
Abstract
Glioblastoma (GBM) remains the most aggressive and lethal primary brain tumor in adults, with a median survival of approximately one year despite recent advancements in surgery, chemotherapy, and radiotherapy. Even with current treatments, six-month progression-free survival rate (PFS-6) ranges from only 9% to 21%; objective response rates (ORR) remain below 10%, and median overall survival (OS) does not exceed 30 weeks. The limited efficacy of current therapies underscores the urgent need for innovative treatment strategies. This paper compares novel therapies for recurrent glioblastoma, focusing on recent clinical trials that explore immunotherapy, oncolytic viruses, CAR-T cell therapy, monoclonal antibodies, and gene-targeted treatments. By examining their mechanisms, clinical outcomes, and limitations, the paper aims to evaluate which emerging treatments hold the most promise for improving survival and quality of life in patients with this devastating disease. The findings highlight the difficulty of finding proper glioblastoma treatments and emphasize the importance of continued research to develop more effective, personalized therapeutic approaches.
Introduction
Glioblastoma continues to be the most aggressive and lethal form of primary brain cancer in adults. Despite modern advancements in surgery, radiation, and chemotherapy, the majority of patients experience tumor recurrence, leading to poor progression-free and long-term survival outcomes.
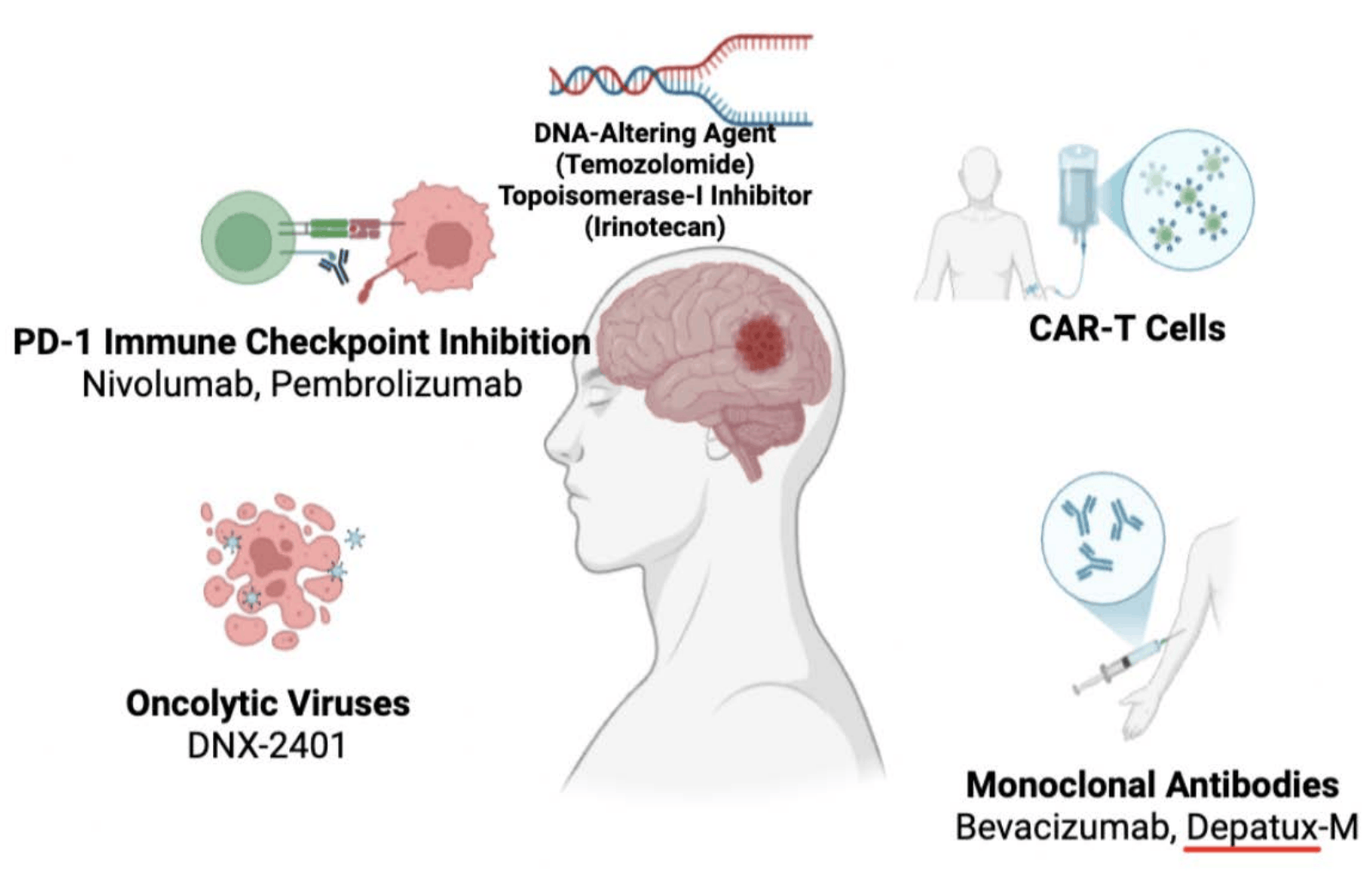
Glioblastoma progression is driven by marked intratumoral heterogeneity, diffuse infiltration, and a profoundly immunosuppressive tumor microenvironment, which collectively limit durable therapeutic response1. The glioblastoma microenvironment is profoundly immunosuppressive. Standard treatment typically involves surgery followed by radiotherapy, however, no current therapies have significantly prolonged OS2. Patients typically die within 6 to 12 months3of the initial diagnosis, which underscores the urgent need for continued and innovative research in this area. This research paper consists of an analysis of clinical trials from the past five years, all sourced from the PubMed database, to provide a current overview of ongoing therapeutic developments. Bevacizumab (BV), an anti-angiogenic agent targeting vascular endothelial growth factor (VEGF), has been approved for use in recurrent glioblastoma, but its benefits are primarily limited to symptom management rather than extending survival. Across clinical trials, BV consistently improves imaging findings and progression-free survival but has not demonstrated an OS benefit, even when used in combination regimens. Additionally, immunotherapies such as checkpoint inhibitors and novel approaches like gene therapy and oncolytic viruses are being explored4, but results have been mixed and challenges remain. The limited efficacy of existing therapies highlights the urgent need for improved treatment strategies for recurrent glioblastoma. The research is organized into four groups covering a total of eleven treatments (Figure 1). These include: oncolytic viruses including DNX2401, usage of monoclonal antibodies specifically BV, including BV+irinotecan (CPT-11), BV+ stereotactic radiosurgery (SRS), BV+pembrolizumab, and BV+VB111, a novel gene therapy that works through vascular disruption and immune activation, stimulating T-cells through Programmed death-ligand 1(PD-L1) inhibition including pembrolizumab+BV and nivolumab+BV, CAR-T therapies, and finally Depatux-M + Temozolomide (TMZ) treatments. Despite transformative success in other solid tumors, immune checkpoint inhibitors have failed to produce meaningful survival benefits in glioblastoma across multiple clinical trials, suggesting intrinsic resistance driven by tumor biology rather than trial design alone.
