
Abstract
Substance use disorders (SUDs) are a highly prevalent global issue worldwide associated with high relapse rates. These outcomes may be caused by substance related changes in brain circuits responsible for reward processing, impulse control, and decision making. Transcranial magnetic stimulation (TMS) is a non-invasive intervention with potential in addressing these addiction related neural changes. This literature review examines the potential of TMS as an emerging intervention for individuals with SUDs, focusing on clinical outcomes including craving, abstinence, and relapse-related measures. This review included 11 peer-reviewed human studies identified through PubMed ScienceDirect, and Google Scholar, published in English within the past 20 years. Eligible studies examined TMS or repetitive TMS (rTMS) as an intervention for SUDs, and reported outcomes related to craving, relapse, or abstinence using clinical or experimental designs, such as randomized controlled trials (RCTs), systematic reviews, and pilot studies. No formal meta-analysis was conducted and a PRISMA-like search strategy guided study selection. TMS, most frequently targeting the dorsolateral prefrontal cortex, was associated with reductions in craving and substance use, with some trials reporting improved relapse related outcomes. Effects were most consistent in alcohol and nicotine use disorders compared with cocaine and stimulate use disorders. Clinical trials further demonstrate that combining repetitive TMS (rTMS) with approaches such as cognitive-behavioral therapy may potentiate treatment outcomes compared to standalone interventions. Overall, evidence suggests that TMS is a promising intervention for targeting neurobiological pathways involved in addiction. Future research should focus on establishing standardized protocols and identifying effective integration within comprehensive treatment plans.
Keywords: TMS; substance use disorder; relapse prevention; neuroplasticity; dorsolateral prefrontal cortex; addiction; efficacy
Introduction
Substance use disorders (SUDs) are a highly prevalent issue worldwide and place substantial impacts on both individuals and society. Global estimates indicate that alcohol, opioid, cannabis, stimulant, and nicotine use disorders affect millions of individuals. Beyond their high prevalence, SUDs are associated with detrimental effects on longevity and brain development, while also imposing a substantial economic and emotional burden.
The prevalence of SUDs has continued to increase, with the percentage of individuals with drug use disorder aged 12 or older increasing from 8.7% in 2021 to 9.8% in 20241. A growth in substance use can be attributed to multiple factors, including technological advancements that facilitate the online drug trade, increased accessibility, and policy changes, such as the legalization of cannabis, which have been linked to greater use among young adults. The emergence of digital marketplaces has increased wholesale activity regarding the distribution, selling, and buying of illegal substances2.
One study reported that beyond age 15, drug use, on average, was estimated to reduce life expectancy by 1.4 years for men and 0.7 years for women3. Other factors contributing to such reductions in longevity are due to the association between substance abuse and higher rates of chronic diseases such as cancer, cardiovascular disease, liver damage, and neurodegenerative conditions like Alzheimer’s, which worsen long-term health outcomes.
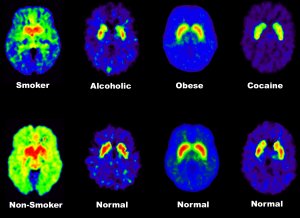
Beyond these consequences, SUDs are associated with structural brain changes, including grey and white matter abnormalities in brain regions involved in cognitive and emotional processing, such as the anterior cingulate (ACC), lateral prefrontal, and insular cortex4. White matter alterations associated with chronic substance use may involve demyelination (damaging of the protective myelin sheath around nerve fibers), cognitive deficits, and disruptions in white matter microstructure, although the permanence of these changes remains uncertain5,6. These neurobiological alterations are further supported by evidence of reduced dopamine D2 receptor availability in individuals with SUDs compared to healthy controls, reflecting impaired reward system functioning associated with increased drug seeking behavior. Collectively, these findings suggest that SUDs involve dysregulation of neural systems associated with reward processing and executive control, contributing to increased vulnerability to craving, as illustrated by reduced dopamine receptor availability in individuals with SUDs (see Figure 1). These findings have contributed to growing interest in interventions targeting neural systems involved in executive control and reward processing.
