Additionally, CBF accommodates cultural variations in emotional expression and regulation, which helps to explain why intervention effectiveness might vary across different student populations25. Although CBF has shown effectiveness in addressing these variations such as anxiety and depression in children26, few studies have examined its impact on self-esteem, especially in group contexts within schools. Within the CBF framework, self-esteem represents a critical cognitive-emotional construct that both influences and is influenced by children’s thought patterns and behavioral responses to emotional situations.
Self-Esteem and Emotional Development in Children
Self-esteem has long been recognized as a crucial factor in children’s emotional development and psychological resilience. High self-esteem in childhood is often correlated with positive outcomes such as increased happiness, social confidence, academic engagement, and emotional stability27,28, while low self-esteem is associated with a diverse number of mental health difficulties including depression, anxiety, suicidal ideation, and behavioral problems29,30. The developmental period of childhood and early adolescence involves heightened sensitivity to peer perception and social belonging31, making this phase a critical time for interventions aimed at strengthening self-esteem. Schools, specifically, have become targets for mental health interventions due to their accessibility and potential for widespread impact32, and many focus on anxiety reduction as well as emotional regulation.
Research has demonstrated that self-esteem can be effectively targeted through structured interventions. Studies implementing Cognitive-Behavioral Group Therapy protocols in school settings have shown significant improvements in children’s self-esteem independent of their perceived working relationships with their facilitators, suggesting that structured approaches can work effectively even without strong therapeutic bonds33. The development of self-esteem and emotional regulation skills within a CBF framework does not occur in isolation but is significantly influenced by the family and cultural contexts in which children’s cognitive schemas are formed.
Family and Cultural Influences on Emotional Regulation
Self-concept, developed by cognitive and social factors/interactions, plays a key role in one’s mental well-being and interpersonal behavior34,35, especially in mothers, who significantly influence the development of their child’s self-perception36. Contrastingly, poor self-concept has been consistently linked to negative psychological outcomes such as anxiety, depression, and dysfunctional behaviors36, suggesting its importance in mental health and family dynamics.
Emotional regulation is not viewed solely as a personal capability but also acts as a communication facilitator, particularly in parenting and familial interactions37, with many studies showing that mothers with proficient emotional regulation skills are better equipped to foster emotional security and foster effective communication within their respective households37, given that good cognitive regulation strategies are taken as well.
Cultural factors also play a significant role in how children develop emotional regulation strategies and respond to interventions. Different cultural approaches to emotional expressions, parenting styles, and help-seeking behaviors can influence both baseline emotional functioning and responsiveness to CBF-based interventions. For example, varying parenting styles, from more Western-oriented styles emphasizing autonomy to traditional authoritarian approaches with increased structure and discipline, may foster different cognitive frameworks in children, ultimately contributing to how they process emotional experiences and coping strategies38,39.
While research has emphasized the role of family functioning in reducing the level of stress and emotional dysregulation in children36,40, studies specifically examining mother-child relationships during elementary years remain limited. This developmental period is particularly important as it involves significant transitions for both children and families. Research suggests that maternal emotional regulation and self-concept work together to influence family functioning, with mothers who have better emotional regulation skills more likely to maintain positive self-concepts, which in turn supports healthier family dynamics during critical developmental phases37. Building on the Cognitive-Behavioral Framework and recognizing the importance of cultural and family influences in shaping children’s cognitive-emotional development, this study investigated how SEL interventions influence elementary students’ emotional regulation, internalizing problems, and self-esteem across diverse populations.
Current Study
Despite the promise of SEL programs, few studies directly compare their effectiveness across diverse populations or examine the mechanisms through which they operate. Drawing on the Cognitive Behavioral Framework20, this study investigated the impact of a social-emotional learning intervention on elementary students’ mental health and coping strategies. The present study addresses this gap by investigating the impact of a structured social-emotional learning intervention on elementary students’ (ages 7-12) emotional regulation, internalizing problems, and self-esteem.
Previous research has identified significant gaps in understanding intervention effectiveness across diverse populations41, and the need for more comparative studies of school-based mental health programs42. Additionally, while studies have demonstrated the potential benefits of various interventions such as CBITS and PATHS43,44, few have directly compared intervention effectiveness while considering the complex interplay between individual development, cultural background, and institutional support systems.
The present study employed a two-wave design examining baseline relationships (Wave 1) and intervention effects (Wave 2) which received weekly social-emotional learning sessions. Based on CBF principles and previous research, the study hypothesized that:
H1: Students with higher emotional regulation will predict higher self-esteem at baseline.
H2: Students with higher internalizing problems will predict lower self-esteem at baseline.
H3: Students in the intervention group will show lower levels of internalizing problems compared to the control group.
H4: Students in the intervention group will demonstrate more effective coping strategies, particularly in problem-focused and emotion-focused coping, compared to the control group.
Method
Participants
This study employed a quasi-experimental design with two groups. Wave 1 involved baseline assessment where participants completed assessments of emotional regulation, internalizing problems, and self-esteem. In Wave 2, participants completed five identical assessments after receiving weekly social-emotional learning (SEL) lessons.
This study included 37 participants across two waves: Wave 1 (N=31) for baseline analysis and Wave 2 (N=6) for intervention analysis. Wave 1 sample consisted of 31 participants ranging in age from 7 to 12 years (M = 9.37, SD = 1.24). The majority of participants were between 8 and 11 years old, with 28.1% being 10 years old, 25.0% being 9 years old, and 18.8% being 8 years old. The gender distribution showed a slightly higher proportion of females (58.1%, n = 18) compared to males (41.9%, n = 13).
In terms of racial/ethnic composition, Asian participants (including those identifying as Asian, Korean, Korean-American, Bengali, and Taiwanese) comprised the largest group (51.6%, n = 16). Mixed-race participants (including Indian-European, Korean-Polish American, Mixed Asian and Ecuadorian, and Multiracial) represented 12.9% (n = 4) of the sample. White participants (including White and White/Non-Hispanic) comprised 9.7% (n = 3) of the sample. The remaining participants identified as Hispanic and Middle Eastern, with each category representing 3.2% (n = 1).
The second wave of participants included 6 elementary school students (Mage = 7.33, SD = 0.82, range =7- 9 years). Half of the participants identified as male and the other half as female. All of the study participants identified as Asian-American and resided in Bergen County New Jersey (see Table 1).
| Characteristics | Wave 1 (n= 31) | Wave 2 (n= 6) |
| Age | ||
| Mean (SD) | 9.37 (1.24) | 7.33 (0.82) |
| Gender | ||
| Female | 58.06% (n= 18) | 50% (n=3) |
| Male | 41.93% (n=13) | 50% (n=3) |
| Race | ||
| Asian | 51.61% (n=16) | 100% (n=6) |
| Mixed-race | 12.90% (n=4) | |
| White | 9.68% (n=3) | |
| Other | 25.80% (n=8) |
Procedure
Participants were recruited through email and word of mouth, to parents, teachers, members in the local community and in other states. Participants who met the following criteria were eligible for the study: (1) identified as elementary school students, 2) who were between 7-12 years old. Participants completed an online 10-minute Google Forms survey which consisted of self-report measures (Wave 1). Parents were encouraged to assist their children in completing the survey. Survey questions to measure internalizing symptoms were age-normed for three different age groups: early childhood (2-5 years), middle childhood (6-10 years), and adolescents (11-18 years). Utilizing age-specific norms and items enhances the accuracy in screening for problems across the emotional and behavioral domains (e.g., Strength and Difficulties Questionnaire; SDQ45) as the scale measures within appropriate developmental groups.