Methods
A focused literature search was conducted to identify recent clinical trials investigating therapeutic strategies for recurrent glioblastoma (rGBM). PubMed was the primary database, supplemented by Google Scholar for cross-verification. Searches covered the period from January 1, 2020, to March 3, 2025, capturing the most current developments in immunotherapy, targeted therapy, and chemotherapeutic approaches. Search terms included “recurrent glioblastoma,” “clinical trial,” “immunotherapy,” “CAR-T,” “oncolytic virus,” “bevacizumab,” “nivolumab,” “pembrolizumab,” “temozolomide,” and “Depatux-M.”
Inclusion criteria required studies to (1) involve human subjects with rGBM, (2) report clinical outcomes such as OS, progression-free survival (PFS), or ORR, and (3) be peer-reviewed and published in English. Exclusion criteria removed animal-only or preclinical studies, review articles, and non-English publications.
The initial search identified 304 articles. After removing duplicates and screening titles and abstracts, 64 full-text articles were reviewed, of which 20 clinical trials met all inclusion criteria. These trials were organized into five therapeutic categories: oncolytic viruses, monoclonal antibodies, PD-1 immune checkpoint inhibitors, CAR-T cell therapies, and chemotherapeutic agents.
Therapies were organized into four categories: oncolytic viruses, monoclonal antibodies, PD-1/PD-L1 immune checkpoint inhibitors (stimulating T-cells), and CAR-T cell therapies. These categories were based on their primary mechanism of action. Monoclonal antibodies, such as BV, directly target tumor or vascular proteins, whereas PD-1/PD-L1 inhibitors act indirectly by stimulating patients’ T-cells to mount an anti-tumor immune response. This categorization clarifies differences in therapeutic approach, mechanism, and expected outcomes across trials. A brief limitation of this review is that it selectively covers studies, relies heavily on early-phase clinical trial data, includes heterogeneous study designs, and reflects evolving evidence in this rapidly developing field of recurrent glioblastoma therapies.
| Treatment | Phase | N | Primary Endpoint | PFS / PFS-6 | OS / OS-12 | ORR | Major Toxicities | Ref |
|---|---|---|---|---|---|---|---|---|
| DNX-2401 + Pembrolizumab | I/II | 49 | Safety, ORR | PFS improved vs. historical | OS-12: 52.7% (vs. ~20% historical) | 10.4% | Edema, headache, fatigue | 5 |
| Bevacizumab (BV) vs. BV + CPT-11 | II | 167 | PFS-6, OS | 42.6% vs. 50.3% | 9.2 vs. 8.7 mo | Radiographic responses observed | Fatigue, HTN; + diarrhea with CPT-11 | 3 |
| BV + SRS | II | 16 | OS | 68.4% improved PFS vs. historical | 11.73 mo (vs. 8.74 historical) | Not primary | Fatigue, seizures, diarrhea | 6 |
| Pembrolizumab ± BV | II | 80 | PFS, OS | No PFS improvement | 8.8 vs. 10.3 mo | Durable responses in subset | HTN, edema | 7 |
| Nivolumab vs. BV (CheckMate-143) | III | 369 | OS | Shorter PFS with Nivolumab | 9.8 vs. 10.0 mo | Low | Immune toxicity | 2 |
| VB-111 + BV | III | 256 | OS | No PFS improvement | OS-12: 25.3% vs. 24.9% | 27.3% vs. 21.9% | CNS events, flu-like symptoms | 8 |
| Depatux-M + TMZ | II/III | 260 | OS | No early PFS difference | OS-24: 19.8% vs. 5.2% | Modest | Corneal epitheliopathy | 9,10 |
| Nivolumab + RM/TMZ | III | 716 | PFS, OS | 10.6 vs. 10.3 mo | 28.9 vs. 32.1 mo | N/A | High discontinuation | 11 |
| CAR-T (EGFR/IL13Rα2) | I | 6 | Safety | Transient shrinkage | No OS data | Did not meet ORR | Severe neurotoxicity | 12 |
Oncolytic viruses
Oncolytic viruses function by selectively infecting and lysing tumor cells while simultaneously stimulating a local immune response. Viral replication within tumor cells releases tumor antigens, promoting immune cell infiltration and converting an immunologically “cold” tumor microenvironment into one more responsive to immunotherapy.
Oncolytic viruses can convert immunologically ‘cold’ tumors into ‘hot’ tumors by stimulating a local immune response, which highlights the possibility for combination therapy13. DNX-2401 is an engineered oncolytic virus that kills cancer cells and triggers immune responses14. A phase 1 trial showed that it might have some promise5. This trial reports on the first human trial combining pembrolizumab and DNX-2401 for recurrent glioblastoma. In the trial, the treatment was generally well tolerated: there were no deaths caused due to the virus, and the most common side effects were brain edema, headache, and fatigue. The results ended in a 10.4%5 objective response rate (OS-12), compared to a 5% historical control. The primary endpoints were safety and ORR. The trial met its secondary endpoint of 12-month Overall Survival, which was 52.7% compared to the historical 20%, marking a significant improvement. Several patients with objective responses demonstrated durable survival defined by overall survival at 24 months (OS-24). Some of them remained alive well beyond 2 years past treatment. Gene analysis showed that tumors with intermediate immune activity were the most likely to respond to treatment: these patients also experienced longer survival and greater PFS and ORR. Immune cell infiltration increased after treatment, especially in responders, suggesting DNX-2401 can reshape the tumor environment to improve immunotherapy. A T-cell inflamed microenvironment and PD-1 gene expression both are positively correlated with tumor reduction. Overall, this study supported the potential of combining oncolytic viruses with inhibitors in glioblastoma and develops a promising future.