Despite the global prevalence and severity of SUDs, existing treatments show variable efficacy with relapse rates ranging from 40% to 60% among individuals in recovery8. A study published in 2019 concluded that the number of alcohol or other drug (AOD) recovery attempts varied widely, ranging from 0 to 100. The mean number of attempts was 5.35, and the median was 29. This increase of the mean compared to the median suggests a positively skewed distribution with heterogeneous recovery trajectories. The variability in achievable recovery outcomes highlights a need for more effective, accessible, and personalized interventions that may improve long-term recovery outcomes for individuals with SUDs. Moreover, widely implemented approaches such as Alcoholics Anonymous, talk therapy, and related interventions provide support but demonstrated consistent long-term reductions in substance use or relapse outcomes.
In recent decades, emerging work in neuroscience has begun to address unique psychobiological factors associated with addiction. Such modalities have included pharmacological treatments, neuromodulation techniques such as deep brain stimulation (DBS) and transcranial direct current stimulation (tDCS), and neurocognitive interventions like mindfulness-based relapse prevention10.
Transcranial magnetic stimulation (TMS) is a non-invasive neuromodulatory technique that has been increasingly investigated as a potential approach for targeting neural mechanisms affected in SUDs by utilizing magnetic pulses to modulate neural activity in targeted brain regions. The rationale for TMS in addiction treatment stems from the fact that chronic substance use disrupts neural circuits involved in reward, decision making, and impulse control. Dysfunction in the prefrontal cortex (PFC) and its connections to limbic regions have been associated with disrupted control, contributing to increased craving and vulnerability to relapse by targeting the dorsolateral prefrontal cortex (DLPFC), TMS may modulate neural activity within these pathways, thus potentially strengthening regulation11. The U.S. Food and Drug Administration (FDA) has approved TMS for the treatment of depression, OCD, migraines, and smoking cessation in patients who have not benefited from other interventions. When administered through the delivery of repeating magnetic pulses, this procedure is referred to as repetitive TMS (rTMS). TMS uses an electromagnetic coil placed against the scalp, generating a magnetic field which induces neural cell membrane to undergo depolarization in cortical tissue under the coil12. Due to the crucial role depolarization plays in neuronal firing, this method affects the related nerve loop activity. TMS may also promote neuroplasticity, supporting long-term changes in brain regions involved in self-control and reward processing13.
This literature review examines the potential of transcranial magnetic stimulation (TMS) as an emerging intervention for SUDs, with a particular focus on clinical outcomes including craving, abstinence, and relapse-related measures published within the past 20 years. The neurobiological mechanisms through which TMS may promote neuroplasticity and strengthen executive control, its integration with existing treatment approaches, and current challenges are also examined.
Methods
This literature review was conducted by searching key terms including “TMS,” “addiction,” “relapse,” “substance use disorder (SUD),” “efficacy,” “DLPFC,” and “treatment.” Sources were identified through academic databases such as PubMed and ScienceDirect, and Google Scholar was utilized as a research tool to identify relevant studies. Search terms included combinations of (“transcranial magnetic stimulation” OR “TMS” OR “rTMS”) AND (“substance use disorder” OR “addiction”) AND (“relapse” OR “craving” OR “abstinence”). Searches were done primarily between July 2025 and February 2026.
To ensure relevance, this review focused on studies published in English within the past 20 years, and excluded studies limited to unrelated neurological conditions. Studies were included if they examined TMS or repetitive TMS (rTMS) as an intervention for SUDs in human participants and reported at least one clinically relevant outcome, such as craving, abstinence, substance use frequency, or relapse-related outcomes. Eligible studies included randomized controlled trials (RCTs), systematic reviews, and pilot studies. They were excluded if they focused primarily on neurological disorders unrelated to SUDs, such as stroke rehabilitation, Parkinson’s disease, or motor disorders. Non-peer reviewed sources were also excluded.