The intervention itself was a social-emotional curriculum in which lessons on emotional regulation were conducted over three weeks in a summer classroom environment approved by a local educational non-profit organization in which a trained facilitator delivered the intervention, with oversight from a head teacher and assistance from other trained volunteers. Training and lesson plans were based on “Merrell’s Strong Start—Grades K–2: A Social and Emotional Learning Curriculum”46 which aims to help students build awareness of their emotions and the emotions of others, and manage emotions in healthy ways. The curriculum involved learning to be more empathetic towards others, such as understanding other people’s feelings in addition to their own, how to deal with worry, anger, happiness, sadness, and also being a good friend. Lessons were held twice a week for one hour and structured so that they started with mindfulness or gratitude activities, introduction to different types of breathing exercises, and activities to promote kindness, self-esteem and inclusivity. The core of each lesson centered on an overview of one of the emotions, interactive activities and worksheets that reinforced the students’ understanding of the emotion, and coping exercises related to the emotion. Lessons usually concluded with students completing a journal entry or drawing about their feelings. The first sessions also included icebreakers in order to build more comfort between the students and the facilitator, in order to allow for more responsiveness and engagement in future lessons. The lessons were designed to target the measured outcomes of this study by delivering the social-emotional content through these activities promoting self-esteem, increasing awareness of emotions, coping exercises and self-reflection exercises.
For Wave 1, all eligible participants who completed consent procedures were included in the baseline assessment. For Wave 2 (intervention component), participants were initially planned to be assigned to intervention or control conditions based on classroom assignments at their elementary program. However, due to recruitment challenges and participant attrition, sufficient control group data was not obtained. Therefore, Wave 2 analyses are limited to the intervention group participants only (N=6). Consequently, this study functions as a pre-post intervention analysis rather than a controlled comparison study. This was based on SEL curriculum based on “Merrell’s Strong Start—Grades K-2: A Social & Emotional Learning Curriculum, Second Edition”46, aligned with CASEL’s five social and emotional competency areas.
Random assignment at the individual level was not feasible within the existing educational structure, as school administrators preferred to implement the intervention at the classroom level to minimize disruption to the school schedule.
Measures
Strength and Difficulties Questionnaire. Children’s socio-emotional difficulties were measured using the Strength and Difficulties Questionnaire (SDQ47. The SDQ is age-normed as follows: 2-5 years, 6-10 years, and 11-18 years. Parents were provided with the survey based on their child’s age. Each age-normed scale comprised four subscales that measured emotional symptoms, peer relationship difficulties, hyperactivity, and conduct problems. Items were reported on a 3-point scale, 0 (Not true) to 2 (Certainly true), with higher scores indicating greater problems in each domain. Analysis of variance (ANOVA) was conducted to examine differences in self-esteem across age groups (7-8 years, 9-10 years, and 11-12 years). Results revealed no significant differences in self-esteem across these age groups, F(3, 28) = 1.192, p = .331; therefore, subscales across age groups were combined. Subscales for emotional symptoms and peer relationship difficulties were combined as internalizing difficulties, and subscales for conduct problems and hyperactivity were grouped as externalizing difficulties45. For the current study, emotional symptoms and peer relationship problems were used to assess internalizing symptoms among participants.
Emotional Regulation Assessment- Panorama Education. Children’s ability to control their emotions was measured using the Emotional Regulation Assessment48. This assessment targets elementary school students. This assessment, was a subset of the entire “Panorama SEL Survey,” measuring grit based on certain situation-based questions. Items were reported on a 5-point scale, 0 (Never) to 5 (A lot), with the higher scores suggesting an improved emotional restraint for each domain. Analysis of variance (ANOVA) was conducted to examine differences in emotion regulation across age groups (7-8 years, 9-10 years, and 11-12 years). Results revealed no significant differences in emotion regulation across these age groups, F(3, 28) = 0.611, p = .614; the subscales were more or less the same, with a combination of internalizing and externalizing difficulties, as the questions tested the emotional regulation of children in reaction to an external situation.
Rosenberg’s Self-Esteem Scale. Children’s difficulties in dealing with self-dignity and self-loathing were measured using Rosenberg’s Self-Esteem Scale (RSES49. While the RSES was originally developed for adolescents and adults, research has demonstrated that age-appropriate modifications can make it suitable for younger populations. For example, Wood and colleagues50 found that simplified language adaptations of the RSES showed acceptable psychometric properties when used with children as young as 8 years old. Following these established approaches, we simplified the language of RSES items to make them developmentally appropriate for the elementary school participants. The survey consisted of one general subscale that measured how the child thought of themselves. Items were reported on a 4-point scale, 0 (Strongly Agree) to 4 (Strongly Disagree), with higher scores indicating more problems in each domain. As this scale was measuring self-esteem, it was combined as measuring internal difficulties, based on self-assessing themselves on either past experiences or how they view themselves as individuals.
Data Analysis
Data were analyzed using R (version 4.13). Analyses were conducted separately for Wave 1 (N=31, cross-sectional baseline data) and Wave 2 (N=6, longitudinal intervention data) to address different aspects of our research questions.
Wave 1 Analysis. To test the first two hypotheses regarding baseline relationships between emotional regulation, internalizing problems, and self-esteem, we conducted two multiple regression analyses:
Model 1 (Emotional regulation predicting self-esteem):
![\[SE = \beta_{0} + \beta_{1}(\text{ER}) + \beta_{2}(\text{Age}) + \beta_{3}(\text{Race}) + \varepsilon\]](https://nhsjs.com/wp-content/ql-cache/quicklatex.com-8e23aee84ec91f292a6dbb31b1ed7739_l3.png "Rendered by QuickLaTeX.com")
Model 2 (Internalizing problems predicting self-esteem):
![\[SE = \beta_{0} + \beta_{1}(\text{SDQ}) + \beta_{2}(\text{Age}) + \beta_{3}(\text{Race}) + \varepsilon\]](https://nhsjs.com/wp-content/ql-cache/quicklatex.com-abcf9a1226c44cf0a182e4e1944d68ef_l3.png "Rendered by QuickLaTeX.com")
Where SE represents self-esteem scores, ER represents emotional regulation scores, SDQ represents internalizing problems scores, and ε represents the error term. Race was included as a categorical variable, with Asian participants serving as the reference group. We reported both unstandardized and standardized regression coefficients, p-values, and effect sizes (R² and adjusted R²) for each model. Before testing these models, preliminary analyses examined whether emotional regulation and self-esteem varied by age groups (7-8 years, 9-10 years, 11-12 years) using one-way ANOVA. These analyses verified that our measures functioned similarly across the age range of the sample, supporting the use of combined analyses rather than age-stratified approaches. However, we acknowledge that these non-significant findings are likely influenced by the low statistical power resulting from our small sample size rather than representing true measurement equivalence across age groups. With only 31 participants distributed across multiple age categories, our ANOVAs had limited ability to detect potentially important age differences in how these measures function. This statistical limitation should be considered when interpreting our combined analyses across age groups.
Wave 2 Analysis. It is critical to note that while the original study design included both intervention and control groups, it wasn’t possible to collect adequate control group data during Wave 2 due to recruitment difficulties and participant attrition. Consequently, all Wave 2 analyses examine changes within the intervention group only, without comparison to a control condition. This fundamental limitation means that any observed changes cannot be attributed to the intervention itself, as they may reflect natural developmental processes, regression to the mean, or other confounding factors. These methodological limitations, combined with the small sample size, mean that observed changes cannot be definitively attributed to the intervention. The following results should therefore be interpreted as preliminary, exploratory observations rather than evidence of intervention effectiveness.