Oncolytic viruses, as a treatment category, offer a new and promising approach to combating glioblastoma by not only destroying tumor cells directly but also drastically transforming the tumor microenvironment to enhance immune response. While individual trials, such as those involving DNX-2401, show modest ORR, they suggest that oncolytic viruses can significantly improve long-term survival when paired with immune checkpoint inhibitors. Their unique ability to heat up otherwise cold tumors possibly opens up new forms of treatment regarding combination therapies. While they only marginally increase ORR, they significantly improve in OS-12 and produce durable responses in a subset of patients suggest that oncolytic viruses could be especially effective when paired with immune checkpoint inhibitors. Overall, oncolytic viruses are an important and evolving strategy in glioblastoma treatment, showcasing the potential to make immunotherapy more effective in a cancer historically resistant to such approaches. Response variability suggests that baseline immune activity strongly influences efficacy, with better outcomes in tumors capable of mounting post-treatment immune infiltration. Modest ORR despite improved OS-12 despite modest objective response rates, indicating immune modulation rather than direct cytolysis as the main driver of benefit.
DNX-2401 combined with pembrolizumab was evaluated in a phase I/II, open-label, single-arm clinical trial involving 49 patients5 with recurrent glioblastoma. The primary endpoints were safety and ORR, with OS as a key secondary endpoint. Outcomes were compared against historical control cohorts, as no randomized comparator arm was included. The study reported an ORR of 10.4%5, compared with approximately 5% in historical rGBM controls, and an OS-12 of 52.7%, compared with an expected historical OS-12 of approximately 20%. Because this was a non-randomized early-phase trial, no p-values or hazard ratios were reported, and the study was not powered for formal statistical comparison. While the improvement in OS-12 suggests a potentially meaningful survival signal, the robustness of these results is modest, and conclusions are limited by the single-arm design and reliance on historical controls rather than a contemporaneous comparison group.
Across oncolytic virus trials, objective response rates remain modest, but select studies demonstrate improved long-term survival compared with historical controls, particularly when combined with immune checkpoint inhibitors. Benefit appears driven by immune modulation rather than direct tumor cytotoxicity, with durable responses limited to immunologically responsive tumors.
Monoclonal antibodies
Bevacizumab exerts its effect by inhibiting vascular endothelial growth factor (VEGF), reducing tumor angiogenesis and vascular permeability. This decreases peritumoral edema and temporarily stabilizes tumor growth, explaining its consistent improvement in PFS without a corresponding improvement in overall survival.
Anti-VEGF therapy and combinations
Bevacizumab, a monoclonal antibody, has shown promise in prolonging survival in several cancers. In a phase II trial3, BV was combined with irinotecan (CPT-11) and improved PFS-6 and ORR in patients3. The patients in the study were randomized to receive either BV or BV + CPT-11 and were treated for up to 104 weeks until disease progression. The primary endpoints of the study were PFS-6 and ORR. Secondary endpoints involved OS, PFS, and the response duration. The median time from the initial diagnosis to study random assignment was 8.6 months for the BV group, compared to 9.8 for the BV + CPT-11 group3. The estimated PFS-6 in the BV group was 42.6%, whereas the PFS rates were 50.3% in the BV+CPT-11 group3. The median PFS rates were 4.2 and 5.6 months, respectively. The median OS rates were 9.2 and 8.7 months3, respectively. The most common side effects for the BV group were fatigue, headache, and hypertension; in the BV+CPT-11 group, fatigue, diarrhea, and nausea. For most patients overall, tumor shrinkage was experienced and the OR’s were durable. The BV was well tolerated. The addition of CPT-11 increased adverse effects but there was no significant decrease in safety15. Bevacizumab alone versus BV combined with CPT-11 was studied in a randomized phase II trial involving 167 patients3 with recurrent glioblastoma. Patients were randomized to receive either BV monotherapy or BV plus CPT-11. The primary endpoints were PFS-6 and OS. The PFS-6 rate was 42.6% in the BV-alone group and 50.3% in the BV+CPT-11 group, while median OS was 9.2 months versus 8.7 months, respectively. Although improvements in radiographic response and PFS were observed, the addition of irinotecan did not result in a statistically significant OS benefit (p > 0.05). These findings demonstrate a modest and clinically limited benefit, with improved disease control but no meaningful survival advantage. Despite modest improvements in PFS and radiographic response, the addition of CPT-11 to BV did not lead to a meaningful OS benefit.
One current approach to managing a recurrent glioblastoma is re-irradiation using intensity-modulated fractionated radiation therapy or SRS6. While standard fractionated radiation only has a median survival extension of 8 months, SRS gives more focused radiation without damaging surrounding healthy tissue. Stereotactic radiosurgery, when combined with BV, a monoclonal antibody targeting VEGF, can improve progression free survival, but OS benefit remains unproven. Glioblastoma remains an aggressive and infiltrative tumor despite the new advancements in treatment. Imaging strategies such as MRIs do not fully capture the tumor’s infiltration. However new strategies such as Magnetic Resonance Spectroscopy (MRS) can identify areas beyond the areas of contrast enhancement. Combining SRS with BV may help enhance treatment success while reducing unintended radiation effects. The trial consisted of patients of 18 and older all with grade 4 glioblastoma who had undergone surgery prior to the test. There were 16 patients in total. Patients underwent SRS, also being guided by an MRI. The radiation varied from person to person and was adjusted based on tumor size, prior radiation, and proximity to critical structures. The patients each underwent MRS 1–14 days before treatment followed by a BV dose (10 mg/kg) one day prior to SRS. The primary endpoint was to assess the efficacy of BV combined with SRS in order to evaluate the OS in patients. Out of the 16 patients, 3 experienced unacceptable toxicity6. There were often fatigue, seizures, and diarrhea as results as well. Median OS was 11.73 months in the BV/SRS group versus 8.74 months historically, compared to the historical control group with 8.74, meaning there was no statistically significant survival benefit of BV/SRS. In the group, 68.4%6showed improvement over the historical control group PFS. The combination of BV with SRS was evaluated in a phase II, single-arm studyincluding 16 adult patients with recurrent or progressive glioblastoma. The primary endpoint was OS, with outcomes compared to a historical control median OS of 8.74 months6. Patients treated with BV plus SRS demonstrated a median OS of 11.73 months6. However, due to the small sample size, absence of a randomized comparator, and lack of formal hypothesis testing, no p-values were reported, and the difference in survival did not reach statistical significance. These results indicate limited robustness, suggesting that while local disease control may improve, the evidence for a true survival benefit remains weak and underpowered. Although SRS combined with BV improved local control and symptoms, the regimen did not produce a statistically significant overall survival advantage.
Immunotherapeutic agents are crucial for treating many cancers, but they don’t always benefit every patient. In particular, phase 3 trials of immunotherapies have not improved survival outcomes in patients with recurrent glioblastoma (rGBM). While the reasons for this remain undetermined, immunosuppressive factors within the tumor microenvironment are likely part of the cause.
