
Revathi Dinesh1, Ollie Fegter1
1 Wayzata High School, Minnesota, USA
Abstract
Background: Dementia affects countless people worldwide, and current treatments lack components for a well rounded recovery which urges research to delve into alternative remedies. Numerous native plant species have been used for their probable cognitive benefits in dementia treatment.
Terms: Throughout this paper, the treatments included are described as native plant-derived. This signifies that the treatment was derived from a plant native to the earth. Essentially, it is not human synthesized. This signifies that the treatment is native to the earth rather than being human synthesized.
Methods and Results: To discover the impact several native plants had on regaining cognition, a systematic review was conducted by reviewing trials through the database PubMed applying specific search terms and meSH terms including medicinal plants, phytotherapy, cognitive dysfunction, cognition disorders, and humans. The articles were first screened by title and abstract through Rayyan to include 146 articles out of 753 search results. Any articles which didn’t include administration of the plant-derived treatment, target population, or correct publication type were excluded. Rayyan was then used for full text screening in which articles were sorted out by relevance, outcome, and study size leading to a final grouping of 15 articles. Through the findings, many plants were discovered to have significant effects on improvement of cognitive function.
Conclusion: This review summarizes various plant-derived treatments that have been proven effective in reducing cognitive decline. As these treatments have been significant in different populations, this review suggests an approach to dementia prevention through plant species native to the earth. With scientists further developing these treatments to adapt to populations globally, these results could be amplified to make a significant improvement in dementia prevention. This review aids in providing confirmation that these plant-based treatments have been successful, and it acts as a foundation for further research.
Introduction
Cognition is recognized as the ability to attain knowledge and function through past experiences, thoughts, and senses. Multiple components of cognition exist including memory, language, and attention. Most frequently, treatments focus on either overall cognition or memory. Although cognitive decline can begin as early as midlife, it is more commonly seen in older adults. At around seventy years old, the average age, approximately two out of three Americans undergo some cognitive decline1. This is simply in America; worldwide, cognitive decline happens to an incredible amount of people at this age. Subjective cognitive decline can often lead to further cognitive impairment. Whether it’s mild impairment or a development of dementia, perceived cognitive impairment can convert into a greater problem. In 2021, 57 million people worldwide had dementia2. It has also been approximated that 5% to 8% of people over the age of 65 have some sort of dementia3.
Mild cognitive impairment (MCI) is the stage of cognitive impairment in between normal cognition and dementia4. The symptoms include slight loss of memory, language, and judgment. For instance, the patient could be forgetful, indecisive, or unable to converse. The impact can be enough for the person and family to understand that there is a problem; however, it wouldn’t affect their daily tasks. MCI can increase the risks of attaining dementia through Alzheimer’s disease or other pathologies. The risk of progressing to dementia after receiving an MCI diagnosis increased by (2.3) times5.
Dementia is a syndrome which is caused by diseases like Alzheimer’s that eliminates neurons over time resulting in a decline in cognition. Suffering from dementia would make it difficult to complete regular activities, remember important events, and keep track of time and direction. The symptoms differ depending on the person, but as the dementia progresses, the person will need assistance in their daily life. Unfortunately, once dementia begins, the cognition continually declines until death.
Alzheimer’s Disease (AD) is the most common cause of dementia. Alzheimer’s disease is the process of neurofibrillary tangles and proteins in the form of amyloid plaques accumulating in the brain resulting in the brain cells shrinking6. Neurofibrillary tangles occur when there is an excess of tau proteins in the brain. Tau proteins end up detaching from the neurons and tangle together to form neurofibrillary tangles. Amyloid plaques occur when proteins clump together which becomes excessive in the brain during Alzheimer’s disease to disrupt cell function7.
Currently, there are no treatments to prevent cognitive decline in dementia patients. Treatments, both pharmacological and non-pharmacological, exist but don’t completely improve cognitive decline. Instead, they focus on small aspects of dementia. A Lancet Report suggests that 45% of dementia risk factors are modifiable8. Among the pharmacological treatments, anti-amyloid treatments are used to remove the beta-amyloid plaques which have formed in the brain. Such treatments allow dementia patients to complete daily tasks without requiring assistance. Donanemab and Lecanemab are two examples of anti-amyloid treatments. Another pharmacological treatment commonly used are drugs like cholinesterase inhibitors (prevent breakdown of acetylcholine), glutamate receptors (regulating glutamate), or a combination of the two. Donepenzil, Benzgalantamine, Galantamine, and Rivastigmine are the more commonly prescribed cholinesterase inhibitors. Memantine is the drug used to regulate the activity of glutamate. Combining Donepezil and memantine provides the drug with both a cholinesterase inhibitor and glutamate regulator9. In addition to pharmacological treatments, nonpharmacological treatments are used. These therapies include small interventions that people do everyday. Memory training, art or music therapy, aromatherapy, contact with animals, psychosocial activation, and physical exercise are all methods used to increase cognitive ability10. Depending on the patient’s symptoms, some therapies might work better or worse.