For Wave 2 (N=6), several complementary analytical approaches were employed to examine potential intervention effects despite the limited sample size. It should be acknowledged that the small sample substantially limits statistical power and necessitates interpreting these results as exploratory rather than confirmatory. First, we conducted paired samples t-tests to compare Time 1 (baseline) and Time 5 (post-intervention) scores for each outcome measure (emotional regulation, internalizing problems, and self-esteem). Effect sizes were calculated using Cohen’s d for paired samples. Second, change scores for each measure were calculated by subtracting Time 1 scores from Time 5 scores. These change scores allowed us to examine the magnitude and direction of changes following the intervention. Means, standard deviations, and ranges for each change score are reported to characterize the variability in participants’ responses to the intervention. Third, a multiple regression analysis was conducted to examine whether changes in emotional regulation and internalizing problems predicted changes in self-esteem:
![\[SE_{\text{change}} = \beta_{0} + \beta_{1}(\text{SDQ}<em>{\text{change}}) + \beta</em>{2}(\text{ER}_{\text{change}}) + \varepsilon\]](https://nhsjs.com/wp-content/ql-cache/quicklatex.com-b6ac860af8836ee6f15a4006f05a0b12_l3.png "Rendered by QuickLaTeX.com")
Finally, linear mixed-effects models (growth curve analyses) were utilized to examine trajectories of change across all five-time points for each outcome measure. The models were specified as:

Where:
- ER_ij, SDQ_ij, and SE_ij represent emotional regulation, internalizing problems, and self-esteem scores for participant i at time j
- β₀ represents the fixed intercept
- β₁ represents the fixed effect of time (intervention effect)
- β₂ represents the fixed effect of age
- β₃ represents the fixed effect of ethnicity
- u₀i represents the random intercept for participant i (allowing for individual differences in baseline levels)
- ε_ij represents the residual error
Fixed effects for time, age, and ethnicity were included to examine their impacts on trajectories of change. Random intercepts were included to account for individual differences in baseline levels of each outcome. Initially, models were tested with random slopes but simplified to random intercepts only due to the limited sample size and model convergence issues. For each model, fixed effects estimates are reported with standard errors and t-values, as well as estimates of between-participant variance (random effects). Despite the small sample size for Wave 2 (N=6), these analyses may provide preliminary insights into potential intervention effects and generate hypotheses for future research. It should be acknowledged that the substantial statistical limitations of these analyses emphasize their exploratory rather than confirmatory nature. By examining these preliminary data with multiple analytical approaches (t-tests, change scores, regression, and growth curve modeling), the study aimed to identify patterns that may warrant investigation in future, larger-scale studies, while being transparent about the statistical constraints.
Results
Wave 1
Analysis of variance (ANOVA) was conducted to examine differences in self-esteem across age groups (7-8 years, 9-10 years, 11-12 years). Results revealed no statistically significant differences in self-esteem across these age groups, F (2, 28) = 1.71, p = 0.20, η² = 0.11 [95% CI: 0.00, 0.27]. Similar non-significant findings were observed for emotion regulation across age groups, F (2, 28) = 0.61, p = 0.614, η² = .04 [95% CI: 0.00, 0.18]. However, these non-significant results should not be interpreted as evidence of true equivalence, as our small sample size substantially limited statistical power to detect potentially meaningful age differences. The decision to combine age groups for analysis was primarily pragmatic given sample size constraints, and this limitation should be considered when interpreting results. Both regression models explained limited variance in self-esteem.
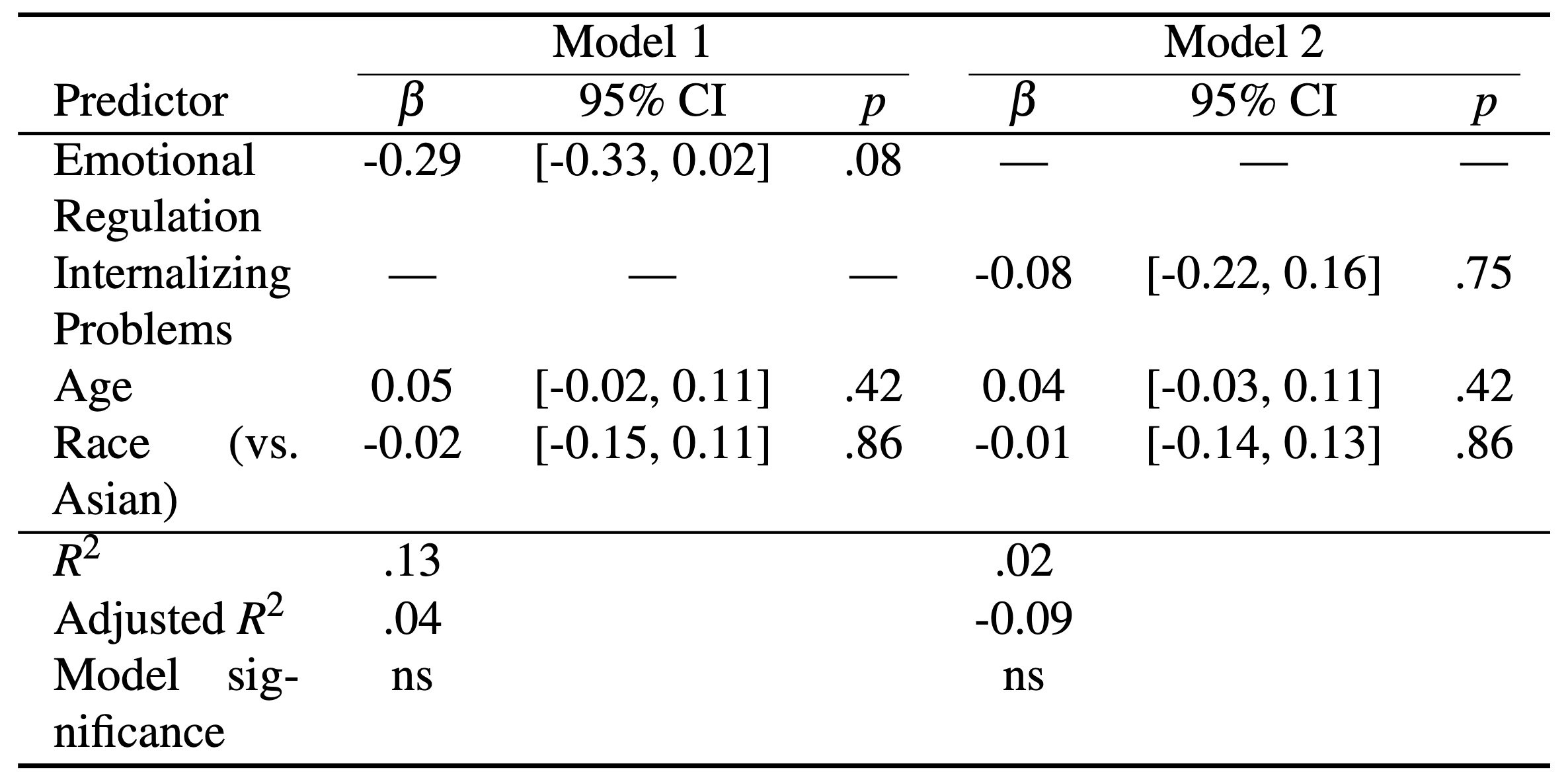
Table 2 Multiple Regression Analysis Predicting Self-Esteem at Baseline (Wave 1, N=31)
Note: β = standardized regression coefficient; CI = confidence interval; ns = not significant (p > .05); — = not included in model
The first model explained only 13.1% of the variance (Adjusted R² = 0.04) and was not statistically significant. Emotional regulation showed a marginally significant negative relationship with self-esteem (β = -0.29, 95% CI [-0.33, 0.02]), suggesting a potential negative association though the confidence interval slightly crossed zero. Age demonstrated a slight positive relationship (95% CI [-0.02, 0.11]), while race showed a minimal effect (95% CI [-0.15, 0.11]).
The second model (internalizing problems, age, and race as predictors) explained even less variance at 1.9% (Adjusted R² = -0.09) and was also not significant. Internalizing problems showed a small negative relationship with self-esteem (95% CI [-0.22, 0.16]), with the confidence interval centered near zero and crossing the null value. Age showed a similar pattern to Model 1 (95% CI [-0.03, 0.11]), and race again demonstrated a minimal effect (95% CI [-0.14, 0.13]). These low R² values and wide confidence intervals indicate that the selected predictors did not adequately capture the factors influencing self-esteem in our sample, suggesting that other unmeasured variables likely play more important roles in determining children’s self-esteem development. Age demonstrated a slight positive relationship, while race showed a minimal effect.