Checkpoint inhibitor combinations with bevacizumab
Glioblastoma is characterized by high levels of angiogenesis, largely driven by elevated production of vascular endothelial growth factor (VEGF) in tumor cells7. Bevacizumab, a VEGF-blocking agent, has been shown to improve PFS, but not OS, in these patients. Importantly, VEGF may also contribute to immune suppression16, further complicating treatment outcomes. Pembrolizumab, an immune checkpoint inhibitor, is an antibody used to treat multiple cancers. A recent study found that pembrolizumab slightly improved PFS in rGBM patients7. Notably, one patient with a hypermutated tumor exhibited a dramatic response, prompting further investigation into whether combining VEGF blockade with pembrolizumab could enhance outcomes in recurrent glioblastoma. The research involved patients who had completed at least 28 days post-surgery and 12 weeks of radiation7. Participants were divided into two cohorts: Cohort A received both pembrolizumab and BV, while Cohort B received pembrolizumab alone. Out of the participants, 73 died due to disease progression, while 7 remain under close monitoring. On average, patients in Cohort A completed three treatment cycles, whereas those in Cohort B completed only 1.57. Cohort A patients had median OS of 8.8 months, and 10 of them experienced tumor shrinkage. In comparison, patients in Cohort B had a slightly longer Median OS of 10.3 months. Further analysis showed that within Cohort A, patients using dexamethasone had shorter survival than those who did not. In Cohort B, survival was poorer among patients with an IDH1 mutation. While no treatment-related deaths occurred, 20% of patients in Cohort A developed high blood pressure, and one patient in Cohort B experienced brain swelling. Glioblastoma’s resistance to immunotherapy was found to be primarily due to its robust immunosuppressive mechanisms. The combination of BV and pembrolizumab did not improve PFS compared to BV alone. However, this combination did result in longer-lasting responses as measured by ORR in some patients. It’s worth noting that high doses of BV may also increase hypoxia, which could negatively impact treatment efficacy.
Pembrolizumab combined with BV was evaluated in a randomized phase II trial involving 80 patients2 with recurrent glioblastoma. Participants were randomized to receive either pembrolizumab plus BV or pembrolizumab alone. The primary endpoints included PFS and OS. Median OS was 8.8 months in the combination arm and 10.3 months in the pembrolizumab-only arm7. The difference in survival outcomes between groups was not statistically significant (p > 0.05), and no improvement in PFS was observed with the addition of BV. These results indicate that the combination therapy offers no statistically robust survival benefit, and overall outcomes are best described as negative, despite occasional durable responses in select patients.
Ofranergene Obadenovec (VB-111) is a novel gene therapy that works through vascular disruption and immune activation10. Trials showed that when combined with BV, OS-12 is comparable to BV alone, with no improvement in OS8. In the study, patients were randomized into two groups: one with a combination arm containing VB-111 and biweekly doses of BV, and one solely containing the same dose of BV. The primary endpoint of the study was OS, whereas the secondary endpoints were ORR and PFS. The study found the median OS in the VB-111 + BV arm to be 6.8 months, compared to 7.9 for the BV-only arm. The 12-month survival rate (OS-12) was nearly identical, being 25.3% and 24.9%, respectively. The ORR were 27.3% and 21.9%, respectively. There were more CNS-related adverse events in the combination arm, including seizures, headaches, syncope, and confusion. There was also a higher rate of infusional adverse effects, with 40% occurrence in the combination arm compared to 14% in the control arm. These included fevers, chills, and flu-like symptoms. Overall, there was no significant survival benefit for the VB-111 + BV treatment over BV alone. Both the safety concerns and no improvement in OS or PFS highlight that the need for better rGBM therapies is still imminent.
Glioblastoma has about 13,000 new U.S. cases and 240,000 worldwide annually. It has a median OS rate of less than two years and lacks early detection. Ofranergene Obadenovec is a novel gene therapy that works through vascular disruption and immune activation. Trials showed that when combined with BV, OS-12 is comparable to BV alone, with no improvement in OS. In the study, patients were randomized into two groups: one with a combination arm containing VB-111 and biweekly doses of BV, and one solely containing the same dose of BV. The primary endpoint of the study was OS, whereas the secondary endpoints were ORR and PFS. The study found the median OS in the VB-111 + BV arm to be 6.8 months, compared to 7.9 for the BV-only arm. The 12-month survival rate was nearly identical, being 25.3% and 24.9%, respectively. The objective response rates were 27.3% and 21.9%, respectively. There was also a higher rate of infusional adverse effects, with 40% occurrence in the combination arm compared to 14% in the control arm, including fevers, chills, and flu-like symptoms. The GLOBE trial was a randomized, phase III controlled study8. enrolling 256 patients with recurrent glioblastoma, comparing VB-111 plus BV to BV monotherapy. The primary endpoint was OS. Median OS was 6.8 months in the VB-111+BV arm versus 7.9 months in the BV-alone arm, with no statistically significant difference between groups (p > 0.05). The 12-month survival rates were nearly identical (25.3% vs 24.9%). Given the phase III design and adequate sample size, these findings represent high-quality negative evidence, demonstrating that VB-111 does not provide a survival advantage when added to BV. Overall, there was no significant survival benefit for the VB-111 + BV treatment over BV alone. Both the safety concerns and subpar efficacy highlight that the need for better rGBM therapies is still imminent.
Monoclonal antibodies, especially BV, have emerged as a significant though limited component in the ongoing efforts to treat glioblastoma. For example, multiple clinical trials suggest that while BV consistently improves PFS, it rarely extends the OS in a statistically significant way3. In trials combining BV with agents like irinotecan (CPT-11), SRS, pembrolizumab, or even gene therapies like VB-111, the results have been mixed. While some patients experienced measurable tumor shrinkage and extended progression free survival, these benefits often came with increased toxicity and did not translate into clear improvements in long-term survival. Notably, however, BV enhanced quality of life through improved progression-free survival and reduced steroid dependence for some patients by reducing symptoms and enabling more effective imaging or localized treatment strategies like SRS. However, in studies such as the one pairing BV with pembrolizumab, the combination failed to significantly outperform either drug alone. Similarly, the VB-111 and BV combination showed no survival advantage and actually resulted in more adverse effects. Nevertheless, monoclonal antibodies remain valuable as glioblastoma treatment. They can improve the progression free survival rates, reduce complications, and potentially enhance the efficacy of future therapies. Monoclonal antibodies are promising but not a solution, and there is still a need for treatment models that can consistently provide a longer long-term survival duration. In clinical practice, BV-based regimens are most reasonable when the goal is edema reduction, steroid-sparing, or short-term symptom stabilization rather than survival extension. Anti-VEGF therapy mainly provides symptomatic and short-term disease control rather than durable survival benefit.