These trials have been conducted to find minor treatments for cognitive decline. Treatments have been found for patients suffering from dementia, MCI, or even normal adults to help slow down their cognitive decline. However, these treatments are rooted in a Western medical model and don’t integrate native/Eastern medical practices. As an underresearched treatment, it may be beneficial to consider the potential of native/Eastern medical practices in preventing or slowing cognitive decline. These treatments are often based on native plant species. There are many plant species out there which can be used as a part of the solution. For example, Ginkgo biloba is a plant species which has been thoroughly studied. The specific extract EGb 761 is widely used for remedies in cognitive impairment11. There are other treatments being done, but they aren’t getting enough recognition. Researchers have conducted trials on various treatments to aid in cognitive decline, but they are dispersed and unrecognized. This systematic review aims to group multiple successful trials of native plant treatments to bring recognition. The current pharmacological treatments aren’t working, but with more awareness of these native plant treatments, they can be implemented to create a significant improvement in dementia prevention.
The articles in the grouping all involve an administration of a native plant-derived treatment. The purpose of this review paper was to identify native plant-derived treatments which have been successful in improving cognition, so every treatment included prominently has had successful results. Ginkgo biloba has been tested multiple times which is reported in this review as five trials for Ginkgo biloba were included. However, as it is a widely studied treatment, there have been studies where the Ginkgo biloba was unable to benefit cognition and there was no statistical significance of the treatment. One such article of Ginkgo biloba is included in this review to demonstrate the differing results of its effectiveness. It is important to note that that article was different from the other articles because it tested for the progression rate towards Alzheimer’s disease instead of improvement in cognition. Although it can be inferred that Alzheimer’s disease was reached in the trial because the cognition didn’t increase, it is a necessary distinction between the treatments. The other trials involving different native plant-derived treatments were more niche as there were few trials conducted with those treatments. However, they have been proved to increase cognition. They arise from different backgrounds whether they are from ancient methods like Traditional Chinese Medicine (TCM), Ayurveda, or traditional Korean medicine, or also basic remedies like aromatherapy from citrus scents or eucalyptol. There are many other treatments involved, but all of them have been proven to improve cognition. There have been less treatments towards these native plant-derived treatments because many people don’t understand the significance that these treatments could have. By grouping them all together and analyzing their importance, more recognition will be passed to these treatments.
Methods
Data were collected by searching for articles in PubMed. Specific search terms included free-text terms and meSH terms. The final search term was as follows: (“medicinal plants”[MeSH Terms] OR “phytotherapy”[MeSH Terms] OR “botanical medicine” OR “traditional medicine” OR “herbal remedy” OR “plant-based treatment”) AND (“cognitive decline” OR “cognitive dysfunction”[MeSH Terms] OR “cognition disorders”[MeSH Terms] OR “mild cognitive impairment” OR dementia) AND (improve* OR enhanc* OR slow* OR prevent* OR treat*) AND (“Humans”[MeSH Terms]) AND English[lang].
Articles were screened using Rayyan, an online systematic review platform, in two steps. For both steps, two reviewers screened the articles. The first reviewer filtered through every article and did initial screening. When the first reviewer was unsure about an article, the second reviewer assisted with the screening. The second reviewer would reiterate the exclusion and inclusion criteria created by the first reviewer to ensure that the screening was aligned with the criteria. Whenever the reviewers disagreed about the inclusion or exclusion of an article, they carefully discussed the exclusion and inclusion criteria and read through the abstract together to make a decision that both agreed on. The first step was to screen by title and abstract. Articles with the following characteristics were excluded: 1) any article that did not include actual administration of a specific treatment, (e.g., systematic review, editorial, and literature review); 2) studies with non-human populations (e.g., mice); 3) treatments including drugs that were not derived from plants; 4) an outcome that did not slow cognitive decline or improve cognition. However, if the article included a negative outcome of a treatment which had already been included, it was included to remove bias and show the differing results of the treatment. The following were inclusion criteria for the articles: 1) articles with administration of the treatment; 2) a population of humans; 3) natural plant-derived treatments; 4) an outcome which slowed cognitive decline or improved cognition; 5) articles with a title but without an abstract to ensure a comprehensive screening process at the full-text stage. Multiple articles reviewed during the title and abstract screening didn’t display an abstract through PubMed, but the reviewers felt it would be inaccurate to exclude potential relevant articles for lack of an abstract. If the title was relevant to the remaining exclusion criteria, it was included in the full text screening.
The final screening was done by reading the full text. In order to do so, PDFs of the included articles were uploaded to Rayyan. There, the entire article was screened whether to be included or excluded in the final grouping. In this step, the first reviewer was unable to access some of the articles, so the second reviewer uploaded the PDFs to aid in the selection of the articles. In the overall grouping, multiple articles were trials conducted for the same treatment, so all trials relative to that treatment were included to either demonstrate its prominence for being vastly studied, or to balance out positive and negative results to reduce bias. The same exclusion criteria were used for the full text screening with a few additions: 1) patients undergoing treatment without suffering from a type of dementia or being in a stage with mild dementia or mild cognitive impairment; 2) positive outcomes without cognition; 3) full text must be accessible. Similarly, the inclusion criteria follow: 1) a population of patients with mild cognitive impairment, a type of dementia, Alzheimer’s disease, or at a senior center; 2) outcomes with an increase in cognition; 3) access to the full text. Accessibility was a major constraint in the selection of the articles because multiple articles were unavailable without institutional access or unavailable through their journal. However, these problems were addressed through contacting the authors of the papers.