The initial search identified approximately 60 studies, and after removal of irrelevant studies, 11 were ultimately included in this review. Data extracted from each selected study included author names, publication year, research design, sample size, TMS protocol parameters, and primary outcomes. Quantitative data, such as relapse and abstinence rates, craving measures, and treatment outcomes, were incorporated to highlight efficacy and trends across studies. Qualitative findings were also utilized to discuss clinical findings and the potential role TMS has on relapse prevention. In this review, the terms “substance use disorder (SUD),” “addiction,” and “relapse prevention” are used when describing individuals with SUDs.
This review was conducted as a literature review rather than a meta-analysis, and no formal quality scoring tool or meta-analytic synthesis was applied, though a PRISMA-like search strategy guided study selection.
Results
Across multiple studies, TMS was associated with reductions in craving intensity and substance use frequency particularly in alcohol and nicotine use disorders, with some studies additionally reporting improvements in abstinence or relapse related outcomes. Substances such as alcohol and nicotine account for a substantial proportion of global addiction cases, with around 400 million people worldwide estimated to have AUDs and 1.3 billion tobacco users, making these findings significant for public health14,15. While research in opioid and other stimulant use disorders remains comparatively limited, current evidence suggests potential benefits that require further exploration for a variety of addictive substances.
Combination with other therapies
Others suggest that non-specific factors, including the structured protocol, support, and increased clinical contact in TMS treatment may contribute to motivational or placebo related reductions in craving. However, compared to control conditions, TMS groups still show greater reductions in craving and substance use measures, with some studies also reporting abstinence and relapse related outcomes, although outcome definitions and assessments varied across studies. These effects are attributed to direct modulation of neural circuits involved in craving, impulse control, and reward processing, which are thought to underlie relapse vulnerability16. In comparison to psychotherapy or pharmacotherapy, which primarily rely on gradual behavioral changes or pharmacological effects, rTMS may promote neurobiological changes17. For instance, rTMS causes acute and lasting neuroplastic changes that can yield measurable improvements in brain function, particularly in dopamine and glutamate activity18. Although TMS as a standalone intervention is promising, studies demonstrate its combination with other approaches, such as cognitive-behavior therapy (CBT), psychotherapy, and Alcoholics Anonymous (AA), can further potentiate treatment outcomes. For instance, a 2022 study discovered the strongest effect in preventing alcohol relapse at 24 weeks resulted from combining left DLPFC rTMS with a full CBT plan19. For a detailed comparison of TMS treatment studies, see Table 1.
Short-term and Long-term Effects
| Study (Author, Year) | Substance Type | TMS protocol (site, frequency, pulses/session, intensity) | Treatment duration (sessions/week x weeks; total sessions) | Sample size (n) | Paired with other therapy | Primary outcome (method) | Primary Findings | Follow up |
| Zangen et al., 2021 | Tobacco/Nicotine | Site: Lateral prefrontal cortex and insular cortex Frequency: 10 Hz high-frequency rTMS Pulses/session: 1,800 pulses per session (60 trains of 30 pulses) Intensity: 120% of the individual’s minimal motor threshold | Schedule: 5 sessions/week for the first 3 weeks (daily on weekdays), followed by 1 session/week for an additional 3 weeks Total Sessions: 18 sessions | Total Enrolled: 262 participants Randomization Allocation: Active: 123 / Sham: 139 Intent-to-Treat (ITT) Set: 234 total (Active vs. Sham groups analyzed as a whole) Completer Analysis Set: 169 total | Symptom Provocation: 5-minute cue-induced craving provocation procedure (handling a cigarette/lighter, viewing smoking images, and listening to a guided audio script). Behavioral Support: ~2 minute post-session