Across BV-based regimens, progression-free survival and radiographic response rates improve consistently, while OS rarely changes. Combination strategies increase toxicity without clear survival benefit, indicating that anti-VEGF therapy primarily provides short-term disease control and symptom relief rather than durable survival extension.
Stimulating T-cells through PD-L1 immune checkpoint inhibition
MGMT methylation is a key factor for glioblastoma treatment as it increases sensitivity to TMZ and generally improves survival11. About 35% of glioblastoma patients have a methylated MGMT promoter. Nivolumab, a PD-1 inhibitor, had proven to be effective in other cancers and can also enhance immune responses when used with radiotherapy. Eligible patients for the study all had stage IV glioblastoma and were over the age of 18. In the study, patients were assigned to one of two groups: group 1 received Nivolumab alongside radiotherapy and TMZ. Group 2 received a placebo instead of Nivolumab, also with radiotherapy and TMZ. The primary endpoints of the study were to find PFS and OS rates. The progression-free survival was defined as the time from randomization to progression or death, and OS as the time from randomization to death. The median PFS for group 1 was 10.6 months, whereas the median PFS for group 2 was 10.311. The investigator-assisted PFS was 14.1 for group 1 and 15.2 for group 2. The median OS was slightly better in the placebo arm (32.1 vs. 28.9 months). Toxicity-related discontinuation occurred in 20.8% of patients in the nivolumab group versus 5.1% in the placebo group; progression-related discontinuation occurred in 49.9% of nivolumab patients versus 62.7% of placebo patients11. Overall, the study found that adding Nivolumab to standard therapy did not improve outcomes.
Programmed death-ligand 1(PD-L1) inhibition through drugs like Nivolumab, while effective in other cancers, showed to have a scarcely limited impact in improving outcomes for glioblastoma patients. The addition of Nivolumab to standard treatment with radiotherapy and TMZ did not significantly enhance PFS or OS compared to the placebo group17. Although the drug slightly reduced the rate of progression-related treatment discontinuation, it also caused a much higher rate of toxicity-related discontinuation. In fact, the placebo group had a marginally better OS18, highlighting that the immune stimulation offered by PD-1 inhibition may not be sufficient to overcome glioblastoma’s immunosuppressive environment. These findings suggest that while targeting the PD-1/PD-L1 pathway is a promising strategy in theory, its efficacy in glioblastoma remains unproven. It also highlights the need for more tailored immunotherapies that address the unique biology of brain tumors.
Across both preclinical studies and clinical trials, immune checkpoint inhibitors have consistently failed to generate durable antitumor responses in glioblastoma. Experimental models frequently demonstrate immune activation without sustained tumor regression, a pattern mirrored in large randomized trials where survival outcomes remained unchanged. These parallel failures suggest a disconnect between immune activation and effective tumor control in glioblastoma.
Across immune checkpoint inhibitor trials, PD-1/PD-L1 blockade fails to improve PFS or OS in recurrent glioblastoma despite evidence of immune activation. These results suggest that intrinsic tumor-mediated immunosuppression limits clinical efficacy.
CAR-T Therapies
To explore new glioblastoma treatments, 6 patients with rGBM were treated with chimeric antigen receptor (CAR T) cells, genetically engineered immune cells that target specific tumor antigens, targeting epidermal growth factor receptor (EGFR) and Interleukin-13 Receptor alpha 2 (IL13Rα2) delivered into the spine12. This phase I study was designed to determine the maximum tolerated dose and assess the safety and feasibility of intrathecal CAR-T cell therapy in patients with recurrent glioblastoma, all of whom had multifocal, progressive disease. Although radiographic tumor shrinkage was observed in all six patients shortly after treatment, none met formal objective response criteria. CAR-T cells were detectable in the cerebrospinal fluid following administration, indicating local persistence and biologic activity, including cytokine release. To address tumor heterogeneity and antigen escape, a bivalent CAR-T construct targeting both epidermal growth factor receptor (EGFR) and interleukin-13 receptor alpha-2 (IL13Rα2) was developed. EGFR epitope 806 is expressed in approximately half of rGBM cases and allows tumor-selective targeting, while IL13Rα2 is highly expressed in glioblastoma and represents an additional therapeutic target. Patients received a single intrathecal or intraventricular dose of CAR-T cells following surgical resection19. Neurotoxicity was common, with all patients experiencing moderate to severe neurologic adverse events consistent with immune effector cell–associated neurotoxicity syndrome (ICANS) and tumor inflammation–associated neurotoxicity (TIAN)20. While these toxicities were generally reversible and manageable, their frequency highlights a major limitation of locoregional CAR-T delivery in the central nervous system21. Radiographic responses were rapid but often transient, with some patients demonstrating partial regression and others exhibiting pseudoprogression prior to stabilization, underscoring the challenge of translating early tumor shrinkage into durable clinical benefit.
Intrathecal bivalent CAR-T cell therapy targeting EGFR and IL13Rα2 was evaluated in a phase I, first-in-human study involving 6 patients with recurrent glioblastoma. The primary endpoint was safety and determination of dose-limiting toxicity. No comparator arm was included, and no p-values were reported, as the study was not designed to assess efficacy statistically. All patients demonstrated transient radiographic tumor shrinkage; however, no patients met formal objective response criteria, and significant neurotoxicity was observed. These findings represent proof-of-concept evidence only, with low robustness and no conclusions possible regarding clinical efficacy
In conclusion, CAR T cell treatment might lead to both ICANS and TIAN in patients with rGBM, especially with direct ventricular delivery. However, more patients are needed to better understand neurotoxicity. For patients eligible for investigational therapies, enrollment in clinical trials, particularly those involving CAR-T cells or oncolytic viruses, is generally more appropriate than relying on BV, given their potential for more durable responses. CAR-T therapy shows promise but requires improved targeting and safer delivery to achieve durable benefit.