Both models revealed significant intercepts, indicating stable baseline self-esteem levels independent of predictor variables. Residual analyses suggested moderate model fit, with residuals ranging from -0.38 to 0.51 for Model 1 and -0.34 to 0.62 for Model 2. These findings suggest that while emotional regulation may have a modest influence on self-esteem, the selected predictors generally did not explain substantial variation in baseline self-esteem levels among participants. In terms of potential ethnic/racial differences, our exploratory analysis indicated that participants who identified as White/Non-Hispanic (β = -0.49, p = 0.05) showed lower self-esteem scores compared to the reference Asian group. However, this finding should be interpreted with extreme caution given the small overall sample size, the limited number of White/Non-Hispanic participants (n = 3), and the skewed distribution heavily favoring Asian participants (51.6%). These substantial methodological limitations prevent drawing reliable conclusions about true ethnic differences in self-esteem, and this observation is presented merely as a potential pattern that would require verification in larger, more balanced samples.
Wave 2
The following analyses of intervention effects (Wave 2, N=6) should be interpreted as exploratory and hypothesis-generating rather than confirmatory, given the very limited sample size. Without a control group, findings of the study cannot be used to determine whether observed changes are due to the intervention or other factors such as natural development, measurement effects, or environmental influences. The statistical power to detect significant effects is severely constrained, and findings should be viewed as generating hypotheses for future research rather than providing reliable evidence of intervention effectiveness. These preliminary findings provide initial insights into potential patterns of change that warrant investigation in future, larger-scale studies.
Initial Changes in Outcomes
To examine changes in participants’ outcomes following the intervention, paired samples t-tests were conducted to compare Time 1 (baseline) and Time 5 (post-intervention) scores. For self-esteem, the analysis revealed no significant change from baseline to post-intervention (M difference = 0.125, t(3) = 0.70, p = 0.53, 95% CI [-0.45, 0.70]). Similarly, internalizing problems showed a non-significant trend toward improvement (M difference = 0.30, t(3) = 1.44, p = 0.25, 95% CI [-0.36, 0.96]), and emotional regulation demonstrated no significant change (M difference = 0.40, t(3) = 0.91, p = 0.43, 95% CI [-1.00, 1.80]). Despite the lack of statistical significance, the moderate effect sizes suggest potential intervention effects that might be detected with adequate statistical power (see Table 3).
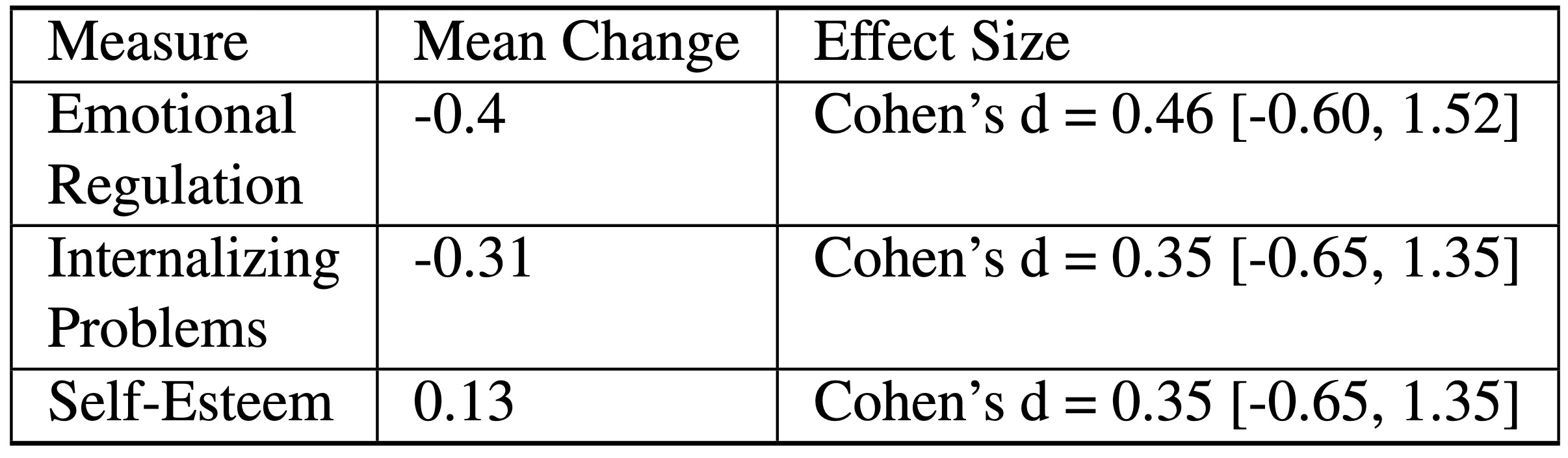
Table 3. Intervention Effects (Wave 2, N=6)
Magnitude of Changes
Examination of change scores from Time 1 to Time 5 revealed modest changes across all measures. Self-esteem showed the smallest mean decrease (-0.13, range: -0.60 to 0.20), followed by strengths and difficulties (-0.31, range: -1.05 to 0.15), and emotion regulation (-0.40, range: -1.40 to 0.60). Two participants had missing data points across all measures. The consistent negative direction of change, albeit small in magnitude, suggests a slight downward trend in participants’ reported outcomes over the study period.
Predictive Relationships
Multiple regression analysis examining whether changes in internalizing problems and emotional regulation predicted changes in self-esteem revealed a strong overall model fit (R² = 0.95, Adjusted R² = 0.85), which should be interpreted with extreme caution due to the minimal sample size and limited degrees of freedom (F(2,1) = 9.29, p = 0.23). With only one residual degree of freedom, this R² value likely represents a substantial overestimate of the true relationship strength. While this strong effect size is notable, it should be interpreted cautiously given the very limited degrees of freedom. Changes in internalizing problems (β = 0.66, p = 0.193) and emotional regulation (β = 0.37, p = 0.16) both showed positive associations with changes in self-esteem, suggesting that improvements in these areas were associated with improvements in self-esteem, though these relationships did not reach statistical significance.
Trajectories of Change Over Time
Growth curve analyses were conducted to examine changes in emotional regulation, internalizing problems, and self-esteem over the intervention period (N = 6, observations = 26). These analyses should be viewed as providing preliminary insights into potential trajectories rather than definitive evidence of intervention effects.
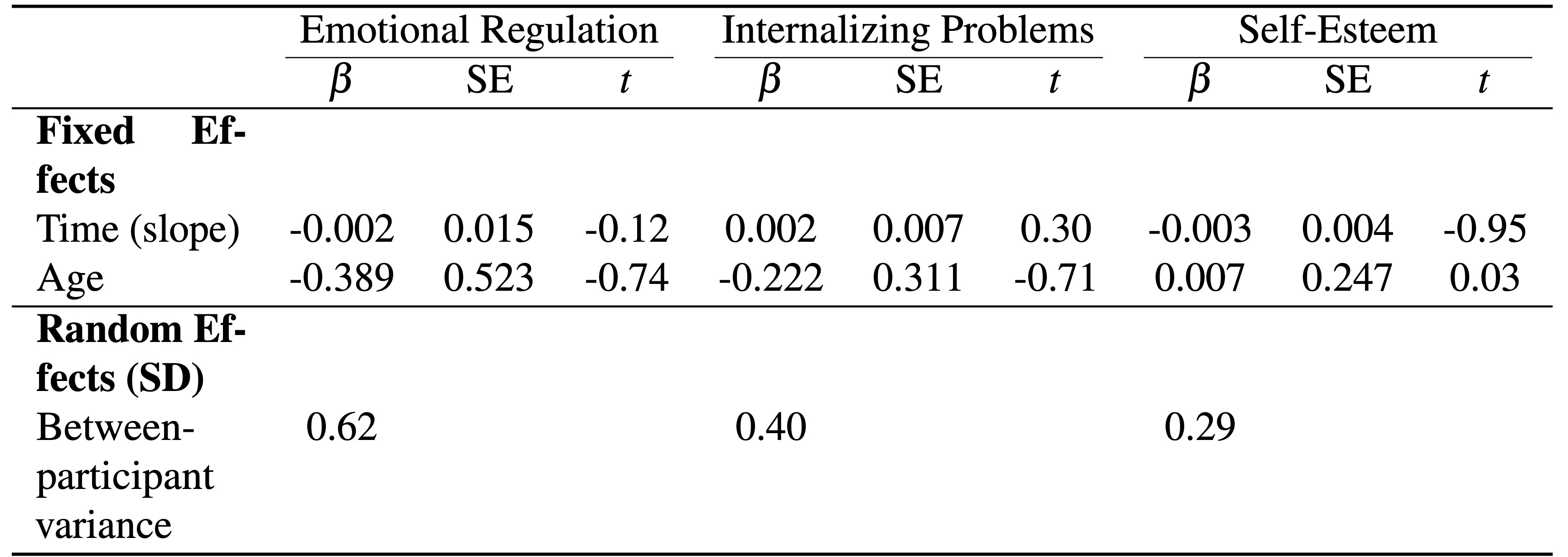
Table 4. Linear Mixed Effects Models for Outcome Trajectories (Wave 2, N=6)
Note: † p < .10; All other effects ns (not significant)
The models showed varying between-participant variance, with emotional regulation highest (SD = 0.62), internalizing problems moderate (SD = 0.40), and self-esteem lowest (SD = 0.29). No significant effects of time or age were found across measures, though internalizing problems showed a small trending improvement over time. When ethnicity was included as a covariate in exploratory analyses, it showed a significant positive association with self-esteem (β = 0.65, t = 2.00) and a marginally positive effect on internalizing problems (β = 0.75, t = 1.79), though no significant effects were found for emotional regulation. These ethnicity effects suggest potential cultural differences in intervention responsiveness that warrant investigation in future studies with larger, more diverse samples.