motivational talk utilizing the National Cancer Institute’s “Clearing the Air” protocol booklet | 4-week continuous quit rate (CQR) verified by urine cotinine. Tracked via daily smoking diaries and objectively validated by biological testing (urine cotinine levels < 200 ng/ml). | Intent-to-Treat (ITT): 19.4% continuous quit rate (Active) vs. 8.7% (Sham); (p=0.017) Completers: (28.0% active vs. 11.7% sham;(p=0.007) Craving/Consumption: Active rTMS yielded a greater reduction in both self-reported daily cigarette consumption and physiological cravings (measured via Tobacco Craving Questionnaires) as early as 2 weeks into treatment. | 6-week acute phase + 12-week extension (monitored to Week 18) |
| Hu et al., 2022 | Alcohol | Site: Left DLPFC (F3) or Right DLPFC (F4) Frequency: High frequency (10 Hz) Pulses per Session: 1,500 pulses (30 trains × 5-second duration) Intensity: 110% of individual resting motor threshold (MT) | Schedule: 5 consecutive days/week for 2 weeks Total Sessions: 10 sessions | Total Enrolled: 263 participants | Paired Therapy: Individual Cognitive Behavioral Therapy (CBT) Group C1: Fixed 8-week structured plan (60 mins/session) Group C0: Unstructured basic plan (10-minute standardized interview) | Relapse rates tracking via alcohol consumption diaries, telephone checks, and outpatient follow-ups | Sham rTMS + C0 vs. Right rTMS + C1: 45.0% relapse rate (sham rTMS + C0) vs. 14.3% (right rTMS + C1); (P = 0.006) Sham rTMS + C0 vs. Left rTMS + C0: 45.0% relapse rate (sham rTMS + C0) vs. 21.9% (left rTMS + C0); (P = 0.031) Sham rTMS + C0 vs. Left rTMS + C1: 45.0% relapse rate (sham rTMS + C0) vs. 22.2% (left rTMS + C1); (P = 0.043) Right rTMS + C0 vs. Right rTMS + C1: Unstructured CBT 37.1% vs. Structured CBT 14.3% ;((P = 0.046) | 24 weeks |
| Dinur-Klein et al., 2014 | Nicotine (Cigarette tobacco smoking) | Site: Lateral prefrontal cortex (PFC) and insula bilaterally Frequency: High-frequency (20 Hz) or Low-frequency (1 Hz) Pulses/Session: Not specified in study Intensity:120% of the resting motor threshold (RMT) | 13 daily sessions over course of treatment | Total Enrolled: 115 participants | Paired with or without a brief smoking provocation (exposure to personalized visual/tactile smoking cues) prior to stimulation | Objective measurement of nicotine consumption through urine cotinine levels combined with subjective patient self-reports | High frequency deep TMS treatment reduced substance consumption and nicotine dependence; combination with cue exposure enhanced effect Combination of treatment with exposure to smoking cues: 44% abstinence rate at end of treatment 6 months following completion of treatment: 33% abstinence rate | 6 months |
| Martinotti et al., 2022 | Cocaine | Site: Left dorsolateral prefrontal cortex (DLPFC) Frequency: 10 Hz Pulses/Session: 4,000 pulses Intensity: Target 120% resting motor threshold (RMT) | Schedule: 2 visits/week (2 sessions/visit) x 5 weeks Total Sessions: 20 sessions | Intent-to-Treat: (N = 72) (37 Active, 35 Sham) Completers: (N = 51) | 3-session Motivational Enhancement Therapy (MET) | Change in spontaneous craving between pre- and post-treatment via the Marijuana Craving Questionnaire Short-Form (MCQ-SF) | Craving: No significant differences, decreased from 45.8 +/- 18.5 to 27.7 +/- 15.1 (active group) vs Decreased from 45.2 +/- 16.3 to 22.6 +/- 11.1 (sham group); p=0.33 Days of Use: sustained lower usage days in final weeks (active group) vs rebounded in usage days during final weeks (sham group); p=0.02 Abstinence: 15.5% of weeks spent abstinent (active group) vs 9.3% of weeks spent abstinent (sham group); p=0.14 | 14 weeks |
In addiction treatment, TMS can produce both immediate and sustained effects, with outcomes varying according to the stimulation protocol used. Short-term effects consist of immediate reductions in cravings, along with improvements in mood and impulse control. Temporary side effects, such as mild headaches, dizziness, or facial muscle twitching, typically resolve within a day. Long term outcomes often involve sustained reductions in addiction severity, marked by reduced cravings and lower substance use. Clinical trials suggest that these benefits may persist for weeks to months following treatment, though efficacy varies depending on the protocol used20.