Immunotherapy is being researched as a potential treatment, as evidence suggests immune cells can function in the central nervous system. Checkpoint inhibitors have also shown promise in models. Nivolumab is a monoclonal antibody which targets the PD-1 checkpoint receptor. Nivolumab was demonstrated to be safe in a phase 1 trial, which led to a phase 3 study which compared nivolumab to BV2. Cohort 2 included patients 18 and older with recurrent stage 4 glioblastoma after initial radiotherapy. The median follow-up for nivolumab was 9.8 months, compared to 9.4 months for BV. There is no significant difference in the OS between nivolumab and BV. The median OS was 9.8 for nivolumab and 10.0 for BV. In addition, the PFS was 1.5 months shorter for nivolumab than BV2. However, nivolumab responses were more durable with a median of 11.1 months compared to 5.3 for BV2. In the trial, nivolumab failed to improve OS compared with BV in patients with recurrent glioblastoma, with median survival remaining comparable between groups. Although nivolumab produced more durable responses in a small subset of patients, the trial did not meet its primary endpoint. Overall, there was no inherent survival benefit of nivolumab.
CAR T cell therapy for glioblastoma has shown potential. In a trial of six patients with rGBM, all demonstrated tumor shrinkage within 24–48 hours, although none met formal objective response criteria. The therapy provoked measurable immune responses, including cytokine release, but also caused moderate to severe neurotoxicities such as confusion, facial weakness, anorexia, fatigue, temporary paralysis, and changes in alertness. One patient required ICU monitoring, and another met dose-limiting toxicity criteria. While symptoms were generally manageable, these findings underscore the risk of neurotoxicity—particularly with direct intrathecal or ventricular delivery—and highlight the need for caution and further refinement. Despite these challenges, CAR T therapy represents a promising approach to overcoming tumor heterogeneity and improving treatment specificity, suggesting potential if toxicity can be better managed in larger trials. Across CAR-T trials, rapid but transient tumor regression is frequently observed alongside significant neurotoxicity. While these studies demonstrate biological activity and feasibility, durable benefit as measured by OS or PFS remains unproven in the absence of larger, controlled trials.
Temozolomide
Epidermal Growth Factor Receptor variants are common in glioblastoma but past treatments that have targeted EGFR haven’t improved outcomes. Deputaxizumab mafodotin (Depatux-M), a new approach, which is an antibody-drug conjugate that targets EGFR, has been promising22. In early trials, Depatux-M produced responses however a main concern was corneal toxicity. Since EGFR amplification is stable, it was used as a biomarker for selecting patients in a controlled and randomized clinical trial testing Depatux-M in recurrent glioblastoma cases. In the trial, patients were assigned to one of three groups: Depatux-M with TMZ, Depatux-M alone, and the control group, which consisted of treatments containing either TMZ or lomustine10. Patients were evaluated via MRI scans, toxicity, side effects, and their health-related quality of life. The primary endpoint was to measure the OS, while secondary endpoints were the PFS and ORR. The goal of the study was to detect an increase in median OS from 7 to 12.9 months22. Out of the 260 patients, 88 patients were assigned to the Depatux-M + TMZ combination arm, 86 to the Depatux-M monotherapy arm, and 86 to the control arm22. Depatux-M’s treatment lasted for 16 weeks in the combination arm and 9 weeks in the monotherapy arm. The most common grade 3-4 toxicity in Depatux-M patients was corneal epitheliopathy, while the control arm primarily experienced hematological toxicities. There were no significant differences in OS or PFS between the Depatux-M group and the control group. However, in the long-term follow-up analysis, the OS difference between the combination and control arms became statistically significant. The OS-24 was 19.8% for the Depatux-M monotherapy, compared to 5.2% for the control group7. The toxicity of Depatux-M showed similar effects to other studies, with grade 3 or 4 corneal epitheliopathy occurring in 25–30% of patients7, however it rarely led to the treatment being discontinued. A similar phase III study6, Intelance I, tested Depatux-M with regular chemotherapy in newly-diagnosed glioblastoma, was discontinued for having no effect, adding doubt for Depatux-M’s efficacy. In conclusion, the trial’s results suggest that Depatux-M combined with TMZ may have a role in treating EGFR-amplified recurrent glioblastoma, however the negative outcome of Intelance I raises further concerns.
Around 50% of glioblastomas show EGFR amplification and about 25% have the EGFRvIII mutation10. Current EGFR therapies, such as antibodies and vaccines, are very ineffective against glioblastoma. Depatuxizumab mafodotin (Depatux-M) is an antibody-drug that targets activated EGFR and EGFRvIII. It works by binding to the receptor and then releasing a toxin that kills the tumor cell. It differs from other therapies because it doesn’t cause common side effects such as rash and diarrhea. Preclinical and early clinical studies showed promising results and led to two clinical trials: INTELLANCE-2, with Depatux-M and TMZ, and INTELLANCE-1, which tested Depatux-M in newly diagnosed glioblastoma. A common side effect was corneal epitheliopathy. The primary endpoint was OS. The secondary endpoints were progression-free survival and neurocognitive function. In the placebo group, the median OS was projected to be 16 months, whereas in the Depatux-M group it was hypothesized to be 21.3 months. However, in reality, the Depatux-M OS was 18.9 months, whereas the placebo was 18.7 months. There was little to no difference in OS durations. Depatux had an average PFS of 8 months, whereas the placebo group had an average duration of 6.3 months, displaying a modest improvement in PFS. 94% of patients in the Depatux-M group experienced any grade of corneal epitheliopathy, whereas only 36% faced it in the placebo group. While Depatux-M showed some progression-free survival benefits in patients, it failed to improve OS which was the key endpoint.
Temozolomide remains a standard component of glioblastoma therapy, often used in combination with newer experimental treatments like Depatux-M. Although Depatux-M initially showed promise in early-phase studies and preclinical models—particularly for EGFR-amplified or EGFRvIII-mutated glioblastomas—its clinical performance has been mixed. In the INTELLANCE-2 trial, the combination of Depatux-M and TMZ resulted in a significant increase in its two-year survival rates compared to historical control groups. However, other trials such as INTELLANCE-1 failed to demonstrate meaningful improvements in OS, which casts doubt on the drug’s efficacy in other cases. A consistent challenge across studies has been the high incidence of corneal toxicity, which while rarely leads to treatment discontinuation, still remains a significant concern for patient quality of life. Ultimately, while Depatux-M combined with TMZ shows potential in some specific contexts, particularly in recurrent glioblastoma with EGFR amplification, it has not yet demonstrated consistent or highly effective benefits across broader patient populations. These results suggest that although EGFR remains a valid target, further refinement of its methods and an increase of patient selection for study is necessary before EGFR-targeted therapies can become reliable standards of care.