Once the articles were chosen, data was extracted in the form of a table. In the table, the author, population, treatment, outcome, and efficacy were noted down for each article. The population was different for each article since some focused on patients with mild cognitive impairment, Alzheimer’s disease, a specific dementia, or even no cognitive impairment. Efficacy was noted by observing the p-values, determining statistical significance, and comparing the absolute score changes.
Results
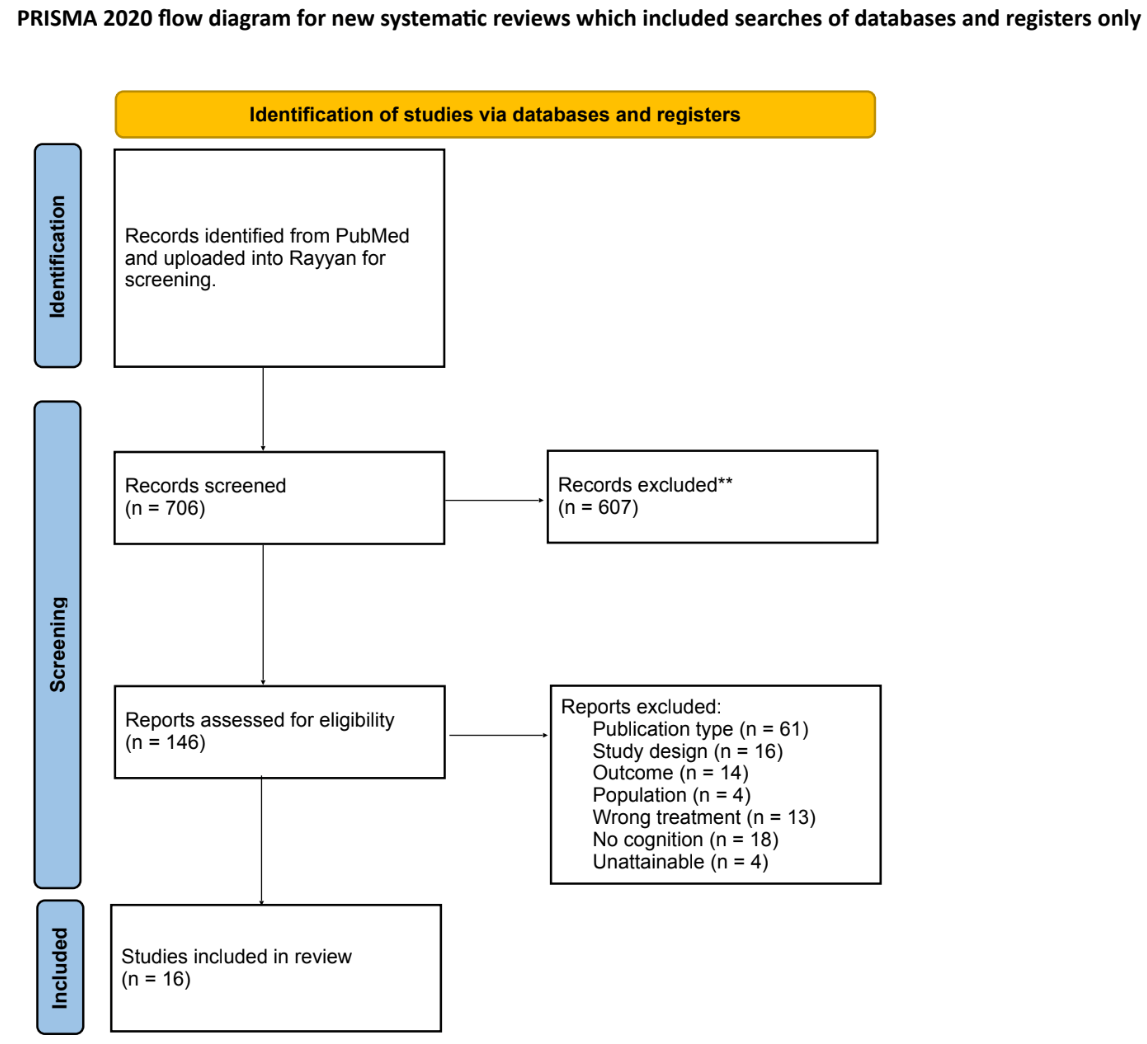
This search returned 753 total articles. The title and abstract screening reduced the total number of articles to 146 that were then screened by full text. After the full text screening, the final grouping of articles included 16 articles. Articles were excluded based on the following reasons: wrong publication type, wrong study design, wrong population, wrong drug, wrong outcome, background article, and being inaccessible. The whole process is demonstrated in Figure 1.