Discussion
Follow up periods varied across trials, which limit standardized conclusions and direct comparisons regarding sustained effects. According to the studies, effects were most consistent in alcohol and nicotine use disorders. Specifically, nicotine trials reported higher abstinence rates in active rTMS groups compared to sham conditions, while alcohol trials reported reduced relapse rates in active groups. In contrast, the study regarding cocaine use disorders demonstrated mixed results, with significant differences in days of use but not in craving or abstinence rates between active and sham conditions.
The variability in findings may reflect the differences in methodology across studies, which includes variances in stimulation frequency, number of pulses per session, treatment duration, follow-up periods, sample size, coil type, and the integration of therapies such as CBT, motivational enhancement therapy, or cue exposure therapy. Additionally, differences in the mechanisms of specific substances may contribute to the variability in treatment responses. Thus, current evidence suggests that TMS demonstrates potential across multiple SUDs, but treatment efficacy may depend on methodological and substance specific factors.
Mechanisms
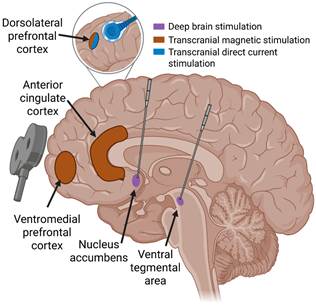
Most broadly, TMS promotes neuroplasticity through a range of underlying physiological mechanisms. Neuroplasticity refers to the brain’s ability to reorganize itself through creating new neural connections, modifying its structure and function, and adapting to experiences21. This is crucial in addiction recovery due to its capability to repair damaged neural pathways and form newer and healthier behaviors22. The emerging evidence for TMS in SUDs is centered around its capacity to modulate neural circuits involved in executive control, reward processing, and impulse regulation, whose dysfunction in SUDs is thought to be linked to craving and relapse vulnerability. rTMS stimulates the dorsolateral prefrontal cortex (DLPFC), a brain area associated with executive functions such as working memory, planning, decision making, inhibition, and cognitive flexibility23. This stimulation has been associated with increased cortical excitability in the DLPFC, which refers to the reactivity of cortical neurons to stimulation in a specific region of the brain24. Additionally, TMS stimulation involving the left DLPFC modulates excitability in the anterior cingulate cortex (ACC), a region linked with executive processing and emotional regulation25. Chronic drug use is linked to abnormal patterns of cortical excitability, causing impairments in regulatory control over drug-seeking behaviors, which contributes to ongoing use and increased relapse risks26. Forms of synaptic plasticity, such as long term potentiation (LTP), which refers to the persistent strengthening of synapses, and long-term depression (LTD) (persistent weakening) are among the neuroplastic mechanisms through which TMS influences addiction27,28. TMS has been shown to induce LTP and LTD-like effects, resulting in neuroplastic changes tied to reductions in craving but their efficacy in maintaining long term abstinence and relapse prevention remains unclear29. Figure 2 highlights brain regions targeted in SUDs, including the DLPFC, ventromedial prefrontal cortex (vmPFC), and anterior cingulate cortex (ACC). These regions are involved in reward processing, executive control, and craving. Dysfunction within these areas is associated with weakened control over drug seeking behaviors, craving, and impulse regulation, which may contribute to relapse vulnerability. Through providing modulation within these regions, TMS may strengthen control over such behaviors and reduce relapse vulnerability. Furthermore, these effects may be attributed to increased dopamine activity in the nucleus accumbens (NAc), a process regulated by glutamate. Consistent drug exposure results in alterations in the ventral tegmental area (VTA) and NAc that further escalate drug seeking behaviors30. Higher dopaminergic activity and modulation of glutamate transmissions within executive control regions, including the DLPFC and anterior cingulate cortex, may contribute to strengthening inhibitory control and decision making, thus reducing impulsivity and compulsive drug seeking behaviors31.