Across EGFR-targeted ADC trials, modest improvements in progression-free survival are offset by limited overall survival benefit and substantial ocular toxicity. These findings suggest that EGFR-directed strategies may benefit select molecular subgroups but are unlikely to broadly improve outcomes. Two additional pivotal trials in recurrent GBM include REGOMA, which compared regorafenib to lomustine23, and EF-11, which compared tumor treating fields (TTFields) to physician’s-choice chemotherapy24.
Conclusion
While no single therapy has yet emerged as a definitive solution for recurrent glioblastoma, this review highlights several promising approaches. CAR-T cell therapies targeting EGFR and IL13Rα2 have shown promising early signs of tumor regression, however neurotoxicity remains a challenge. Oncolytic viruses like DNX-2401 offer encouraging safety profiles and potential immune activation. Among the treatments examined, combinations involving BV, especially with checkpoint inhibitors like pembrolizumab, appear to offer the most consistent benefits in prolonging PFS. While BV-based combinations reliably reduce edema and prolong PFS, they have not demonstrated an OS benefit, and their clinical impact remains modest25. Ultimately, a better treatment for glioblastoma is still needed: continued clinical research is essential to refine these strategies and improve outcomes for patients facing this aggressive cancer.
References
- Hanahan, D., & Weinberg, Robert A. (2011). Hallmarks of cancer: the next Generation. Cell, 144(5), 646–674. https://doi.org/10.1016/j.cell.2011.02.013 [↩]
- Reardon, D. A., Brandes, A. A., Omuro, A., Mulholland, P., Lim, M., Wick, A., Baehring, J., Ahluwalia, M. S., Roth, P., Bähr, O., Phuphanich, S., Sepulveda, J. M., De Souza, P., Sahebjam, S., Carleton, M., Tatsuoka, K., Taitt, C., Zwirtes, R., Sampson, J., & Weller, M. (2020). Effect of Nivolumab vs Bevacizumab in Patients With Recurrent Glioblastoma: The CheckMate 143 Phase 3 Randomized Clinical Trial. JAMA Oncology, 6(7), 1003–1010. https://doi.org/10.1001/jamaoncol.2020.1024 [↩] [↩] [↩] [↩] [↩]
- Friedman, H. S., Prados, M. D., Wen, P. Y., Mikkelsen, T., Schiff, D., Abrey, L. E., Yung, W. K. A., Paleologos, N., Nicholas, M. K., Jensen, R., Vredenburgh, J., Huang, J., Zheng, M., & Cloughesy, T. (2009). Bevacizumab Alone and in Combination With Irinotecan in Recurrent Glioblastoma. Journal of Clinical Oncology, 27(28), 4733–4740. https://doi.org/10.1200/jco.2008.19.8721 [↩] [↩] [↩] [↩] [↩] [↩] [↩] [↩] [↩]
- R. G. W. Verhaak, K. A. Hoadley, E. Purdom, et al. Integrated genomic analysis identifies clinically relevant subtypes of glioblastoma. Cancer Cell, 17(1), 98–110, 2010. [↩]
- Nassiri, F., Patil, V., Yefet, L. S., Singh, O., Liu, J., Dang, R. M. A., Yamaguchi, T. N., Daras, M., Cloughesy, T. F., Colman, H., Kumthekar, P. U., Chen, C. C., Aiken, R., Groves, M. D., Ong, S. S., Ramakrishna, R., Vogelbaum, M. A., Khagi, S., Kaley, T., & Melear, J. M. (2023). Oncolytic DNX-2401 virotherapy plus pembrolizumab in recurrent glioblastoma: a phase 1/2 trial. Nature Medicine, 29, 1–9. https://doi.org/10.1038/s41591-023-02347-y [↩] [↩] [↩] [↩] [↩]
- Mantica, M., Drappatz, J., Lieberman, F., Hadjipanayis, C. G., Lunsford, L. D., & Niranjan, A. (2023). Phase II study of border zone stereotactic radiosurgery with bevacizumab in patients with recurrent or progressive glioblastoma multiforme. Journal of Neuro-Oncology, 164(1), 179–190. https://doi.org/10.1007/s11060-023-04398-0 [↩] [↩] [↩] [↩] [↩] [↩]
- Nayak, L., Molinaro, A. M., Peters, K., Clarke, J. L., Jordan, J. T., de Groot, J., Nghiemphu, L., Kaley, T., Colman, H., McCluskey, C., Gaffey, S., Smith, T. R., Cote, D. J., Severgnini, M., Yearley, J. H., Zhao, Q., Blumenschein, W. M., Duda, D. G., Muzikansky, A., & Jain, R. K. (2021). Randomized Phase II and Biomarker Study of Pembrolizumab plus Bevacizumab versus Pembrolizumab Alone for Patients with Recurrent Glioblastoma. Clinical Cancer Research, 27(4), 1048–1057. https://doi.org/10.1158/1078-0432.ccr-20-2500 [↩] [↩] [↩] [↩] [↩] [↩]
- T. Cloughesy, A. Brenner, J. de Groot, N. Butowski, L. Zach, J. Campian,733 B. Ellingson, L. Freedman, Y. Cohen, N. Lowenton-Spier, T. Rach-734 milewitz Minei, S. Fain Shmueli, P. Wen, N. Avgeropoulos, J. Beck,735 T. Benkers, F. Bokstein and E. Burton, A randomized controlled phase736 III study of VB-111 combined with bevacizumab vs bevacizumab737 monotherapy in patients with recurrent glioblastoma (GLOBE). Neuro-738 Oncology, 22(5), 705–717, 2019. https://doi.org/10.1093/739 neuonc/noz232. [↩] [↩] [↩]
- Lassman, A. B., Pugh, S. L., Wang, T. J. C., Aldape, K., Gan, H. K., Preusser, M., Vogelbaum, M. A., Sulman, E. P., Won, M., Zhang, P., Moazami, G., Macsai, M. S., Gilbert, M. R., Bain, E. E., Blot, V., Ansell, P. J., Samanta, S., Kundu, M. G., Armstrong, T. S., & Wefel, J. S. (2022). Depatuxizumab mafodotin in EGFR-amplified newly diagnosed glioblastoma: a phase III randomized clinical trial. Neuro-Oncology, 25(2). https://doi.org/10.1093/neuonc/noac173 [↩]