The 607 articles excluded during the title and abstract screening were ineligible for the following reasons. 376 articles were excluded from the full text screening because they weren’t in the format of the desired article (i.e. systematic review, editorial, or literature review). 75 articles were excluded from the full text screening because they had the wrong study design (i.e. protocols). 61 articles were excluded from the full text screening because the result did not include a cognitive increase. 40 articles were excluded from the full text screening because they had a population other than humans (i.e. mice, or lab experiments on cells). 33 articles were excluded from the full text screening because they did not present primary data, but rather they aided in background information (i.e., narrative review). 22 articles were excluded from the full text screening because they included treatments with a drug administered or various methods without the administration of a native plant based treatment.
The 130 articles excluded during the full text screening phase were excluded for the following reasons. 61 articles were excluded for being of the wrong publication type (i.e. editorials, systematic reviews, or educational articles). 16 articles were excluded for having the wrong study design (i.e. protocols). 14 articles were excluded for including the wrong outcome (i.e. no significant change in cognition). 4 articles were excluded for using the wrong population (i.e. mice). 13 articles were excluded for using the wrong drugs or treatment (i.e. traditional methods without native species use (exercise focused) or a drug based treatment). 18 articles were excluded for not being relevant to cognition. 4 articles were excluded for not being accessible as they were unavailable and the authors did not provide the paper upon request.
A summary of the final included articles is presented in Table 1.
The specific findings of each article are listed in Table 2.
| Study | Plant Species/Intervention | Population | Findings |
| D. Choudhary et al.,12. | Ashwagandha root extract. | Adults over the age of 35 with MCI in Pune, India (N=50). | Improved memory and cognition compared to the control group. Mini Mental State Examination (MMSE) was used to test cognition. |
| D. Jimbo et. al.,13. | Aromatherapy with lemon, rosemary, lavender, and orange essential oils. | Dementia patients with an age range of 80-95 in Japan (N=28). | Significance in improvement overall (p<0.05). Functional Assessment Staging of Alzheimer’s disease (FAST) and Touch Panel-type Dementia Assessment Scale (TDAS) were used to test cognition. |
| M. Delfan et al.,14. | Bacopa monnieri capsules. | Patients with MCI over the age of 50 in Lorestan County (N=62). | Overall significant improvement for cognition (p<0.001). Montreal Cognitive Assessment (MoCA) was used to test cognition. |
| J. Shi et al.,15. | Conventional therapy with herbal medicine in comparison to only conventional therapy. This was a part of Traditional Chinese Medicine (TCM). | Alzheimer’s disease patients in China (N=344). | Significant improvement in CT + H group in comparison to CT group. After 18 months (p=0.002). After 24 months (p<0.001). MMSE was used to test cognition. |
| D. Chowdhury et al.,16. | Film-coated tablet containing 120 mg EGb 761 (the specific Ginkgo biloba extract). | Adults with a major neurocognitive disorder over the age of 50 in India (N=150). | Consortium to Establish a Registry for Alzheimer’s Disease (CERAD) recall of CP (p<0.0001). |
| O. Băjenaru et al.,17. | Ginkgo biloba extract, EGb 761. | MCI patients over the age of 50 in Romania (N=500). | Significant improvement in cognition (p<0.0001). MMSE was used to test cognition. |
| S. Goto et al.,18. | Eucalyptol oil. | Individuals with a disability in a senior center in Japan (N=70). | There was significant improvement in one group (p=0.002). MMSE was used to test cognition. |
| S. I. Gavrilova et al.,19. | Ginkgo biloba tablets containing 240 mg of EGb 761. | MCI patients in Russia over the age of 55 in Russia (N=159). | There was a significant improvement in cognition (p<0.05). The Trail-Making Test (TMT-A or TMT-B) was used to test cognition. |
| R. Krikorian et al.,20. | Daily consumption of grape juice. The amount varied per weight. | Adults with a mean age of 78 who have early memory decline in the USA (N=12). | There was a significance in cognitive improvement (p=0.04). The California Verbal Learning Test (CVLT) was used to test cognition. |
| M. Tsolaki et al.,21. | Crocus sativus; dose unspecified. | Participants had MCI with a mean age of 70 years (N=35). | There was a significance in cognitive improvement (p=0.05). MMSE and MoCA were used to test cognition. |
| S.-T. Lee et al.,22. | White ginseng powder that was put into a capsule. | Patients with Alzheimer’s disease with an age range of 47-83 years in South Korea (N=97). | Yes, there was a significant improvement in cognition (p=0.029, and p=0.009). MMSE and Alzheimer’s Disease Assessment Scales (ADAS) were used to test cognition. |
| S. Akhondzadeh et al.,23. | Salvia officinalis Extract. 60 drops per day. | Patients having earlier Alzheimer’s disease with an age range of 65-80 years in Iran (N=39). | Yes, there was a significant increase in cognition (p<0.0001). ADAS was used to test cognition. |
| S. Akhondzadeh et al.,24. | Melissa officinalis extract 60 drops/day. | Patients of mild to moderate Alzheimer’s disease with an age range of 65-80 years old in Tehran, Iran (N=35). | Yes, significant cognitive improvement over time (p<0.0001). ADAS was used to test cognition. |
| A. R. Whyte et al.,25. | Wild blueberry extract capsules. The participants took 2 capsules daily. | The study included adults with normal and healthy habits with an age range of 65-80 years old (N=112). | Yes, there was a significance in the difference between the treatment group and placebo (p=0.038). The Reys Auditory Verbal Learning Task (RAVLT) was used to test cognition. |