Limitations
The current literature on TMS for SUDs has several limitations despite promising findings. Many studies feature relatively small sample sizes, which may reduce statistical power and limit the extent to which the findings can be applied to broader populations. Furthermore, there is variation in stimulation protocols including differences in frequency, intensity, session duration, follow-up periods, and total number of treatments. This variability complicates direct comparisons across studies and complicates efforts to establish standardized protocols for optimal treatment outcomes. Sham TMS conditions present methodological challenges because active stimulation can produce noticeable scalp sensations and muscle contractions. If sham conditions fail to mimic such physical sensations, it may affect the blinding aspect for participants. Additionally, expectancy effects and placebo responses may account for the improvements noted in sham groups, ultimately hindering the assessment of the efficacy of the treatment. Addressing these inconsistencies in future research may help establish more standardized guidelines and improve understanding of the potential role of TMS in SUD treatment.
Additional limitations involve the broader clinical implementation of TMS for SUDs. The cost of treatment is considerable, with access influenced by insurance policies, clinic availability, and –evolving research standards. Although insurance often provides coverage for FDA-approved indications such as depression, reimbursement for addiction treatment remains uncertain. Due to the ongoing development of TMS research, availability for addiction treatment is limited and is not FDA-approved as a first-line treatment. Variability in patient characteristics, comorbid conditions, substance type, and stimulation parameters further complicates the development of standardized treatment protocols. Additionally, due to this review following a non-systematic rather than a systematic approach and not including formal quality assessment, potential selection bias and variability in study quality should also be considered when interpreting the findings.
Conclusion
Addiction remains a serious and increasingly prevalent issue that requires effective and innovative treatments. TMS presents potential as a non-invasive intervention that targets the neurobiological pathways involved in SUDs. Although research indicates it may improve craving, abstinence and some relapse related outcomes as a standalone therapy, improved outcomes were observed by some studiesthrough the integration with other modalities, such as CBT or pharmacological treatment. To thoroughly gain insight regarding its clinical potential, future studies should focus on establishing standardized protocols and identifying the most effective ways to integrate TMS within comprehensive treatment plans.
References
- SAMHSA. SAMHSA releases annual National Survey on Drug Use and Health. 2025. https://www.samhsa.gov/newsroom/press-announcements/20250728/samhsa-releases-annual-national-survey-on-drug-use-and-health. [↩]
- C. Silvi Marchini. The digital drug revolution: How online markets are reshaping global illicit trade. Global Initiative. 27 May 2025. https://globalinitiative.net/analysis/digital-drug-revolution-online-markets-global-illicit-trade-ocindex/. [↩]
- D. A. Glei, S. H. Preston. Estimating the impact of drug use on US mortality, 1999-2016. PLOS ONE. Vol. 15, pg. e0226732, 2020. https://doi.org/10.1371/journal.pone.0226732. [↩]
- A. M. Muller, D. L. Pennington, D. J. Meyerhoff. Substance-specific and shared gray matter signatures in alcohol, opioid, and polysubstance use disorder. Frontiers in Psychiatry. Vol. 12, 2022. https://doi.org/10.3389/fpsyt.2021.795299. [↩]