Figure 1 illustrates the individual trajectories of emotional regulation across the five assessment points, demonstrating the stability of this construct throughout the intervention period.

As shown in Figure 1, emotional regulation remained relatively stable throughout the intervention period (β = -0.002, t = -0.12, p > 0.05), with individual participants showing varied response patterns but no overall group improvement. The wide confidence intervals reflect both the small sample size and substantial individual differences in baseline levels and intervention responsiveness.
Collectively, these preliminary exploratory analyses suggest several potential patterns that warrant investigation in future research with larger samples: (1) modest decreases in internalizing problems over the intervention period, (2) strong interconnections between changes in emotional regulation, internalizing problems, and self-esteem, and (3) notable individual differences in intervention responsiveness. However, the limited sample size substantially restricts the statistical power and generalizability of these findings. Future research should examine these patterns with adequately powered designs to determine their reliability and clinical significance. For internalizing problems, there was a trending decrease over time (β = -0.08, SE = 0.04, t = -1.92), suggesting potential improvement, though this change did not reach statistical significance (see Figure 2).

Figure 2 demonstrates the most encouraging pattern among the three outcomes, with internalizing problems showing a consistent downward trajectory across the intervention period. Despite the lack of statistical significance due to the limited sample size, the effect size was moderate-to-large (Cohen’s d = 0.72), suggesting meaningful clinical improvement. Individual trajectories reveal that 4 out of 6 participants experienced reductions in internalizing problems, with the steepest improvements occurring during the middle weeks of the intervention. This pattern aligns with previous research indicating that SEL interventions are particularly effective for reducing anxiety and depressive symptoms in elementary students.
Figure 3 illustrates the self-esteem scores during SEL intervention over five-time points. Self-esteem scores showed minimal change over time (β = -0.03, SE = 0.03, t = -1.04), with participants maintaining relatively stable levels around the initial average of 2.93. The random effects indicated more variation between participants than within participants across all three measures, suggesting consistent individual differences throughout the intervention period.

The stability shown in Figure 3 indicates that self-esteem was largely unresponsive to the brief intervention period. This relatively flat trajectory reflects the inherent stability of self-esteem as a psychological construct, which typically develops gradually over extended periods rather than showing rapid changes in response to brief interventions. The low between-participant variance (SD = 0.29) suggests this pattern was consistent across individuals, indicating that the lack of change was not simply due to individual differences but rather reflects the nature of self-esteem development in children. These findings suggest that meaningful improvements in self-esteem may require more intensive, longer-term interventions that provide multiple opportunities for successful experiences and sustained positive feedback.
Comparison of Wave 1 and Wave 2 Results
The analysis revealed distinct patterns between Wave 1 (baseline assessment, N=31) and Wave 2 (intervention component, N=6). While Wave 1 examined cross-sectional relationships at baseline, Wave 2 explored potential changes following intervention.
In Wave 1, emotional regulation showed a negative relationship with self-esteem (β = -0.29, p = 0.08, 95% CI [-0.33, 0.02]), contrary to our hypothesis that better emotional regulation would predict higher self-esteem. The effect size was modest (partial η² = 0.10), explaining approximately 10% of the variance in self-esteem when controlling for other factors. Similarly, internalizing problems exhibited a small negative relationship with self-esteem (β = -0.08, p = 0.75, 95% CI [-0.22, 0.161], partial η² = 0.01), aligning with our expectations but with a very small effect size that didn’t approach statistical significance.
Wave 2 intervention analyses revealed different patterns. While changes weren’t statistically significant due to the limited sample size, the effect sizes were noteworthy. For internalizing problems, the intervention produced a moderate-to-large effect (Cohen’s d = 0.72, 95% CI [-0.50, 1.94]) suggesting potential improvements in emotional difficulties. The effect on emotional regulation was moderate (Cohen’s d = 0.46, 95% CI [-0.60, 1.52]), while self-esteem showed a smaller effect (Cohen’s d = 0.35, 95% CI [-0.65, 1.35]).
Interestingly, the relationship patterns also differed between waves. While Wave 1 showed a negative relationship between emotional regulation and self-esteem, Wave 2 revealed a positive association between changes in these measures (β = 0.37, p = 0.16), suggesting that intervention-related improvements in emotional regulation might correspond with improvements in self-esteem, contrary to the baseline relationship.
These contrasting findings highlight the complex, potentially bidirectional relationships between these constructs. The negative baseline relationship between emotional regulation and self-esteem might reflect developmental processes where children who focus heavily on regulating emotions may experience reduced spontaneity and authentic self-expression, potentially influencing self-esteem. Conversely, the positive change relationship suggests that learning better regulation strategies through intervention might enhance self-perception and confidence.
The wide confidence intervals across all Wave 2 analyses underscore the exploratory nature of these findings and the need for replication with larger samples. Nevertheless, these preliminary results suggest that the relationships between emotional regulation, internalizing problems, and self-esteem may function differently in intervention contexts compared to baseline conditions, highlighting the value of examining both static relationships and dynamic change processes in understanding children’s social-emotional development.
Discussion
Drawing on the Cognitive-Behavioral Framework (CBF), this study aimed to examine the relationship between emotional regulation, internalizing problems, and self-esteem. Furthermore, the study investigated the complex patterns in how social-emotional learning interventions interact with individual and contextual factors. Regarding H1, the hypothesis that students with higher emotional regulation will predict higher self-esteem at baseline was not supported, as emotional regulation demonstrated a marginally significant negative relationship with baseline self-esteem. Contrary to our hypothesis, emotional regulation showed a negative relationship with baseline self-esteem, suggesting potential developmental complexities in how children manage and express emotions during this age period. A possible reason for this within the ages of 7-12 is that children who excel at regulating their emotions could overly rely on strategies such as suppression, which would vary for each individual and their particular situations (the Wave 2 participants were mainly from low-income families, which may have contributed for their need to internalize their problems rather than seeking help from their families, thereby lowering self-esteem). This can lead to a disconnection between their internal experiences and how they present themselves to others, contributing to feelings of reduced self-worth51. In addition, at these ages, individuals are still shaping their identities and their understanding of emotions52. The over-regulation of emotions could potentially hinder their ability to express their genuine selves, resulting in lower self-esteem. While this interpretation may offer a theoretical explanation, it should be interpreted with caution given the relatively small sample size and nonsignificant findings. Additional studies with larger samples and greater statistical power are necessary to confirm these developmental patterns. Most importantly, the absence of adequate comparison group in Wave 2 prevents us from drawing any conclusions about intervention effectiveness, compared to natural development of other factors as observed changes in the intervention group cannot be distinguished from natural developmental processes or other confounding factors.