| S. T. DeKosky et al.,26. | Ginkgo biloba tablets containing 120mg, twice a day. | Participants were adults over the age of 75 years old with prevalent dementia in the United States (N=3069). | No, there was not a significance in the difference between the treatment groups and placebo as both groups developed dementia. The Modified Mini-Mental State Examination (3MSE) and ADAS-cog (cognitive subscale of ADAS) were used to test cognition. |
| B. E. Snitz et al.,27. | Ginkgo biloba tablets containing 120mg, twice a day. | Participants were adults with prevalent dementia from 4 communities in the United States (N=3069). | No, there was no significance between the treatment and placebo groups as both developed dementia. 3MSE and ADAS-cog were used to test cognition. |
| Study | Results (p-values and absolute score changes) |
| D. Choudhary, S. Bhattacharyya & S. Bose (2017). | Logical memory I (p = 0.007), logical memory II (p = 0.006), verbal paired associates II (p = 0.031). In logical memory I, the Wechsler Memory Scale (WMS-III India) reported approximately a +4.12 change in the Ashwagandha group from the baseline score of 8.62 to the week 8 score of 12.74. This is much greater than the change of the placebo group which went from a baseline score of 9.00 to a week 8 score of 11.04 which is only a +2.04 change. Similarly, in logical memory II the approximate change of the ashwagandha group was +3.88 (baseline score of 7.50 to week 8 score of 11.38) while the placebo group was only +1.77 (baseline score of 7.73 to week 8 score of 9.50), which shows statistical significance. Finally in verbal paired associated II, the approximate change of the ashwagandha group was +1.58 (baseline score of 9.21 to week 8 score of 10.79) while the placebo group’s change was about +0.54 (baseline score of 8.65 to week 8 score of 9.19). |
| D. Jimbo et al. (2009). | All patient groups (p<0.05), AD group (p<0.01). |
| M. Delfan et al. (2024). | Total change in cognition score was significant (p<0.001). The cognitive impairment overall score of the control group at the zero-day mean was 20.06 and the second month mean score was 21.93 which has approximately a +1.87 change. The cognitive impairment overall score of the intervention group was 20.16 and the second month mean score was 24.80 which has approximately a +4.62 change which is a significant difference from the control group. |
| J. Shi et al. (2017). | Patients treated in the CT + H group became significantly more stable in 12 months in comparison to the CT group (p = 0.012). Similarly, CT + H patients improved in comparison to CT patients after 18 months (P = 0.002). After 24 months, 33.33% of CT + H patients improved in MMSE while only 7.69% of CT patients improved MMSE (p=0.02). In addition, only 16.67% of patients in the CT + H group experienced a decrease in MMSE in comparison to the 65.38% of patients in the CT group (p<0.001). |
| D. Chowdhury et al. (2024). | The Consortium to Establish a Registry for Alzheimer’s Disease (CERAD) was used to monitor cognition improvement. Memory (CERAD recall of CP, p<0.0001). The baseline score of the CERAD recall of CP was 4.1 and the week 18 score was 5.9 which had approximately a +1.8 change which is a significant difference. |
| O. Băjenaru et al. (2020). | Yes, there was a significant improvement (p<0.0001). There was a significant increase in MMSE scores after the 24 month follow up as the mean MMSE score at baseline was around 26.7 and the mean score after the follow up was 28.2 which has approximately a +1.5 change. |
| S. Goto et al. (2020). | Significance was established at p<0.05: and a result was considered to be trending at p<0.1. Group 1 significantly improved from 7.8 to 10.3 (p=0.002). By contrast, the average MMSE of Group 2 remained at the same level. Showed improvement in one treatment group (p=0.002) but not the other (p>0.05). |
| S. I. Gavrilova et al. (2014). | The Trail-Making Test (TMT-A or TMT-B) was used to test for cognition improvements. The TMT-A score in the EGb 761 group changed by around -22.4 with a standard deviation of 23.0. The TMT-A score in the placebo group changed by around -18.1 with a standard deviation of 25.2. The TMT-B score in the EGb 761 group changed by around -44.7 with a standard deviation of 36.8. The TMT-B score in the placebo group changed by around -32.2 with a standard deviation of 39.0. |
| R. Krikorian et al. (2009). | The California Verbal Learning Test (CVLT) was used to test the patients’ improvements in cognition through learning and recall. The placebo group had a CVLT learning test score of 33.2 at the baseline and had the same score after 12 weeks. However, the Concord grape juice group changed by 3.4 with a change from the baseline score of 35.2 to a final score of 38.6. In addition, in the placebo group of the CVLT recall group there was a -0.4 change as the baseline score was a 5.4, and the final score was a 5.0. The Concord grape juice group had a bigger change in score of 1.2 as the baseline score was 6.0 and the final score was 7.2. |
| M. Tsolaki et al. (2016). | Yes, MMSE showed significant change (p=0.05). The MMSE score in the intervention group before the treatment was around 27.41, but the score after the 12 month intervention was around 28.18 which was a change of about 0.77. However, the MMSE score of the control group changed significantly less as the first MMSE score was 27.89, but the final score was 27.11. |
| S.-T. Lee et al. (2008). | Yes, after ginseng treatment, the cognitive subscale of ADAS and the MMSE score began to show improvements and continued up to 12 weeks (p=0.029 and p=0.009 vs. baseline, respectively. The MMSE score in the ginseng group improved by around 1.8 points from baseline until the end of the 12 week intervention. However, the control group changed by around -0.03 from baseline until the end of the 12 week intervention. Similarly, in the ADAS-cog score, the ginseng group showed improvement from baseline until the end of the 12 week intervention with a change of around -4.2. In comparison, the control group only changed by around 1.1. |