- P. O. Gaudreault, S. G. King, P. Malaker, N. Alia-Klein, R. Z. Goldstein. Whole-brain white matter abnormalities in human cocaine and heroin use disorders: association with craving, recency, and cumulative use. Molecular Psychiatry. Vol. 28, pp. 780–791, 2023. https://doi.org/10.1038/s41380-022-01833-y. [↩]
- C. G. Connolly, R. P. Bell, J. J. Foxe, H. Garavan. Dissociated grey matter changes with prolonged addiction and extended abstinence in cocaine users. PLoS ONE. Vol. 8, pg. e59645, 2013. https://doi.org/10.1371/journal.pone.0059645. [↩]
- N. Volkow. PET – Human Addiction. Wikimedia Commons. 2001. https://commons.wikimedia.org/wiki/File:PET_-_Human_Addiction.jpg. [↩]
- M. Beaulieu, et al. A systematic review and meta-analysis of the efficacy of the long-term treatment and support of substance use disorders. Social Science & Medicine. Vol. 285, pg. 114289, 2021. https://doi.org/10.1016/j.socscimed.2021.114289. [↩]
- J. F. Kelly, M. C. Greene, B. G. Bergman, B. B. Hoeppner. How many recovery attempts does it take to successfully resolve an alcohol or drug problem? Estimates and correlates from a national study of recovering U.S. adults. Alcoholism: Clinical and Experimental Research. Vol. 43, pg. 1533-1544, 2019. https://doi.org/10.1111/acer.14067. [↩]
- P. A. Spagnolo, D. Goldman. Neuromodulation interventions for addictive disorders: Challenges, promise, and roadmap for future research. Brain. 2017. https://doi.org/10.1093/brain/aww284. [↩]
- C. W. Dickey, et al. Transcranial magnetic stimulation to the dorsolateral prefrontal cortex modulates single-neuron activity in humans. openRxiv. 2026. https://doi.org/10.64898/2026.03.15.711839. [↩]
- S. Groppa, A. Oliviero, A. Eisen, A. Quartarone, P. Cohen, M. Mall, S. Kaelin-Lang, T. Mima, S. Rossi, M. Rossini, C. Ziemann, U. Ziemann, R. Siebner, C. Classen, A. Valls-Solé, H. Wassermann, P. M. Rossini. A practical guide to diagnostic transcranial magnetic stimulation: Report of an IFCN committee. Clinical Neurophysiology. Vol. 123, no. 5, pg. 858–882, 2012. https://doi.org/10.1016/j.clinph.2012.01.010. [↩]
- G. S. Pell, Y. Roth, H. Shachar, M. Isserles, N. Barnea-Ygael, A. Zangen. Behavioral and Functional Brain Activity Alterations Induced by TMS Coils with Different Spatial Distributions. eNeuro. Vol. 10, pg. ENEURO.0287-22.2023, 2023, https://doi.org/10.1523/ENEURO.0287-22.2023. [↩]
- WHO. Over 3 million annual deaths due to alcohol and drug use, majority among men. World Health Organization. 2024. https://www.who.int/news/item/25-06-2024-over-3-million-annual-deaths-due-to-alcohol-and-drug-use-majority-among-men. [↩]
- World Health Organization. Tobacco. World Health Organization. 2025. https://www.who.int/news-room/fact-sheets/detail/tobacco. [↩]
- C. A. Hanlon, L. T. Dowdle, J. S. Henderson. Modulating neural circuits with transcranial magnetic stimulation: Implications for addiction treatment development. Pharmacological Reviews. Vol. 70, pg. 661-683, 2018. https://doi.org/10.1124/pr.116.013649. [↩]
- D. D. Mehta, A. Praecht, H. B. Ward, M. Sanches, M. Sorkhou, V. M. Tang, V. R. Steele, C. A. Hanlon, T. P. George. A systematic review and meta-analysis of neuromodulation therapies for substance use disorders. Neuropsychopharmacology. 2023. https://doi.org/10.1038/s41386-023-01776-0. [↩]
- J. Moretti, E. Z. Poh, J. Rodger. rTMS-induced changes in glutamatergic and dopaminergic systems: Relevance to cocaine and methamphetamine use disorders. Frontiers in Neuroscience. Vol. 14, 2020. https://doi.org/10.3389/fnins.2020.00137. [↩]