While the study predicted that students with higher internalizing problems will have lower self-esteem (H2), H2 was partially supported, with internalizing problems showing a small negative association with self-esteem, though the effect was minimal. It may be that these participants were not yet old enough to be aware of the connection between internal struggles with their sense of self-worth, buffering the effect it could have on them. Some participants may have protective factors, such as participation in sports, activities they love, or having individuals in their lives that actively encourage them, reducing the negative effect their internal problems could have on their self-esteem. In particular, extracurricular engagement, positive teacher relationships, or access to community resources may provide emotional support and foster resilience. In addition, positive attachment relationships with caregivers and exposure to emotional education, whether at home or school, can serve as buffering mechanisms. The limited explanatory power of both baseline models (13.1% and 1.9% variance explained) suggests that other factors not captured in our measurements may play more crucial roles in children’s self-esteem development, reflecting CBF’s recognition that multiple cognitive, emotional, and environmental factors influence psychological outcomes20,21. This emphasizes the importance of recruiting a larger and more diverse group of participants in future studies in order to examine possible cultural influences on self-esteem development and responses to intervention. Any generalization made from this study should also be treated as exploratory as the homogeneity of the sample, particularly in socioeconomic status and race, limits the validity of the findings.
The limited explanatory power of both baseline models (13.1% and 1.9% variance explained) suggests that other factors not captured in our measurements may play more crucial roles in children’s self-esteem development. This aligns with the Cognitive-Behavioral Framework’s recognition that multiple cognitive, emotional, and environmental factors influence psychological outcomes20,53. Future research should incorporate a broader range of potential predictors, such as parental attitudes, peer relationships, academic performance, and specific cognitive patterns related to self-evaluation. These unmeasured influences may have impacted the observed associations and should be evaluated in future studies. For instance, changes in the level of stress at home, classroom environments, or previous exposure to mental health services could have affected both the emotional regulation and self-esteem within the participants, preventing accurate conclusions in the study. The apparent ethnic difference in self-esteem between White/Non-Hispanic and Asian participants, while intriguing, cannot be reliably interpreted given our small, demographically imbalanced sample. This highlights the importance of recruiting larger, more diverse samples in future studies to examine potential cultural influences on self-esteem development and intervention responsiveness.
For the intervention hypotheses, H3 showed limited support, with results showing a trending decrease in internalizing problems over time, though this change was not statistically significant. H4 regarding improved coping strategies was not supported, as emotional regulation demonstrated no significant change from baseline to post-intervention. This was most likely due to the limitations of an insufficient timeframe and small sample size, as the social-emotional curriculum was delivered over a period too brief for participants to fully grasp the material. However, many of the individuals may have already had the skills to regulate their emotions from the start, which could be the reason behind the little change in emotional regulation. Nevertheless, it is still important to note how these interpretations are theoretical, given the lack of any statistical significance, and should not be treated as definite conclusions. As stated previously, a larger sample is required to further evaluate this hypothesis.
Nevertheless, the intervention findings revealed more complex patterns. The strong relationships between changes in internalizing problems, emotional regulation, and self-esteem reflect CBF’s emphasis on the interconnected nature of thoughts, emotions, and behaviors in influencing mental health outcomes20,23. Despite initial minimal race effects, intervention analyses suggested varying outcomes among different ethnic groups, particularly among Asian participants. This may relate to differences in cognitive schemas and thought patterns shaped by varying parenting approaches. For example, assimilated Asian parents who adopt more Western-minded, democratic or permissive parenting styles, emphasizing nurturance, softer punishments, and greater autonomy, may foster different cognitive frameworks in their children compared to parents who employ more traditional authoritarian approaches with increased structure and discipline. These contrasting parenting cognitive models could influence how children process emotional experiences and develop coping strategies, thereby affecting their responsiveness to CBF-based interventions54. Between-participant variance patterns suggested individual differences in intervention responsiveness, reflecting how personal cognitive styles and learned thought patterns may interact differently with CBF intervention components. The contrasting findings between Wave 1 baseline analyses and Wave 2 intervention effects highlight how cognitive-behavioral patterns can shift through targeted intervention, demonstrating CBF’s premise that maladaptive thought patterns and emotional responses can be modified through structured learning experiences55.
The intervention findings must be interpreted with substantial caution given the extremely limited sample size (N=6). The lack of statistically significant changes from baseline to post-intervention, the unusually high R² value in our change score regression model, and the wide confidence intervals in our trajectory plots all reflect the statistical limitations of this exploratory analysis. Rather than providing reliable evidence of intervention effects, these preliminary observations serve primarily to generate hypotheses for future, adequately powered studies. The patterns observed– such as the trending decrease in internalizing problems and the apparent relationships between changes across measures– should be viewed as tentative directions for future research rather than established findings.
Limitations
It is important to interpret the findings of this study within the context of several key limitations. The most significant limitation of this study was our inability to maintain an adequate control group for Wave 2 analyses. While the study design originally included both intervention and control conditions, recruitment challenges and participant attrition resulted in insufficient control group data. This fundamental flaw means that any changes observed in the intervention group cannot be attributed to the intervention itself, severely limiting our ability to evaluate intervention effectiveness relative to natural development or control conditions. Without control comparisons, observed changes may simply reflect natural development, regression to the mean, practice effects, or other unmeasured factors. In addition, the small sample size (N=31 for Wave 1 and N=6 for Wave 2) significantly limited statistical power and the ability to detect meaningful effects. The restricted sample size for the intervention analysis (Wave 2) is particularly problematic for drawing conclusions about intervention effectiveness. These sample constraints position our study as exploratory rather than confirmatory, with results best viewed as generating hypotheses for future research rather than providing definitive evidence.
Additionally, the sample was predominantly Asian and recruited mostly from northern New Jersey. This demographic homogeneity limits the generalizability of findings to other racial and ethnic groups and various geographic regions. Future research should benefit from recruiting a more diverse sample across different racial and ethnic groups and regions to better understand how social-emotional interventions may impact different populations. In addition, the participants completed the survey with their caregivers and class aids, which may have impacted the results of the study as caregivers could have influenced the participants’ true responses to make them appear as ideal participants (no mental health concerns/illnesses and portraying characteristics of a “happy” child). Furthermore, several participants in the study identified as having ADHD and autism, suggesting their possible struggles with memory and recall, emotional dysregulation, executive functioning, and attention to detail, all of which may have contributed to the general results of the study.
Another significant limitation was our failure to collect data on important family-level variables such as parental education, socioeconomic status, parenting styles, and home environment characteristics. The CBF recognizes that children’s thought patterns and behavioral responses are shaped within family contexts, where parents often model coping strategies and reinforce particular cognitive approaches to emotional challenges. Without data on these family factors, we were unable to analyze how they might have moderated intervention effectiveness. For example, parental education level might influence the cognitive frameworks parents use to discuss emotions with their children, potentially enhancing or limiting the impact of CBF-based intervention components. Similarly, socioeconomic stressors could affect baseline cognitive patterns related to emotional regulation and self-esteem. Additionally, cultural differences in cognitive approaches to emotion among our predominantly Asian sample likely influenced children’s responses to the intervention in ways we could not systematically examine. Future studies should incorporate a comprehensive assessment of these family-level variables to better understand how they interact with cognitive-behavioral interventions and potentially mediate changes in children’s emotional regulation, internalizing problems, and self-esteem.
Implications
Future research directions should focus on employing larger, more diverse samples with longer intervention periods to better understand how cognitive-behavioral patterns develop and change over time. The integration of multiple informants and contexts could provide a more nuanced understanding of how different environmental influences shape cognitive schemas and affect intervention effectiveness across different populations and settings56. Furthermore, examining the role of cultural factors as potential moderators of intervention effectiveness could enhance our understanding of how to optimize social-emotional learning programs for diverse student populations.
The findings in this study suggest the potential value of long-term studies in assessing how early SEL interventions can influence the developmental trajectories of individuals. While it had limitations and varying results among participants, this research suggested that SEL intervention and CBF principles are effective in children’s emotional development. The mental health challenges faced by youth in our communities are critical and require the aid of educators, policymakers, and caretakers to better utilize culturally adaptive methods and programs to facilitate the integration of interventions into educational contexts. When applied, it could potentially enhance the impact of future social-emotional learning programs and improve mental health outcomes for a broader range of children from diverse ethnicities, socioeconomic status, family dynamics, and other factors including those with cognitive and learning disabilities.