| S. Akhondzadeh et al. (2003). | Yes (p<0.0001). S. officinalis extract produced a significant better outcome on cognitive functions than placebo (ADAS-cog: F=4.77, d.f.=1, p=0.03) (CDR-SB: F=10.84, d.f.=1, p<0.003). |
| S. Akhondzadeh et al. (2003). | Yes, significant change on ADAS-cog score across time (p<0.0001). The change at the end of the trial was also significant with the same p-value (p<0.0001). The change in the ADAS score in the Melissa extract group after the 16 weeks of intervention from baseline was around -6.40. However, the change in the ADAS score in the placebo group was 5.60 which is significantly different from the Melissa extract group. |
| Adrian R. Whyte et al. (2018). | Post hoc simple contrast analysis, using placebo as the reference category, revealed a significantly better performance following WBE111 intervention (mean = 0.926) in comparison to placebo (mean = 0.871) (p=0.038). |
| DeKosky et al. (2008). | 523 of the individuals in the study developed dementia, 246 from the placebo group and 277 from the Ginkgo group. 92% of the dementia proved to be possible or probable Alzheimer’s disease. Ginkgo biloba also had no effect on the rate of progression to dementia in participants with MCI (HR, 1.13; 95% CI, 0.85-1.50; P = .39). |
| B. E. Snitz et al. (2009). | The rates of decline between the Ginkgo and placebo groups didn’t differ in memory (0.043; 95% confidence interval [CI], 0.034-0.051 vs 0.041; 95% CI, 0.032-0.050), and executive functions (0.092; 95% CI, 0.086-0.099 vs 0.089; 95% CI, 0.082-0.096). Between ADAS-Cog and 3MSE, there were differing rates, but both ultimately showed no significant difference between groups (for 3MSE, P=.71; for ADAS-Cog, P=.97). |
Discussion
The purpose of this review was to summarize the potential of native/Eastern medical practices, specifically plant-based treatments, in preventing or slowing cognitive decline. To do this, a systematic review was conducted. All the participants in the studies were older adults from different countries of the world. Overall, results suggested that multiple treatments from native plant species displayed a significant improvement in cognition.
Certain treatments produced better results in cognitive improvement than others. The study with the administration of Bacopa monnieri capsules showed notable results. The study focused on aiding patients of MCI for cognitive function and reported improvements. Similarly, multiple papers included were written with trials for the Ginkgo biloba extract. Two particular studies were completed with participants over the age of 50 years old; however, one study focused on patients with a major neurocognitive disorder, and the other focused on patients with MCI. Since both studies targeted different populations, the treatment differed, but Ginkgo biloba showed effective results. Ginkgo biloba showed benefits for people who suffered from different stages of cognitive decline, suggesting the extract might be useful in multiple cases. Other studies which demonstrated a significant increase in cognition were the separate studies done for S. officinalis and Melissa officinalis extracts. Both studies were completed in the same year, with similar populations, with similar treatments, and with a common author. Both papers returned a result of significant improvement in cognition.
Although many treatments returned significant increases in cognition, some treatments appeared to be less effective. The treatments done with individuals with no or only minor cognitive decline returned significant results with smaller effect sizes than studies done with individuals with MCI or dementia. For example, one study used grape juice consumption as a treatment to reduce cognitive decline in adults with early cognitive decline. This study included the administration of grape juice which was effective, but not as effective as the trials listed above. As such, these results suggest that concentrated plant extracts, such as Ginkgo biloba, may be more effective in improving cognition than dietary supplements that could commonly be found in households (e.g., grape juice, essential oils). However, the population played an important part in the results as well. It was easier to conduct trials for people who suffered from MCI than people who either had cognitive decline through experiencing dementia or completely healthy with no cognitive decline. Once a person is suffering from extreme cognitive decline through Alzheimer’s disease or vascular dementia, it becomes more difficult to combat the cognitive decline with medication from a native plant species. Similarly, specific plants are helpful when there is a problem which can be identified and prevented earlier on, like patients with MCI. However, for healthier adults who haven’t experienced cognitive decline, it is harder to find a specific treatment to solve a problem which hasn’t been created yet.
As this paper includes treatments for patients ranging from faint cognition loss to MCI to AD, it is inaccurate to generalize all of the findings relative to one another. While treatments directed towards Alzheimer’s disease have been successful, it is unfair to compare them to the results of a treatment directed towards MCI and deem it less effective. Analyzing as a whole, the papers with treatments for patients with MCI have been more successful to decrease cognitive decline in their patients because the patients experience cognitive decline, but it is not incredibly severe yet. It is important to note that the treatments for MCI have been more successful because the brain isn’t severely impacted by then, but the AD treatments have been slightly successful towards improving cognition in their treatments. These developments should be treated differently as the patients’ conditions differ between the populations.