- Martin, Eoli, M., Juan Manuel Sepúlveda, Smits, M., Annemiek Walenkamp, Jean-Sebastian Frenel, Franceschi, E., Clément, P. M., Olivier Chinot, Filip, Whenham, N., Sanghera, P., Weller, M., Hendrik Jan Dubbink, French, P. J., Looman, J., Dey, J., Krause, S., Ansell, P., & Nuyens, S. (2019). INTELLANCE 2/EORTC 1410 randomized phase II study of Depatux-M alone and with temozolomide vs temozolomide or lomustine in recurrent EGFR amplified glioblastoma. Neuro-Oncology, 22(5), 684–693. https://doi.org/10.1093/neuonc/noz222 [↩] [↩] [↩]
- Lim, M., Weller, M., Idbaih, A., Steinbach, J., Finocchiaro, G., Raval, R. R., Ansstas, G., Baehring, J., Taylor, J. W., Honnorat, J., (2022). Phase III trial of chemoradiotherapy with temozolomide plus nivolumab or placebo for newly diagnosed glioblastoma with methylated MGMT promoter. Neuro-Oncology, 24(11), 1935–1949. https://doi.org/10.1093/neuonc/noac116 [↩] [↩] [↩] [↩]
- Bagley, S. J., Logun, M., Fraietta, J. A., Wang, X., Desai, A. S., Bagley, L. J., Nabavizadeh, A., Jarocha, D., Martins, R., Maloney, E., Lledo, L., Stein, C., Marshall, A., Leskowitz, R., Jadlowsky, J. K., Christensen, S., Oner, B. S., Plesa, G., Brennan, A., & Gonzalez, V. (2024). Intrathecal bivalent CAR T cells targeting EGFR and IL13Rα2 in recurrent glioblastoma: phase 1 trial interim results. Nature Medicine, 1–10. https://doi.org/10.1038/s41591-024-02893-z [↩] [↩]
- Russell, S. J., Peng, K.-W., & Bell, J. C. (2012). Oncolytic virotherapy. Nature Biotechnology, 30(7), 658–670. https://doi.org/10.1038/nbt.2287 [↩]
- Gilbert, M. R., Wang, M., Aldape, K., Lassman, A., Sorensen, A. G., Mikkelson, T., Groves, M., Werner-Wasik, M., Regine, W., & Mehta, M. (2009). RTOG 0625: A phase II study of bevacizumab with irinotecan in recurrent glioblastoma (GBM). Journal of Clinical Oncology, 27(15_suppl), 2011–2011. https://doi.org/10.1200/jco.2009.27.15_suppl.2011 [↩]
- Batchelor, T. T., Sorensen, A. G., di Tomaso, E., Zhang, W.-T., Duda, Dan G., Cohen, K. S., Kozak, K. R., Cahill, D. P., Chen, P.-J., Zhu, M., Ancukiewicz, M., Mrugala, M. M., Plotkin, S., Drappatz, J., Louis, D. N., Ivy, P., Scadden, David T., Benner, T., Loeffler, J. S., & Wen, P. Y. (2007). AZD2171, a Pan-VEGF Receptor Tyrosine Kinase Inhibitor, Normalizes Tumor Vasculature and Alleviates Edema in Glioblastoma Patients. Cancer Cell, 11(1), 83–95. https://doi.org/10.1016/j.ccr.2006.11.021 [↩]
- Jain, R. K. (2005). Normalization of Tumor Vasculature: An Emerging Concept in Antiangiogenic Therapy. Science, 307(5706), 58–62. https://doi.org/10.1126/science.1104819 [↩]
- Jackson, C. M., Choi, J., & Lim, M. (2019). Mechanisms of immunotherapy resistance: lessons from glioblastoma. Nature Immunology, 20(9), 1100–1109. https://doi.org/10.1038/s41590-019-0433-y [↩]
- Lim, M., Xia, Y., Bettegowda, C., & Weller, M. (2018). Current State of Immunotherapy for Glioblastoma. Nature Reviews Clinical Oncology, 15(7), 422–442. https://doi.org/10.1038/s41571-018-0003-5 [↩]
- Brown, C. E., & Mackall, C. L. (2019). CAR T cell therapy: inroads to response and resistance. Nature Reviews Immunology, 19(2), 73–74. https://doi.org/10.1038/s41577-018-0119-y [↩]
- Neelapu, S. S., Tummala, S., Kebriaei, P., Wierda, W., Gutierrez, C., Locke, F. L., Komanduri, K. V., Lin, Y., Jain, N., Daver, N., Westin, J., Gulbis, A. M., Loghin, M. E., de Groot, J. F., Adkins, S., Davis, S. E., Rezvani, K., Hwu, P., & Shpall, E. J. (2018). Chimeric antigen receptor T‑cell therapy — assessment and management of toxicities. Nature Reviews Clinical Oncology, 15(1), 47–62. https://doi.org/10.1038/nrclinonc.2017.148 [↩]
- Arvanitis, C. D., Ferraro, G. B., & Jain, R. K. (2019). The blood–brain barrier and blood–tumour barrier in brain tumours and metastases. Nature Reviews Cancer, 20(1). https://doi.org/10.1038/s41568-019-0205-x [↩]
- Lassman, A. B., Pugh, S. L., Wang, T. J. C., Aldape, K., Gan, H. K., Preusser, M., Vogelbaum, M. A., Sulman, E. P., Won, M., Zhang, P., Moazami, G., Macsai, M. S., Gilbert, M. R., Bain, E. E., Blot, V., Ansell, P. J., Samanta, S., Kundu, M. G., Armstrong, T. S., & Wefel, J. S. (2022). Depatuxizumab mafodotin in EGFR-amplified newly diagnosed glioblastoma: a phase III randomized clinical trial. Neuro-Oncology, 25(2). https://doi.org/10.1093/neuonc/noac173 [↩] [↩] [↩]
- A. Lombardi, A. De Salvo, F. Brandes, M. Tosoni, R. Spena, M. Faedi, A. Bartolini, C. Fabi, S. Bianconi, & G. Ermani. REGOMA: regorafenib versus lomustine in patients with recurrent glioblastoma. The Lancet Oncology, 19(1), 110–119 (2018). https://doi.org/10.1016/S1470-2045(18)30675-2 [↩]
- L. Stupp, A. Wong, R. Kanner, M. Steinberg, G. S. Gahramanov, & H. Mason. EF-11: tumor treating fields versus physician’s-choice chemotherapy in recurrent glioblastoma. European Journal of Cancer, 48(2), 219–226 (2012). https://doi.org/10.1016/j.ejca.2012.04.011 [↩]
- Weller, M., Wick, W., Aldape, K., Brada, M., Berger, M., Pfister, S. M., Nishikawa, R., Rosenthal, M., Wen, P. Y., Stupp, R., & Reifenberger, G. (2015). Glioma. Nature Reviews. Disease Primers, 1(1), 15017. https://doi.org/10.1038/nrdp.2015.17 [↩]