In addition to these, in future investigations, a full-scale study should incorporate a more rigorous and comprehensive design in order to better evaluate the effectiveness of social-emotional learning interventions on elementary students’ mental health. Expanding the sample size to include several hundred participants rather than the relatively low number of participants in the study would increase the statistical power and allow for greater applicability of the findings. Furthermore, an effort to recruit a demographically diverse sample on top of the expansion of the sample size, across racial, ethnic, socioeconomic, and geographic backgrounds, could also enable researchers in the future to explore how different groups could respond to SEL interventions and to identify potential cultural markers of effectiveness. Extending the duration of the intervention, such as implementing it over an entire academic year with follow-up assessments, would be beneficial, as it could more effectively capture the development of emotional regulation and coping strategies. This extended timeframe would also provide insight into whether more significant gains are experienced over time, consistent with the principles of CBF. Future studies should also integrate data from multiple informants (e.g., parents, caregivers) and utilize mixed methods, combining quantitative self-report scales with observational measures, behavioral tasks, and interviews, to capture a broader range of perspective to yield more accurate results related to emotional regulation, coping strategies, and mental health.
Conclusion
This study explored the effectiveness of social-emotional learning (SEL) interventions on elementary students’ mental health, focusing on emotional regulation, internalizing problems, as well as self-esteem through the Cognitive-Behavioral Framework (CBF). Findings from the baseline phase (Wave 1) showed that emotional regulation was negatively associated with self-esteem, while internalizing problems only had a minimal relationship, with both findings resulting in little statistical significance. These findings suggest that other variables could potentially play a more prominent role in shaping students’ emotional well-being, remaining consistent with CBF’s emphasis on how environmental factors influence the development of cognitive schemas and thought patterns that mediate emotional and behavioral responses. During the intervention phase (Wave 2), although improvements in emotional regulation and internalizing symptoms were not statistically significant and moderate, there were strong interrelationships among the outcome variables (R2=.95). These associations indicate the potential utilization of SEL programming, especially when considered within the developmental contexts of diverse student populations. Ethnic differences, particularly among many of the Asian participants, revealed culturally unanticipated responses to intervention, reinforcing the importance of integrating cultural responsiveness into the program. In general, while the intervention did not yield notable shifts in emotional outcomes within the relatively short time frame, the direction of change and the inter-variable dynamics provide support for CBF’s applicability in intervention research. These findings emphasize the importance of considering the developmental stage, cultural background, and environmental contexts of the individual when evaluating school-based mental health support.
References
- R. M. Ghandour, L. J. Sherman, C. J. Vladutiu, M. M. Ali, S. E. Lynch, R. H. Bitsko, S. J. Blumberg. Prevalence and treatment of depression, anxiety, and conduct problems in US children. The Journal of Pediatrics, 206, 256-267 (2019). [↩]
- D. G. Whitney, M. D. Peterson. US national and state-level prevalence of mental health disorders and disparities of mental health care use in children. JAMA Pediatrics, 173(4), 389-391 (2019). [↩]
- R. Leeb, R. Bitsko, L. Radhakrishnan, P. Martinez, R. Njai, K. Holland. Mental health-related emergency department visits among children aged <18 years during the COVID-19 pandemic – United States, January 1-October 17, 2020. Morbidity and Mortality Weekly Report, 69, 1675-1680. https://doi.org/10.15585/mmwr.mm6945a3 (2020). [↩]
- M. Alegría, K. Alvarez, R. Z. Ishikawa, K. DiMarzio, S. McPeck. Removing obstacles to eliminating racial and ethnic disparities in behavioral health care. Health Affairs, 35(6), 991–999. https://doi.org/10.1377/hlthaff.2016.0029 (2016). [↩]
- Centers for Disease Control and Prevention. Mental health treatment among children aged 5–17 years: United States, 2021. https://www.cdc.gov/nchs/products/databriefs/db472.htm (2023). [↩]
- L. M. Gutman, H. Joshi, M. Parsonage, I. Schoon. Centre for Mental Health, & University College London. Children of the new century: Mental health findings from the Millennium Cohort Study. (2014). [↩]
- M. M. Ali, K. West, J. L. Teich, S. Lynch, R. Mutter, J. Dubenitz. Utilization of mental health services in educational settings by adolescents in the United States. Journal of School Health, 89(5), 393–401. https://doi.org/10.1111/josh.12753 (2019). [↩]
- V. Irwin, K. Wang, J. Cui, A. Thompson. Report on indicators of school crime and safety: 2021 (NCES 2022-092/NCJ 304625). National Center for Education Statistics, U.S. Department of Education, and Bureau of Justice Statistics, Office of Justice Programs, U.S. Department of Justice. https://nces.ed.gov/pubsearch/pubsinfo.asp?pubid=2022092 (2022). [↩]
- National Center for Education Statistics. Over half of public schools report staffing and funding limit their efforts to effectively provide mental health services to students in need [Press release]. U.S. Department of Education. https://nces.ed.gov/whatsnew/press_releases/5_9_2024.asp (2024). [↩]
- The Jed Foundation. New report scores school mental health in our state and provides a roadmap for a hopeful future [Press release]. https://www.jedfoundation.org/new-report-scores-school-mental-health-in-our-state-and-provides-a-roadmap-for-a-hopeful-future/ (2022). [↩]
- J. E. Zins, M. J. Elias. Social and emotional learning. In G. G. Bear, K. M. Minke (Eds.), Children’s needs III: Development, prevention, and intervention (pp. 1–13). National Association of School Psychologists. (2006). [↩]
- Collaborative for Academic, Social, and Emotional Learning. Safe and sound: An educational leader’s guide to evidence-based social and emotional learning (SEL) programs. Collaborative for Academic, Social, and Emotional Learning (CASEL). (2003). [↩]
- J. A. Durlak, R. P.Weissberg, A. B. Dymnicki, R. D. Taylor, K. B. Schellinger. The impact of enhancing students’ social and emotional learning: A meta‐analysis of school‐based universal interventions. Child Development, 82(1), 405-432. https://doi.org/10.1111/j.1467-8624.2010.01564.x (2011). [↩]
- B. E. Compas, S. S. Jaser, A. H. Bettis, K. H. Watson, M. A. Gruhn, J. P. Dunbar, … J. C. Thigpen. Coping, emotion regulation, and psychopathology in childhood and adolescence: A meta-analysis and narrative review. Psychological Bulletin, 143(9), 939-991. https://doi.org/10.1037/bul0000110 (2017). [↩]
- C. Zenner, S. Herrnleben-Kurz, H. Walach. Mindfulness-based interventions in schools—a systematic review and meta-analysis. Frontiers in Psychology, 5, 603. https://doi.org/10.3389/fpsyg.2014.00603 (2014). [↩]
- K. W. Merrell. Social-emotional intervention in schools: Current status, progress, and promise. School Psychology Review, 31(2), 143-147 (2002). [↩]
- R. F. W. Diekstra. Effectiveness of school-based social and emotional education programmes worldwide. In C. Clouder, B. Mackay, M. Bernard, & T. P. P. Deakin-Crick (Eds.), Social and emotional education: An international analysis (pp. 255–284). Fundación Marcelino Botín. (2008). [↩]