Several limitations were significant throughout this research paper. Firstly, Ginkgo biloba was a widely tested treatment, and it was successful in many treatments. However, as it was widely tested, it had quite a few results which were unsuccessful. To prevent showing bias, results that were both successful and unsuccessful were included. It should be pointed out that successful results were in the majority, so it suggests that Ginkgo biloba was an effective treatment. It should also be considered that these treatments were all conducted in different regions in which the individuals have different diets and lifestyles. These diets could allow those patients to be familiar with what their treatment contains, making it easier to be successful. However, when that treatment is applied in other geographic populations, those people may have a different reaction to the treatment because they are not used to what the treatment contains. Their diets are different as people around the world eat different things. Currently, it is inaccurate to generalize treatment results from one area to global populations, but hopefully with further research, they can be. Finally, the goal of this research paper was to identify various successful treatments which would improve cognition and analyze them together. This impacted the outcome of this paper as it was selective towards papers which demonstrated an improvement in cognition. However, to reduce bias, if an included treatment also had unsuccessful trials, they would be included to show the overall effectiveness of the treatment.
Conclusion
In conclusion, various native plant species were administered in different treatments in order to reduce cognitive decline or improve cognition. The trials included participants with a wide spectrum of cognitive decline from having healthy cognition to suffering from dementia. Through the analysis of the papers, some plant species were found to have significantly better improvements of cognition than others, but ultimately, all treatments analyzed ended up improving cognition at different levels. This systematic review serves as initial evidence of these successful treatments. Future research should conduct robust clinical trials to provide further evidence of their efficacy across populations and levels of cognitive decline. This will allow for further development of effective intervention for cognitive decline, improving quality of life on an individual and global scale.
References
- J. M. Hale, D. C. Schneider, N. K. Mehta, M. Myrskylä, Cognitive impairment in the U.S.: Lifetime risk, age at onset, and years impaired, SSM – Population Health. Vol. 11, pg. 100590, 2020 [↩]
- Dementia, World Health Organization, 2025 [↩]
- E. Nichols, J. D. Steinmetz, S. E. Vollset, K. Fukutaki, J. Chalek, F. Abd-Allah, A. Abdoli, A. Abualhasan, E. Abu-Gharbieh, T. T. Akram, H. A. Hamad, F. Alahdab, F. M. Alanezi, V. Alipour, S. Almustanyir, H. Amu, I. Ansari, J. Arabloo, T. Ashraf, … T. Vos, Estimation of the global prevalence of dementia in 2019 and forecasted prevalence in 2050: An analysis for the Global Burden of Disease Study 2019, The Lancet Public Health. Vol. 7, pg. e105–e125, 2022 [↩]
- National Center for Biotechnology Information (US), Mild Cognitive Impairment, StatPearls Publishing, Treasure Island (FL), 2024 [↩]
- N. L. Campbell, F. Unverzagt, M. A. LaMantia, B. A. Khan, M. A. Boustani, Risk factors for the progression of mild cognitive impairment to dementia, Clinics in Geriatric Medicine. Vol. 29, pg. 873–893, 2013 [↩]
- Mayo Foundation for Medical Education and Research, Alzheimer’s disease, Mayo Clinic, 2024 [↩]
- National Institute on Aging, What happens to the brain in Alzheimer’s disease?, 2024 [↩]
- G. Livingston, J. Huntley, K. Y. Liu, S. G. Costafreda, G. Selbæk, S. Alladi, Dementia prevention, intervention, and care: 2024 report of the Lancet Standing Commission, The Lancet. Vol. 404, pg. 1543–1600, 2024 [↩]
- Alzheimer’s Association, Medications for memory, cognition & dementia-related behaviors, 2024 [↩]
- U.S. National Library of Medicine, Alzheimer’s disease: Learn more – Non-drug interventions for Alzheimer’s disease, InformedHealth.org [Internet], 2022 [↩]
- S. Weinmann, S. Roll, C. Schwarzbach, C. Vauth, S. N. Willich, Effects of Ginkgo biloba in dementia: Systematic review and meta-analysis, BMC Geriatrics. Vol. 10, pg. 14, 2011 [↩]