- X. Hu, T. Zhang, H. Ma, X. Zhou, H. Wang, X. Wang, C. Cheng, Y. Li, R. Duan, B. Zhang, H. Wang, J. Lu, C. Kang, N. Zhao, Y. Zhang, L. Tian, J. Liu, J. Shi, Z. Wang, X. Zhou. Repetitive transcranial magnetic stimulation combined with cognitive behavioral therapy treatment in alcohol-dependent patients: A randomized, double-blind sham-controlled multicenter clinical trial. Frontiers in Psychiatry. Vol. 13, 2022. https://doi.org/10.3389/fpsyt.2022.935491. [↩]
- D. A. Gorelick, A. Zangen, M. S. George. Transcranial magnetic stimulation in the treatment of substance addiction. Annals of the New York Academy of Sciences. Vol. 1327, 2014. https://doi.org/10.1111/nyas.12479. [↩]
- J. Kricheldorff, K. Goke, M. Kiebs, F. H. Kasten, C. S. Herrmann, K. Witt, R. Hurlemann. Evidence of neuroplastic changes after transcranial magnetic, electric, and deep brain stimulation. Brain Sciences. Vol. 12, pg. 929, 2022. https://doi.org/10.3390/brainsci12070929. [↩]
- R. Estrada-Medina, et al. Neuroplasticity and recovery of the brain affected by substance use disorder: Multilevel mechanisms and new therapeutic strategies (2020–2025). Frontiers in Molecular Neuroscience. Vol. 19, 2026. https://doi.org/10.3389/fnmol.2026.1760387. [↩]
- I. Hertrich, S. Dietrich, C. Blum, H. Ackermann. The role of the dorsolateral prefrontal cortex for speech and language processing. Frontiers in Human Neuroscience. Vol. 15, pg. 645209, 2021. https://doi.org/10.3389/fnhum.2021.645209. [↩]
- M. Grall-Bronnec, A. Sauvaget. The use of repetitive transcranial magnetic stimulation for modulating craving and addictive behaviours: A critical literature review of efficacy, technical and methodological considerations. Neuroscience & Biobehavioral Reviews. Vol. 47, pg. 592-613, 2014. https://doi.org/10.1016/j.neubiorev.2014.10.013. [↩]
- M. Tik, A. Hoffmann, R. Sladky, L. Tomova, A. Hummer, L. Navarro de Lara, H. Bukowski, J. Pripfl, B. Biswal, C. Lamm, C. Windischberger. Towards understanding rTMS mechanism of action: Stimulation of the DLPFC causes network-specific increase in functional connectivity. NeuroImage. Vol. 162, pg. 289-296, 2017. https://doi.org/10.1016/j.neuroimage.2017.09.022. [↩]
- E. Bellamoli, P. Manganotti, R. P. Schwartz, C. Rimondo, M. Gomma, G. Serpelloni, A. Fertonani. rTMS in the treatment of drug addiction: An update about human studies. Behavioural Neurology. Vol. 2014, pg. 815215, 2014. https://doi.org/10.1155/2014/815215. [↩]
- G. C. Teskey. Long-term potentiation and long-term depression. Oxford Research Encyclopedia of Psychology. 2025. https://doi.org/10.1093/acrefore/9780190236557.013.789. [↩]
- S. R. Vorel, S. H. Lisanby. Therapeutic potential of TMS-induced plasticity in the prefrontal cortex. Oxford University Press. 2012. https://doi.org/10.1093/oxfordhb/9780198568926.013.0038. [↩]
- T. V. P. Bliss, S. F. Cooke. Long-term potentiation and long-term depression: A clinical perspective. Clinics. Vol. 66, pg. 3-17, 2011. https://doi.org/10.1590/s1807-59322011001300002. [↩]
- R. Sinha. Chronic stress, drug use, and vulnerability to addiction. Annals of the New York Academy of Sciences. Vol. 1141, pg. 105-130, 2008. https://doi.org/10.1196/annals.1441.030. [↩]
- N. D. Volkow, G. J. Wang, J. S. Fowler, D. Tomasi, F. Telang. Addiction: Beyond dopamine reward circuitry. Proceedings of the National Academy of Sciences. Vol. 108, pg. 15037-15042, 2011. https://doi.org/10.1073/pnas.1010654108. [↩]
- T. S. Oesterle, N. L. Bormann, M. Al-Soleiti, S. Kung, B. Singh, M. T. McGinnis, S. Correa da Costa, T. Rummans, M. Chauhan, J. M. Rojas Cabrera, S. A. Vettleson-Trutza, K. M. Scheitler, H. Shin, K. H. Lee, M. S. Gold. Invasive and non-invasive neuromodulation for the treatment of substance use disorders: A review of reviews. Brain Sciences. Vol. 15, no. 7, pg. 723, 2025. https://doi.org/10.3390/brainsci15070723. [↩]



{kind=link}