- Conduct Problems Prevention Research Group. The effects of the Fast Track preventive intervention on the development of conduct disorder across childhood. Child Development, 81(3), 1001–1016 (2010). [↩]
- M. T. Greenberg, C. Domitrovich, B. Bumbarger. The prevention of mental disorders in school-aged children: Current state of the field. Prevention & Treatment, 4(1), Article 1. https://doi.org/10.1037/1522-3736.4.1.41a (2001). [↩]
- A. T. Beck. Cognitive therapy and the emotional disorders. International Universities Press. (1976). [↩] [↩] [↩] [↩] [↩]
- A. Ellis. Reason and emotion in psychotherapy. Lyle Stuart. (1962). [↩] [↩]
- P. C. Kendall. Cognitive-behavioral therapies with youth: Guiding theory, current status, and emerging developments. Journal of Consulting and Clinical Psychology, 61(2), 235-247. https://doi.org/10.1037/0022-006X.61.2.235 (1993). [↩]
- R. W. Christner, J. L. Stewart, C. A. Mulligan, Eds. Handbook of cognitive-behavior group therapy with children and adolescents: Specific settings and presenting problems. Routledge. (2007). [↩] [↩]
- D. Meichenbaum. Cognitive-behavior modification: An integrative approach. Plenum Press. (1977). [↩]
- A. E. Kazdin, J. R. Weisz (Eds.). Evidence-based psychotherapies for children and adolescents. Guilford Press. (1998). [↩]
- P. C. Kendall, M. A. Southam-Gerow. Long-term follow-up of a cognitive-behavioral therapy for anxiety-disordered youth. Journal of Consulting and Clinical Psychology, 64(4), 724–730. https://doi.org/10.1037/0022-006X.64.4.724 (1996). [↩]
- U. Orth, R. W. Robins, K. F. Widaman. Life-span development of self-esteem and its effects on important life outcomes. Journal of Personality and Social Psychology, 102(6), 1271–1288. https://doi.org/10.1037/a0025558 (2012). [↩]
- M. R. Leary, G. Macdonald. Individual differences in self-esteem: A review and theoretical integration. In M. R. Leary & J. P. Tangney (Eds.), Handbook of self and identity (pp. 401–418). Guilford Press. (2003). [↩]
- K. H. Trzesniewski, M. B. Donnellan, T. E. Moffitt, R. W. Robins, R. Poulton, A. Caspi. Low self-esteem during adolescence predicts poor health, criminal behavior, and limited economic prospects during adulthood. Developmental Psychology, 42(2), 381–390. https://doi.org/10.1037/0012-1649.42.2.381 (2006). [↩]
- M. Masselink, E. Van Roekel, A. J. Oldehinkel. Self-esteem in early adolescence as predictor of depressive symptoms in late adolescence and early adulthood: The mediating role of motivational and social factors. Journal of Youth and Adolescence, 47, 932–946. https://doi.org/10.1007/s10964-017-0727-z (2018). [↩]
- K. R. Wentzel, S. Jablansky, N. R. Scalise. Peer social acceptance and academic achievement: A meta-analytic study. Journal of Educational Psychology, 113(1), 157. https://doi.org/10.1037/edu0000468 (2021). [↩]
- M. D. Weist, E. A. Mellin, K. L. Chambers, N. A. Lever, D. Haber, C. Blaber. Challenges to collaboration in school mental health and strategies for overcoming them. Journal of School Health, 82(2), 97–105. https://doi.org/10.1111/j.1746-1561.2011.00672.x (2012). [↩]
- S. R. Shirk, M. Karver. Prediction of treatment outcome from relationship variables in child and adolescent therapy: A meta-analytic review. Journal of Consulting and Clinical Psychology, 71(3), 452–464. https://doi.org/10.1037/0022-006X.71.3.452 (2003). [↩]
- D. M. Melamed, J. Botting, K. Lofthouse, L. Pass, R. Meiser-Stedman. The relationship between negative self-concept, trauma, and maltreatment in children and adolescents: A meta-analysis. Clinical Child and Family Psychology Review, 27(1), 220-234 (2024). [↩]
- C. Inguglia, S. Ingoglia, A. L. Coco. The relation between emotional support, self-concept, and social functioning among school-aged children. BPA-Applied Psychology Bulletin (Bollettino di Psicologia Applicata), 60(267) (2013). [↩]
- J. Simons, C. M. Capio, P. Adriaenssens, H. Delbroek, I. Vandenbussche. Self-concept and physical self-concept in psychiatric children and adolescents. Research in Developmental Disabilities, 33(3), 874-881 (2012). [↩] [↩] [↩]
- J. Zitzmann, L. Rombold-George, C. Rosenbach, B. Renneberg. Emotion regulation, parenting, and psychopathology: A systematic review. Clinical Child and Family Psychology Review, 27(1), 1-22 (2024). [↩] [↩] [↩]
- A. E. Kazdin, J. R. Weisz (Eds.). Evidence-based psychotherapies for children and adolescents. Guilford Press. (1998). [↩]
- H. F. Behrendt, W. Scharke, B. Herpertz‐Dahlmann, K. Konrad, C. Firk. Like mother, like child? Maternal determinants of children’s early social‐emotional development. Infant Mental Health Journal, 40(2), 234-247 (2019). [↩]
- J. Zitzmann, L. Rombold-George, C. Rosenbach, B. Renneberg. Emotion regulation, parenting, and psychopathology: A systematic review. Clinical Child and Family Psychology Review, 27(1), 1-22 (2024). [↩]
- J. A. Durlak, R. P.Weissberg, A. B. Dymnicki, R. D. Taylor, K. B. Schellinger. The impact of enhancing students’ social and emotional learning: A meta‐analysis of school‐based universal interventions. Child Development, 82(1), 405-432. https://doi.org/10.1111/j.1467-8624.2010.01564.x (2011). [↩]
- M. Rones, K. Hoagwood. School-based mental health services: A research review. Clinical Child and Family Psychology Review, 3(4), 223-241 (2000). [↩]
- L. H. Jaycox, A. K. Langley, B. D. Stein, M. Wong, P. Sharma, M. Scott, M. Schonlau. Support for students exposed to trauma: a pilot study. School Mental Health, 1(2), 49–60. https://doi.org/10.1007/s12310-009-9007-8 (2009). [↩]
- H. F. Crean, D. B. Johnson. Promoting Alternative Thinking Strategies (PATHS) and elementary school-aged children’s aggression: Results from a cluster randomized trial. American Journal of Community Psychology, 52, 56–72 (2013). [↩]
- R. Goodman. Psychometric properties of the strengths and difficulties questionnaire. Journal of the American Academy of Child & Adolescent Psychiatry, 40(11), 1337-1345 (2001). [↩] [↩]
- S. A. Whitcomb, J. Parisi Damico. Merrell’s Strong Start—Grades K-2: A Social & Emotional Learning Curriculum, Second Edition. Brookes Publishing. (2016). [↩] [↩]
- R. Goodman. Psychometric properties of the strengths and difficulties questionnaire. Journal of the American Academy of Child & Adolescent Psychiatry, 40(11), 1337-1345 (2001).) [↩]
- H. Gehlbach. Emotional Regulation Assessment [Assessment instrument]. Panorama Education. https://www.panoramaed.com (2015). [↩]
- M. Rosenberg. Rosenberg self-esteem scale. APA PsycTests. (1965).) [↩]
- C. Wood, M. Griffin, J. Barton, G. Sandercock. Modification of the Rosenberg scale to assess self-esteem in children. Frontiers in Public Health, 9, 655892. https://doi.org/10.3389/fpubh.2021.655892 (2021). [↩]
- J. J. Gross, O. P. John. Individual differences in two emotion regulation processes: Implications for affect, relationships, and well-being. Journal of Personality and Social Psychology, 85(2), 348–362. https://doi.org/10.1037/0022-3514.85.2.348 (2003). [↩]
- K. V. Jakobsen, P. Fischer. Challenges Conducting Developmental Research. Child and Adolescent Development. (2023). [↩]
- A. Ellis. Reason and emotion in psychotherapy. Lyle Stuart. (1962). [↩]
- A. E. Kazdin, J. R. Weisz (Eds.). Evidence-based psychotherapies for children and adolescents. Guilford Press. (1998). [↩]
- P. C. Kendall. Cognitive-behavioral therapies with youth: Guiding theory, current status, and emerging developments. Journal of Consulting and Clinical Psychology, 61(2), 235-247. https://doi.org/10.1037/0022-006X.61.2.235 (1993). [↩]
- R. W. Christner, J. L. Stewart, C. A. Mulligan, Eds. Handbook of cognitive-behavior group therapy with children and adolescents: Specific settings and presenting problems. Routledge. (2007). [↩]



{kind=link}