- D. Choudhary, S. Bhattacharyya, S. Bose, Efficacy and safety of Ashwagandha (Withania somnifera (L.) Dunal) root extract in improving memory and cognitive functions, Journal of Dietary Supplements. Vol. 14, pg. 599–612, 2017 [↩]
- D. Jimbo, Y. Kimura, M. Taniguchi, M. Inoue, K. Urakami, Effect of aromatherapy on patients with Alzheimer’s disease, Psychogeriatrics: The Official Journal of the Japanese Psychogeriatric Society. Vol. 9, pg. 173–179, 2010 [↩]
- M. Delfan, P. Kordestani-Moghaddam, M. Gholami, K. Kazemi, R. Mohammadi, Evaluating the effects of Bacopa monnieri on cognitive performance and sleep quality of patients with mild cognitive impairment: A triple-blinded, randomized, placebo-controlled trial, Explore (New York, N.Y.). Vol. 20, pg. 145–153, 2024 [↩]
- J. Shi, J. Ni, T. Lu, X. Zhang, M. Wei, T. Li, W. Lu, Y. Wang, Y. Shi, J. Tian, Adding Chinese herbal medicine to conventional therapy brings cognitive benefits to patients with Alzheimer’s disease: A retrospective analysis, BMC Complementary and Alternative Medicine. Vol. 17, pg. 533–540, 2017 [↩]
- D. Chowdhury, A. K. Roy, V. R. Reddy, Y. K. Gupta, P. Nigam, R. Hoerr, Multicenter, open-label, prospective study shows safety and therapeutic benefits of a defined Ginkgo biloba extract for adults with major neurocognitive disorder, Dementia and Geriatric Cognitive Disorders. Vol. 63, pg. 271–281, 2024 [↩]
- O. Băjenaru, G. Prada, F. Antochi, C. Jianu, C. Tudose, A. Cuciureanu, A. A. Docu, V. Perrot, M. Avram, C. Tiu, Effectiveness and safety profile of Ginkgo biloba standardized extract (EGB761®) in patients with amnestic mild cognitive impairment, CNS & Neurological Disorders Drug Targets. Vol. 20, pg. 124–131, 2021 [↩]
- S. Goto, H. Suzuki, T. Nakagawa, K. Shimizu, The effect of eucalyptol on nursing home residents, Scientific Reports. Vol. 10, pg. 3405–3413, 2020 [↩]
- S. I. Gavrilova, U. W. Preuss, J. W. M. Wong, R. Hoerr, R. Kaschel, N. Bachinskaya, GIMCIPlus Study Group, Efficacy and safety of Ginkgo biloba extract EGB 761 in mild cognitive impairment with neuropsychiatric symptoms: A randomized, placebo-controlled, double-blind, multi-center trial, International Journal of Geriatric Psychiatry. Vol. 29, pg. 1087–1095, 2014 [↩]
- R. Krikorian, T. A. Nash, M. D. Shidler, B. Shukitt-Hale, J. A. Joseph, Concord grape juice supplementation improves memory function in older adults with mild cognitive impairment, The British Journal of Nutrition. Vol. 103, pg. 730–734, 2009 [↩]
- M. Tsolaki, E. Karathanasi, I. Lazarou, K. Dovas, E. Verykouki, A. Karacostas, K. Georgiadis, A. Tsolak, K. Adam, I. Kompatsiaris, Z. Sinakos, Efficacy and safety of Crocus sativus L. in patients with mild cognitive impairment: One-year single-blind randomized, with parallel groups, clinical trial, Journal of Alzheimer’s Disease (JAD). Vol. 54, pg. 129–141, 2016 [↩]
- S.-T. Lee, K. Chu, J.-Y. Sim, J.-H. Heo, M. Kim, Panax ginseng enhances cognitive performance in Alzheimer disease, Alzheimer Disease and Associated Disorders. Vol. 22, pg. 222–226, 2008 [↩]
- S. Akhondzadeh, M. Noroozian, M. Mohammadi, S. Ohadinia, A. H. Jamshidi, M. Khani, Salvia officinalis extract in the treatment of patients with mild to moderate Alzheimer’s disease: A double blind, randomized and placebo-controlled trial, Journal of Clinical Pharmacy and Therapeutics. Vol. 28, pg. 53–59, 2003 [↩]
- S. Akhondzadeh, M. Noroozian, M. Mohammadi, S. Ohadinia, A. H. Jamshidi, M. Khani, Melissa officinalis extract in the treatment of patients with mild to moderate Alzheimer’s disease: A double blind, randomised, placebo controlled trial, Journal of Neurology, Neurosurgery, and Psychiatry. Vol. 74, pg. 863–866, 2003 [↩]
- A. R. Whyte, N. Cheng, E. Fromentin, C. M. Williams, A randomized, double-blinded, placebo-controlled study to compare the safety and efficacy of low dose enhanced wild blueberry powder and wild blueberry extract (ThinkBlue™) in maintenance of episodic and working memory in older adults, Nutrients. Vol. 10, pg. 660–670, 2018 [↩]
- S. T. DeKosky, J. D. Williamson, A. L. Fitzpatrick, R. A. Kronmal, D. G. Ives, J. A. Saxton, O. L. Lopez, G. Burke, M. C. Carlson, L. P. Fried, L. H. Kuller, J. A. Robbins, R. P. Tracy, N. F. Woolard, L. Dunn, B. E. Snitz, R. L. Nahin, C. D. Furberg, Ginkgo biloba for prevention of dementia: a randomized controlled trial, JAMA. Vol. 300, pg. 2253-2262, 2008 [↩]
- B. E. Snitz, E. S. O’Meara, M. C. Carlson, A. M. Arnold, D. G. Ives, Ginkgo biloba for Preventing Cognitive Decline in Older Adults: A Randomized Trial, JAMA. Vol. 302, No. 21, 2009 [↩]
 Using Public Bioinformatics Resources")

